Association of the Joint Effect of Menopause and Hormone Replacement Therapy and Cancer in African American Women: The Jackson Heart Study


 ,
,
Abstract
:1. Introduction
2. Study Design and Methods
Outcome Measures
Reproductive Measures
Demographic and Socioeconomic Measures
Clinical Risk Factors
Behavioral Risk Factors
Data Analytic Plan
3. Results
4. Conclusions
Perspective
Acknowledgments
References
- National Center for Health Statistics. Fast Facts from A-Z. Available online: http://www.cdc.gov/nchs (accessed on 15 June 2010).
- McCullough, ML; Feigelson, HS; Diver, WR; Patel, AV; Thun, M; Calle, EE. Risk factors for fatal breast cancer in African-American women and White women in a large us prospective cohort. Am. J. Epidemiol 2005, 10, 1093. [Google Scholar]
- Schootman, M; Lian, M; Deshpande, AD; Baker, EA; Pruitt, SL; Aft, R; Jeffe, DB. Temporal trends in geographic disparities in small-area breast cancer. Cancer 2009, 11, 5329–5338. [Google Scholar]
- Komenaka, IK; Martinez, ME; Pennington, RE, Jr; Hsu, C; Clare, SE; Thompson, PA; Murphy, C; Zork, NM; Goulet, RJ, Jr. Underinsured African-American women have worse breast cancer outcomes than underinsured white women. J. Natl. Cancer Inst. Part B 2010, 102, 1190. [Google Scholar]
- Albain, KS; Unger, JM; Crowley, JJ; Coltman, CA, Jr; Hershman, DL. Racial disparities in cancer survival among randomized clinical trials patients of the Southwest Oncology Group. J. Natl. Cancer Inst 2009, 10, 984–992. [Google Scholar]
- Taylor, HA, Jr. The Jackson Heart Study: An overview. Ethn. Dis. Part A 2005, 15, 1–3. [Google Scholar]
- Taylor, HA; Wilson, JG; Jones, DW; Sarpong, DF; Srinivasan, A; Garrison, RJ; Nelson, C; Wyatt, SB. Toward resolution of cardiovascular health disparities in African Americans: Design and methods of the Jackson Heart Study. Ethn. Dis. Part B 2005, 15, 4–17. [Google Scholar]
- Fuqua, SR; Wyatt, SB; Sarpong, DF; Henderson, FR; Cunningham, MF; Taylor, HA, Jr. Recruiting African-American research participation in the Jackson Heart Study: Methods, response rates, and sample description. Ethn. Dis 2005, 15, 18–29. [Google Scholar]
- Wilson, JG; Rotimi, CN; Ekunwe, L; Royal, CD; Crump, ME; Wyatt, SB; Steffes, MW; Adeyemo, A; Zhou, J; Taylor, HA, Jr; Jaquish, C. Study design for genetic analysis in the Jackson Heart Study. Ethn. Dis 2005, 15, 30–37. [Google Scholar]
- Carithers, T; Dubbert, PM; Crook, E; Davy, B; Wyatt, SB; Bogle, ML; Taylor, HA, Jr; Tucker, KL. Dietary assessment in African Americans: methods used in the Jackson Heart Study. Ethn. Dis 2005, 15, 18–29. [Google Scholar]
- Dubbert, PM; Carithers, T; Ainsworth, BA; Taylor, HA, Jr; Wilson, G; Wyatt, SB. Physical activity assessment methods in the Jackson Heart Study. Ethn. Dis 2005, 15, 56–61. [Google Scholar]
- Payne, TJ; Wyatt, SB; Mosley, TH; Dubbert, PM; Guiterrez-Mohammed, ML; Calvin, RL; Taylor, HA, Jr; Williams, DR. Sociocultural methods in the Jackson Heart Study: Conceptual and descriptive overview. Ethn. Dis 2005, 15, 38–48. [Google Scholar]
- Carpenter, M; Crow, R; Steffes, M; Rock, W; Heilbraun, J; Evans, G; Skelton, T; Jensen, R; Sarpong, D. Laboratory, reading center, and coordinating center data management methods in the Jackson Heart Study. Am. J. Med. Sci 2004, 328, 131–144. [Google Scholar]
- Baecke, JAH; Burema, J; Fritjers, J. A short questionnaire for the measurement of habitual activity in epidemiological studies. Am. J. Clin. Nutr 1982, 36, 936–942. [Google Scholar]
- Carithers, TC; Talegawker, SA; Rowser, ML; Henry, OR; Dubbert, PM; Bogle, ML; Taylor, HA, Jr; Tucker, KL. Validity and calibration of food frequency questionnaires used with African American adults in the Jackson Heart Study. J. Am. Diet. Assoc 2009, 109, 1184–1193. [Google Scholar]
- Ziegler, RG; Mason, TJ; Stemhagen, A; Hoover, R; Schoesberg, JB; Gridley, G; Virgo, PW; Fraumeni, JR, Jr. Carotenoid Intake, vegetables, and the risk of lung cancer among white men in New Jersey. Am. J. Epidemiol 1986, 123, 1080–1095. [Google Scholar]
- Ziegler, RG. Vegetables, fruits, and carotenoids and the risk of cancer. Am. J. Clin. Nutr 1991, 55, 251–259. [Google Scholar]
- Potischman, N; McCulloch, CE; Byers, T; Nemoto, T; Stubbe, N; Milch, R; Parker, R; Rasmussen, KM; Root, M; Graham, S. Breast cancer and dietary and plasma concentration of carotenoid and vitamin A. Am. J. Clini. Nutr 1990, 52, 909–915. [Google Scholar]
- The Practical Guide: Identification, Evaluation, and Treatment of Overweight Obesity in Adults; NIH Publication No 00-4084; National Institute of Health, National Heart Lung blood Institute, North American Association for the Study of Obesity: Bethesda, MD, USA, 2000.
- Nicholson, WK; Brown, AF; Gathe, J; Grumbach, K; Washington, AE; Perex-stable, EJ. Hormone replacement therapy for African American women: missed opportunities for effective intervention. Menopause 1999, 6, 147–155. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Age (years) | 56 ± 11 |
| BMI, (Kg/m2) | 32.8 ± 7.4 |
| Obesity (%) | 60.3 |
| Education Level (%) | |
| Less than HS | 18.4 |
| High School/GED | 20.6 |
| Greater than HS but less than BA/BS | 27.7 |
| Bachelor Degree or Higher | 33.3 |
| Family Income (%) | |
| Low | 17.3 |
| Lower- Middle | 27.0 |
| Upper Middle | 29.9 |
| Affluent | 25.8 |
| Family History of Cancer (%) | 1,576 (59.8) |
| Total number of pregnancies | 3.5 ± 2.5 |
| Total number of live born children | 3.2 ± 2.2 |
| Menopausal Post (%) | 2,338 (73.7) |
| HRT Use (%) | 710 (22.6) |
| Characteristics | Non-Cancer (n = 3,012) | Cancer (n = 190) | P-Value |
|---|---|---|---|
| Age (years) | 56 ± 11 | 62 ± 11 | <0.0001 |
| BMI, (Kg/m2) | 32.8 ± 7.4 | 31.9 ± 6.9 | 0.0914 |
| Obesity | 60.5 | 56.1 | 0.2331 |
| Education Level | 0.4203 | ||
| Less than HS | 18.40 | 20.53 | |
| High School/GED | 20.59 | 19.47 | |
| Greater than HS but less than BA/BS | 27.68 | 31.58 | |
| Bachelor Degree or Higher | 33.33 | 28.42 | |
| Family Income | 0.7465 | ||
| Low | 17.28 | 19.23 | |
| Lower- Middle | 26.98 | 29.49 | |
| Upper Middle | 29.92 | 26.92 | |
| Affluent | 25.82 | 24.36 | |
| Current Smoking, Yes | 10.33 | 8.47 | 0.4126 |
| Heavy Alcohol Use (%) | 5.71 | 6.52 | 0.8055 |
| Fruit Intake (grams/day) | 1.5 ± 1.1 | 1.5 ± 0.8 | 0.8412 |
| Vegetable Intake (grams/day) | 1.4 ± 0.6 | 1.3 ± 0.5 | 0.0635 |
| % Calories due to Fat | 34.9 ± 7.2 | 34.1 ± 7.0 | 0.1100 |
| Amt. of Fat Intake (grams) | 76.4 ± 47.5 | 69.6 ± 39.2 | 0.0267 |
| Total Dietary Fiber (grams) | 14.7 ± 7.0 | 14.1 ± 5.5 | 0.1489 |
| Beta-Carotene (Mcg) | 3,288 ± 1,545 | 3,190 ± 1,512 | 0.4043 |
| Total Vitamin E (Mg) | 66.1 ± 107.9 | 85.7 ± 121.9 | 0.0349 |
| Vitamin C (Mg) | 188.9 ± 190.2 | 210.7 ± 207.4 | 0.1344 |
| Lycopene (Mcg) | 4,209 ± 4,989 | 3,253 ± 2,921 | < 0.0001 |
| %Calories from Alcohol | 0.5 ± 2.0 | 0.3 ± 1.2 | 0.0291 |
| Post Menopausal (%) | 72.7 | 89.0 | < 0.0001 |
| HRT Use, Yes (%) | 22.8 | 21.3 | 0.6402 |
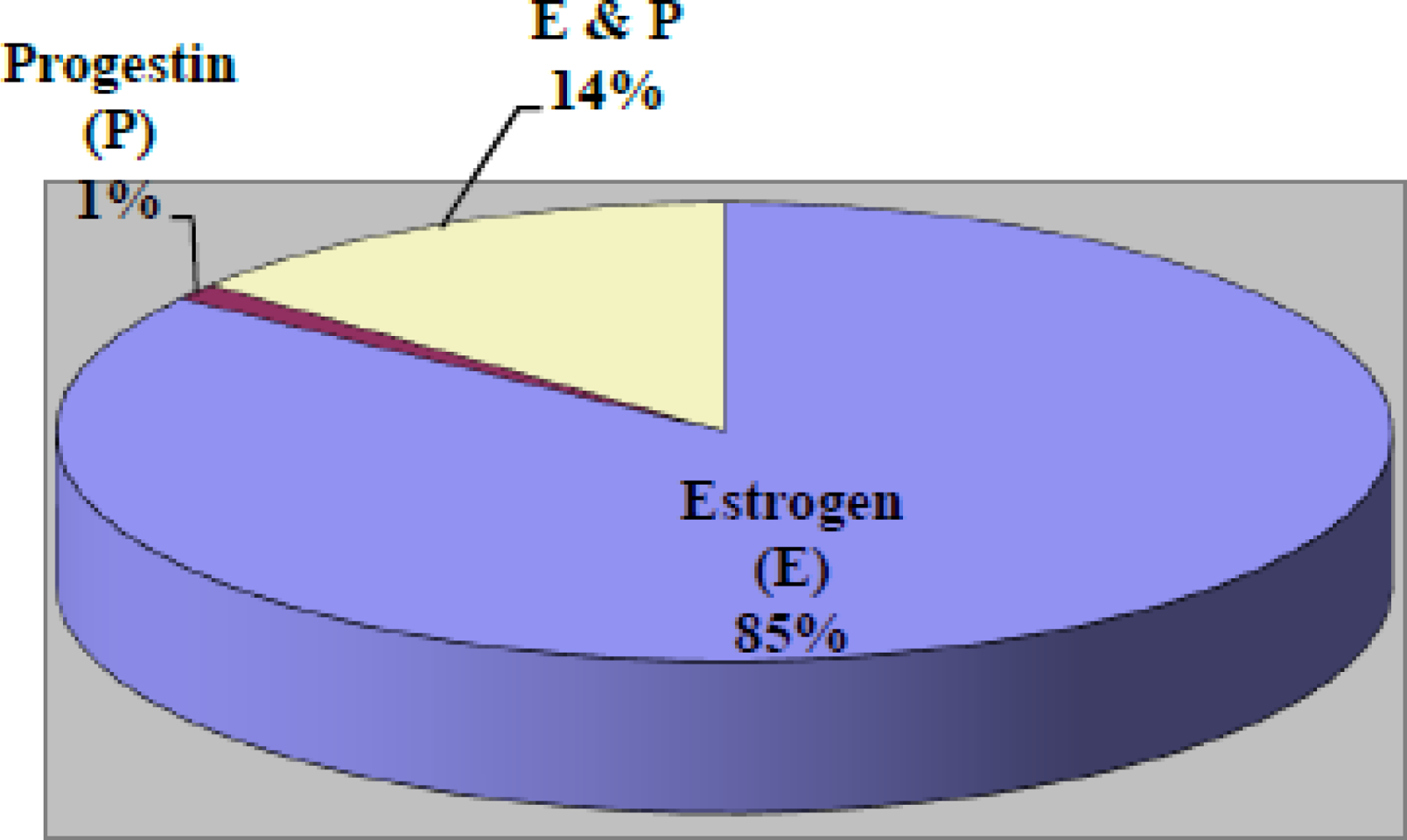
| Types of HRT | 0.6402 | ||
| Estrogen | 74.5 | 67.1 | 0.2987 |
| Progestin | 1.1 | 0.0 | 0.7143 |
| Estrogen & Progestin | 12.6 | 8.2 | 0.1767 |
| Family History of Cancer | 59.0 | 71.7 | 0.0019 |
| Physical Activity Total | 8.1 ± 2.6 | 7.3 ± 2.6 | < 0.0001 |
| Active Living | 2.1 ± 0.8 | 2.0 ± 0.8 | 0.2479 |
| Home and Garden | 2.3 ± 0.6 | 2.2 ± 0.6 | 0.0443 |
| Sport Index | 2.1 ± 1.2 | 2.0 ± 1.2 | 0.1418 |
| Work Index | 2.6 ± 0.7 | 2.6 ± 0.6 | 0.7368 |
| Type Two Diabetes | 20.12 | 27.37 | 0.0196 |
| Hypertension | 66.14 | 73.91 | 0.0300 |
| Prevalent CVD | 9.25 | 12.77 | 0.2331 |
| Age start taking birth control pills | 22 ± 5 | 23 ± 5 | 0.0050 |
| Age stop taking birth control pills | 30 ± 7 | 30 ± 6 | 0.9026 |
| Years you have used birth control | 8 ± 6 | 7 ± 5 | 0.0710 |
| Characteristics | Non-Breast Cancer (n = 3,165) | Breast Cancer (n = 37) | P-Value |
|---|---|---|---|
| Age, years | 56 ± 12 | 63 ± 10 | 0.0012 |
| BMI, (Kg/m2) | 32.8 ± 7.4 | 32.4 ± 6.8 | 0.7548 |
| Obesity | 60.3 | 62.2 | 0.8207 |
| Education Level | 0.9104 | ||
| Less than HS | 18.65 | 16.22 | |
| High School/GED | 20.46 | 21.62 | |
| Greater than HS but less than BA/BS | 27.85 | 32.43 | |
| Bachelor Degree or Higher | 33.05 | 29.73 | |
| Family Income | 0.8961 | ||
| Low | 17.44 | 20.0 | |
| Lower- Middle | 27.30 | 23.33 | |
| Upper Middle | 29.70 | 26.67 | |
| Affluent | 25.57 | 30.0 | |
| Current Smoking, Yes | 10.25 | 2.70 | |
| Heavy Alcohol Use (%) | 5.76 | 0.0 | 0.0707 |
| Fruit Intake (grams/day) | 1.5 ± 1.1 | 1.6 ± 0.7 | 0.3092 |
| Vegetable Intake (grams/day) | 1.4 ± 0.6 | 1.3 ± 0.4 | 0.0776 |
| % Calories due to Fat | 34.9 ± 7.2 | 34.6 ± 7.8 | 0.8336 |
| Amt. of Fat Intake (grams) | 75.8 ± 47.0 | 80.8 ± 47.4 | 0.5305 |
| Total Dietary Fiber (grams) | 14.7 ± 6.9 | 14.8 ± 5.2 | 0.8968 |
| Beta-Carotene (Mcg) | 3286 ± 1544 | 3056 ± 1239 | 0.3799 |
| Total Vitamin E (Mg) | 67.0 ± 108.6 | 74.5 ± 1193.2 | 0.6813 |
| Vitamin C (Mg) | 189.3 ± 190.6 | 227.1 ± 224.9 | 0.2437 |
| Lycopene (Mcg) | 4144 ± 4900 | 3663 ± 2250 | 0.2250 |
| %Calories from Alcohol | 0.5 ± 1.9 | 0.3 ± 1.1 | 0.4515 |
| Post Menopausal (%) | 73.4 | 94.6 | 0.0037 |
| HRT Use, Yes (%) | 22.7 | 13.5 | 0.1853 |
| Types of HRT | |||
| Estrogen | 74.2 | 61.5 | 0.1637 |
| Progestin | 1.0 | 0.0 | 0.3710 |
| Estrogen & Progestin | 12.3 | 0.0 | 0.2732 |
| Family History of Cancer | 59.7 | 65.5 | 0.5269 |
| Physical Activity Total | 8.1 ± 2.6 | 7.7 ± 2.0 | 0.4029 |
| Active Living | 2.1 ± 0.8 | 2.0 ± 0.8 | 0.6252 |
| Home and Garden | 2.3 ± 0.6 | 2.3 ± 0.6 | 0.8008 |
| Sport Index | 2.1 ± 1.2 | 2.0 ± 1.2 | 0.6959 |
| Work Index | 2.6 ± 0.7 | 2.5 ± 0.7 | 0.5325 |
| Type Two Diabetes | 20.54 | 27.78 | 0.2858 |
| Hypertension | 66.56 | 80.56 | 0.0764 |
| Prevalent CVD | 9.44 | 5.56 | 0.4167 |
| Age start taking birth control pills | 22 ± 5 | 24 ± 5 | 0.0953 |
| Age stop taking birth control pills | 30 ± 7 | 31 ± 5 | 0.3383 |
| Years you have used birth control | 8 ± 6 | 7 ± 5 | 0.3157 |
| Characteristics | Pre-Menopause (n = 835) | Post-Menopause w/out HRT (n = 1,673) | Post-Menopause w/HRT (n = 634) | P-Value |
|---|---|---|---|---|
| Age, years | 45 ± 8 | 61 ± 10 | 58 ± 9 | <0.0001 |
| BMI, (kg/m2) | 33.3 ± 8.3 | 32.9 ± 7.2 | 32.0 ± 6.7 | 0.0063 |
| Obesity, Yes | 61.44 | 61.12 | 56.99 | 0.1463 |
| Education Level | <0.0001 | |||
| Less than High School | 6.73 | 25.52 | 14.80 | |
| High School/GED | 15.63 | 23.67 | 19.21 | |
| Greater than HS but less than BA/BS | 36.90 | 23.55 | 28.35 | |
| Bachelor Degree or Higher | 40.75 | 27.26 | 37.64 | |
| Family Income | <0.0001 | |||
| Low | 16.45 | 20.75 | 10.70 | |
| Lower- Middle | 21.70 | 31.20 | 23.89 | |
| Upper Middle | 35.60 | 25.86 | 31.37 | |
| Affluent | 26.24 | 22.19 | 34.05 | |
| Current Smoking, Yes | 10.71 | 10.17 | 8.85 | 0.4860 |
| Heavy Alcohol Use | 6.3 | 6.0 | 3.4 | 0.5325 |
| Fruit Intake | 1.4 ± 1.1 | 1.5 ± 1.1 | 1.5 ± 1.1 | 0.1369 |
| Vegetable Intake | 1.5 ± 0.7 | 1.4 ± 0.6 | 1.4 ± 0.6 | <0.0001 |
| % Calories due to Fat | 36.4 ± 7.2 | 34.2 ± 7.0 | 34.4 ± 7.2 | <0.0001 |
| Amt. of Fat Intake | 89.6 ± 53.1 | 70.5 ± 43.4 | 70.3 ± 38.3 | <0.0001 |
| Total Dietary Fiber | 15.4 ± 7.1 | 14.4 ± 6.9 | 14.3 ± 6.1 | 0.0006 |
| Beta-Carotene | 3,183 ± 1,629 | 3,280 ± 1,477 | 3,408 ± 1,462 | 0.0209 |
| Total Vitamin E | 52.7 ± 95.9 | 66.9 ± 108.8 | 85.1 ± 120.4 | <0.0001 |
| Vitamin C | 177.9 ± 175.0 | 187.5 ± 190.7 | 210.2 ± 208.1 | 0.0053 |
| Lycopene | 4,969 ± 5,998 | 3,827 ± 4105 | 3,754 ± 4,139 | <0.0001 |
| %Calories from Alcohol | 0.7 ± 2.4 | 0.4 ± 1.8 | 0.4 ± 1.4 | 0.0008 |
| Ever taken Birth Control, Yes | 82.5 | 49.5 | 62.9 | <0.0001 |
| Age of Onset Use of Birth Control | 20 ± 4 | 23 ± 5 | 23 ± 5 | <0.0001 |
| Duration of Use of Birth Control | 9 ± 7 | 7 ± 6 | 8 ± 6 | <0.0001 |
| Family History of Cancer | 51.72 | 63.50 | 60.34 | <0.0001 |
| Physical Activity Total | 9.0 ± 2.3 | 7.6 ± 2.6 | 8.2 ± 2.5 | <0.0001 |
| Active Living | 2.2 ± 0.8 | 2.0 ± 0.8 | 2.1 ± 0.8 | <0.0001 |
| Home and Garden | 2.4 ± 0.6 | 2.2 ± 0.6 | 2.2 ± 0.5 | <0.0001 |
| Sport Index | 2.2 ± 1.2 | 2.0 ± 1.2 | 2.2 ± 1.2 | <0.0001 |
| Work Index | 2.6 ± 0.7 | 2.7 ± 0.6 | 2.6 ± 0.6 | 0.0103 |
| Breast Cancer | 0.84 | 2.09 | 0.94 | 0.0223 |
| Cancer (General) | 3.40 | 11.05 | 7.33 | <0.0000 |
| Type Two Diabetes | 11.0 | 25.3 | 20.2 | <0.0001 |
| Hypertension | 43.4 | 73.8 | 78.3 | <0.0001 |
| Prevalent CVD | 4.1 | 12.7 | 8.1 | <0.0001 |
| Outcome | Models | Pre-Menopause | Post-Menopause w/out HRT | Post-Menopause w/ HRT |
|---|---|---|---|---|
| Prevalent Cancer | I | 1.00 | 3.33 (2.09,5.32) | 2.31 (1.34,4.00) |
| II | 1.00 | 1.97 (1.15,3.38) | 1.53 (0.85,2.75) | |
| III | 1.00 | 1.76 (0.98,3.17) | 1.54 (0.81,2.91) | |
| Prevalent Breast Cancer | ||||
| I | 1.00 | 7.59 (1.81,31.82) | 3.29 (0.64,17.03) | |
| II | 1.00 | 4.85 (1.03,22.85) | 2.32 (0.42,12.74) | |
| III | 1.00 | 3.56 (0.73,17.43) | 1.79 (0.30,10.60) |
© 2011 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Jenkins, B.W.C.; Addison, C.; Wilson, G.; Liu, J.; Fortune, M.; Robinson, K.; White, M.; Sarpong, D. Association of the Joint Effect of Menopause and Hormone Replacement Therapy and Cancer in African American Women: The Jackson Heart Study. Int. J. Environ. Res. Public Health 2011, 8, 2491-2504. https://doi.org/10.3390/ijerph8062491
Jenkins BWC, Addison C, Wilson G, Liu J, Fortune M, Robinson K, White M, Sarpong D. Association of the Joint Effect of Menopause and Hormone Replacement Therapy and Cancer in African American Women: The Jackson Heart Study. International Journal of Environmental Research and Public Health. 2011; 8(6):2491-2504. https://doi.org/10.3390/ijerph8062491
Chicago/Turabian StyleJenkins, Brenda W. Campbell, Clifton Addison, Gregory Wilson, Jiankang Liu, Melody Fortune, Kiana Robinson, Monique White, and Daniel Sarpong. 2011. "Association of the Joint Effect of Menopause and Hormone Replacement Therapy and Cancer in African American Women: The Jackson Heart Study" International Journal of Environmental Research and Public Health 8, no. 6: 2491-2504. https://doi.org/10.3390/ijerph8062491