Article Text

Abstract
Background Indigenous children suffer a disproportionally high burden of unintentional injuries. A more detailed understanding of the underlying causes, risk factors and gaps in research is required to inform prevention efforts and direct future research. The aim of this review was to systematically assess the evidence regarding differences in rates of unintentional injuries between indigenous and non-indigenous children and to identify leading causes and underlying risk factors contributing to these differences.
Method We systematically searched the literature including 10 electronic databases, institutional websites and reference lists of relevant studies. Due to the substantial heterogeneity between studies, results were summarised in a narrative synthesis and no meta-analysis was carried out.
Results A total of 39 studies were included in this review. Most studies were descriptive and only five adjusted for potential confounding in the analysis. Indigenous to non-indigenous rate ratios for morbidity and mortality for unintentional injury ranged from 1.2 to 2.3 and 1.8 to 8.2, respectively. The difference varied greatly by cause of injury and between studies, ranging from a reduced risk of hospitalisation due to fall injuries to a 17-fold increased risk of mortality due to pedestrian injuries. Burns, poisoning and transport injuries were the major contributors to the increased injury burden in indigenous children. The studies offered only limited insight into the underlying causes of these differences, but socioeconomic status and parents’ educational attainment were contributing factors.
Conclusions Indigenous children experience a significantly higher burden of morbidity and mortality from unintentional injuries across different indigenous communities worldwide. Most of these injuries are highly preventable, presenting substantial potential to improve indigenous child health. However, there is limited evidence to illuminate the underlying risk factors for unintentional injuries in indigenous children, and this is a priority for further research.
- Risk/Determinants
Statistics from Altmetric.com
Background
Unintentional injuries are a leading cause of child morbidity and mortality. Worldwide, they cause around 830 000 child deaths each year, with road crashes, drowning, burns, falls and poisoning being the main contributors.1 Studies in indigenous communities have consistently shown that indigenous children are disproportionally affected by unintentional injuries, with some studies reporting morbidity and mortality rates at least double those in non-indigenous children.2–8
Reducing child injuries and health inequalities for indigenous people are key policy priorities internationally. A child's right to a safe environment and protection from injury is affirmed in the Convention on the Rights of the Child,9 ratified by 193 governments, while the right of indigenous people to the highest attainable standard of physical and mental health is acknowledged in the declaration of the rights of indigenous people adopted by the United Nations in 2007.10
Despite this, empirical research on unintentional injuries and their underlying risk factors in indigenous children is limited.11–14 Cultural alienation and dispossession,15 low socioeconomic status5 ,16–18 and geographical remoteness2 ,4 ,11 ,16 ,19 have been discussed as key factors contributing to the higher burden of injury among indigenous children. However much of the evidence on low socioeconomic status and geographical remoteness stems from population-level studies and is not specific to indigenous children. A more detailed understanding of the underlying causes in indigenous children is required to inform prevention efforts.
Toward this aim, we performed a systematic review of international studies that investigated inequalities in unintentional injuries between indigenous and non-indigenous children, in order to address the following questions: (1) How large is the difference in rates of unintentional injury in indigenous compared with non-indigenous children? (2) Does this difference vary according to the cause of injury? and (3) What are the underlying risk factors contributing to these differences?
Methods
Search strategy
We systematically searched the literature for studies relating to three concept areas: children (0–19 years); indigenous status; and unintentional injuries. The search was conducted in November 2012 and updated in November 2013. Studies were identified using an electronic database search and searching of institutional websites and reference lists of relevant studies. (The electronic database search covered 10 databases which were chosen on the basis of their relevance to child injuries and indigenous health (Scopus, Pubmed, CINHAL, PSYCINFO, Web of Science, Pro Quest Social Science, INFORMIT (ATSI Health, RURAL, Indigenous collection and Health Collection), SafetyLit, Cochrane Library Databases, Native Health database of the University of Mexico). The search strategy used a combination of keywords and subject headings (box 1, and see online supplement table S1). No publication date period or other limitations were applied. Additionally, the websites of Health Canada, United States Centers for Disease Control (including the Morbidity and Mortality Weekly Report), Australian Institute of Health and Welfare and New Zealand Ministry of Health were searched.
Search terms used to identify relevant studies for the review
Population
-
child*
-
adolesc*
-
teen*
-
paediatric*
-
pediatric*
-
youth
-
infant
-
“young people”
-
juveniles
-
1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 Or 9
Exposure†
-
indigenous
-
aborigin*
-
tribe*
-
tribal
-
“minority group”
-
inuit
-
maori
-
“american indian”
-
“native american”
-
“first nation*”
-
metis
-
sami
-
11 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
Outcome
-
injur*
-
accident*
-
poison*
-
burn*
-
fall*
-
drowning*
-
24 OR 25 OR 26 OR 27 OR 28 OR 29
Combined search
10 AND 23 AND 30
†In an exploratory analysis using PubMed, we found the search terms indigenous and aborigin* identified the vast majority of large indigenous populations worldwide, although some populations were only identified using specific names (eg, Sami). The majority of small indigenous populations were identified using the search term ‘tribe’.
Inclusion criteria, data extraction and quality appraisal
Studies were included in the review if they met each of the following criteria: (1) presented findings from primary research; (2) investigated one or more types of unintentional injuries; (3) included children aged 0–19 years; (4) included indigenous children and a comparator group; and (5) presented results as rates or ratios, not just numbers. Where more than one study presented findings for the same geography and injury types, using the same datasets, we included only the most recent study. Studies meeting the inclusion criteria were summarised using a standardised data extraction form, including the following items: author and year, place, study period, indigenous group studied, age group, study design, analysis and outcome measure, adjustment for confounding, datasets/data linkage, injury outcomes, measure of indigenous status, results, comments and method of study identification. Injury rate ratios for indigenous and non-indigenous children were extracted or calculated. Study selection and data abstraction was carried out in a standardised way by one author (HM). In the case of difficult decisions, the other authors were consulted. The study selection process is summarised in a flow diagram (figure 1).

PRISMA diagram flow chart of systematic literature search.20
Methodological quality was assessed using the Liverpool University Quality Assessment Tool (LQAT), which was adapted for the current review questions. The tool focuses on five main methodological domains (sampling, exposure/intervention, outcome, analysis and impact), and is derived from larger LQATs used in a number of systematic reviews.21 ,22 The tool has been independently appraised against other quality assessment instruments.23
Results
The electronic database search returned 3577 records, and 255 records were identified from other sources. Of these, 1209 were duplicates, leaving 2499 records for screening of title and abstract. From these, 96 studies were included for full-text analysis, and 39 met the inclusion criteria for the review (figure 1). The relatively large number of records obtained from ‘other’ sources (255) reflected the capabilities of search engines of institutional websites, which did not allow for the same level of detail as the database search. Four records were identified from the grey literature, all of which were included in the systematic review. Of the 39 studies included in the review, 21 were from the USA,2 ,7 ,19 ,24–41 8 from Australia,4 ,8 ,42–47 7 from Canada3 ,5 ,48–52 and 3 from New Zealand.6 ,17 ,53 More than half the studies (n=23) presented mortality data,2 ,5 ,7 ,19 ,24 ,26–28 ,30 ,31 ,34–38 ,40 ,41 ,45 ,46 ,48 ,49 ,51 ,52 with the remainder investigating mortality and morbidity (n=8),3 ,6 ,8 ,39 ,42 ,47 ,53 ,54 morbidity only (n=7)4 ,17 ,29 ,33 ,43 ,44 ,50 and Years of Potential Life Lost (n=1).25 All studies investigating morbidity outcomes were based on hospital data, the terms, morbidity and hospitalisation, are therefore used interchangeably hereafter. Transport injuries were most frequently studied, followed by burn injuries and drowning (table 1). Most studies were descriptive, used routinely collected mortality and/or hospital morbidity data, and did not investigate the effect of potential confounding or explanatory variables in the analysis. Only five studies adjusted for covariates.26 ,30 ,39 ,41 ,44 Most studies derived an individual's indigenous status from a single source, mainly hospital morbidity or mortality data; however, five studies used an ecological study design where indigenous status was measured at an area level.3 ,49–52
Ten most researched causes of unintentional child injury in studies identified in the systematic literature search*
Of the 39 studies included in the review, 27 specifically focussed on children (defined as 0–19 years in this study). The other 12 studies included people older than 19 years in the sample and/or provided less detailed results for 0–19-year-olds or smaller sub-groups within this age range. Fifteen studies analysed data collected in the last decade,8 ,17 ,24 ,25 ,29–31 ,38 ,39 ,42 ,44 ,47 ,50–52 and the remaining studies were based on data prior to 2002.
How large is the inequality in rates of unintentional injury in indigenous compared with non-indigenous children?
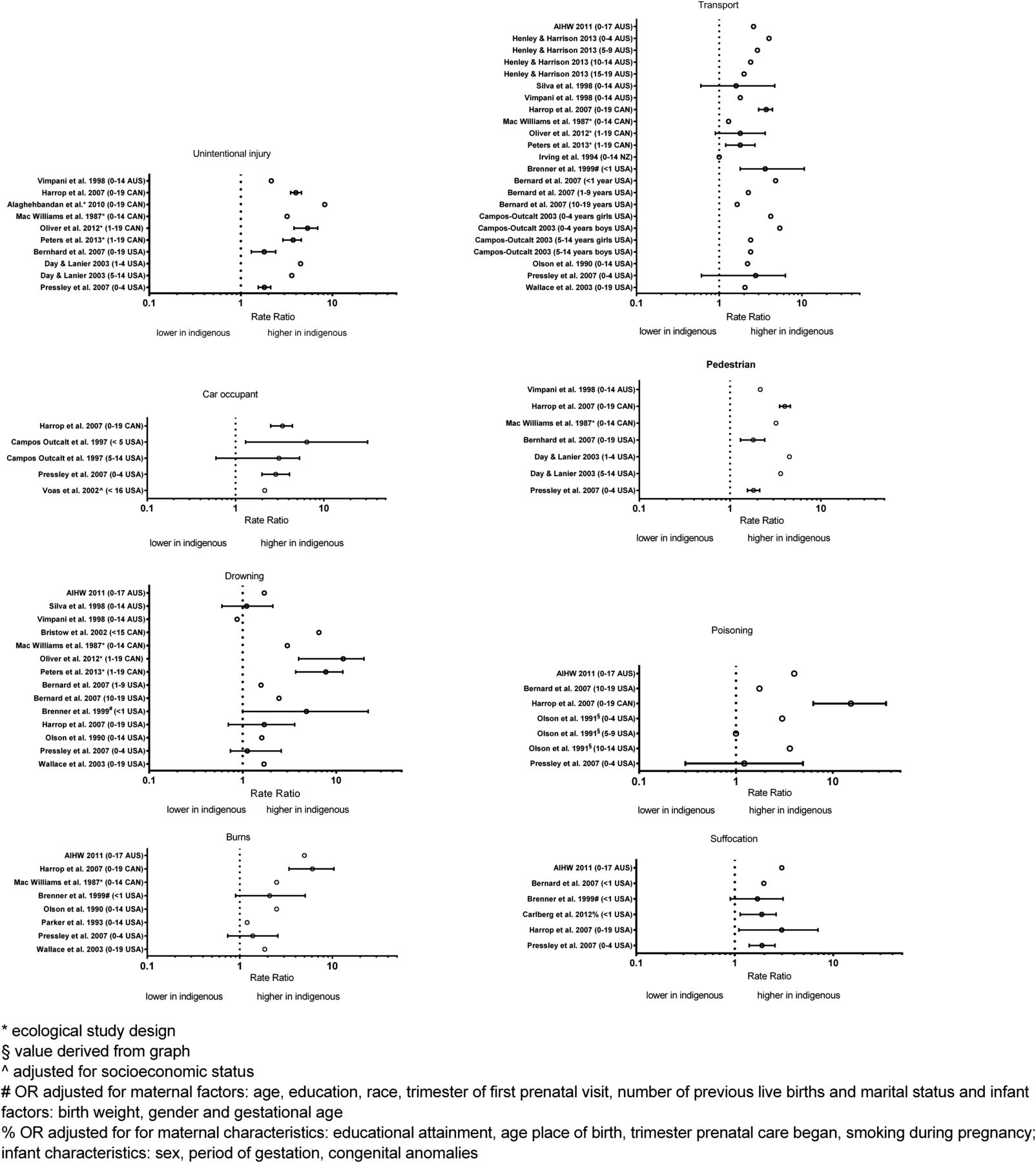
Out of the 39 studies included in this review, 13 reported findings for all unintentional injury outcomes combined. Indigenous to non-indigenous rate ratios for morbidity and mortality ranged from 1.2 to 2.33 ,33 ,50 and 1.8 to 8.2,3 ,5 ,19 ,24 ,31 ,38 ,46 ,49 ,51 ,52 respectively. One study from the USA reported 1.6 and 1.8 times higher rates of years of potential life lost among American Indian and Alaskan Native boys and girls, respectively, compared with white American children25 (figures 2 and 3 and see online supplement 2 table S2). The greatest differences in morbidity and mortality between indigenous and non-indigenous children were reported by four Canadian studies that used an ecological study design,3 ,50–52 measuring indigenous status at the area, as opposed to the individual, level.3 ,50 ,51 Four studies differentiated by age groups,3 ,19 ,24 ,31 (see online supplement table S2), two of these from the USA reported higher mortality inequalities in the youngest age groups (under 1-year-olds and 1–4-year-olds) compared with 1–9 and 10–19-year–olds, respectively.19 ,24 By comparison, a recent study from the USA reported lower mortality inequalities in the under 1-year-olds and 1–4–year-olds, compared with the 5–14-year–olds,31 and a Canadian study showed no age pattern in the size of inequalities in the analysis of hospital data.3

Rate ratios of morbidity due to unintentional injuries for indigenous to non-indigenous children.

{kind=link}
{kind=link}
{kind=link}
Rate ratios of mortality due to unintentional injuries for indigenous to non-indigenous children.
Does this difference vary according to the cause of injury?
Transport, land transport and motor vehicle crash (MVC) injuries
Transport-related injuries were the most commonly investigated injury type, and were reported in 29 out of the 39 studies included in our review (figures 2 and 3 and see online supplement 2 table S2).2–8 ,24 ,26–28 ,32–35 ,38–43 ,45 ,46 ,49–53 Of these 29 studies 24 reported results for all land transport and MVC injuries combined, whereas the remainder investigated more specific causes of transport injuries. For all transport injuries combined, rate ratios of hospitalisation, and mortality between indigenous and non-indigenous children ranged from 0.8 to 4.03 ,4 ,8 ,32 ,33 ,42 ,43 ,47 ,50 ,53 and 1.6–5.9,2 ,5 ,7 ,8 ,24 ,34 ,38 ,40 ,42 ,45 ,46 ,49 ,51–53 respectively. Almost all studies showed higher rates of hospitalisation and death from transport injuries in indigenous compared with non-indigenous children. In contrast with the findings of most studies, two recent studies from Australia showed no difference in, or slightly lower, hospitalisation rates in older Aboriginal children, aged over 10 years.8 ,47 Seven studies differentiated by age groups in the analysis, all reported the highest difference in hospitalisation and mortality due to transport injuries between indigenous and non-indigenous children in the youngest age groups.2 ,8 ,24 ,27 ,40 ,43 ,47 (see online supplement table S2) Morbidity and mortality rate ratios were about double in the 0–4-year-olds compared with the 5–9-year-olds.
Motor vehicle occupant injuries
Five studies included in our review investigated MVCs where the child was an occupant.5 ,8 ,27 ,38 ,41 Rate ratios for morbidity and mortality for indigenous compared with non-indigenous children ranged from 1.1 to 2.88 and 2.1 to 3.45 ,27 ,38 respectively. The greatest morbidity difference of 2.8 was reported for the youngest age group (0–4-year-olds) in a recent study from Australia.8
Pedestrian injuries
Nine studies looked at differences in pedestrian injuries between indigenous and non-indigenous children.5–8 ,27 ,28 ,35 ,38 ,54 Rate ratios for hospital admissions and deaths from pedestrian injuries comparing indigenous and non-indigenous children ranged from 1.5 to 4.56 ,8 ,32 and 0.7 to 17,5 ,6 ,7 ,27 ,28 ,35 ,38 ,54 respectively. The highest mortality rate ratio of 17 was reported for non-motor vehicle transport-related pedestrian injuries in a Canadian study; however, the study sample was small and the 95% CI around the point estimate was wide (7.8–35.9).5 By comparison, one study from the USA27 reported a lower risk of mortality in Native American children in Arizona compared with the rest of the population. Two studies from Australia and the USA reported that the largest difference in hospitalisation due to pedestrian injuries between indigenous and non-indigenous children was in the youngest age group (0–4 years).8 ,28
Burns and scalds
Fourteen studies compared rates of burn and scald injuries between indigenous and non-indigenous children.3 ,5 ,7 ,17 ,26 ,32–34 ,37 ,38 ,42 ,47 ,49 ,50 All studies showed an increased risk of injuries and death from burns among indigenous children, and one study reported no difference for hospitalisation due to scalds in indigenous compared with non-indigenous children.33 Rate ratios for hospitalisation and mortality due to burn injuries in indigenous compared with non-indigenous children ranged from 1.3 to 4.43 ,17 ,33 ,42 ,47 ,50 ,54 and 1.2 to 6.1,5 ,7 ,34 ,37 ,38 ,42 ,49 respectively.
Studies from Australia and New Zealand reported higher inequalities for hospitalisation due to burn injuries in the younger compared with the older age groups (see online supplement table S2).17 ,47
Drowning
Fourteen studies investigated differences in injuries due to drowning between indigenous and non-indigenous children5 ,7 ,24 ,26 ,34 ,38 ,42 ,45 ,46 ,48–52 A Canadian study that measured indigenous status at the area level reported a 3.7 times higher rate of hospitalisation due to drowning for children living in areas with a high proportion of Aboriginal people (ie, more than 33%).50 There was substantial variation in mortality rate ratios between the different studies, ranging from 0.9 to 10.1.5 ,7 ,24 ,34 ,38 ,42 ,45 ,46 ,48 ,49 ,51 ,52 The highest mortality difference of 10.1 (95% CI 5.0 to 20.5) was reported in a Canadian study, which measured indigenous status at the area level (92% of children in this area identified as Inuit at the last census).51
Falls
Ten studies investigated differences in injuries due to falls between indigenous and non-indigenous children.3 ,5 ,33 ,38 ,42 ,44 ,47 ,49 ,50 ,54 Findings varied greatly between studies, with rate ratios for hospitalisation and mortality ranging from 0.3 to 2.03 ,33 ,42 ,44 ,47 ,50 ,54 and 0.5–2.2,5 ,38 ,49 respectively. Although most studies showed a lower risk or no significant difference in rates of hospitalisation and mortality due to falls in indigenous compared with non-indigenous children, three studies that measured indigenous status at the area level reported a significant positive association.3 ,49 ,50 A study from Australia differentiating by 5-year age groups, showed no pattern in inequalities by age groups.47
Poisoning
Nine studies reported differences in injuries due to poisoning.3 ,5 ,24 ,33 ,36 ,38 ,42 ,47 ,50 Rate ratios for indigenous compared with non-indigenous children for hospitalisation and mortality ranged from 1.1 to 3.93 ,33 ,42 ,47 ,50 and 1.2 to 15.4,5 ,24 ,36 ,38 ,42 respectively. The highest rate ratio of 15.4 for mortality was reported in a Canadian study; however, the study sample was small and the 95% CI around the point estimate was wide (ie, 6.3 to 35.5).5 An Australian study reported the greatest inequalities for hospitalisation due to poisoning in 5–9-year-old children, with rate ratios of 2.5 and 2.9 for Aboriginal compared with non-Aboriginal boys and girls, respectively.47 An Australian study differentiagting by 5-year age groups reported the highest inequalities for poisoning hospitilisation in 5–9-year-old boys and girls.47
Suffocation
Seven studies investigated differences in hospitalisation and mortality due to suffocation5 ,24 ,26 ,30 ,34 ,38 ,42 Five studies showed 1.9–3 times higher mortality rates due to suffocation in indigenous children compared with non-indigenous children.5 ,24 ,38 ,42 By comparison, a study from Washington in the USA reported no difference in hospitalisation rates for suffocation between American Indian and Native Alaskan children compared with children of all other ethnic backgrounds.33 A study investigating maternal and infant characteristics associated with deaths from suffocation and strangulation in infants reported an adjusted OR of 1.8 (95% CI 1.2 to 2.67) for American Indian children compared with white American children.30
Cutting and piercing injuries
Four studies investigated differences in injuries requiring hospitalisation due to cutting and piercing.3 ,33 ,47 ,50 All of these showed increased rates of hospitalisation in indigenous children, with rate ratios ranging from 1.1 to 3.4 for indigenous compared with non-indigenous children.3 ,33 ,47 ,50 The largest difference (rate ratio 3.4) was reported among 15–19-year-old girls in an Australian study.47
What are the underlying risk factors?
Only five studies included in our review adjusted for covariates in the analysis,26 ,30 ,39 ,41 ,44 and were therefore able to provide some insight into underlying risk factors and the influence of confounding.
A recently published study from the USA investigated maternal and infant characteristics associated with infant deaths due to suffocation.30 This study adjusted for a number of covariates relating to the mother (education, age, ethnicity, place of birth, trimester prenatal care begun, smoking during pregnancy and parity) and child (sex, period of gestation, congenital anomalies) (see online supplement 2 table S2). Adjusting for all covariates reduced the risk of death from suffocation in American Indian infants from 2.9 (95% CI 2.0 to 4.3) to 1.8 (95% CI 1.2 to 2.7). Another study from the USA adjusted for a number of covariates relating to the child (birth weight, gender and gestational age) and their mother (age, education, race, trimester of first prenatal visit, number of previous live births and marital status) in the analysis of injury mortality (see online supplement table S2). Compared with white children, Native American children had higher adjusted odds of death from all unintentional injury outcomes included in that study (figure 3 and see online supplement table S2).26 However, this study did not quantify how adjusting for these covariates influenced the size of the inequalities, because the unadjusted rate ratios were calculated at the population level, and adjusted ORs were derived from a matched case control study design. Another study in the USA adjusted for area-level socioeconomic status in an analysis of deaths among child car occupants where the driver was under the influence of alcohol.41 This study reported adjusted odds for Native American compared with white children of 2.1 and 0.5, respectively, for being injured in a car crash where the driver was under the influence of alcohol and for not being restrained in the vehicle. After adjusting for socioeconomic factors, the odds of not being restrained decreased from 0.4 to 0.5.41 In California, the crude rate of in-hospital death due to injury was lower in Native American (0.6 per 100) compared with non-Hispanic white children (0.8 per 100), but after adjustment for a number of covariates in the analysis, there was no statistical difference of in-hospital death (OR 0.6, 95% CI 0.2 to 2.1) (see online supplement 2 table S5).39 An Australian study explored the interaction of gender and Aboriginal status on fall injuries.44 After including an interaction term for gender and Aboriginality in the model, the IRR (1.2 95% CI 0.9 to 1.4) for Aboriginal compared with non-Aboriginal children decreased by 21% compared with the unadjusted rate.
Discussion
Key findings
Our review highlighted the persistence of inequalities in morbidity and mortality from unintentional injury between indigenous and non-indigenous children across different communities worldwide. For most causes of unintentional injury, indigenous children experienced significantly higher morbidity and mortality, and inequalities were generally larger for mortality compared with morbidity. The leading causes of inequalities were burns, poisoning and transport injuries. Studies that differentiated by age group showed that the inequalities, in particular for transport injuries, were greatest in the younger age groups. Comparing the earliest studies from the late 1980s with the most recent studies showed that little progress in reducing these inequalities has been achieved in the last 35 years.
The existing literature provides only limited insight into the underlying risk factors for unintentional injuries in indigenous children. Most studies identified were purely descriptive, and only five investigated the impact of potential confounding factors or explanatory variables in their analyses.26 ,30 ,39 ,41 ,44 However, socioeconomic status and educational attainment of the mother explained some of the differences between indigenous and non-indigenous children.30 ,41
Strengths and limitations
To our knowledge, this is the first systematic review of studies of inequalities in unintentional injuries between indigenous and non-indigenous children. Our findings will assist in guiding policy and planning by identifying the magnitude of inequalities and how these vary by type of injury. They also highlight gaps in current research, which will assist in planning and prioritising new research in this field. Although we made great efforts to identify all relevant articles in databases and in the grey literature, by using a rigorous approach and comprehensive search strategy, we may have missed some publications. Additionally, we cannot exclude the potential for publication bias.55 The studies included in this review had methodological limitations. Most were descriptive and did not consider potential confounders in the analysis. Five studies were of ecological design, measuring indigenous status at the area level, and therefore were potentially subject to the ecological fallacy.3 ,49–52 A number of studies did not present CIs, making it impossible to judge the precision of the estimates. Fluctuations over time are a general problem in the analysis of small populations and rare events, and the CIs for risk estimates presented in some of the studies were very wide. Due to the heterogeneity among studies, we could not pool the findings from the different studies included in the review.
Finally, incomplete recording of indigenous status in hospital and death records is a recognised issue that can lead to underestimation of injury rates in indigenous children.56–59 A study from the USA that reviewed the quality of recording of ethnicity in mortality and population data found that American Indian and Native American status might be underestimated by 20.6% in population rates.58 An Australian study reported that completeness of recording of Aboriginal status in hospital records across different states in Australia ranged from 45% to 98% with 80% completeness being considered acceptable for the purpose of data analysis.58 Changes and improvements in recording of indigenous status over time, as well as algorithms used to enhance the recording of indigenous status across linked health records will also influence results.60 ,61
Explanation of higher rates in indigenous children
It has been well documented that inequalities in health arise from inequalities in society.62 Past policies of colonization and dispossession have led to a cycle of disadvantage, poor education, high unemployment, low income, separation of families and overcrowded living conditions,15 thus contributing to the social and health inequalities in indigenous communities.40 ,63 Low socioeconomic status increases the risk of childhood injuries,64 and three studies in this review26 ,30 ,41 demonstrated its contribution to the higher burden of injuries in indigenous children. The underlying mechanism may be a higher exposure to a wider range of hazards in the living environment, and lack of means of protection.64 A large proportion of indigenous people live in remote areas, and remoteness, in turn, has been linked with higher rates of injuries.65 ,66 This has been attributed to greater exposure to risk factors, in particular, for transport-related injuries, and reduced access to and lower quality of healthcare in remote areas.54 Higher rates of transport injuries have been explained by longer travelling distances, poorer quality roads, driver fatigue, failure to use seatbelts, alcohol and drug use, overcrowding of cars, unsafe cars and travelling at higher speeds.11 ,15 ,65 ,67–69 Road safety measures might also be less vigorously enforced in remote areas,4 and the autonomous legal status of reservations might lead to different road safety laws and less stringent law enforcement.2 ,40
Measures for prevention
Recommendations for measures to prevent injuries among indigenous children are of particular importance for health policy. It is notable that successful prevention measures have been implemented at a population level for some of the injuries with the largest reported inequalities—transport, drowning, burns and poisoning. Some of the means by which this has been achieved include implementing legislation and raising awareness on use of child passenger restraints and booster seats, fencing of swimming pools, installation of smoke alarms, regulation of hot water temperature, and ensuring safe storage of medicine and cleaning products.70–75
However, most studies in this review were descriptive and made only general recommendations because they did not identify risk factors unique to indigenous communities. The most common suggestions for prevention across all studies were to initiate further studies to better identify risk factors and barriers to, and attitudes towards, safety measures in indigenous communities, and to design prevention programmes that are culturally acceptable, and specifically reach indigenous communities. Further recommendations were to target injury types with the largest inequalities, to improve access to healthcare in remote areas, to provide better information on the epidemiology of injuries to indigenous communities, and to raise awareness of and to enforce prevention measures that have proven successful at the population level. However, traditional injury prevention programmes may not be appropriate for indigenous people for a variety of reasons.15 They may be too limiting and rigid and not take sufficiently into consideration the local conditions, culture and social structures, and may not be suitable for indigenous service providers with limited resources.15
To successfully tackle inequalities, injury prevention strategies should account for these factors and should also take a cross-sectoral approach that addresses the underlying wider social and environmental determinant of indigenous ill-health.11 ,15 Based on the work of the WHO Commission on Social Determinants of Health (CSDH) it has been recommended to primarily focus on six domains to improve indigenous health: early child development, education and skills development, employment and working conditions, minimum income for healthy living, sustainable communities, and a social-determinants approach to prevention.62
Recommendations for further research
The studies identified in this review offered only limited insight into the reasons for the higher unintentional injury rates among indigenous children. The ability to link and analyse routinely collected administrative datasets is ever increasing, so future research should draw upon a wider set of data to include a range of covariates in the analysis and so improve the ascertainment of indigenous status. The potential impact of uncertainties in recording indigenous status in routine datasets should be explored in sensitivity analyses.76
The application of sophisticated analytical approaches, such as multilevel modelling, could be used to investigate the contribution of individual-level versus area-level factors to inequalities in unintentional injuries between indigenous and non-indigenous children. Such methods have been applied to explore the influence of area and socioeconomic status on child injuries77 and of area and individual factors road traffic crashes in Australian Aboriginal people.78 To tackle the inequalities identified in this review, future research needs to extend beyond the identification of risk factors, and should look at the modifiable underlying mechanisms and how these can be addressed. A combination of quantitative and qualitative methods might offer better insight into underlying reasons, beliefs and cultural aspects that contribute to differences in unintentional injury rates. A mixed-method approach could also help to explore more distal determinants of indigenous health, such as government policy. Importantly, future research in this area must embody principles of indigenous community engagement and ownership, to ensure the ethical integrity of the research and the appropriateness of potential solutions that it suggests.
Key message
Indigenous children experience a significantly higher burden of morbidity and mortality from unintentional injuries across different indigenous communities worldwide, but there is limited evidence from quantitative studies to illuminate the underlying risk factors and causes of these inequalities. Given that most of these injuries are highly preventable,1 there should be substantial potential to improve indigenous child health and to reduce health inequalities. More research into the risk factors for unintentional injuries in indigenous children is needed to guide policy and programme development that will lead to reductions in these health inequalities.
What is already known on the subject
-
Unintentional injuries are a leading cause of child morbidity and mortality.
-
Indigenous children are disproportionally affected by unintentional injuries.
What this study adds
-
The leading causes of inequalities in unintentional injuries between indigenous and non-indigenous children were burns, poisoning and transport injuries.
-
Little progress in reducing these inequalities has been achieved in the last 35 years.
-
There is limited evidence from quantitative studies to illuminate the underlying risk factors and causes of these inequalities.
Acknowledgments
The authors would like to thank Geoff Lattimore of the University of Western Sydney for his initial support in developing the search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All the authors contributed to the conception and design of the study, interpretation of data and drafting or critical revision of the manuscript. HM led and contributed to all stages of the systematic review and drafted the manuscript. LJ, KF and RI provided methodological input at the different stages of the systematic review. All authors contributed to the critical revision of the manuscript. All authors gave final approval of the version to be published.
-
Funding HM was supported by an NHMRC capacity building grant (#573122) and a University of Sydney/University of Western Sydney Cross Cultural Public Health Research Award. KF was supported by an NHMRC Early Career Fellowship (#1016475) and an NHMRC capacity building grant (#573122). RI was supported by fellowship funding from the NHMRC (#APP1031781).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Additional, detailed information on search strategy and results are provided in the online supplements.