Article Text

Abstract
Introduction A number of factors contribute to the performance and motivation of India’s Accredited Social Health Activists (ASHAs). This study aims to identify the key motivational factors (and their relative importance) that may help retain ASHAs in service.
Methods A discrete choice experiment (DCE) survey presented ASHAs with eight unlabelled choice sets, each describing two hypothetical jobs that varied based on five attributes, specifically salary, workload, travel allowance, supervision and other job benefits. Multinomial logit and latent class (LC) models were used to estimate stated preferences for the attributes.
Result We invited 318 ASHAs from 53 primary health centres of Guntur, a district in south India. The DCE was completed by 299 ASHAs using Android tablets. ASHAs were found to exhibit a strong preference for jobs that incorporated training leading to promotion, a fixed salary and free family healthcare. ASHAs were willing to sacrifice 2530 Indian rupee (INR) from their monthly salary, for a job offering training leading to promotion opportunity and 879 INR for a free family health-check. However, there was significant heterogeneity in preferences across the respondents. The LC model identified three distinct groups (comprising 51%, 35% and 13% of our cohort, respectively). Group 1 and 2 preferences were dominated by the training and salary attributes with group 2 having higher preference for free family health-check while group 3 preferences were dominated by workload. Relative to group 3, ASHAs in groups 1 and 2 were more likely to have a higher level of education and less likely to be the main income earners for their families.
Conclusion ASHAs are motivated by both non-financial and financial factors and there is significant heterogeneity between workers. Policy decisions aimed at overcoming workforce attrition should target those areas that are most valued by ASHAs to maximise the value of investments into these workers.
Trial registration number CTRI/2018/03/012425.
- motivation
- preferences
- willingness to sacrifice salary
- latent class analysis
- discrete choice experiment (DCE)
- the accredited social health activists (ASHAs)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- motivation
- preferences
- willingness to sacrifice salary
- latent class analysis
- discrete choice experiment (DCE)
- the accredited social health activists (ASHAs)
Key questions
What is already known?
One of the major challenges faced by the Indian health system is keeping Accredited Social Health Activists (ASHAs) motivated, and retaining them in service.
Several factors including individual, social, economic and work-related factors impact the motivation and retention of the ASHAs
What are the new findings?
Career progression was found to be the main influencing factor for ASHAs choosing between job options in addition to fixed salary and other non-financial factors such as priority free family health-check and reduced workload.
There is a heterogeneity in the preference profile of ASHAs depending on their sociodemographic factors.
What do the new findings imply?
Policy recommendations should consider the preferences of health workers and target features most valued by ASHAs.
Non-financial and financial incentives should be combined to improve health workers’ satisfaction and performance.
Discrete choice experiments provide evidence about effective incentives for community health workers in order to improve their motivation to remain in the workforce.
Introduction
The shortage of health workforce in low-income and middle-income countries is a major challenge to achieve the United Nation’s Sustainable Development Goals (SDGs). Projections by the WHO indicate that in order to achieve the SDGs by 2030, there is a worldwide shortfall of 18 million health workers, of which 6.9 million will be in Southeast Asia.1 One promising approach to overcome workforce shortages has been the formal incorporation of community health workers (CHWs) in the health systems as frontline care providers and form a link between the community and the health system.2 CHWs are health workers who do not hold formal professional certification but receive job-related preservice training, and usually reside in the community where they work.3 CHWs have been a cornerstone of health systems in several countries.4 Over 26 different CHW programmes have been identified in the literature across more than 24 low-income and middle-income countries; with remarkable diversity in their remuneration, training and job description.5
One of the major challenges faced by health systems is keeping CHWs motivated and retaining them in service. Attrition rates for CHWs are variable and are reported to be between 3% in the Solomon Islands and 77% in other low-income and middle-income countries.6 High attrition rates impact on service delivery as the continuous replacement of CHWs results in increased recruitment and training costs,7 lost chances to build on experience and trust built between the community and the CHW. A number of factors contribute to the performance and motivation of CHWs including financial and non-financial incentives.6 Despite a large literature describing the CHW motivation and retention in the local health settings,8–11 there is limited empirical evidence on the importance of the different factors and the trade-offs that CHW may be willing to make between them.
In India, the National Rural Health Mission introduced a cadre of CHWs, the ‘Accredited Social Health Activist’ (ASHA) in 2005. ASHAs reside in the rural communities where they work and their main task is to link the community to the public health system. They are female volunteers who are remunerated according to a performance-based incentive system, where they receive money conditional on delivering services or attaining targets such as tracking and ensuring full childhood immunisation. They are often confronted by challenges such as lack of support by supervisors, and insufficient and/or delayed remuneration which impacts their motivation12 and often leads to attrition. While some studies have explored factors which motivate ASHAs (eg, adequate compensation and community recognition),13 14 there is no empirical evidence about the relative importance of the different incentives that may help to retain ASHAs in service.
Understanding the preferences of ASHAs is essential to the development of interventions aimed at reducing attrition rates across the health system. This is particularly important in settings where the resources available to fund health services are constrained. Discrete choice experiments (DCEs) have been widely used to elicit the preferences of healthcare workers across a variety of settings. A DCE is a quantitative research method that is regarded as a more useful tool than ranking techniques in policy analysis and planning. DCEs can be designed to provide insight into the relative value of specific components (attributes) of interventions, the trade-offs respondents may be willing to make between the attributes and the overall value attached to a programme.15 16
This article aims to elicit the preferences of ASHAs in Guntur, a district in Andhra Pradesh, southern India, for attributes of their work that may increase motivation and reduce the rates of attrition, quantify the relative importance of the different attributes and the impact of demographic factors on preferences.
Methods
The study was registered with ‘Clinical Trials Registry—India’ (http://ctri.nic.in). A participant information sheet and consent form were used to gain consent of participating ASHAs.
Patient and public involvement
This research was done without patient involvement. It was not appropriate or possible to involve patients or the public in this work
Development of DCE for ASHAs
Identification of the attributes and levels
Contextual factors and challenges that CHWs face in undertaking their daily tasks were identified through a literature review of peer-reviewed articles and grey literature of the CHWs’ perspectives and experiences and a review of policy documents relating to the recruitment, training, job description, remuneration, supervision and career progression of ASHAs.17 In addition, synthesis of focus group discussions and in-depth interviews of ASHAs from a related study in the same region of India18 helped us understand the enablers and barriers faced by ASHAs while performing their duties in the community. The emerging themes guided the development of a list of key attributes relating to the ASHA’s job conditions, satisfaction, expectations and motivating factors. Once the attributes were finalised, the research team assigned levels to each attribute to reflect the realistic options that ASHAs experience in their work.
Expert consultation and construction of job sets
Attributes and levels were finalised after consulting researchers and programme managers familiar with the Indian health system. They were asked to review the attributes and provide insight regarding whether the attributes and levels depicted realistic options. In addition, the wording of the different levels was edited to ensure they were comprehensible and relevant to the ASHAs. From this process, the included attributes in the DCE were as follows: fixed salary, workload, travel allowance, supervision, job benefits incorporating training leading to promotion to the next level of auxiliary nurse midwife (ANM), free family health-check and free household products. A list of the attributes and levels in the DCE is presented in table 1.
Attributes and levels used in the discrete choice experiment
DCE design
The DCE was designed following standard practices19 using the software Ngene V.1.2.0 (ChoiceMetrics Pty, Sydney, New South Wales, Australia).20 We used a d-efficient fractional factorial design with two blocks of eight questions using a multinomial logit model with no interaction terms specified in the design. The ASHA’s educational level was taken into consideration when determining the number of attributes in each choice set to minimise cognitive burden.21 The final design was translated into the local language (Telugu). Participants were asked to respond to eight choice sets each containing two unlabelled job profiles. The respondents were required to choose their preferred alternative from the two options. After choosing the preferred job profile, they were asked if they would accept that job if it was offered, thereby providing an indication of preference relative to their current job. The DCE was piloted with 20 ASHAs to confirm cognitive understanding and ensure appropriateness of the wording of the questions, attributes and levels to the ASHAs. The data from the pilot were analysed and the estimated coefficients were used as prior estimates to maximise the statistical efficiency of the design of the DCE. The final design was split into two blocks (each answered by approximately half of the cohort). The DCE and collection of sociodemographic information (age, education, years of service, working hours, location of work, other paid job and main household earning status) were administered on computer tablets using an offline Android-based application developed by the research team.22
Data collection
The study was conducted in Guntur, the second most populous district of Andhra Pradesh, a southern state of India. Guntur was selected because of its rural status with more than 66% of its population living in the rural areas. Data collection occurred from April to June 2018 with primary health centres (PHCs) as the sampling unit of the study. We randomly selected 53 PHCs out of a total of 84 PHCs in Guntur, representing all the rural and remote regions of the district. Six ASHAs from each of the selected PHCs were invited to participate in the study, the ASHA’s supervisors facilitated the invitation of the ASHAs to the DCE sessions which took place within the PHCs’ premises. The DCE was self-administered on the tablets in the local language (Telugu). A member of the research team explained the nature of the study to the participants, went through the introductory statement with them and explained the job sets. They also ensured that the ASHAs responded individually by discouraging group discussions. The introductory statement is provided in online supplementary material 1.
Supplemental material
Analysis
DCEs are theoretically based on random utility theory where independent rational actors act to maximise their individual utility.23 We assume that participants will choose the job that maximises their individual benefit or utility which depends on the attributes such that:

where:
Salary=Fixed monthly salary;
Training=Mandatory regular training leading to promotion to the next level ANM;
Health=Priority free family health-check;
Supervision=Field visits supervision;
Travel=Travel allowance;
Workload=Daily workload.
At the end of the study, data from the computer tablets were extracted into an Excel spreadsheet and analysed using NLOGIT software V.6 (7 September 2016. Copyright 1986–2016 Econometric Software). The analysis of the DCE has followed the general approach outlined by the International Society of Pharmacoeconomics and Outcomes Research and published guides to model specification.24 25 The multinomial logit model was used to estimate the relative utility of job attributes. Salary and workload hours were modelled as continuous variables, and the others were specified as categorical and effects coded. A willingness to ‘sacrifice salary’ analysis was carried out in order to estimate the strength of the ASHAs’ preferences to a single standard—how much salary are the ASHAs willing to sacrifice in order to secure their ‘desired job’.
A latent class (LC) model was used to explore preference heterogeneity by identifying the existence of LCs with differing preference profiles. It is not possible to assign an individual participant to a specific LC; however, inclusion of sociodemographic factors as covariates in the LC model provides an understanding of the distinguishing characteristics of the classes. The final LC model was specified with three LCs based on log-likelihood tests and comparison with models having two or four LCs. The sociodemographic factors used to predict LC membership included education, other paid job and main household earning status. The final model included covariates that were statistically significant predictors (p<0.1) of an individual being a member of an LC.
Results
ASHA characteristics
A total of 318 ASHAs were invited to participate in the study from 53 PHCs across Guntur, of which 299 completed the DCE giving a response rate of 94%. The average age of participating ASHAs was 35 years, all were females and 60% of them had completed at least 12 years of education. All but 4 of the 299 ASHAs, resided in the villages they worked in. Most of the ASHAs (75%) had worked in the role for more than 6 years, worked for at least 6 hours/day (65%) and had another paid job (68%). The demographics of the ASHAs are presented in table 2.
Demographics of the ASHAs participating in the discrete choice experiment (n=299)
Multinomial logit model
The multinomial logit model was a good fit to the data (pseudo R2 0.263); it showed that the main factor which influenced ASHAs’ job choice was training leading to career progression to the cadre of ANM. This was followed by a fixed monthly salary and priority free family health-check at the local PHC. Provision of travel allowance, workload and supportive supervision did not have an influence on the ASHA’s job choice. The option of having free household products was inversely related to motivation.
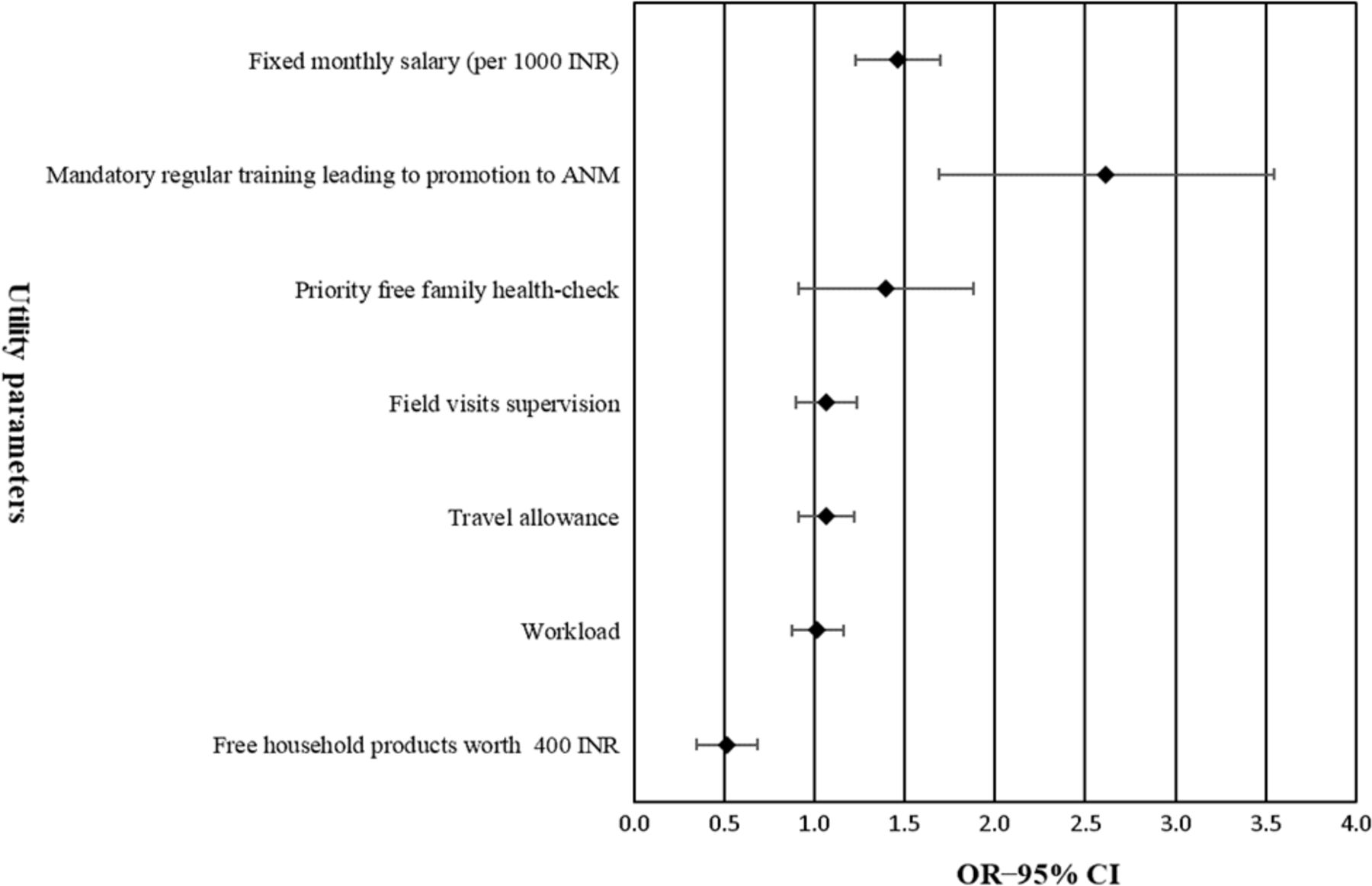
The willingness to sacrifice salary analysis showed that ASHAs were willing to sacrifice 2530 Indian rupee (INR) (US$35.45) of their monthly salary for a job that offers them training with an opportunity for promotion to the ANM position and 879 INR (US$12.32) for free priority family health-check at the local PHC. Multinomial logit model analysis results and willingness to sacrifice salary analysis results are presented in table 3 and figure 1.
Multinomial logit model results (n=299, McFadden pseudo R2=0.263, log-likelihood function=−1222.07, number of observations=2392)

{kind=link}
Willingness to ‘sacrifice salary’ analysis (per 1000 INR) after ‘fixed monthly salary’ (n=299, McFadden pseudo R2 = 0.263). ANM, auxiliary nurse midwife; INR, Indian rupee.
LC model
The LC model was a good fit to the data (pseudo R2 of 0.279); it identified three distinct classes of ASHAs. Group 1 and 2 ASHAs were both strongly influenced by the presence of training leading to promotion to the ANM position, followed by salary. In addition, group 2 ASHAs were highly influenced by priority free family health-check at the local PHC. Interestingly, both groups were less likely to accept the job choice if it offered them free household products worth 400 INR. In contrast, group 3 ASHAs preferred less workload and no other factor had a statistically significant effect on their choices. Results of LC model analysis are presented in table 4.
Latent class logit model results (n=299, McFadden pseudo R2=0.279, log-likelihood function=−1194.76, number of observations=2392)
The probability of belonging to a particular respondent class varied based on education level, having another paid job and whether they were the main household earner. Compared with group 3, group 1 ASHAs were more likely to have a higher level of education (OR 4.03; 95% CI 1.47 to 11.00) and less likely to be the main household earners for their families (OR 0.41; 95% CI 0.16 to 2.07). Group 2 ASHAs were more likely to have a higher level of education (OR 7.09; 95% CI 1.84 to 27.33), have another paid job (OR 3.64; 95% CI 1.14 to 11.60) and less likely to be the main household earners for their families (OR 0.21; 95% CI 0.07 to 0.70).
Discussion
Our findings demonstrate that more than 85% of the participating ASHAs were influenced by the opportunity of promotion through training and were willing to sacrifice 2530 INR (US$35.45) out of their monthly salary for a job that offers them career progression. These data are in line with previous literature specifying the importance of career development for motivating CHWs in India.26 Our results are also broadly consistent with previous human resource for health research utilising DCE, which indicate that career development and continuing education were the main influence shaping the preference profile for nurses in Malawi and Hanson,27 Lao28 and community health officers in Ghana.29 Although training with a promotion opportunity is not a direct financial incentive, it offers the CHWs an opportunity to progress to the next cadre with higher salary, more authority and recognition. Priority free family health-check and low workload were other driving factors that affected the ASHAs’ choices. These findings support the growing evidence of the importance of the non-financial interventions in motivating CHWs in developing countries,15 and the need for a bundle of combined non-financial and financial benefits.6 The recent WHO guidelines for optimising CHW programs30 recommended a fair financial incentive to be provided to the CHWs which should be proportionate to the workload they perform and could include career development pathway for the well performing members. This should be accompanied by a non-financial package that could be tailored to the local context. Both options are indispensable, where monetary incentives provide security and allow for personal development of the workers; non-monetary incentives provide satisfaction and can optimise the CHW’s performance.
Our study showed a significant heterogeneity of ASHAs’ preferences, which varied depending on their education level, having another paid job or by being the main household earner. Age did not have a significant effect on the ASHA’s decisions. For instance, the ASHAs in group 2 valued the priority free family health-check at the local PHC, were more likely to have a second paid job and were less influenced by training opportunities compared with the ASHAs in group 1. This may be because ASHAs having larger families may need more health visits, and are more concerned that training might take them away from their families or cost them more days off their second job. This preference heterogeneity suggests that policy options are perceived differently by ASHAs depending on their individual circumstances. While policy decisions cannot be tailored to individual preferences, they need to be contextualised to the overall preferences of the ASHAs. Our study demonstrates that there are two broad groups of ASHAs, higher educated ones aiming for career progression with a better pay and recognition; and less educated ASHAs more interested in immediate high pay with no intention for further training to be promoted. These results could be used by policy makers to offer two or more packages for ASHAs. Since the educational requirement for ASHA’s selection has recently increased to a minimum of 10 years of education, the less educated ASHAs may receive a fixed salary and the higher educated ASHAs could compromise some of their pay to cover their training expenses for an opportunity to be promoted to the next cadre. This can be applied until the less educated ASHAs are progressively eliminated out of the programme, allowing for a higher educated cadre with more capacity and tendency to advance.
The DCE is a useful method for human resource research and helps to investigate the impact of potential policy options on different subgroups within the study population. It is of value to low-income and middle-income countries where the need to make the best use of the limited resources. However, DCE requires expertise and competence in design and analysis. The United States Agency for International Development (USAID) has developed a rapid DCE tool31 for low-income and middle-income countries to design and implement evidence-based recruitment and retention strategies. The tool is a simplified and reliable version of the DCE, and does not require a high level of expertise. It has been used to identify attraction strategies for Lao’s health workers to accept rural positions.32
Although DCE is a reliable tool, the results will always be dependent on the attributes used and the clarity by which these attributes were presented to the participants. This highlights the importance of initial qualitative work to obtain pragmatic policy options that are realistic and accord well with the experiences of health workers. One of the limitations of our study is that we did not perform any tests to ensure internal validity of the DCE among the participants and that they have a complete understanding of the study. Instead, we used ‘think aloud’ and ‘verbal probing’ techniques to cognitively test our DCE survey.22 While the results of our study can be generalised to the state of Andhra Pradesh due to similar remuneration policies, the findings may not be applicable to other states of India, due to the variation in the remuneration policies of ASHAs. All our participants were from the same Indian district and we did not compare them to other districts, where ASHAs might have a different preferences profile. Previously, human resource retention policies were exclusively decided by policy makers, this study provides a rigorous method for identifying the preferences of the local health workers to improve their motivation.
The Government of India has recently announced a revised pay scale for the ASHAs with a free social security cover.33 These guidelines are supposed to come into effect immediately. Given that different states in India have the authority to implement the new recommendations,34 the following years will see how this policy is rolled out in the different states and districts of India.
Conclusion
Bundled incentives of both financial and non-financial packages are attractive to ASHAs. Policy decisions should be contextualised to local health worker’s preferences to guarantee their satisfaction and better performance and improved quality of service. Our study demonstrates the potential value of using DCEs in other low-income and middle-income countries to analyse local CHW preference profile and identify the most effective policy interventions that can vary from one setting to another and from one country to another.
Acknowledgments
We would like to acknowledge Dr Praveen Deversetty for his involvement in the DCE attributes and for the logistics and planning for the development of the Android DCE application. We would also like to acknowledge the effort done by Mr Bhanu Bangari and Miss Nirosha Yeddalapudi in developing the Android-based application. We would also like to thank Mr Mohammed Abdul Ameer for conducting the DCE and all the ASHAs for their participation.
References
Footnotes
Handling editor Sanni Yaya
Contributors The study design was developed by RJ and MA-A. BA and MA-A performed the analysis under the supervision of MH and KH. MA-A and RJ drafted this article and all authors revised the manuscript.
Funding RJ is funded by the Australian National Heart Foundation Future Leader Fellowship. SJ is funded by an NHMRC Principal Research Fellowship.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Approval for the overall study was obtained from The George Institute Ethics Committee of The George Institute for Global Health, India (project number 009/2017).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data relevant to the study are included in the article or uploaded as supplementary information.