





Abstract
Endometriosis is a chronic condition affecting between 2 and 17% of women of reproductive age. Common symptoms are chronic pelvic pain, fatigue, congestive dysmenorrhoea, heavy menstrual bleeding and deep dyspareunia. Studies have demonstrated the considerable negative impact of this condition on women's quality of life (QoL), especially in the domains of pain and psychosocial functioning. The impact of endometriosis is likely to be exacerbated by the absence of an obvious cause and the likelihood of chronic, recurring symptoms. The aims of this paper are to review the current body of knowledge on the social and psychological impact of endometriosis on women's lives; to provide insights into women's experience of endometriosis; to provide a critical commentary on the current state of knowledge and to make recommendations for future psycho-social research.
The review draws on a method of critical narrative synthesis to discuss a heterogeneous range of both quantitative and qualitative studies from several disciplines. This included a systematic search, a structured process for selecting and collecting data and a systematic thematic analysis of results.
A total of 42 papers were included in the review; 23 used quantitative methods, 16 used qualitative methods and 3 were mixed methods studies. The majority of papers came from just four countries: UK (10), Australia (8), Brazil (6) and the USA (5). Key categories of impact identified in the thematic analysis were diagnostic delay and uncertainty; ‘QoL’ and everyday activities; intimate relationships; planning for and having children; education and work; mental health and emotional wellbeing and medical management and self-management.
Endometriosis has a significant social and psychological impact on the lives of women across several domains. Many studies have methodological limitations and there are significant gaps in the literature especially in relation to a consideration of the impact on partners and children. We recommend additional prospective and longitudinal research utilizing mixed methods approaches and endometriosis-specific instruments to explore the impact of endometriosis in more diverse populations and settings. Furthermore, there is an urgent need to develop and evaluate interventions for supporting women and partners living with this chronic and often debilitating condition.
Introduction
Endometriosis is a chronic condition affecting women of reproductive age. It is characterized by the presence of endometrial-like tissue outside the uterus which induces a local inflammatory response (Kennedy et al., 2005; de Nardi and Ferrero, 2011). It is an enigmatic condition; the aetiology is uncertain and contested (Damewood et al., 1997; World Endometriosis Society and the World Endometriosis Research Foundation, 2012). Common symptoms are chronic pelvic pain, fatigue, congestive dysmenorrhoea, heavy menstrual bleeding and deep dyspareunia (Lemaire, 2004; de Nardi and Ferrero, 2011), and it is suggested that 47% of infertile women have endometriosis (Meuleman et al., 2009). The prevalence of endometriosis is difficult to assess but has been estimated at between 2 and 17% of the female population (Damewood et al., 1997; Eskenazi and Warner, 1997; Bernuit et al., 2011). There is no cure for endometriosis and so management focuses on symptom relief. This can involve a range of interventions including analgesics, hormonal therapy, both minimally invasive and radical surgery, and, where relevant, fertility treatment, with varying rates of success (European Society of Human Reproduction and Embryology, 2013).
Given the chronic nature of endometriosis, the potential impact on fertility and intimate relationships, the delays in diagnosis and the problematic experiences of care (Dancet et al., 2012), the social psychological impact of endometriosis on women is worthy of attention. Furthermore, there are very significant costs associated with endometriosis. A recent large-scale multicentre study of the economic costs of endometriosis revealed substantial direct and indirect costs, with annual healthcare expenditure comparable with that of other major chronic conditions such as diabetes (Simoens et al., 2012). Endometriosis is therefore of considerable importance both directly in terms of its potentially negative impact on the large number of women affected by the condition and indirectly on healthcare systems and society.
The aims of this paper are to review the current body of knowledge on the social and psychological impact of endometriosis on women's lives; to provide insights into women's experience of endometriosis; to provide a critical commentary on the current state of knowledge and to make recommendations for future psycho-social research. The research question is: ‘What is the impact of endometriosis on women's lives and how has this been studied?’
Methods
To meet these objectives we adopted a method of review which involves an interpretive process and which allows the inclusion of a diversity of questions and studies, both quantitative and qualitative, from a range of disciplines. The review therefore draws on a method of critical narrative synthesis (Dixon-Woods et al., 2006; Popay et al., 2006) rather than a classic systematic review methodology. We have, however, adhered to the PRISMA principles as far as applicable for this type of review (Moher et al., 2009) and our reporting broadly follows this approach.
Information sources and search strategy
In February 2012, a systematic search of 13 health, medical, multidisciplinary, social science and psychology-specific databases was conducted. Appropriate search terms were constructed by reviewing abstracts, titles and keywords from a sample of papers relating to the socio-psychological impact of endometriosis known to the authors. As there appeared to be little homogeneity in the terminology used a decision was made to use ‘endometriosis’ as the sole search term for the social science and psychology-specific databases to ensure an inclusive approach. Sixteen further search terms were subsequently combined with ‘endometriosis’ when searching health, medical and multidisciplinary databases in order to limit the results to papers relevant to the review. Table I shows the databases searched and the search terms used.
Literature review databases and search terms.
| Disciplines | Databases accessed | Search terms used |
|---|---|---|
| Social science and psychology specific | Social Science Citation Index Applied Social Sciences Index and Abstracts International Bibliography of Social Sciences PsycINFO PsycARTICLES | Endometriosis |
| Health, medical and multi-disciplinary | Pubmed Academic Search Premier CINAHL Plus British Nursing Index Scopus Cochrane Library Ingenta Connect CSA Illumina | Endometriosis AND (feel OR cope OR stress OR emotion* OR distress OR quality OR experien* OR impact OR psycho* OR qualitative OR depression OR anxiety OR affect OR coping OR social OR socio*) |
| Disciplines | Databases accessed | Search terms used |
|---|---|---|
| Social science and psychology specific | Social Science Citation Index Applied Social Sciences Index and Abstracts International Bibliography of Social Sciences PsycINFO PsycARTICLES | Endometriosis |
| Health, medical and multi-disciplinary | Pubmed Academic Search Premier CINAHL Plus British Nursing Index Scopus Cochrane Library Ingenta Connect CSA Illumina | Endometriosis AND (feel OR cope OR stress OR emotion* OR distress OR quality OR experien* OR impact OR psycho* OR qualitative OR depression OR anxiety OR affect OR coping OR social OR socio*) |
Literature review databases and search terms.
| Disciplines | Databases accessed | Search terms used |
|---|---|---|
| Social science and psychology specific | Social Science Citation Index Applied Social Sciences Index and Abstracts International Bibliography of Social Sciences PsycINFO PsycARTICLES | Endometriosis |
| Health, medical and multi-disciplinary | Pubmed Academic Search Premier CINAHL Plus British Nursing Index Scopus Cochrane Library Ingenta Connect CSA Illumina | Endometriosis AND (feel OR cope OR stress OR emotion* OR distress OR quality OR experien* OR impact OR psycho* OR qualitative OR depression OR anxiety OR affect OR coping OR social OR socio*) |
| Disciplines | Databases accessed | Search terms used |
|---|---|---|
| Social science and psychology specific | Social Science Citation Index Applied Social Sciences Index and Abstracts International Bibliography of Social Sciences PsycINFO PsycARTICLES | Endometriosis |
| Health, medical and multi-disciplinary | Pubmed Academic Search Premier CINAHL Plus British Nursing Index Scopus Cochrane Library Ingenta Connect CSA Illumina | Endometriosis AND (feel OR cope OR stress OR emotion* OR distress OR quality OR experien* OR impact OR psycho* OR qualitative OR depression OR anxiety OR affect OR coping OR social OR socio*) |
Process for selecting papers
Eligibility criteria
The review was designed to take a broad overview of the topic, going beyond conventional ‘quality-of-life’ studies, to include the contribution of work from several disciplines including sociology, psychology and anthropology and both qualitative and quantitative approaches, to provide a more comprehensive and holistic picture of the impact of endometriosis on the lives of women.
Inclusion criteria
Peer-reviewed, English-language journal articles that examined the social and psychological impact of endometriosis, its treatment and management were included in the review. No age limits on participants or date restrictions were imposed.
Exclusion criteria
Papers solely investigating the prevalence, medical or clinical features of endometriosis or reporting clinical effectiveness of treatments were excluded. Reviews, opinion pieces, commentaries and clinical cases studies which did not include new data were also excluded.
Screening
Documents identified through database searching were screened and assessed for eligibility. First, duplicates and ineligible publication types were removed. Following this, titles and, if needed, abstracts and full texts were screened by two authors independently (H.M. and C.L.) based on clearly defined inclusion and exclusion criteria and those deemed ineligible were removed.
Quality assessment
A quality assurance tool appropriate for both quantitative and qualitative studies was applied to full text papers (Shepherd et al., 2006). This included seven criteria and, consistent with its prior use, papers were required to achieve a score of at least four out of seven to be included (Dancet et al., 2010). Three authors quality assured the papers (by L.C., E.D. and C.L.); papers identified for potential exclusion were then reviewed by a fourth author (N.H.) and a decision was made.
Data collection process
A data extraction sheet was developed and applied to each paper to independently extract data (by all authors). Papers which met the inclusion criteria and quality assessment criteria were examined comprehensively and information from each paper was collated in an Excel spreadsheet recording: authors; publication date; research setting; research aims; research design; participants; sample size; recruitment method; data analysis methods; key findings; key themes and methodological limitations including risk of bias. For each paper, one author acted as the primary reviewer and a second author verified the data extraction. Any discrepancies were discussed between reviewers and consensus was achieved.
Analysis
To report on paper findings, analysis and organization of the extracted data were conducted according to principles of systematic thematic analysis (Dixon-Woods et al., 2005; Braun and Clarke, 2006; Ward et al., 2009). Stage one included a process of ‘open coding’ which was used by all seven authors to organize data from each paper during data extraction. Open coding refers to a process of selecting and naming significant issues which arise from a body of data. This process was carried out for all 42 papers. Open codes were then collated by one author (C.L.) and organized under higher order categories, or substantial themes, according to standard principles of thematic analysis (Braun and Clarke, 2006). For example, the codes ‘stress’, ‘self-esteem’, ‘depression’, ‘anxiety’ and ‘isolation’ were grouped under the substantial theme ‘mental health and emotional wellbeing’. The resultant framework of substantial themes was discussed and refined by three authors (L.C., C.L. and N.H.) and the final seven substantial themes were agreed. The extracted data were then reorganized according to these substantial themes, and they were employed as the structuring framework for the narrative summary.
To report on paper characteristics, quantitative data on the characteristics of papers were collated and counted. These are reported in the section ‘Characteristics of papers’.
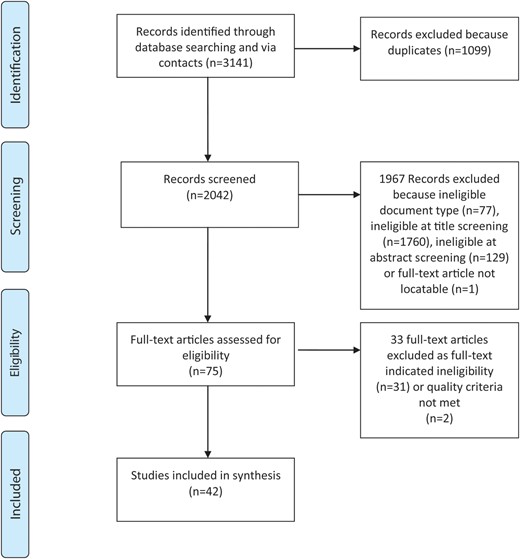
Results: search, screening and selection
The database searches resulted in a total of 1963 papers and 2 further papers were identified via contacts while duplicates and ineligible document types were excluded. After screening the titles, 1760 papers were excluded, and after screening the abstracts, 129 papers were excluded. Following this full text papers were sought. One paper (Kumar et al., 2010) was not included as it could not be located: an inter-library loan request was unsuccessful as a supplier could not be located, and the author did not respond to email requests. After screening full texts, 31 papers were excluded, and after quality assuring full texts, 2 papers were excluded, resulting in 42 papers for inclusion. An overview of the search results and screening criteria is summarized in Fig. 1.
Search results and screening.
Characteristics of papers
Given the wide-ranging nature of this review, considerable variation was found in research aims and questions, methodology, sample size and outcome measures. Table II provides an overview of the heterogeneity of the data using the variables: author/date/country; study aim/research question; research design and method and sample. In some instances data from one study were reported on in two or more papers, and therefore the 42 papers do not represent 42 separate studies or samples.
Paper characteristics.
| Authors, year of publication, country of analysis and participants (if different) | Study aim/research question | Research design and methods | Sample |
|---|---|---|---|
| Ballard et al. (2006), UK | To investigate the possible reasons for a delayed diagnosis of endometriosis and the impact of delay on women's experiences of endometriosis | Qualitative Interviews | 28 women with suspected or confirmed endometriosis. Recruited via hospital/clinic |
| Bernuit et al. (2011), Germany (analysis), cross country (participants) | To elucidate the differences in diagnoses and treatment experiences of women and to assess the impact of endometriosis on their QoL | Quantitative Author devised online survey | 21 749 women of which 5.1% had surgically or non-surgically diagnosed endometriosis. Recruited via online market research company |
| Butt and Chesla (2007), USA | To investigate the responses in couples' relationships to living with chronic pelvic pain from endometriosis | Qualitative Interviews | 13 women with endometriosis and 13 male partners of women with endometriosis. Recruited via hospital/clinic and support group |
| Chene et al. (2012), France | To compare pain symptoms and the QoL between epiphenomenon and endometriosis disease | Quantitative Author devised questionnaire; SF-36; simplified sexual satisfaction Subscale of the DSFI; pain VAS | 437 women with endometriosis. Recruited via hospital/clinic |
| Christian (1993), USA | To determine the relationship between women's symptoms of endometriosis and self-esteem | Quantitative Author devised questionnaire; RSES | 23 women with endometriosis. Recruited via hospital/clinic |
| Cox et al. (2003a), Australia | To identify the information and support needs of women with endometriosis | Mixed Author devised questionnaire | 465 women with endometriosis. Recruited via hospital/clinic and support group |
| Cox et al. (2003b), Australia | To identify information needs of women facing laparoscopy for endometriosis | Qualitative Focus groups | 61 women with endometriosis. Recruited via hospital/clinic and support group |
| Cox et al. (2003c), Australia | To determine women's needs for information related to laparoscopy for endometriosis | Mixed Author devised questionnaire and focus groups | 61 women with endometriosis. Recruitment route not stated |
| Denny (2004a), UK | To explore women's experiences of living with endometriosis | Qualitative Interviews | 15 women with endometriosis. Recruited via hospital/clinic, support group and snowballing |
| Denny (2004b), UK | To explore women's experiences of living with the pain of endometriosis and examine delay in the diagnosis of the disease | Qualitative Interviews | 20 women with endometriosis. Recruited via hospital/clinic, support group and snowballing |
| Denny (2009), UK | To explore women's experiences of living with endometriosis in a prospective study over a 1-year period | Qualitative Interviews and diaries | 30 women with endometriosis. Recruited via hospital/clinic |
| Denny and Mann (2007), UK | To determine how much of an impact endometriosis-associated dyspareunia has on the lives and relationships of women | Mixed Interviews | 30 women with endometriosis. Recruited via hospital/clinic |
| Denny and Mann (2008), UK | To elicit the experience of endometriosis and the impact on women's lives; to explore the experience of women with endometriosis in the primary care setting | Qualitative Interviews | 30 women with endometriosis. Recruited via hospital/clinic |
| Eriksen et al. (2008), Denmark | To compare patients with endometriosis with and without pain symptoms to see if they differed on four psychological parameters (coping, emotional inhibition, depression and anxiety); to examine the effects of pain caused by endometriosis on psychosocial functioning | Quantitative Author devised questionnaire; CSQ; CECS; BDI; State Anxiety Scale of the STAI | 63 women with endometriosis. Recruited via hospital/clinic. |
| Fagervold et al. (2009), Norway | To investigate longitudinally the consequences of endometriosis in women diagnosed with the disease 15 years ago. | Quantitative Author devised questionnaire | 78 women with endometriosis. Recruited via hospital/clinic |
| Ferrero et al. (2005), Italy | To characterize the sexual function in women with endometriosis and deep dyspareunia | Quantitative Adapted sexual satisfaction Subscale of the DSFI; GSSI; VAS | 136 women of which 96 had endometriosis. Recruited via hospital/clinic |
| Fourquet et al. (2011), Puerto Rico | To quantify the impact of endometriosis-related symptoms on physical and mental health status, health-related QoL and work-related aspects | Quantitative SF-12; EHP-5; WPAI | 193 women with endometriosis. Recruited via Endometriosis Research Programme |
| Fourquet et al. (2010), Puerto Rico | To assess the burden of endometriosis by obtaining patient-reported outcome data describing the experience of living with endometriosis | Quantitative Author devised questionnaire | 107 women with endometriosis. Recruited via Endometriosis Research Programme |
| Gilmour et al. (2008), New Zealand | To explore the impact of symptomatic endometriosis on women's social and working lives | Qualitative Interviews | 18 women with endometriosis. Recruited via support group |
| Huntington and Gilmour (2005), New Zealand | To explore women's perceptions of living with endometriosis, its effects on their lives and the strategies used to manage their disease | Qualitative Interviews | 18 women with endometriosis. Recruited via support group |
| Jones et al. (2004), UK | To explore and describe the impact of endometriosis upon QoL; to identify and understand, from the patient's perspective, the areas of health-related QoL that are affected by endometriosis and to address the benefits of using a qualitative methodology for item generation in the development of disease-specific health status questionnaires | Qualitative Interviews | 24 women with endometriosis. Recruited via hospital/clinic |
| Lemaire (2004), USA | To examine the frequency, severity, interference with daily life and symptom distress associated with endometriosis and to explore the relationships among symptoms, emotional distress, uncertainty and a preference for and adequacy of information | Quantitative Author devised questionnaire; MUIS-C; adapted HOSI | 298 women with endometriosis. Recruited via support group |
| Lorençatto et al. (2006), Brazil | To compare the prevalence of depression in women with endometriosis according to the presence or absence of pelvic pain | Quantitative BDI | 100 women with endometriosis. Recruited via hospital/clinic |
| Low et al. (1993), UK | To investigate the possibility of a specific psychological profile associated with endometriosis | Quantitative Author devised questionnaire; EPQ; BDI; GHQ 30; STAI; GRIMS; SF-MPQ | 81 women of which 40 had endometriosis. Recruited via hospital/clinic |
| Manderson et al. (2008), Australia | To explore whether and how women's experience of gynaecological or reproductive health problems or conditions impacted their gendered, social and personal identities | Qualitative Interviews | 40 women of which 25 had endometriosis. Recruited via community newsletter and snowballing |
| Markovic et al. (2008), Australia | To explore the influence of socio-demographic background and social and family norms on the illness narratives of endurance and contest among women with endometriosis | Qualitative Interviews | 30 women with endometriosis. Recruited via community newsletter and snowballing |
| Marques et al. (2004), Brazil | To assess the QoL in women with chronic pelvic pain associated with endometriosis and to correlate QoL with personal characteristics | Quantitative Author devised questionnaire; medical records; SF-36 | 57 women with endometriosis. Recruited via hospital/clinic |
| Mathias et al. (1996), USA | To determine the prevalence of chronic pelvic pain in US women aged 18–50 and to examine its association with health-related QoL, work productivity and healthcare utilization | Quantitative Author devised telephone administered questionnaire, including section based on MOS | 773 women with pelvic pain of which 74 had endometriosis. Recruited via research company |
| Nnoaham et al. (2011), cross country | To assess the impact of endometriosis on health-related QoL and work productivity | Quantitative Author devised questionnaire; SF-36; WPAI | 1418 women of which 745 had endometriosis. Recruited via hospital/clinic |
| Petrelluzzi et al. (2008), Brazil | To evaluate the perceived stress index, QoL and hypothalamus–pituitary–adrenal axis activity in women with endometriosis and chronic pelvic pain | Quantitative Pain VAS; SF-36; PSQ; salivary cortisol concentrations | 175 women of which 93 had endometriosis. Recruited via hospital/clinic |
| Peveler et al. (1996), UK | To compare the groups of laparoscopy-negative pelvic pain patients and patients with laparoscopically confirmed endometriosis, using measures of mood, personality and social adjustment; to investigate further the relative importance of psychological and social factors in such patients | Quantitative Pain index measure; pain VAS; BSI; EPQ; SAS | 91 women of which 40 had endometriosis. Recruited via hospital/clinic |
| Roth et al. (2011), USA | To compare women with chronic pelvic pain from endometriosis with those with chronic pelvic pain from other reasons to determine if there are any psychological variables uniquely associated with endometriosis | Quantitative Clinic devised questionnaire; BDI; BSI; MPQ; PDI | 138 women of which 30 had endometriosis. Recruited via hospital/clinic |
| Seear (2009a), Australia | No explicit study aim or research question, but focuses on factors associated with delayed diagnosis of endometriosis | Qualitative Interviews | 20 women with endometriosis. Recruited via support group and snowballing |
| Seear (2009b), Australia | To explore the experiences of women living with endometriosis; to examine how women become experts in their own care and the ramifications of these processes for women | Qualitative Interviews | 20 women with endometriosis. Recruited via support group and snowballing |
| Seear (2009c), Australia | To examine the phenomenon of non-compliance with health advice among women diagnosed with endometriosis | Qualitative Interviews | 20 women with endometriosis. Recruitment route not stated |
| Sepulcri and do Amaral, (2009), Brazil | To assess depressive symptoms, anxiety and QoL in women with pelvic endometriosis | Quantitative Author devised questionnaire; pain VAS; BDI; HAM-D; STAI; HAM-A; WHOQOL-BREF | 104 women with endometriosis. Recruited via hospital/clinic |
| Siedentopf et al. (2008), Germany | To identify if (i) psychosocial factors differ in endometriosis; (ii) related psychosocial aspects alter immune markers of depression/sickness behaviour and (iii) serum immune marker may be indicative for endometriosis (last two aims not included in review) | Quantitative Blood tests; ADS; SF-36; adapted PSQ; F-SoZU | 69 women of which 38 had endometriosis. Recruited via hospital/clinic |
| Simoens et al. (2012), cross country | To calculate the costs and health-related QoL of women with endometriosis-associated symptoms | Quantitative Author devised questionnaire; WPAI; EuroQol-5D | 909 women with endometriosis. Recruited via hospital/clinic |
| Souza et al. (2011), Brazil | To compare the QoL in patients with chronic pelvic pain due to endometriosis or other reasons | Quantitative WHOQOL-BREF; Pain VAS; HARS; BDI | 57 women with pelvic pain of which 32 had endometriosis. Recruited via hospital/clinic |
| Tripoli et al. (2011), Brazil | To evaluate the QoL of women with chronic pelvic pain with and without endometriosis | Quantitative WHOQOL-BREF; GRISS | 134 women of which 49 had endometriosis. Recruited via hospital/clinic |
| Waller and Shaw (1995), UK | To investigate whether there are psychological differences between women with symptomatic as opposed to asymptomatic mild endometriosis | Quantitative Author devised questionnaire; BDI; STAI; GRISS | 117 women of which 49 had endometriosis. Recruited via hospital/clinic |
| Whelan (2007), Canada (analysis), cross country (participants) | To analyse the epistemological strategies and standards used by members of an endometriosis patient community | Qualitative Focus groups and survey | 24 women with endometriosis. Recruited via support group and online community |
| Authors, year of publication, country of analysis and participants (if different) | Study aim/research question | Research design and methods | Sample |
|---|---|---|---|
| Ballard et al. (2006), UK | To investigate the possible reasons for a delayed diagnosis of endometriosis and the impact of delay on women's experiences of endometriosis | Qualitative Interviews | 28 women with suspected or confirmed endometriosis. Recruited via hospital/clinic |
| Bernuit et al. (2011), Germany (analysis), cross country (participants) | To elucidate the differences in diagnoses and treatment experiences of women and to assess the impact of endometriosis on their QoL | Quantitative Author devised online survey | 21 749 women of which 5.1% had surgically or non-surgically diagnosed endometriosis. Recruited via online market research company |
| Butt and Chesla (2007), USA | To investigate the responses in couples' relationships to living with chronic pelvic pain from endometriosis | Qualitative Interviews | 13 women with endometriosis and 13 male partners of women with endometriosis. Recruited via hospital/clinic and support group |
| Chene et al. (2012), France | To compare pain symptoms and the QoL between epiphenomenon and endometriosis disease | Quantitative Author devised questionnaire; SF-36; simplified sexual satisfaction Subscale of the DSFI; pain VAS | 437 women with endometriosis. Recruited via hospital/clinic |
| Christian (1993), USA | To determine the relationship between women's symptoms of endometriosis and self-esteem | Quantitative Author devised questionnaire; RSES | 23 women with endometriosis. Recruited via hospital/clinic |
| Cox et al. (2003a), Australia | To identify the information and support needs of women with endometriosis | Mixed Author devised questionnaire | 465 women with endometriosis. Recruited via hospital/clinic and support group |
| Cox et al. (2003b), Australia | To identify information needs of women facing laparoscopy for endometriosis | Qualitative Focus groups | 61 women with endometriosis. Recruited via hospital/clinic and support group |
| Cox et al. (2003c), Australia | To determine women's needs for information related to laparoscopy for endometriosis | Mixed Author devised questionnaire and focus groups | 61 women with endometriosis. Recruitment route not stated |
| Denny (2004a), UK | To explore women's experiences of living with endometriosis | Qualitative Interviews | 15 women with endometriosis. Recruited via hospital/clinic, support group and snowballing |
| Denny (2004b), UK | To explore women's experiences of living with the pain of endometriosis and examine delay in the diagnosis of the disease | Qualitative Interviews | 20 women with endometriosis. Recruited via hospital/clinic, support group and snowballing |
| Denny (2009), UK | To explore women's experiences of living with endometriosis in a prospective study over a 1-year period | Qualitative Interviews and diaries | 30 women with endometriosis. Recruited via hospital/clinic |
| Denny and Mann (2007), UK | To determine how much of an impact endometriosis-associated dyspareunia has on the lives and relationships of women | Mixed Interviews | 30 women with endometriosis. Recruited via hospital/clinic |
| Denny and Mann (2008), UK | To elicit the experience of endometriosis and the impact on women's lives; to explore the experience of women with endometriosis in the primary care setting | Qualitative Interviews | 30 women with endometriosis. Recruited via hospital/clinic |
| Eriksen et al. (2008), Denmark | To compare patients with endometriosis with and without pain symptoms to see if they differed on four psychological parameters (coping, emotional inhibition, depression and anxiety); to examine the effects of pain caused by endometriosis on psychosocial functioning | Quantitative Author devised questionnaire; CSQ; CECS; BDI; State Anxiety Scale of the STAI | 63 women with endometriosis. Recruited via hospital/clinic. |
| Fagervold et al. (2009), Norway | To investigate longitudinally the consequences of endometriosis in women diagnosed with the disease 15 years ago. | Quantitative Author devised questionnaire | 78 women with endometriosis. Recruited via hospital/clinic |
| Ferrero et al. (2005), Italy | To characterize the sexual function in women with endometriosis and deep dyspareunia | Quantitative Adapted sexual satisfaction Subscale of the DSFI; GSSI; VAS | 136 women of which 96 had endometriosis. Recruited via hospital/clinic |
| Fourquet et al. (2011), Puerto Rico | To quantify the impact of endometriosis-related symptoms on physical and mental health status, health-related QoL and work-related aspects | Quantitative SF-12; EHP-5; WPAI | 193 women with endometriosis. Recruited via Endometriosis Research Programme |
| Fourquet et al. (2010), Puerto Rico | To assess the burden of endometriosis by obtaining patient-reported outcome data describing the experience of living with endometriosis | Quantitative Author devised questionnaire | 107 women with endometriosis. Recruited via Endometriosis Research Programme |
| Gilmour et al. (2008), New Zealand | To explore the impact of symptomatic endometriosis on women's social and working lives | Qualitative Interviews | 18 women with endometriosis. Recruited via support group |
| Huntington and Gilmour (2005), New Zealand | To explore women's perceptions of living with endometriosis, its effects on their lives and the strategies used to manage their disease | Qualitative Interviews | 18 women with endometriosis. Recruited via support group |
| Jones et al. (2004), UK | To explore and describe the impact of endometriosis upon QoL; to identify and understand, from the patient's perspective, the areas of health-related QoL that are affected by endometriosis and to address the benefits of using a qualitative methodology for item generation in the development of disease-specific health status questionnaires | Qualitative Interviews | 24 women with endometriosis. Recruited via hospital/clinic |
| Lemaire (2004), USA | To examine the frequency, severity, interference with daily life and symptom distress associated with endometriosis and to explore the relationships among symptoms, emotional distress, uncertainty and a preference for and adequacy of information | Quantitative Author devised questionnaire; MUIS-C; adapted HOSI | 298 women with endometriosis. Recruited via support group |
| Lorençatto et al. (2006), Brazil | To compare the prevalence of depression in women with endometriosis according to the presence or absence of pelvic pain | Quantitative BDI | 100 women with endometriosis. Recruited via hospital/clinic |
| Low et al. (1993), UK | To investigate the possibility of a specific psychological profile associated with endometriosis | Quantitative Author devised questionnaire; EPQ; BDI; GHQ 30; STAI; GRIMS; SF-MPQ | 81 women of which 40 had endometriosis. Recruited via hospital/clinic |
| Manderson et al. (2008), Australia | To explore whether and how women's experience of gynaecological or reproductive health problems or conditions impacted their gendered, social and personal identities | Qualitative Interviews | 40 women of which 25 had endometriosis. Recruited via community newsletter and snowballing |
| Markovic et al. (2008), Australia | To explore the influence of socio-demographic background and social and family norms on the illness narratives of endurance and contest among women with endometriosis | Qualitative Interviews | 30 women with endometriosis. Recruited via community newsletter and snowballing |
| Marques et al. (2004), Brazil | To assess the QoL in women with chronic pelvic pain associated with endometriosis and to correlate QoL with personal characteristics | Quantitative Author devised questionnaire; medical records; SF-36 | 57 women with endometriosis. Recruited via hospital/clinic |
| Mathias et al. (1996), USA | To determine the prevalence of chronic pelvic pain in US women aged 18–50 and to examine its association with health-related QoL, work productivity and healthcare utilization | Quantitative Author devised telephone administered questionnaire, including section based on MOS | 773 women with pelvic pain of which 74 had endometriosis. Recruited via research company |
| Nnoaham et al. (2011), cross country | To assess the impact of endometriosis on health-related QoL and work productivity | Quantitative Author devised questionnaire; SF-36; WPAI | 1418 women of which 745 had endometriosis. Recruited via hospital/clinic |
| Petrelluzzi et al. (2008), Brazil | To evaluate the perceived stress index, QoL and hypothalamus–pituitary–adrenal axis activity in women with endometriosis and chronic pelvic pain | Quantitative Pain VAS; SF-36; PSQ; salivary cortisol concentrations | 175 women of which 93 had endometriosis. Recruited via hospital/clinic |
| Peveler et al. (1996), UK | To compare the groups of laparoscopy-negative pelvic pain patients and patients with laparoscopically confirmed endometriosis, using measures of mood, personality and social adjustment; to investigate further the relative importance of psychological and social factors in such patients | Quantitative Pain index measure; pain VAS; BSI; EPQ; SAS | 91 women of which 40 had endometriosis. Recruited via hospital/clinic |
| Roth et al. (2011), USA | To compare women with chronic pelvic pain from endometriosis with those with chronic pelvic pain from other reasons to determine if there are any psychological variables uniquely associated with endometriosis | Quantitative Clinic devised questionnaire; BDI; BSI; MPQ; PDI | 138 women of which 30 had endometriosis. Recruited via hospital/clinic |
| Seear (2009a), Australia | No explicit study aim or research question, but focuses on factors associated with delayed diagnosis of endometriosis | Qualitative Interviews | 20 women with endometriosis. Recruited via support group and snowballing |
| Seear (2009b), Australia | To explore the experiences of women living with endometriosis; to examine how women become experts in their own care and the ramifications of these processes for women | Qualitative Interviews | 20 women with endometriosis. Recruited via support group and snowballing |
| Seear (2009c), Australia | To examine the phenomenon of non-compliance with health advice among women diagnosed with endometriosis | Qualitative Interviews | 20 women with endometriosis. Recruitment route not stated |
| Sepulcri and do Amaral, (2009), Brazil | To assess depressive symptoms, anxiety and QoL in women with pelvic endometriosis | Quantitative Author devised questionnaire; pain VAS; BDI; HAM-D; STAI; HAM-A; WHOQOL-BREF | 104 women with endometriosis. Recruited via hospital/clinic |
| Siedentopf et al. (2008), Germany | To identify if (i) psychosocial factors differ in endometriosis; (ii) related psychosocial aspects alter immune markers of depression/sickness behaviour and (iii) serum immune marker may be indicative for endometriosis (last two aims not included in review) | Quantitative Blood tests; ADS; SF-36; adapted PSQ; F-SoZU | 69 women of which 38 had endometriosis. Recruited via hospital/clinic |
| Simoens et al. (2012), cross country | To calculate the costs and health-related QoL of women with endometriosis-associated symptoms | Quantitative Author devised questionnaire; WPAI; EuroQol-5D | 909 women with endometriosis. Recruited via hospital/clinic |
| Souza et al. (2011), Brazil | To compare the QoL in patients with chronic pelvic pain due to endometriosis or other reasons | Quantitative WHOQOL-BREF; Pain VAS; HARS; BDI | 57 women with pelvic pain of which 32 had endometriosis. Recruited via hospital/clinic |
| Tripoli et al. (2011), Brazil | To evaluate the QoL of women with chronic pelvic pain with and without endometriosis | Quantitative WHOQOL-BREF; GRISS | 134 women of which 49 had endometriosis. Recruited via hospital/clinic |
| Waller and Shaw (1995), UK | To investigate whether there are psychological differences between women with symptomatic as opposed to asymptomatic mild endometriosis | Quantitative Author devised questionnaire; BDI; STAI; GRISS | 117 women of which 49 had endometriosis. Recruited via hospital/clinic |
| Whelan (2007), Canada (analysis), cross country (participants) | To analyse the epistemological strategies and standards used by members of an endometriosis patient community | Qualitative Focus groups and survey | 24 women with endometriosis. Recruited via support group and online community |
ADS, Allgemeine Depressionsskala, general depression scale; BDI, Beck Depression Inventory; BSI, Brief Symptom Inventory; CSQ, Coping Styles Questionnaire; CECS, Courthald Emotional Control Scale; DFSI, Derogatis Sexual Functioning Inventory; EHP, Endometriosis Health Profile; EPQ, Eyesenck Personality Questionnaire; EuroQol-5D, Health-related quality of life measure; F-SoZU, Fragebogen zur sozialen Unterstü tzung (measuring social support); GHQ, General Health Questionnaire; GRIMS, Golombok Rust Inventory of Marital State; GRISS, Golombok Rust Inventory of Sexual Satisfaction; GSSI, Global Sexual Satisfaction Inventory; HAM-A, Hamilton Rating Scale for Anxiety; HAM-D, Hamilton Rating Scale for Depression; HARS, Hamilton Anxiety Rating Scale; HOSI, Krantz Health Opinion Survey, Information Subscale; MOS, Medical Outcomes Study; MPQ, McGill Pain Questionnaire; MUIS-C, Mischel Uncertainty in Illness Scale-Community Form; PDI, Pain Disability Index; PSQ, Perceived Stress Questionnaire; RSES, Rosenberg Self-Esteem Scale; SAS, Social Adjustment Scale; SF, Short Form Health Survey; SF-MPQ, Short Form McGill Pain; STAI, State-Trait Anxiety Inventory; VAS, visual analogue scale; WHOQOL-BREF, World Health Organization Quality of Life instrument short version; WPAI, Work Productivity and Activity Impairment Survey.
Paper characteristics.
| Authors, year of publication, country of analysis and participants (if different) | Study aim/research question | Research design and methods | Sample |
|---|---|---|---|
| Ballard et al. (2006), UK | To investigate the possible reasons for a delayed diagnosis of endometriosis and the impact of delay on women's experiences of endometriosis | Qualitative Interviews | 28 women with suspected or confirmed endometriosis. Recruited via hospital/clinic |
| Bernuit et al. (2011), Germany (analysis), cross country (participants) | To elucidate the differences in diagnoses and treatment experiences of women and to assess the impact of endometriosis on their QoL | Quantitative Author devised online survey | 21 749 women of which 5.1% had surgically or non-surgically diagnosed endometriosis. Recruited via online market research company |
| Butt and Chesla (2007), USA | To investigate the responses in couples' relationships to living with chronic pelvic pain from endometriosis | Qualitative Interviews | 13 women with endometriosis and 13 male partners of women with endometriosis. Recruited via hospital/clinic and support group |
| Chene et al. (2012), France | To compare pain symptoms and the QoL between epiphenomenon and endometriosis disease | Quantitative Author devised questionnaire; SF-36; simplified sexual satisfaction Subscale of the DSFI; pain VAS | 437 women with endometriosis. Recruited via hospital/clinic |
| Christian (1993), USA | To determine the relationship between women's symptoms of endometriosis and self-esteem | Quantitative Author devised questionnaire; RSES | 23 women with endometriosis. Recruited via hospital/clinic |
| Cox et al. (2003a), Australia | To identify the information and support needs of women with endometriosis | Mixed Author devised questionnaire | 465 women with endometriosis. Recruited via hospital/clinic and support group |
| Cox et al. (2003b), Australia | To identify information needs of women facing laparoscopy for endometriosis | Qualitative Focus groups | 61 women with endometriosis. Recruited via hospital/clinic and support group |
| Cox et al. (2003c), Australia | To determine women's needs for information related to laparoscopy for endometriosis | Mixed Author devised questionnaire and focus groups | 61 women with endometriosis. Recruitment route not stated |
| Denny (2004a), UK | To explore women's experiences of living with endometriosis | Qualitative Interviews | 15 women with endometriosis. Recruited via hospital/clinic, support group and snowballing |
| Denny (2004b), UK | To explore women's experiences of living with the pain of endometriosis and examine delay in the diagnosis of the disease | Qualitative Interviews | 20 women with endometriosis. Recruited via hospital/clinic, support group and snowballing |
| Denny (2009), UK | To explore women's experiences of living with endometriosis in a prospective study over a 1-year period | Qualitative Interviews and diaries | 30 women with endometriosis. Recruited via hospital/clinic |
| Denny and Mann (2007), UK | To determine how much of an impact endometriosis-associated dyspareunia has on the lives and relationships of women | Mixed Interviews | 30 women with endometriosis. Recruited via hospital/clinic |
| Denny and Mann (2008), UK | To elicit the experience of endometriosis and the impact on women's lives; to explore the experience of women with endometriosis in the primary care setting | Qualitative Interviews | 30 women with endometriosis. Recruited via hospital/clinic |
| Eriksen et al. (2008), Denmark | To compare patients with endometriosis with and without pain symptoms to see if they differed on four psychological parameters (coping, emotional inhibition, depression and anxiety); to examine the effects of pain caused by endometriosis on psychosocial functioning | Quantitative Author devised questionnaire; CSQ; CECS; BDI; State Anxiety Scale of the STAI | 63 women with endometriosis. Recruited via hospital/clinic. |
| Fagervold et al. (2009), Norway | To investigate longitudinally the consequences of endometriosis in women diagnosed with the disease 15 years ago. | Quantitative Author devised questionnaire | 78 women with endometriosis. Recruited via hospital/clinic |
| Ferrero et al. (2005), Italy | To characterize the sexual function in women with endometriosis and deep dyspareunia | Quantitative Adapted sexual satisfaction Subscale of the DSFI; GSSI; VAS | 136 women of which 96 had endometriosis. Recruited via hospital/clinic |
| Fourquet et al. (2011), Puerto Rico | To quantify the impact of endometriosis-related symptoms on physical and mental health status, health-related QoL and work-related aspects | Quantitative SF-12; EHP-5; WPAI | 193 women with endometriosis. Recruited via Endometriosis Research Programme |
| Fourquet et al. (2010), Puerto Rico | To assess the burden of endometriosis by obtaining patient-reported outcome data describing the experience of living with endometriosis | Quantitative Author devised questionnaire | 107 women with endometriosis. Recruited via Endometriosis Research Programme |
| Gilmour et al. (2008), New Zealand | To explore the impact of symptomatic endometriosis on women's social and working lives | Qualitative Interviews | 18 women with endometriosis. Recruited via support group |
| Huntington and Gilmour (2005), New Zealand | To explore women's perceptions of living with endometriosis, its effects on their lives and the strategies used to manage their disease | Qualitative Interviews | 18 women with endometriosis. Recruited via support group |
| Jones et al. (2004), UK | To explore and describe the impact of endometriosis upon QoL; to identify and understand, from the patient's perspective, the areas of health-related QoL that are affected by endometriosis and to address the benefits of using a qualitative methodology for item generation in the development of disease-specific health status questionnaires | Qualitative Interviews | 24 women with endometriosis. Recruited via hospital/clinic |
| Lemaire (2004), USA | To examine the frequency, severity, interference with daily life and symptom distress associated with endometriosis and to explore the relationships among symptoms, emotional distress, uncertainty and a preference for and adequacy of information | Quantitative Author devised questionnaire; MUIS-C; adapted HOSI | 298 women with endometriosis. Recruited via support group |
| Lorençatto et al. (2006), Brazil | To compare the prevalence of depression in women with endometriosis according to the presence or absence of pelvic pain | Quantitative BDI | 100 women with endometriosis. Recruited via hospital/clinic |
| Low et al. (1993), UK | To investigate the possibility of a specific psychological profile associated with endometriosis | Quantitative Author devised questionnaire; EPQ; BDI; GHQ 30; STAI; GRIMS; SF-MPQ | 81 women of which 40 had endometriosis. Recruited via hospital/clinic |
| Manderson et al. (2008), Australia | To explore whether and how women's experience of gynaecological or reproductive health problems or conditions impacted their gendered, social and personal identities | Qualitative Interviews | 40 women of which 25 had endometriosis. Recruited via community newsletter and snowballing |
| Markovic et al. (2008), Australia | To explore the influence of socio-demographic background and social and family norms on the illness narratives of endurance and contest among women with endometriosis | Qualitative Interviews | 30 women with endometriosis. Recruited via community newsletter and snowballing |
| Marques et al. (2004), Brazil | To assess the QoL in women with chronic pelvic pain associated with endometriosis and to correlate QoL with personal characteristics | Quantitative Author devised questionnaire; medical records; SF-36 | 57 women with endometriosis. Recruited via hospital/clinic |
| Mathias et al. (1996), USA | To determine the prevalence of chronic pelvic pain in US women aged 18–50 and to examine its association with health-related QoL, work productivity and healthcare utilization | Quantitative Author devised telephone administered questionnaire, including section based on MOS | 773 women with pelvic pain of which 74 had endometriosis. Recruited via research company |
| Nnoaham et al. (2011), cross country | To assess the impact of endometriosis on health-related QoL and work productivity | Quantitative Author devised questionnaire; SF-36; WPAI | 1418 women of which 745 had endometriosis. Recruited via hospital/clinic |
| Petrelluzzi et al. (2008), Brazil | To evaluate the perceived stress index, QoL and hypothalamus–pituitary–adrenal axis activity in women with endometriosis and chronic pelvic pain | Quantitative Pain VAS; SF-36; PSQ; salivary cortisol concentrations | 175 women of which 93 had endometriosis. Recruited via hospital/clinic |
| Peveler et al. (1996), UK | To compare the groups of laparoscopy-negative pelvic pain patients and patients with laparoscopically confirmed endometriosis, using measures of mood, personality and social adjustment; to investigate further the relative importance of psychological and social factors in such patients | Quantitative Pain index measure; pain VAS; BSI; EPQ; SAS | 91 women of which 40 had endometriosis. Recruited via hospital/clinic |
| Roth et al. (2011), USA | To compare women with chronic pelvic pain from endometriosis with those with chronic pelvic pain from other reasons to determine if there are any psychological variables uniquely associated with endometriosis | Quantitative Clinic devised questionnaire; BDI; BSI; MPQ; PDI | 138 women of which 30 had endometriosis. Recruited via hospital/clinic |
| Seear (2009a), Australia | No explicit study aim or research question, but focuses on factors associated with delayed diagnosis of endometriosis | Qualitative Interviews | 20 women with endometriosis. Recruited via support group and snowballing |
| Seear (2009b), Australia | To explore the experiences of women living with endometriosis; to examine how women become experts in their own care and the ramifications of these processes for women | Qualitative Interviews | 20 women with endometriosis. Recruited via support group and snowballing |
| Seear (2009c), Australia | To examine the phenomenon of non-compliance with health advice among women diagnosed with endometriosis | Qualitative Interviews | 20 women with endometriosis. Recruitment route not stated |
| Sepulcri and do Amaral, (2009), Brazil | To assess depressive symptoms, anxiety and QoL in women with pelvic endometriosis | Quantitative Author devised questionnaire; pain VAS; BDI; HAM-D; STAI; HAM-A; WHOQOL-BREF | 104 women with endometriosis. Recruited via hospital/clinic |
| Siedentopf et al. (2008), Germany | To identify if (i) psychosocial factors differ in endometriosis; (ii) related psychosocial aspects alter immune markers of depression/sickness behaviour and (iii) serum immune marker may be indicative for endometriosis (last two aims not included in review) | Quantitative Blood tests; ADS; SF-36; adapted PSQ; F-SoZU | 69 women of which 38 had endometriosis. Recruited via hospital/clinic |
| Simoens et al. (2012), cross country | To calculate the costs and health-related QoL of women with endometriosis-associated symptoms | Quantitative Author devised questionnaire; WPAI; EuroQol-5D | 909 women with endometriosis. Recruited via hospital/clinic |
| Souza et al. (2011), Brazil | To compare the QoL in patients with chronic pelvic pain due to endometriosis or other reasons | Quantitative WHOQOL-BREF; Pain VAS; HARS; BDI | 57 women with pelvic pain of which 32 had endometriosis. Recruited via hospital/clinic |
| Tripoli et al. (2011), Brazil | To evaluate the QoL of women with chronic pelvic pain with and without endometriosis | Quantitative WHOQOL-BREF; GRISS | 134 women of which 49 had endometriosis. Recruited via hospital/clinic |
| Waller and Shaw (1995), UK | To investigate whether there are psychological differences between women with symptomatic as opposed to asymptomatic mild endometriosis | Quantitative Author devised questionnaire; BDI; STAI; GRISS | 117 women of which 49 had endometriosis. Recruited via hospital/clinic |
| Whelan (2007), Canada (analysis), cross country (participants) | To analyse the epistemological strategies and standards used by members of an endometriosis patient community | Qualitative Focus groups and survey | 24 women with endometriosis. Recruited via support group and online community |
| Authors, year of publication, country of analysis and participants (if different) | Study aim/research question | Research design and methods | Sample |
|---|---|---|---|
| Ballard et al. (2006), UK | To investigate the possible reasons for a delayed diagnosis of endometriosis and the impact of delay on women's experiences of endometriosis | Qualitative Interviews | 28 women with suspected or confirmed endometriosis. Recruited via hospital/clinic |
| Bernuit et al. (2011), Germany (analysis), cross country (participants) | To elucidate the differences in diagnoses and treatment experiences of women and to assess the impact of endometriosis on their QoL | Quantitative Author devised online survey | 21 749 women of which 5.1% had surgically or non-surgically diagnosed endometriosis. Recruited via online market research company |
| Butt and Chesla (2007), USA | To investigate the responses in couples' relationships to living with chronic pelvic pain from endometriosis | Qualitative Interviews | 13 women with endometriosis and 13 male partners of women with endometriosis. Recruited via hospital/clinic and support group |
| Chene et al. (2012), France | To compare pain symptoms and the QoL between epiphenomenon and endometriosis disease | Quantitative Author devised questionnaire; SF-36; simplified sexual satisfaction Subscale of the DSFI; pain VAS | 437 women with endometriosis. Recruited via hospital/clinic |
| Christian (1993), USA | To determine the relationship between women's symptoms of endometriosis and self-esteem | Quantitative Author devised questionnaire; RSES | 23 women with endometriosis. Recruited via hospital/clinic |
| Cox et al. (2003a), Australia | To identify the information and support needs of women with endometriosis | Mixed Author devised questionnaire | 465 women with endometriosis. Recruited via hospital/clinic and support group |
| Cox et al. (2003b), Australia | To identify information needs of women facing laparoscopy for endometriosis | Qualitative Focus groups | 61 women with endometriosis. Recruited via hospital/clinic and support group |
| Cox et al. (2003c), Australia | To determine women's needs for information related to laparoscopy for endometriosis | Mixed Author devised questionnaire and focus groups | 61 women with endometriosis. Recruitment route not stated |
| Denny (2004a), UK | To explore women's experiences of living with endometriosis | Qualitative Interviews | 15 women with endometriosis. Recruited via hospital/clinic, support group and snowballing |
| Denny (2004b), UK | To explore women's experiences of living with the pain of endometriosis and examine delay in the diagnosis of the disease | Qualitative Interviews | 20 women with endometriosis. Recruited via hospital/clinic, support group and snowballing |
| Denny (2009), UK | To explore women's experiences of living with endometriosis in a prospective study over a 1-year period | Qualitative Interviews and diaries | 30 women with endometriosis. Recruited via hospital/clinic |
| Denny and Mann (2007), UK | To determine how much of an impact endometriosis-associated dyspareunia has on the lives and relationships of women | Mixed Interviews | 30 women with endometriosis. Recruited via hospital/clinic |
| Denny and Mann (2008), UK | To elicit the experience of endometriosis and the impact on women's lives; to explore the experience of women with endometriosis in the primary care setting | Qualitative Interviews | 30 women with endometriosis. Recruited via hospital/clinic |
| Eriksen et al. (2008), Denmark | To compare patients with endometriosis with and without pain symptoms to see if they differed on four psychological parameters (coping, emotional inhibition, depression and anxiety); to examine the effects of pain caused by endometriosis on psychosocial functioning | Quantitative Author devised questionnaire; CSQ; CECS; BDI; State Anxiety Scale of the STAI | 63 women with endometriosis. Recruited via hospital/clinic. |
| Fagervold et al. (2009), Norway | To investigate longitudinally the consequences of endometriosis in women diagnosed with the disease 15 years ago. | Quantitative Author devised questionnaire | 78 women with endometriosis. Recruited via hospital/clinic |
| Ferrero et al. (2005), Italy | To characterize the sexual function in women with endometriosis and deep dyspareunia | Quantitative Adapted sexual satisfaction Subscale of the DSFI; GSSI; VAS | 136 women of which 96 had endometriosis. Recruited via hospital/clinic |
| Fourquet et al. (2011), Puerto Rico | To quantify the impact of endometriosis-related symptoms on physical and mental health status, health-related QoL and work-related aspects | Quantitative SF-12; EHP-5; WPAI | 193 women with endometriosis. Recruited via Endometriosis Research Programme |
| Fourquet et al. (2010), Puerto Rico | To assess the burden of endometriosis by obtaining patient-reported outcome data describing the experience of living with endometriosis | Quantitative Author devised questionnaire | 107 women with endometriosis. Recruited via Endometriosis Research Programme |
| Gilmour et al. (2008), New Zealand | To explore the impact of symptomatic endometriosis on women's social and working lives | Qualitative Interviews | 18 women with endometriosis. Recruited via support group |
| Huntington and Gilmour (2005), New Zealand | To explore women's perceptions of living with endometriosis, its effects on their lives and the strategies used to manage their disease | Qualitative Interviews | 18 women with endometriosis. Recruited via support group |
| Jones et al. (2004), UK | To explore and describe the impact of endometriosis upon QoL; to identify and understand, from the patient's perspective, the areas of health-related QoL that are affected by endometriosis and to address the benefits of using a qualitative methodology for item generation in the development of disease-specific health status questionnaires | Qualitative Interviews | 24 women with endometriosis. Recruited via hospital/clinic |
| Lemaire (2004), USA | To examine the frequency, severity, interference with daily life and symptom distress associated with endometriosis and to explore the relationships among symptoms, emotional distress, uncertainty and a preference for and adequacy of information | Quantitative Author devised questionnaire; MUIS-C; adapted HOSI | 298 women with endometriosis. Recruited via support group |
| Lorençatto et al. (2006), Brazil | To compare the prevalence of depression in women with endometriosis according to the presence or absence of pelvic pain | Quantitative BDI | 100 women with endometriosis. Recruited via hospital/clinic |
| Low et al. (1993), UK | To investigate the possibility of a specific psychological profile associated with endometriosis | Quantitative Author devised questionnaire; EPQ; BDI; GHQ 30; STAI; GRIMS; SF-MPQ | 81 women of which 40 had endometriosis. Recruited via hospital/clinic |
| Manderson et al. (2008), Australia | To explore whether and how women's experience of gynaecological or reproductive health problems or conditions impacted their gendered, social and personal identities | Qualitative Interviews | 40 women of which 25 had endometriosis. Recruited via community newsletter and snowballing |
| Markovic et al. (2008), Australia | To explore the influence of socio-demographic background and social and family norms on the illness narratives of endurance and contest among women with endometriosis | Qualitative Interviews | 30 women with endometriosis. Recruited via community newsletter and snowballing |
| Marques et al. (2004), Brazil | To assess the QoL in women with chronic pelvic pain associated with endometriosis and to correlate QoL with personal characteristics | Quantitative Author devised questionnaire; medical records; SF-36 | 57 women with endometriosis. Recruited via hospital/clinic |
| Mathias et al. (1996), USA | To determine the prevalence of chronic pelvic pain in US women aged 18–50 and to examine its association with health-related QoL, work productivity and healthcare utilization | Quantitative Author devised telephone administered questionnaire, including section based on MOS | 773 women with pelvic pain of which 74 had endometriosis. Recruited via research company |
| Nnoaham et al. (2011), cross country | To assess the impact of endometriosis on health-related QoL and work productivity | Quantitative Author devised questionnaire; SF-36; WPAI | 1418 women of which 745 had endometriosis. Recruited via hospital/clinic |
| Petrelluzzi et al. (2008), Brazil | To evaluate the perceived stress index, QoL and hypothalamus–pituitary–adrenal axis activity in women with endometriosis and chronic pelvic pain | Quantitative Pain VAS; SF-36; PSQ; salivary cortisol concentrations | 175 women of which 93 had endometriosis. Recruited via hospital/clinic |
| Peveler et al. (1996), UK | To compare the groups of laparoscopy-negative pelvic pain patients and patients with laparoscopically confirmed endometriosis, using measures of mood, personality and social adjustment; to investigate further the relative importance of psychological and social factors in such patients | Quantitative Pain index measure; pain VAS; BSI; EPQ; SAS | 91 women of which 40 had endometriosis. Recruited via hospital/clinic |
| Roth et al. (2011), USA | To compare women with chronic pelvic pain from endometriosis with those with chronic pelvic pain from other reasons to determine if there are any psychological variables uniquely associated with endometriosis | Quantitative Clinic devised questionnaire; BDI; BSI; MPQ; PDI | 138 women of which 30 had endometriosis. Recruited via hospital/clinic |
| Seear (2009a), Australia | No explicit study aim or research question, but focuses on factors associated with delayed diagnosis of endometriosis | Qualitative Interviews | 20 women with endometriosis. Recruited via support group and snowballing |
| Seear (2009b), Australia | To explore the experiences of women living with endometriosis; to examine how women become experts in their own care and the ramifications of these processes for women | Qualitative Interviews | 20 women with endometriosis. Recruited via support group and snowballing |
| Seear (2009c), Australia | To examine the phenomenon of non-compliance with health advice among women diagnosed with endometriosis | Qualitative Interviews | 20 women with endometriosis. Recruitment route not stated |
| Sepulcri and do Amaral, (2009), Brazil | To assess depressive symptoms, anxiety and QoL in women with pelvic endometriosis | Quantitative Author devised questionnaire; pain VAS; BDI; HAM-D; STAI; HAM-A; WHOQOL-BREF | 104 women with endometriosis. Recruited via hospital/clinic |
| Siedentopf et al. (2008), Germany | To identify if (i) psychosocial factors differ in endometriosis; (ii) related psychosocial aspects alter immune markers of depression/sickness behaviour and (iii) serum immune marker may be indicative for endometriosis (last two aims not included in review) | Quantitative Blood tests; ADS; SF-36; adapted PSQ; F-SoZU | 69 women of which 38 had endometriosis. Recruited via hospital/clinic |
| Simoens et al. (2012), cross country | To calculate the costs and health-related QoL of women with endometriosis-associated symptoms | Quantitative Author devised questionnaire; WPAI; EuroQol-5D | 909 women with endometriosis. Recruited via hospital/clinic |
| Souza et al. (2011), Brazil | To compare the QoL in patients with chronic pelvic pain due to endometriosis or other reasons | Quantitative WHOQOL-BREF; Pain VAS; HARS; BDI | 57 women with pelvic pain of which 32 had endometriosis. Recruited via hospital/clinic |
| Tripoli et al. (2011), Brazil | To evaluate the QoL of women with chronic pelvic pain with and without endometriosis | Quantitative WHOQOL-BREF; GRISS | 134 women of which 49 had endometriosis. Recruited via hospital/clinic |
| Waller and Shaw (1995), UK | To investigate whether there are psychological differences between women with symptomatic as opposed to asymptomatic mild endometriosis | Quantitative Author devised questionnaire; BDI; STAI; GRISS | 117 women of which 49 had endometriosis. Recruited via hospital/clinic |
| Whelan (2007), Canada (analysis), cross country (participants) | To analyse the epistemological strategies and standards used by members of an endometriosis patient community | Qualitative Focus groups and survey | 24 women with endometriosis. Recruited via support group and online community |
ADS, Allgemeine Depressionsskala, general depression scale; BDI, Beck Depression Inventory; BSI, Brief Symptom Inventory; CSQ, Coping Styles Questionnaire; CECS, Courthald Emotional Control Scale; DFSI, Derogatis Sexual Functioning Inventory; EHP, Endometriosis Health Profile; EPQ, Eyesenck Personality Questionnaire; EuroQol-5D, Health-related quality of life measure; F-SoZU, Fragebogen zur sozialen Unterstü tzung (measuring social support); GHQ, General Health Questionnaire; GRIMS, Golombok Rust Inventory of Marital State; GRISS, Golombok Rust Inventory of Sexual Satisfaction; GSSI, Global Sexual Satisfaction Inventory; HAM-A, Hamilton Rating Scale for Anxiety; HAM-D, Hamilton Rating Scale for Depression; HARS, Hamilton Anxiety Rating Scale; HOSI, Krantz Health Opinion Survey, Information Subscale; MOS, Medical Outcomes Study; MPQ, McGill Pain Questionnaire; MUIS-C, Mischel Uncertainty in Illness Scale-Community Form; PDI, Pain Disability Index; PSQ, Perceived Stress Questionnaire; RSES, Rosenberg Self-Esteem Scale; SAS, Social Adjustment Scale; SF, Short Form Health Survey; SF-MPQ, Short Form McGill Pain; STAI, State-Trait Anxiety Inventory; VAS, visual analogue scale; WHOQOL-BREF, World Health Organization Quality of Life instrument short version; WPAI, Work Productivity and Activity Impairment Survey.
Settings
Over half of the papers were published between 2005 and 2010, indicating a recent increase in research on the social and psychological impact of endometriosis. The majority of papers came from just 4 countries: UK (10), Australia (8), Brazil (6) and the USA (5). Of the remaining papers, six were from Western Europe, two from New Zealand, two from Puerto Rica and one from Canada and two papers reported on cross-country studies (Argentina, Belgium, Brazil, China, Ireland, Italy, Nigeria, Spain, UK and USA, Nnoaham et al., 2011; Belgium, Denmark, France, Germany, Hungary, Italy, the Netherlands, Switzerland, UK and USA, Simoens et al., 2012). The majority of papers were therefore from high-income countries with developed healthcare systems. Participants were recruited from single hospitals/clinics (17), multiple hospitals/clinics (6), support groups (3) or from multiple (10) or other (4) settings, or the setting was not stated (2).
Design
Papers reported on quantitative (23), qualitative (16) and mixed methods (3) studies. The majority of papers from the UK and Australia (12 of 18) reported on qualitative studies, whereas the majority of papers from Brazil and the USA (9 of 11) reported on quantitative studies. The quantitative studies used a range of quality of life (QoL) instruments and assessments/inventories of aspects such as symptoms (including pain), wellbeing, mental health, personality, impact on work, etc. Qualitative studies predominantly used interview data collection methods, although a small number collected data via focus groups, questionnaires and diaries. Cross-sectional studies accounted for 40 papers while 2 papers reported longitudinal studies.
Participants
Sample sizes varied considerably: from 23 to ∼1110 women with endometriosis with a mean of 207 in quantitative papers; from 13 to 61 women with endometriosis with a mean of 25 in qualitative papers and from 30 to 465 women with endometriosis with a mean of 185 in mixed methods studies. Most papers reported on studies of women with confirmed (i.e. surgically diagnosed) endometriosis, although in papers where women were recruited via routes other than hospitals and clinics, diagnosis was based on self-report and not clinically verified. Thirteen papers reported on studies with broader samples where women with endometriosis were included as a subset, and where data about women without endometriosis were used for comparison. Only one study included male partners alongside women with endometriosis.
Findings on the social and psychological impact of endometriosis
Key categories identified in the thematic analysis were: diagnostic delay and uncertainty; ‘QoL’ and everyday activities; intimate relationships; planning for and having children; education and work; mental health and wellbeing and medical and self-management. Pain is a significant symptom that arises in all of these categories, and as such the impact of pain is considered throughout the findings.
Diagnostic delay and uncertainty
There were 21 papers (50%; 14 qualitative, 5 quantitative and 2 mixed methods) which reported findings relating to the impact of endometriosis in terms of diagnostic delay or uncertainty. Women with endometriosis frequently experience significant delays from symptom onset to diagnosis (Cox et al., 2003a; Denny, 2004a, b; Denny and Mann, 2008; Sepulcri and do Amaral, 2009; Fourquet et al., 2010; Bernuit et al., 2011; Nnoaham et al., 2011), ranging from 5 (Sepulcri and do Amaral, 2009) to 8.9 years (Fourquet et al., 2010). Diagnostic delays have been shown to be associated with reduced health-related QoL (Nnoaham et al., 2011). It is useful, therefore, to outline the findings regarding delayed diagnosis. The authors have distinguished between delays at the patient level and delays at the medical level (Ballard et al., 2006).
Diagnostic delay: factors at the patient level
The delay at the patient level refers to the time between symptom onset and seeking medical help. Cox et al. (2003a, b) identified an average delay of 3.8 years between symptom onset and help-seeking behaviour. It is suggested that women fail to seek medical help due to difficulty in distinguishing between normal and pathological symptoms; because they consider themselves ‘unlucky’ as opposed to ‘unwell’ and because they fear that disclosure would result in embarrassment and in them being perceived as weak (Cox et al., 2003b; Ballard et al., 2006).
Women themselves and those around them (family and friends) are frequently unaware of endometriosis as a condition (Denny, 2009; Fourquet et al., 2010). The perception of menstrual irregularities as ‘normal’ and the perception of menstrual pain as something to be endured also contribute to delay in seeking help (Cox et al., 2003b; Denny, 2004b; Ballard et al., 2006), particularly for adolescents (Manderson et al., 2008; Markovic et al., 2008). Denny (2004b) and Seear (2009a) refer to an ‘etiquette of menstruation’ (Laws, 1990) whereby in many societies, menstruation itself is perceived as something private and something to be hidden. Women may thus actively conceal their menstrual irregularities, especially from men. Others, such as mothers and friends, facilitate and encourage this concealment (Seear, 2009a). However, the influence of family and friends who are able to identify pain experiences as abnormal and encourage help seeking, as well as disrupted social roles such as in performing education or work tasks, may also serve as catalysts that shift a woman's understanding of her symptoms from being normal to pathological (Manderson et al., 2008).
Diagnostic delay: factors relating to the medical profession
Delays to diagnosis have also been identified once women have sought medical help for their symptoms and misdiagnosis is common (Denny, 2004b; Jones et al., 2004; Huntington and Gilmour, 2005; Denny and Mann, 2008). Studies demonstrate medical level delays, between help-seeking and diagnosis, of between 3.7 (Cox et al., 2003a) and 5.7 years (Denny and Mann, 2008). Delays were found to be common at the primary care level and reflect resistance to referral (Denny and Mann, 2008; Nnoaham et al., 2011). Several papers suggest that prior to diagnosis, women commonly experience repeated visits to doctors where symptoms are normalized, dismissed and/or trivialized, resulting in women feeling ignored and disbelieved (Cox et al., 2003a, b; Denny, 2004a, b, 2009; Jones et al., 2004; Ballard et al., 2006; Denny and Mann, 2008; Manderson et al., 2008; Markovic et al., 2008). Women were often initially referred to inappropriate secondary care, or were misdiagnosed, most commonly with irritable bowel syndrome or pelvic inflammatory disease (Jones et al., 2004; Ballard et al., 2006; Denny and Mann, 2008). General practitioners were reported as lacking knowledge, awareness and sympathy and displaying attitudes that perpetuate myths about endometriosis (Cox et al., 2003b; Denny, 2004b; Jones et al., 2004; Denny and Mann, 2008).
On receiving a diagnosis, symptomatic women frequently reported that they felt a sense of relief, legitimation (i.e. confirmation that their symptoms were genuine), liberation and empowerment, replacing feelings of fear and self-doubt (Cox et al., 2003a; Denny, 2004b; Huntington and Gilmour, 2005; Ballard et al., 2006; Manderson et al., 2008; Seear, 2009b). Others reported feelings of anger at the delay to diagnosis and feeling vindicated that their persistence was valid (Denny, 2004b; Denny and Mann, 2008). Diagnosis provides women with a language with which to explain their experiences and sanctions access to support services (Ballard et al., 2006). Conversely, asymptomatic women who were diagnosed opportunistically experienced a different response, often characterized by shock and disbelief (Cox et al., 2003a).
Uncertainty, which is a factor in delayed diagnosis especially at the patient level (see above), continues post-diagnosis; endometriosis is a disease characterized by uncertainty at several levels (Lemaire, 2004; Butt and Chesla, 2007; Whelan, 2007; Denny, 2009). Along with ‘diagnostic uncertainty’, women experience ‘symptomatic uncertainty’ (relating to the variability of symptoms and the trial and error approach to treatment) and ‘trajectory uncertainty’ (relating to uncertainty about their future) (Denny, 2009).
‘QoL’ and everyday activities
There were 17 papers (40%; 14 quantitative and 3 qualitative) which reported findings relating to the impact of endometriosis on QoL and everyday activities. QoL measures have been widely used in studies of endometriosis, and are discussed in several review papers (Gao et al., 2006; Jia et al., 2012). Most utilize general QoL measures [e.g. Short Form Health Survey-36 and -12 (SF-36 and SF-12)] rather than those specific to endometriosis [Endometriosis Health Profile-30 and -5 (EHP-30 and EHP-5]. A number of studies demonstrate reduced QoL among women with endometriosis (Marques et al., 2004; Petrelluzzi et al., 2008; Siedentopf et al., 2008; Bernuit et al., 2011; Tripoli et al., 2011; Chene et al., 2012), and one study demonstrated that a minority of women consider themselves to have a current state of health ‘worse than death’ (Simoens et al., 2012).
Pain is consistently reported as a central and destructive feature of life with endometriosis and several studies report a negative correlation between pain and QoL (Sepulcri and do Amaral, 2009; Nnoaham et al., 2011; Souza et al., 2011; Tripoli et al., 2011). Endometriosis symptoms, and specifically pain, have a detrimental impact on daily life and physical functioning (e.g. sleeping, eating, moving) (Jones et al., 2004; Petrelluzzi et al., 2008). Between 16% (Simoens et al., 2012) and 61% (Fourquet et al., 2011) of women experience difficulties with mobility, daily activities and/or self-care. Fourquet et al. (2011) also found that women had SF-12 scores denoting statistically significant disability in physical and mental health components, indicating that the women in this study experienced substantial disability and Nnoaham et al. (2011) found that women with endometriosis had reduced physical health compared with the normative population. Sleeping has also been found to be negatively affected by endometriosis (Fourquet et al., 2010).
Household and housekeeping activities (e.g. cooking, shopping, cleaning, gardening and childcare) are also affected (Jones et al., 2004) for between 23% (Bernuit et al., 2011) and 71% (Fourquet et al., 2010) of women with endometriosis. Bernuit et al. (2011) found that of all the women who reported that endometriosis had a negative impact on their QoL (67% of the total sample), a third (36%) said it affected their relationships with family, whereas in a smaller scale study, Fourquet et al. (2010) found that 45% of women reported a negative impact on childcare.
Energy and vitality were also reported to be negatively impacted by endometriosis (Jones et al., 2004). For example, Fourquet et al. (2011) found that 27% of women with endometriosis reported low energy levels, while Petrelluzzi et al. (2008) reported that women had poor QoL (SF-36) scores for vitality. A negative impact of pain on sport and exercise has also been demonstrated (Fourquet et al., 2010; Bernuit et al., 2011).
Several authors have documented the impact of endometriosis on women's social lives. Studies report that between 19 and 48% of women experience an impact on their social lives (Fagervold et al., 2009; Fourquet et al., 2010, 2011; Bernuit et al., 2011). Petrelluzzi et al. (2008) found that women with endometriosis and chronic pelvic pain of moderate intensity showed a poorer QoL in the social functioning dimension than a control group. Gilmour et al. (2008) and Jones et al. (2004) reported that women experienced a reduction in social activities due to pain, fatigue and the need for toilet access, or worry about the onset of pain while they were out, leaving them feeling depressed, moody and angry. Women also described feeling less able to socialize when they are out (due to being preoccupied with worry about their condition), resulting in reduced confidence (Jones et al., 2004).
However, the impact of endometriosis symptoms, especially pain, is dynamic: it changes over time and across life stages. A retrospective study of women diagnosed 15 years previously highlighted the way that pain changes over the life course: the majority of women who had been pain free at diagnosis reported experiencing pain post-diagnosis; but pain experiences changed again at menopause, as 96.9% of post-menopausal women reported being pain free, compared with 19.6% of premenopausal women (although other symptoms such as flatulence and urinary symptoms were common among post-menopausal women) (Fagervold et al., 2009).
Intimate relationships
There were 12 papers (29%; 6 qualitative, 5 quantitative and 1 mixed methods) which offered findings relating to the impact of endometriosis on intimate relationships, including, but not limited to, findings about the incidence and impact of dyspareunia (painful sexual intercourse).
Papers suggest a substantial impact of endometriosis on the quality of sex life: between 33.5% (Bernuit et al., 2011) and 71% (Fourquet et al., 2011) of women reported that endometriosis negatively affected their sex lives. Chene et al. (2012) reported that the quality of sex life was affected in both women with minimal and with severe endometriosis.
Specifically, incapacitating pain and dyspareunia were found to have an impact on sex life (Fourquet et al., 2010). One large, cross-country study suggested that 24–25% of women with diagnosed endometriosis experienced dyspareunia (Bernuit et al., 2011). Other, smaller scale studies have reported higher rates at between almost 50 and 100% (of sexually active participants) (Christian, 1993; Denny, 2004a, b; Jones et al., 2004; Denny and Mann, 2007; Chene et al., 2012). Denny and Mann (2007) found that for 69% of women, dyspareunia included pain in the hours and days after sex and Ferrero et al. (2005) suggested that women with endometriosis had frequently suffered dyspareunia during their entire sex lives. Responses to dyspareunia include starting but then stopping intercourse; changing positions; enduring intercourse because of a desire for pregnancy and enduring intercourse because of a reluctance to allow endometriosis to affect yet another aspect of life or because of a desire for closeness with a partner (Denny and Mann, 2007). Both Denny and Mann (2007) and Jones et al. (2004) report that the majority of women who experience dyspareunia subsequently avoid or limit sexual intercourse. This results in feelings of inadequacy and guilt (Jones et al., 2004). A number of studies report that women with endometriosis and pain symptoms report less frequent sex than those with asymptomatic endometriosis and controls (Waller and Shaw, 1995; Tripoli et al., 2011). Fagervold et al. (2009) found a correlation between dyspareunia (which 1/3 reported) and negative impacts on relationships. Qualitative research found that women were reluctant to discuss dyspareunia with healthcare professionals and that women reported that healthcare professionals did not ask about this (Denny, 2004a, b). However, Bernuit et al. (2011) found that nearly half (47%) of women with diagnosed endometriosis who reported that pain affected their QoL had visited their doctor due to dyspareunia. Interventions to enable couples to address the impact of endometriosis on sexual relations are limited and those that are available are reported by couples to be unhelpful (Butt and Chesla, 2007).
Several studies have found that women feel that the symptoms and experience of endometriosis more generally (including but not limited to dyspareunia) have had a negative impact on their relationships and have in some cases contributed to relationship breakdown (Cox et al., 2003c; Denny, 2004a, b; Jones et al., 2004; Huntington and Gilmour, 2005; Fagervold et al., 2009). Fagervold et al. (2009) reported that 40 out of 78 (51%) women felt that endometriosis had a negative effect on their relationship (but for most only at certain points in the cycle), that 12 reported serious problems with relationships and that 6 had experienced relationship breakdown as a result. However, in some cases partners were also identified as an important source of support (Denny, 2004a). In a rare though small-scale study of women and their male partners, Butt and Chesla (2007) found that the experience of living with endometriosis disrupted day-to-day life and intimate relatedness for couples. They identified five relationship ‘coping’ patterns: ‘together but alone’; ‘battling together’; ‘conjoined through disability’; ‘totalized by caregiving’ and ‘engaged in mutual care’ (Butt and Chesla, 2007).
Planning for and having children
There were 10 papers (24%; 5 quantitative, 4 qualitative and 1 mixed methods) which offered findings relating to the impact of endometriosis on planning for and having children. Sepulcri and do Amaral (2009) and Christian (1993) reported that ∼50% of couples had experienced problems conceiving. Infertility may be more common however as Fourquet et al. (2010) found that 71% of women had attempted to conceive and 90% of these had experienced difficulties.
However, Fourquet et al. (2010) also found that only 47% of women who had difficulties conceiving sought infertility treatment and Mathias et al. (1996) found that only 4% of women were undergoing infertility treatment. Fagervold et al. (2009) reported that of 45 women with infertility, 76% went on to deliver a biological child and 44% of these were conceived via IVF.
Infertility, or concerns about possible infertility, is reported to result in worry, depression and feelings of inadequacy among women, and to contribute to relationship breakdown (Jones et al., 2004). However, other studies found no correlation between infertility and negative effects on relationships (Fagervold et al., 2009). Women felt that GPs' attitudes and knowledge, and their experiences of delayed diagnosis, subsequently influenced their experiences of in/fertility (Denny and Mann, 2008). Women experience uncertainty regarding fertility in the future (Denny, 2009) and report wanting more information about potential infertility (Cox et al., 2003a).
Education and work
There were 12 papers (29%; 7 quantitative, 4 qualitative and 1 mixed methods) which offered findings relating to the impact of endometriosis on education and work.
A focus on the impact of endometriosis on education has been included in a small number of papers with inconclusive findings. Whilst some studies reported that endometriosis had affected women's study activity and grades, and had caused some to leave education before completion (Huntington and Gilmour, 2005; Gilmour et al., 2008), others reported that only a minority of women had experienced negative consequences on their education (Fagervold et al., 2009).
More commonly, researchers have explored how endometriosis has impacted on women's working lives. The authors have suggested that women miss an average of 7.41 h of work per week when symptoms are at their worse (Fourquet et al., 2011), and that more generally they have an average of 13% loss of work time (Fourquet et al., 2011) or miss 19.3 days of work per year (Fourquet et al., 2010). Similarly, Nnoaham et al. (2011) found that women with endometriosis lost an average of 10.8 h weekly, but this was mainly due to reduced effectiveness at work, as opposed to absenteeism. Several papers suggest that women's endometriosis symptoms, particularly pain symptoms, impact on productivity at work with between 23 and 66% reporting limitations in their ability to perform work-related activities (Fourquet et al., 2010, 2011; Bernuit et al., 2011). Fourquet et al. (2010) also reported that 84–85% of women described a decrease in their quality of work, and elsewhere these authors report an average rate of work impairment and reduced effectiveness of 65% (presenteeism) and an average loss of efficiency levels of 64% (work productivity loss) (Fourquet et al., 2011). These findings have been echoed by other authors (Mathias et al., 1996; Cox et al., 2003c; Denny, 2004a; Huntington and Gilmour, 2005; Gilmour et al., 2008; Fagervold et al., 2009). According to Simoens et al. (2012), the average cost of productivity loss per woman with endometriosis is estimated to be €6298, double the average direct healthcare cost. Menstrual pain, incapacitating pain, abdominal pain and depression predict poor performance at work (Fourquet et al., 2010).
Informing employers of their diagnosis of endometriosis and of its symptoms causes tensions for women, as while it is felt to be a private condition, women also need support in employment (Gilmour et al., 2008). Women do not always inform employers of their diagnosis or symptoms for a range of reasons including the potential implications of this and because they find it difficult to discuss a gender-specific condition with male employers (Gilmour et al., 2008). Gilmour et al. (2008) suggest that the decision to disclose may be affected by women's past experiences of being disbelieved. Gilmour et al. (2008) and Denny (2004a) both found that women reported variability in employers' responses: for example, some were supportive, sympathetic and willing to make adjustments to working practices, whereas others lacked sympathy and understanding and trivialized or disbelieved symptoms.
Mental health and emotional wellbeing
There were 21 papers (50%; 15 quantitative, 4 qualitative and 2 mixed methods) which offered findings relating to the impact of endometriosis on mental health and emotional wellbeing. The heterogeneity of papers in this theme precludes an overall thematic synthesis, and the results are presented first for quantitative studies and then the contributions of qualitative work are discussed.
Quantitative studies: depression, anxiety and emotional distress
Papers reporting on quantitative studies into the links between endometriosis and mental health and emotional wellbeing have varying results, both within and across papers. For example, Siedentopf et al. (2008) found that women with endometriosis reported higher levels of perceived stress compared with controls and Petrelluzzi et al. (2008) found that women with endometriosis and chronic pelvic pain of moderate intensity show higher perceived levels of stress than those of the standard population, and have low QoL scores relating to mental health. Conversely, Low et al. (1993) found the rates of psychoticism among women with endometriosis to be within normal range, and that women with endometriosis were at the boundary of mild depression and the normal range. Waller and Shaw (1995) found that women with endometriosis had similar anxiety levels compared with control groups. Overall, the weight of the evidence points to higher rates of depression, anxiety and emotional distress than control groups and the general population (Low et al., 1993; Peveler et al., 1996; Lemaire, 2004; Lorençatto et al., 2006; Petrelluzzi et al., 2008; Siedentopf et al., 2008; Sepulcri and do Amaral, 2009; Fourquet et al., 2011; Simoens et al., 2012).
No firm conclusions can be drawn about the role of pain when comparing women with endometriosis-related pain and those with endometriosis who do not have pain (Waller and Shaw, 1995; Marques et al., 2004; Lorençatto et al., 2006; Eriksen et al., 2008; Sepulcri and do Amaral, 2009), but overall findings comparing women with chronic pelvic pain associated with endometriosis to women with chronic pelvic pain from other or unknown causes suggest that it is the experience of pain, as opposed to endometriosis itself, that is associated with mental health difficulties and emotional distress (Low et al., 1993; Waller and Shaw, 1995; Peveler et al., 1996; Roth et al., 2011; Souza et al., 2011). However, some authors have pointed out that even when rates of depression, anxiety and emotional distress appeared to be higher for women with endometriosis-related pain, the causal direction could not be identified (Lorençatto et al., 2006; Sepulcri and do Amaral, 2009). Data regarding correlations between endometriosis stage and mental health and emotional wellbeing also appear inconclusive (Marques et al., 2004; Siedentopf et al., 2008; Sepulcri and do Amaral, 2009).
Qualitative studies: the experience of emotional distress
Emotional distress is a pervasive theme throughout the range of papers reporting on qualitative studies and suggest that emotional distress is a key feature of living with endometriosis for many women and also for their partners. Endometriosis is reported to result in feelings of emotional distress, hopelessness, isolation, worthlessness and depression and feeling suicidal (Cox et al., 2003a, b; Whelan, 2007). Women feel they cannot cope with the pain, leaving them miserable, depressed, moody and short tempered. They experience loneliness as a result of social isolation and are reluctant to discuss their experiences with others as they feel their accounts are not always believed. Physical appearance and self-image may be affected by a range of factors including treatments that cause feelings of bloatedness, having greasy or spotty skin and weight gain (Jones et al., 2004). The impact of endometriosis on mental health and emotional wellbeing may extend to partners: Butt and Chesla (2007) described the emotional pain and multiple griefs and losses experienced by both women and their male partners.
Medical management and self-management
There were 11 papers (26%; 10 qualitative and 1 mixed methods) which offered findings relating to the impact of endometriosis in relation to medical and self-management.
Medical management
Treatments intended to reduce symptoms often carry side effects that impact on QoL (Denny, 2004a; Jones et al., 2004) and offer only short-term relief (Denny, 2009). Denny (2004a) found that women felt more positive about surgical treatment than drug treatment. However, women worry about various aspects of treatment including side effects and hospital stays, and report frustration at having to rely on medical treatment, and anger at the lack of effective treatments (Jones et al., 2004). Markovic et al. (2008) describe how the narratives of endurance that characterize women's experiences pre-diagnosis (e.g. endurance of pain) continue post-diagnosis as they endure treatments which may compromise overall health and wellbeing, and this was particularly true for adolescents who were more accepting of the dominant biomedical model. The long-term effects of medical treatment also concern many women (Denny, 2004a, b).
Women with endometriosis have experienced significant variability in healthcare professionals' attitudes and behaviours which are frequently described as problematic (see the section ‘diagnostic delay and uncertainty’). For example, women report feeling that the quality, intensity, duration and impact of pain are central to their experiences. However, while healthcare professionals express interest in the level and location of the pain, they do not ask in depth questions about the nature of the pain (i.e. its quality, effect and duration) (Denny, 2004a, b, 2009).
Self-management
In response to the limitations of medical treatment, some women also attempt to manage their endometriosis and alleviate symptoms through lifestyle changes (e.g. changes to diet and exercise) and through complementary and/or alternative therapies (Cox et al., 2003c; Huntington and Gilmour, 2005; Gilmour et al., 2008; Markovic et al., 2008). However, healthcare practitioners' information and advice-giving regarding non-medical and self-management strategies has been described as lacking (Huntington and Gilmour, 2005; Gilmour et al., 2008). For some women, non-medical management strategies were used alongside medical treatment (Cox et al., 2003c), whilst others turned to this approach due to disenchantment with medical treatment and a rejection of the biomedical approach (Cox et al., 2003c; Markovic et al., 2008). This use of alternatives to biomedicine is largely described as an ‘empowering’ experience that has allowed women to ‘take control’ of their management (Cox et al., 2003c; Huntington and Gilmour, 2005; Gilmour et al., 2008; Seear, 2009b) and can promote healthier living more generally (Gilmour et al., 2008). However, authors have also reported on the problematic aspects of non-medical- and self-management, including the financial constraints in access to some treatments (Cox et al., 2003c; Seear, 2009c) and the extent to which such management methods can disrupt life (Huntington and Gilmour, 2005). Becoming an ‘expert patient’ by developing knowledge and engaging in self-management is demanding and has been found to both reduce and compound the stress of living with endometriosis (Seear, 2009b).
Discussion
This is the first comprehensive review of the socio-psychological impact of endometriosis incorporating both qualitative and quantitative studies from a range of disciplines. We have used a thematic approach to consolidate this body of knowledge and to provide insights into women's experience of endometriosis.
That women experience considerable delays between symptom onset and diagnosis has been well evidenced (e.g. Arruda et al., 2003) and papers included in this review confirm this. These delays occur at both the patient level and the medical level. Receiving a diagnosis often results in feelings of relief and vindication. It is concerning that findings regarding the delay to diagnosis, and the features that contribute to this, have been well documented for several years, and yet these delays continue to be significant features of the experience of endometriosis for many women. Endometriosis is characterized by uncertainty and this uncertainty is not only a key feature of the diagnostic delay, but also of living with and making sense of endometriosis post-diagnosis. The uncertainty surrounding diagnosis, treatment and prognosis needs to be acknowledged and discussed with women in the clinical encounter.
Quantitative studies have concluded that endometriosis symptoms can negatively and substantially impact QoL and daily activities such as household tasks, energy and vitality and socializing as well as physical functioning. Qualitative studies suggest that the negative impact of endometriosis on daily life and on women's lives is complex, multidimensional and pervasive. Many women feel that endometriosis controls and restricts their lives, leaving them powerless. Again, these findings have persisted over time, and the paucity of effective and long-term treatments and the absence of a cure are likely to be key contributing factors. Findings regarding the incidence of dyspareunia vary, but suggest that it has a significant social and psychological impact.
However, research into the impact on QoL and everyday activities focuses almost entirely on women. While studies suggests that intimate relationships are affected by pain, dyspareunia and infertility, little is known about how endometriosis impacts on women's partners and children or how wider family members are affected by and respond to women with endometriosis. The very limited research with male partners suggests that relationships can be negatively impacted (Fernandez et al., 2006), although elsewhere partners are also identified as important sources of support (Denny, 2004a). Given the pervasive impact of endometriosis across many social domains, the lack of research on partners and couples' relationships is particularly stark. This is all the more problematic, since there is evidence from other conditions that male partners are impacted by living with and caring for a partner with a chronic condition (Scott et al., 2004).
Limited research suggests that the impact, or potential impact, of endometriosis on fertility causes worry, depression and feelings of inadequacy. Considering that almost half of infertile women have endometriosis, it is perhaps surprising that there has been little research into the social and psychological experience of infertility, or of anticipated infertility, among women with endometriosis.
There is consistent evidence of a negative impact of endometriosis on women's working lives and the difficulties they experience in disclosing information to employers. However, the links between research evidence and policy and law relating to disability and employment are rarely made. For example, there appears to have been little exploration of how equality legislation might apply to some women with endometriosis and women's experiences of reasonable adjustments.
The weight of evidence from quantitative studies suggests that rates of depression, anxiety and emotional distress are higher for women with endometriosis than control groups or the general population. While no firm conclusions can be drawn about the role of pain when comparing women with endometriosis pain and women with pain-free endometriosis, the overall findings comparing women with chronic pelvic pain-related to endometriosis and women with chronic pelvic pain from other or unknown causes suggest that it is the experience of pain, as opposed to endometriosis itself, that is associated with mental health difficulties and emotional distress. Qualitative studies highlight the emotional distress that characterizes many women's lives, including feelings of isolation, guilt, worry, worthlessness and hopelessness, and feeling unable to cope. The mechanisms by which this occurs are unclear however, as pain, emotional distress, fatigue and dissatisfaction with health care and available treatments are all interwoven within the complex experience of endometriosis. Despite calls for care and support to better focus on psychological and emotional experiences and impact, depression, anxiety and emotional distress appear to prevail and there are few reports of systematic interventions to address these issues.
While this review does not consider treatment outcomes and efficacy, the reviewed papers suggest that the experience of medical treatment is often problematic for many women. In response to this, some women have attempted to self-manage their endometriosis through lifestyle changes and/or complementary and alternative therapies. However, these strategies can also be problematic since they may involve financial and practical difficulties and may themselves pose risks to wellbeing.
It is possible to suggest a number of strategies to reduce the negative social and psychological impact of endometriosis. Better awareness of the varied clinical features and manifestations of endometriosis and selection of the most appropriate investigations by healthcare practitioners may reduce delays to diagnosis at the medical level (Huntington and Gilmour, 2005; Ballard et al., 2006; Denny and Mann, 2008). This can only be achieved by improved education of all healthcare professionals who may come into contact with women with endometriosis. Increasing women's awareness of physiology and of endometriosis through education in schools and via support groups may help women to distinguish between menstrual pain and endometriosis and reduce patient delays in seeking help (Cox et al., 2003b; Lemaire, 2004). Seear (2009a), however, warns that strategies to increase awareness of endometriosis and to help women distinguish between normal and abnormal pain need to be grounded in an understanding of why pain is normalized, and of the stigma associated with menstrual irregularities.
Health care management post-diagnosis needs to be more holistic. It should be informed by an understanding of the multidimensional impact of endometriosis and underpinned by a biopsychosocial approach that includes emotional support, stress reduction, social support, adaptive coping strategies, psychosexual treatment and a focus on QoL issues, sex and relationships, pain management and career counselling (Peveler et al., 1996; Huntington and Gilmour, 2005; Lorençatto et al., 2006; Butt and Chesla, 2007; Denny and Mann, 2007; Siedentopf et al., 2008; Seear, 2009b; Roth et al., 2011). Recent research has identified problematic care experiences in endometriosis centres and identified the need for a more patient-centred approach to care (Dancet et al., 2012).
Women report receiving insufficient information at diagnosis, and express a desire for more information about surgery (e.g. anaesthetic procedures, the location and size of incisions, possible complications and recovery time and pain) (Cox et al., 2003a) and general information about living with and managing endometriosis (Huntington and Gilmour, 2005).
More information (both verbal and written) about the management, including non-medical- and self-management, of endometriosis should therefore be made available to women. This must be delivered in a helpful format and provided in a timely manner. However, in doing this we need to take account of the contested and problematic nature of endometriosis and of the ‘knowledge’ surrounding it (Seear, 2009b, c).
Support/information groups are of value and help women to interpret their experiences, feelings and emotions. Information and confidence gained from such groups allows women to evaluate medical information and negotiate with healthcare practitioners, insurers and employers (Whelan, 2007). Such groups also offer a route into wider patient communities, which are an important source of support. Indeed, women have deemed other women with endometriosis to be the most useful and valued source of information (Whitney, 1998). The rise in online communication has also provided women with new and different ways to share information and provide and receive support (Emad, 2006; Neal and McKenzie, 2011). Support groups also provide researchers with links to patients for research studies and are an invaluable mechanism to achieve patient and public engagement in research and service improvement activities.
Methodological issues
Overall the quality of the papers was good, with just two excluded in the quality assessment phase. However, some limitations and weaknesses can be identified.
Quantitative studies of the impact of endometriosis are primarily concerned with establishing correlations between the characteristics of women with endometriosis and their symptoms and QoL. Many researchers rely on a priori categories pertaining to the impacts and implications of endometriosis, which may not be derived from qualitative, inductive research into how women experience the condition (see Jones et al., 2004 and Dancet et al., 2011 for exceptions to this). Most studies are cross-sectional and use general QoL instruments whose psychometric properties and internal consistency are not well established in endometriosis (Jia et al., 2012). Such instruments often exclude important issues such as infertility, which may be of considerable significance to a more holistic understanding of the endometriosis experience.
Even studies that use generic instruments do not always include control groups and may not take account of medical confounders such as disease severity and co-morbidities. Very few quantitative studies account for social variables such as educational level, socio-economic status and ethnicity. While such studies helpfully challenge theories that position endometriosis as a lifestyle or psychosomatic disease, and make visible the correlations between extent of disease, symptoms and QoL, they are limited in their ability to uncover the subjective experiences of living with the condition and the meanings it has for women with endometriosis and those around them. Such issues are found to be highly relevant in qualitative papers.
Qualitative research suggests that the experience of endometriosis and its treatment varies considerably across the life course. Experiences fluctuate according to women's ages, social circumstances and biographical priorities and are dependent on a range of socio-demographic characteristics. Such studies highlight that women may have conflicting and contradictory understandings and meanings of endometriosis and that the impact of endometriosis is multifaceted and complex. Qualitative work has also highlighted the way in which women may adopt a range of strategies to respond to and resist the impact of endometriosis. However, while these studies produce rich data, they often include small sample sizes and their generalizability is limited as a result.
Both quantitative and qualitative studies may include skewed samples, e.g. more severe and long-term cases due to recruitment methods focused primarily on secondary care clinics or support groups. In addition, few studies link endometriosis to wider theories of gender, disability, stigma or inequality of access and virtually nothing is known about how social class, educational status, age or ethnicity impacts on the experience of endometriosis. Women with endometriosis often have a combination of symptoms and whilst it is difficult to assess the individual significance of chronic pelvic pain, deep dyspareunia and severe dysmenorrhoea in a woman experiencing all three of these symptoms, very few studies have tried to quantify, either objectively or subjectively, the relative importance of each.
Suggestions for future research
Prospective and retrospective longitudinal cohort studies would enable us to more adequately capture the changing and dynamic nature of the impact of endometriosis on people's lives. This is particularly relevant given the impact of this condition on life-course markers such as childbearing, relationships and career progression and its inherent association with both menarche and menopause. Future QoL research should consider utilizing endometriosis-specific instruments, such as the EHP-30 and EHP-5, which have been developed as a result of qualitative research with women.
Researchers should consider the use of mixed methods to explore the impact of endometriosis to draw on the combined strengths of qualitative and quantitative research (Plano Clark, 2010; Tashakkori and Teddlie, 2010). While there are difficulties in bringing together approaches from different paradigms (Bryman, 2006), there are many advantages in taking a broader, more holistic and more comprehensive biopsychosocial approach to understanding the impact of endometriosis.
A wider range of people should be recruited into studies of all kinds, which may mean adapting recruitment sites and methods, and there is a need to report more fully on the socio-demographic characteristics of participants. Since factors relating to the organization and financing of healthcare systems impact on access to services, availability of treatment regimes, the provision of information and forms of support for endometriosis patients, further comparative, cross-country research would be helpful in identifying areas of good practice in supporting women.
Some authors have suggested the experience of endometriosis is qualitatively different for adolescents (Cox et al., 2003a; Manderson et al., 2008; Markovic et al., 2008). However, there has been little research focusing specifically on the social and psychological impact of endometriosis on adolescents (although there has been some research into the impact of chronic pain on adolescents) (see Forgeron, 2011). Given the potential impact of endometriosis on mental wellbeing, social life and educational achievement during formative years, such research would be of value.
The impact of endometriosis on relationships between women and their partners, and the impact of endometriosis on partners themselves, has been underexplored and warrants further investigation. Similarly, the impacts on children of women with endometriosis and on the wider family have been paid scant attention and should be considered in future research.
Importantly, research is needed which can assist the development of interventions to tackle the negative social and psychological impact of endometriosis and its treatment. Such interventions should be collaboratively developed with patients, partners and support/information groups, tailored to the needs of specific groups of patients and robustly evaluated (Crawford et al., 2002).
Finally, a review into women's experiences of care and support would be of value in identifying problematic experiences and in collating recommendations for how care can be improved.
Conclusion
This review has identified a large number of studies which address the psychological and social impact of endometriosis on women's lives, with the majority identifying a significant impact across several domains. The review has discussed some of the methodological limitations of existing studies and identified significant gaps in the literature. We recommend further research which utilizes mixed methods approaches and endometriosis-specific instruments to explore the impact of endometriosis in more diverse populations. In particular, there is an urgent need to develop and evaluate interventions for supporting women and their partners living with this chronic and often debilitating condition.
Authors' roles
L.C. conceived the study, and participated in study design, collection and analysis of data, and drafting and revising of manuscript and critical discussion. C.L. participated in study design, collection and analysis of data, and drafting and revising of manuscript and critical discussion. N.H. and H.M. participated in study design, collection and analysis of data, and drafting and revising of manuscript and critical discussion. E.D., M.B. and N.R.F. participated in collection and analysis of data, and drafting and revising of manuscript and critical discussion.
Funding
This review was funded by the UK Economic and Social Research Council, grant reference ES/J003662/1.

{kind=link}