Seasonality of Suicidal Behavior

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Potential Environmental Mediators
3.1. Bioclimatic Factors
3.2. Geographic Location
3.3. Allergens
3.4. Viruses
3.5. Pollutants
4. Clinical Determinants: Effect of Morbidity

5. Demographic Variables
5.1. Age
5.2. Gender
5.3. Month of Birth
5.4. Socioeconomic Factors
6. Suicide Methods
7. Conclusions

Acknowledgments
Conflict of Interest
References and Notes
- Ajdacic-Gross, V.; Wang, J.; Bopp, M.; Eich, D.; Rössler, W.; Gutzwiller, F. Are seasonalities in suicide dependent on suicide methods? A reappraisal. Soc. Sci. Med. 2003, 57, 1173–1181. [Google Scholar]
- Maes, M. Seasonality in violent suicide but not in nonviolent suicide or homicide. Am. J. Psychiatry 1993, 150, 1380–1385. [Google Scholar]
- Ajdacic-Gross, V.; Bopp, M.; Ring, M.; Gutzwiller, F.; Rossler, W. Seasonality in suicide—A review and search of new concepts for explaining the heterogeneous phenomena. Soc. Sci. Med. 2010, 71, 657–666. [Google Scholar]
- Chew, K.S.Y.; McCleary, R. The spring peak in suicides: A cross-national analysis. Soc. Sci. Med. 1995, 40, 223–230. [Google Scholar]
- Qin, P. Suicide risk in relation to level of urbanicity—A population-based linkage study. Int. J. Epidemiol. 2005, 34, 846–852. [Google Scholar]
- Kung, H.C.; Pearson, J.L.; Liu, X. Risk factors for male and female suicide decedents ages 15–64 in the United States. Soc. Psych. Psych. Epidemiol. 2003, 38, 419. [Google Scholar]
- Rock, D.; Greenberg, D.; Hallmayer, J. Season-of-birth as a risk factor for the seasonality of suicidal behaviour. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 98–105. [Google Scholar]
- Lorant, V. A European comparative study of marital status and socio-economic inequalities in suicide. Soc. Sci. Med. 2005, 60, 2431–2441. [Google Scholar]
- Smith, J.C.; Mercy, J.A.; Conn, J.M. Marital status and the risk of suicide. Am. J. Public Health 1988, 78, 78–80. [Google Scholar]
- Preti, A. The influence of seasonal change on suicidal behaviour in Italy. J. Affect. Disord. 1997, 44, 123–130. [Google Scholar]
- Souêtre, E. Seasonality of suicides: Environmental, sociological and biological covariations. J. Affect. Disord. 1987, 13, 215–225. [Google Scholar]
- Qin, P.; Agerbo, E.; Mortensen, P.B. Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: A National register-based study of all suicides in Denmark, 1981–1997. Am. J. Psychiatry 2003, 160, 765–772. [Google Scholar] [CrossRef]
- Qin, P.; Mortensen, P.B.; Waltoft, B.L.; Postolache, T.T. Allergy is associated with suicide completion with a possible mediating role of mood disorder—A population-based study. Allergy 2011, 66, 658–664. [Google Scholar]
- Töro, K. Relationship between suicidal cases and meteorological conditions. J. Forensic Leg. Med. 2009, 16, 277–279. [Google Scholar]
- Kim, Y.; Kim, H.; Kim, D.-S. Association between daily environmental temperature and suicide mortality in Korea (2001–2005). Psychiatry Res. 2011, 186, 390–396. [Google Scholar]
- Kim, C.; Jung, S.H.; Kang, D.R.; Kim, H.C.; Moon, K.T.; Hur, N.W.; Shin, D.C.; Suh, I. Ambient particulate matter as a risk factor for suicide. Am. J. Psychiatry 2010, 167, 1100–1107. [Google Scholar]
- Okusaga, O.; Yolken, R.H.; Langenberg, P.; Lapidus, M.; Arling, T.A.; Dickerson, F.B.; Scrandis, D.A.; Severance, E.; Cabassa, J.A.; Balis, T.; Postolache, T.T. Association of seropositivity for influenza and coronaviruses with history of mood disorders and suicide attempts. J. Affect. Disord. 2011, 130, 220–225. [Google Scholar]
- Lee, H.-C.; Lin, H.-C.; Tsai, S.-Y.; Li, C.-Y.; Chen, C.-C.; Huang, C.-C. Suicide rates and the association with climate: A population-based study. J. Affect. Disord. 2006, 92, 221–226. [Google Scholar]
- Postolache, T.T.; Stiller, J.W.; Herrell, R.; Goldstein, M.A.; Shreeram, S.S.; Zebrak, R.; Thrower, C.M.; Volkov, J.; No, M.J.; Volkov, I.; Rohan, K.J.; Redditt, J.; Parmar, M.; Mohyuddin, F.; Olsen, C.; Moca, M.; Tonelli, L.H.; Merikangas, K.; Komarow, H.D. Tree pollen peaks are associated with increased nonviolent suicide in women. Mol. Psychiatry 2004, 10, 232–235. [Google Scholar]
- Partonen, T.; Haukka, J.; Viilo, K.; Hakko, H.; Pirkola, S.; Isometsä, E.; Lönnqvist, J.; Särkioja, T.; Väisänen, E.; Räsänen, P. Cyclic time patterns of death from suicide in northern Finland. J. Affect. Disord. 2004, 78, 11–19. [Google Scholar]
- Vyssoki, B.; Praschak-Rieder, N.; Sonneck, G.; Blüml, V.; Willeit, M.; Kasper, S.; Kapusta, N.D. Effects of sunshine on suicide rates. Comp. Psychiatry 2012, in press. [Google Scholar]
- Souêtre, E. Influence of environmental factors on suicidal behavior. Psychiatry Res. 1990, 32, 253–263. [Google Scholar]
- Altamura, C. Seasonal and circadian rhythms in suicide in Cagliari, Italy. J. Affect. Disord. 1999, 53, 77–85. [Google Scholar]
- Rock, D. Increasing seasonality of suicide in Australia 1970–1999. Psychiatry Res. 2003, 120, 43–51. [Google Scholar]
- Volpe, F.M.; Tavares, A.; Del Porto, J.A. Seasonality of three dimensions of mania: Psychosis, aggression and suicidality. J. Affect. Disord. 2008, 108, 95–100. [Google Scholar]
- Deisenhammer, E.A.; Kemmler, G.; Parson, P. Association of meteorological factors with suicide. Acta Psychiatr. Scand. 2003, 108, 455–459. [Google Scholar]
- Lambert, G.; Reid, C.; Kaye, D.; Jennings, G.; Esler, M. Increased suicide rate in the middle-aged and its association with hours of sunlight. Am. J. Psychiatry 2003, 160, 793–795. [Google Scholar]
- Ajdacic-Gross, V.; Lauber, C.; Sansossio, R.; Bopp, M.; Eich, D.; Gostynski, M.; Gutzwiller, F.; Rössler, W. Seasonal associations between weather conditions and suicide—Evidence against a classic hypothesis. Am. J. Epidemiol. 2007, 165, 561–569. [Google Scholar]
- Dixon, P.G. Effects of temperature variation on suicide in five U.S. counties, 1991–2001. Int. J. Biometeorol. 2007, 51, 395–403. [Google Scholar] [CrossRef]
- Nejar, K.A.; Benseñor, I.M.; Lotufo, P.A. Sunshine and suicide at the tropic of Capricorn, São Paulo, Brazil, 1996–2004. Rev. Saude Publica 2007, 41, 1062–1064. [Google Scholar] [CrossRef]
- Maes, M. Synchronized annual rhythms in violent suicide rate, ambient temperature and the light-dark span. Acta Psychiatr. Scand. 1994, 90, 391–396. [Google Scholar]
- Petridou, E.; Papadopoulos, F.; Frangakis, C.; Skalkidou, A.; Trichopoulos, D. A role of sunshine in the triggering of suicide. Epidemiology 2002, 13, 106–109. [Google Scholar]
- Meares, R. A sex difference in the seasonal variation of suicide rate: A single cycle for men, two cycles for women. Br. J. Psychiatry 1981, 138, 321–325. [Google Scholar]
- Micciolo, R. Seasonal variation in suicide: Is there a sex difference? Psychol. Med. 1989, 19, 199–203. [Google Scholar] [CrossRef]
- Koskinen, O.; Pukkila, K.; Hakko, H.; Tiihonen, J.; Väisänen, E.; Särkioja, T.; Räsänen, P. Is occupation relevant in suicide? J. Affect. Disord. 2002, 70, 197–203. [Google Scholar] [CrossRef]
- Hiltunen, L.; Suominen, K.; Lonnqvist, J.; Partonen, T. Relationship between daylength and suicide in Finland. J. Circadian Rhythms 2011, 9, 10:1–10:12. [Google Scholar]
- Bjorksten, K.; Kripke, D.; Bjerregaard, P. Accentuation of suicides but not homicides with rising latitudes of Greenland in the sunny months. BMC Psychiatry 2009, 9. [Google Scholar]
- Ruuhela, R.; Hiltunen, L.; Venalainen, A.; Pirinen, P.; Partonen, T. Climate impact on suicide rates in Finland from 1971 to 2003. Int. J. Biometeorol. 2009, 53, 167–175. [Google Scholar]
- Hakko, H. Seasonal variation in suicide occurrence in Finland. Acta Psychiatr. Scand. 1998, 98, 92–97. [Google Scholar]
- Näyhä, S. Autumn incidence of suicides re-examined: Data from Finland by sex, age and occupation. Br. J. Psychiatry 1982, 141, 512–517. [Google Scholar]
- Räsänen, P.; Hakko, H.; Jokelainen, J.; Tiihonen, J. Seasonal variation in specific methods of suicide: A national register study of 20234 Finnish people. J. Affect. Disord. 2002, 71, 51–59. [Google Scholar]
- Papadopoulos, F.C.; Frangakis, C.E.; Skalkidou, A.; Petridou, E.; Stevens, R.G.; Trichopoulos, D. Exploring lag and duration effect of sunshine in triggering suicide. J. Affect. Disord. 2005, 88, 287–297. [Google Scholar]
- Lin, H.C.; Chen, C.S.; Xirasagar, S.; Lee, H.C. Seasonality and climatic associations with violent and nonviolent suicide: A population-based study. Neuropsychobiology 2008, 57, 32–37. [Google Scholar]
- Flisher, A.J.; Parry, C.D.H.; Bradshaw, D.; Juritz, J.M. Seasonal variation of suicide in South Africa. Psychiatry Res. 1997, 66, 13–22. [Google Scholar]
- Rocchi, M.B.L.; Sisti, D.; Miotto, P.; Preti, A. Seasonality of suicide: Relationship with the reason for suicide. Neuropsychobiology 2007, 56, 86–92. [Google Scholar]
- Oravecz, R.; Rocchi, M.B.L.; Sisti, D.; Zorko, M.; Marusic, A.; Preti, A. Changes in the seasonality of suicides over time in Slovenia, 1971 to 2002. J. Affect. Disord. 2006, 95, 135–140. [Google Scholar]
- Preti, A.; Miotto, P. Seasonality in suicides: The influence of suicide method, gender and age on suicide distribution in Italy. Psychiatry Res. 1998, 81, 219–231. [Google Scholar]
- Christodoulou, C.; Papadopoulos, I.N.; Douzenis, A.; Kanakaris, N.; Leukidis, C.; Gournellis, R.; Vlachos, K.; Papadopoulos, F.C.; Lykouras, L. Seasonality of violent suicides in the Athens greater area. Suicide Life Threat. Behav. 2009, 39, 321–331. [Google Scholar]
- Nakaji, S.; Parodi, S.; Fontana, V.; Umeda, T.; Suzuki, K.; Sakamoto, J.; Fukuda, S.; Wada, S.; Sugawara, K. Seasonal changes in mortality rates from main causes of death in Japan. Eur. J. Epidemiol. 2004, 19, 905–913. [Google Scholar]
- Ho, T.P.; Chao, A.; Yip, P. Seasonal variation in suicides re-examined: No sex difference in Hong Kong and Taiwan. Acta Psychiatr. Scand. 1997, 95, 26–31. [Google Scholar]
- Tonelli, L.H.; Katz, M.; Kovacsics, C.E.; Gould, T.D.; Joppy, B.; Hoshino, A.; Hoffman, G.; Komarow, H.; Postolache, T.T. Allergic rhinitis induces anxiety-like behavior and altered social interaction in rodents. Brain Behav. Immun. 2009, 23, 784–793. [Google Scholar]
- Tonelli, L.H.; Hoshino, A.; Katz, M.; Postolache, T.T. Acute stress promotes aggressive-like behavior in rats made allergic to tree pollen. Int. J. Child. Health Hum. Dev. 2008, 1, 305–312. [Google Scholar]
- Tonelli, L.H.; Stiller, J.; Rujescu, D.; Giegling, I.; Schneider, B.; Maurer, K.; Schnabel, A.; Möller, H.J.; Chen, H.H.; Postolache, T.T. Elevated cytokine expression in the orbitofrontal cortex of victims of suicide. Acta Psychiatr. Scand. 2008, 117, 198–206. [Google Scholar]
- Manalai, P.; Hamilton, R.G.; Langenberg, P.; Kosisky, S.E.; Lapidus, M.; Sleemi, A.; Scrandis, D.; Cabassa, J.A.; Rogers, C.A.; Regenold, W.T.; Dickerson, F.; Vittone, B.J.; Guzman, A.; Balis, T.; Postolache, T.T. Pollen-specific Immunoglobulin E positivity is associated with worsening of depression scores in bipolar patients during high pollen season. Bipolar Disord. 2012, in press. [Google Scholar]
- Keiser, O.; Spoerri, A.; Brinkhof, M.W.; Hasse, B.; Gayet-Ageron, A.; Tissot, F.; Christen, A.; Battegay, M.; Schmid, P.; Bernasconi, E.; Egger, M. Suicide in HIV-infected individuals and the general population in Switzerland, 1988–2008. Am. J. Psychiatry 2010, 167, 143–150. [Google Scholar]
- Strahilevitz, M.; Strahilevitz, A.; Miller, J.E. Air pollutants and the admission rate of psychiatric patients. Am. J. Psychiatry 1979, 136, 205–207. [Google Scholar]
- Szyszkowicz, M. Air pollution and emergency department visits for depression in Edmonton, Canada. Int. J. Occup. Med. Environ. Health 2007, 20, 241–245. [Google Scholar]
- Henriksson, M.M. Mental disorders and comorbidity in suicide. Am. J. Psychiatr. 1993, 150, 935–940. [Google Scholar]
- Valtonen, H.; Suominen, K.; Partonen, T.; Ostamo, A.; Lonnqvist, J. Time patterns of attempted suicide. J. Affect. Disord. 2006, 90, 201–207. [Google Scholar]
- Haukka, J.; Suominen, K.; Partonen, T.; Lonnqvist, J. Determinants and outcomes of serious attempted suicide: A nationwide study in Finland, 1996–2003. Am. J. Epidemiol. 2008, 167, 1155–1163. [Google Scholar]
- Reutfors, J.; Ösby, U.; Ekbom, A.; Nordström, P.; Jokinen, J.; Papadopoulos, F.C. Seasonality of suicide in Sweden: Relationship with psychiatric disorder. J. Affect. Disord. 2009, 119, 59–65. [Google Scholar] [CrossRef]
- Brådvik, L.; Berglund, M. Seasonal distribution of suicide in alcoholism. Acta Psychiatr. Scand. 2002, 106, 299–302. [Google Scholar]
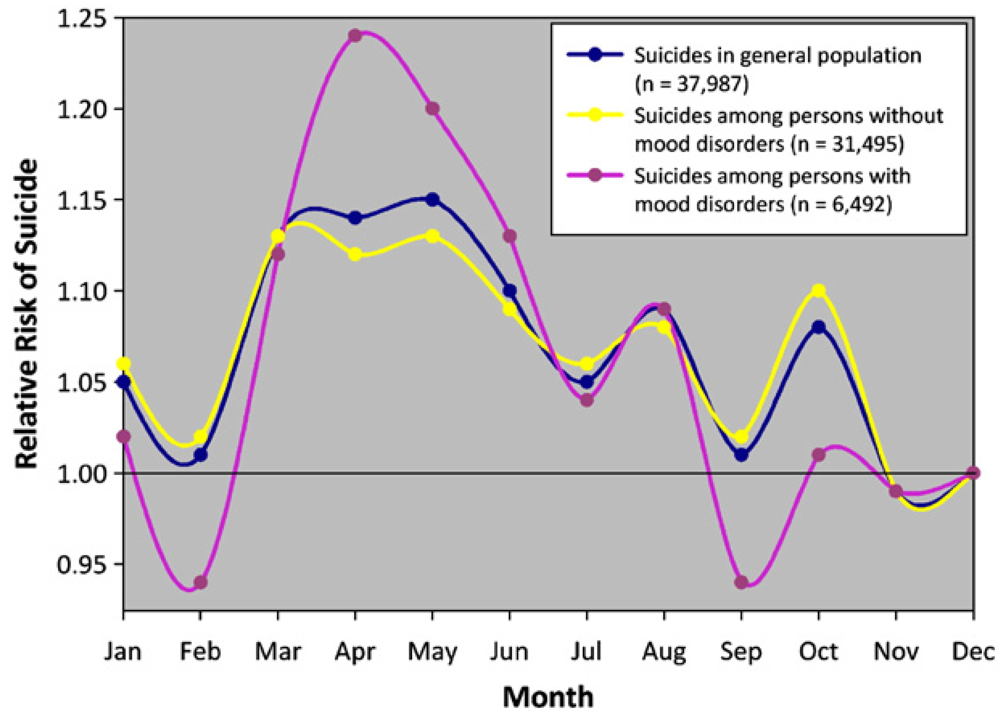
- Postolache, T.T.; Mortensen, P.B.; Tonelli, L.H.; Jiao, X.; Frangakis, C.; Soriano, J.J.; Qin, P. Seasonal spring peaks of suicide in victims with and without prior history of hospitalization for mood disorders. J. Affect. Disord. 2010, 121, 88–93. [Google Scholar]
- Kim, C.D.; Lesage, A.D.; Seguin, M.; Chawky, N.; Vanier, C.; Lipp, O.; Turecki, G. Seasonal differences in psychopathology of male suicide completers. Comp. Psychiatry 2004, 45, 333–339. [Google Scholar]
- Timonen, M.; Viilo, K.; Hakko, H.; Särkioja, T.; Meyer-Rochow, V.B.; Väisänen, E.; Räsänen, P. Is seasonality of suicides stronger in victims with hospital-treated atopic disorders? Psychiatry Res. 2004, 126, 167–175. [Google Scholar] [CrossRef]
- Lahti, A.; Räsänen, P.; Karvonen, K.; Särkioja, T.; Meyer-Rochow, V.B.; Hakko, H. Autumn peak in shooting suicides of children and adolescents from Northern Finland. Neuropsychobiology 2006, 54, 140–146. [Google Scholar]
- McCleary, R.; Chew, K.S.; Hellsten, J.J.; Flynn-Bransford, M. Age- and sex-specific cycles in United States suicides, 1973 to 1985. Am. J. Public Health 1991, 81, 1494–1497. [Google Scholar]
- Preti, A.; Miotto, P.; Coppi, M.D. Season and suicide: Recent findings from Italy. Crisis 2000, 21, 59–70. [Google Scholar]
- Meares, R.; Mendelsohn, F.A.; Milgrom-Friedman, J. A sex difference in the seasonal variation of suicide rate: a single cycle for men, two cycles for women. Br. J. Psychiatry 1981, 138, 321–325. [Google Scholar]
- Sebestyen, B.; Rihmer, Z.; Balint, L.; Szokontor, N.; Gonda, X.; Gyarmati, B.; Bodecs, T.; Sandor, J. Gender differences in antidepressant use-related seasonality change in suicide mortality in Hungary, 1998–2006. World J. Biol. Psychiatry 2010, 11, 579–585. [Google Scholar]
- Mergl, R.; Havers, I.; Althaus, D.; Rihmer, Z.; Schmidtke, A.; Lehfeld, H.; Niklewski, G.; Hegerl, U. Seasonality of suicide attempts: Association with gender. Eur. Arch. Psychiatry Clin. Neurosci. 2010, 260, 393–400. [Google Scholar]
- Barker, A.; Hawton, K.; Fagg, J.; Jennison, C. Seasonal and weather factors in parasuicide. Br. J. Psychiatry 1994, 165, 375–380. [Google Scholar]
- Masterton, G. Monthly and seasonal variation in parasuicide. A sex difference. Br. J. Psychiatry 1991, 158, 155–157. [Google Scholar] [CrossRef]
- Jessen, G.; Andersen, K.; Arensman, E.; Bille-Brahe, U.; Crepet, P.; De Leo, D.; Hawton, K.; Haring, C.; Hjelmeland, H.; Michel, K.; Ostamo, A.; Salander-Renberg, E.; Schmidtke, A.; Temesvary, B.; Wasserman, D. Temporal fluctuations and seasonality in attempted suicide in Europe. Arch. Suicide Res. 1999, 5, 57–69. [Google Scholar]
- Kessler, R.C.; Berglund, P.; Borges, G.; Nock, M.; Wang, P.S. Trends in suicide ideation, plans, gestures, and attempts in the United States, 1990–1992 to 2001–2003. JAMA 2005, 293, 2487–2495. [Google Scholar]
- Dome, P.; Kapitany, B.; Ignits, G.; Rihmer, Z. Season of birth is significantly associated with the risk of completed suicide. Biol. Psychiatry 2010, 68, 148–155. [Google Scholar]
- Chotai, J.; Forsgren, T.; Nilsson, L.-G.; Adolfsson, R. Season of birth variations in the temperament and character inventory of personality in a general population. Neuropsychobiology 2001, 44, 19–26. [Google Scholar]
- Chotai, J.; Salander Renberg, E. Season of birth variations in suicide methods in relation to any history of psychiatric contacts support an independent suicidality trait. J. Affect. Disord. 2002, 69, 69–81. [Google Scholar]
- Micciolo, R.; Williams, P.; Zimmermann-Tansella, C.; Tansella, M. Geographical and urban-rural variation in the seasonality of suicide: Some further evidence. J. Affect. Disord. 1991, 21, 39–43. [Google Scholar]
- Christodoulou, C.; Douzenis, A.; Papadopoulos, F.; Papadopoulou, A.; Bouras, G.; Gournellis, R.; Lykouras, L. Suicide and seasonality. Acta Psychiatr. Scand. 2012, 125, 127–146. [Google Scholar]
- Ajdacic-Gross, V.; Bopp, M.; Sansossio, R.; Lauber, C.; Gostynski, M.; Eich, D.; Gutzwiller, F.; Rössler, W. Diversity and change in suicide seasonality over 125 years. J. Epidemiol. Community Health 2005, 59, 967–972. [Google Scholar] [Green Version]
- Kposowa, A.J.; McElvain, J.P.; Breault, K.D. Immigration and suicide: The role of marital status, duration of residence, and social integration. Arch. Suicide Res. 2008, 12, 82–92. [Google Scholar] [CrossRef]
- Cheng, Q.; Chen, F.; Yip, P.S. The Foxconn suicides and their media prominence: Is the Werther Effect applicable in China? BMC Public Health 2011, 11. [Google Scholar]
- Li, X.; Stanton, B.; Fang, X.; Xiong, Q.; Yu, S.; Lin, D.; Hong, Y.; Zhang, L.; Chen, X.; Wang, B. Mental health symptoms among rural-to-urban migrants in China: A comparison with their urban and rural counterparts. World Health Popul. 2009, 11, 24–38. [Google Scholar]
- Lin, D.; Li, X.; Wang, B.; Hong, Y.; Fang, X.; Qin, X.; Stanton, B. Discrimination, perceived social inequity, and mental health among rural-to-urban migrants in China. Community Ment. Health J. 2011, 47, 171–180. [Google Scholar] [CrossRef]
- Lester, D. Seasonal variation in suicide and the methods used. Percept. Mot. Skills 1999, 89, 160–165. [Google Scholar]
- Kalediene, R.; Starkuviene, S.; Petrauskiene, J. Seasonal patterns of suicides over the period of socio-economic transition in Lithuania. BMC Public Health 2006, 6. [Google Scholar]
- Hakko, H.; Räsänen, P.; Tiihonen, J. Secular trends in the rates and seasonality of violent and nonviolent suicide occurrences in Finland during 1980–95. J. Affect. Disord. 1998, 50, 49–54. [Google Scholar]
- Linkowski, P.; Martin, F.; De Maertelaer, V. Effect of some climatic factors on violent and non-violent suicides in Belgium. J. Affect. Disord. 1992, 25, 161–166. [Google Scholar]
- Björkstén, K.S.; Bjerregaard, P.; Kripke, D.F. Suicides in the midnight sun—A study of seasonality in suicides in West Greenland. Psychiatry Res. 2005, 133, 205–213. [Google Scholar]
- Salib, E. Elderly suicide and weather conditions: Is there a link? Int. J. Geriatr. Psychiatry 1997, 12, 937–941. [Google Scholar] [CrossRef]
- Yip, P.S.; Chao, A.; Ho, T.P. A re-examination of seasonal variation in suicides in Australia and New Zealand. J. Affect. Disord. 1998, 47, 141–150. [Google Scholar]
- Lester, D.; Frank, M.L. Seasonal variation in suicide rates in the United States. J. Clin. Psychiatry 1988, 49. [Google Scholar] [PubMed]
- Lester, D.; Frank, M. Sex differences in the seasonal distribution of suicides. Br. J. Psychiatry 1988, 153, 115–117. [Google Scholar]
- Coccaro, E.F. Central serotonin and impulsive aggression. Br. J. Psychiatry 1989, 8, 52–62. [Google Scholar]
- Maes, M.; Scharpe, S.; Verkerk, R.; D'Hondt, P.; Peeters, D.; Cosyns, P.; Thompson, P.; Meyer, F.D.; Wauters, A.; Neels, H. Seasonal variation in plasma L-Tryptophan availability in healthy volunteers: Relationships to violent suicide occurrence. Arch. Gen. Psychiatry 1995, 52, 937–946. [Google Scholar]
- Lambert, G.W.; Reid, C.; Kaye, D.M.; Jennings, G.L.; Esler, M.D. Effect of sunlight and season on serotonin turnover in the brain. Lancet 2002, 360, 1840–1842. [Google Scholar]
- Woo, J.M.; Gibbons, R.D.; Rogers, C.A.; Qin, P.; Kim, J.B.; Roberts, D.W.; Noh, E.S.; Mann, J.J.; Postolache, T.T. Pollen counts and suicide rates. Association not replicated. Acta Psychiatr. Scand. 2012, 125, 168–175. [Google Scholar] [CrossRef]
- Yip, P.; Chao, A.; Chiu, C. Seasonal variation in suicides: Diminished or vanished. Br. J. Psychiatry 2000, 177, 366–369. [Google Scholar]
- Yip, P.S.F.; Yang, K.C.T. A comparison of seasonal variation between suicide deaths and attempts in Hong Kong SAR. J. Affect. Disord. 2004, 81, 251–257. [Google Scholar] [Green Version]
- Rihmer, Z.; Rutz, W.; Pihlgren, H.; Pestality, P. Decreasing tendency of seasonality in suicide may indicate lowering rate of depressive suicides in the population. Psychiatry Res. 1998, 81, 233–240. [Google Scholar]
- Yip, P.S.F.; Yang, K.C.T.; Qin, P. Seasonality of suicides with and without psychiatric illness in Denmark. J. Affect. Disord. 2006, 96, 117–121. [Google Scholar]
- Bridges, F.S.; Yip, P.S.F.; Yang, K.C.T. Seasonal changes in suicide in the united states, 1971 to 2000. Percept. Mot. Skills 2005, 100, 920–924. [Google Scholar]
- Casey, P.; Gemmell, I.; Hiroeh, U.; Fulwood, C. Seasonal and socio-demographic predictors of suicide in Ireland: A 22 year study. J. Affect. Disord. 2011. [Google Scholar]
- Corcoran, P.; Reilly, M.; Salim, A.; Brennan, A.; Keeley, H.S.; Perry, I.J. Temporal variation in Irish suicide rates. Suicide Life Threat. Behav. 2004, 34, 429–438. [Google Scholar]
- Schreiber, G.; Dycian, A.; Kaplan, Z.; Bleich, A. A unique monthly distribution of suicide and parasuicide through firearms among Israeli soldiers. Acta Psychiatr. Scand. 1993, 87, 110–113. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Woo, J.-M.; Okusaga, O.; Postolache, T.T. Seasonality of Suicidal Behavior. Int. J. Environ. Res. Public Health 2012, 9, 531-547. https://doi.org/10.3390/ijerph9020531
Woo J-M, Okusaga O, Postolache TT. Seasonality of Suicidal Behavior. International Journal of Environmental Research and Public Health. 2012; 9(2):531-547. https://doi.org/10.3390/ijerph9020531
Chicago/Turabian StyleWoo, Jong-Min, Olaoluwa Okusaga, and Teodor T. Postolache. 2012. "Seasonality of Suicidal Behavior" International Journal of Environmental Research and Public Health 9, no. 2: 531-547. https://doi.org/10.3390/ijerph9020531