





Abstract
Background: Caesarean section (CS) rates have been increasing dramatically in the past decades around the world. The objective of our study was to investigate the factors increasing the likelihood of undergoing CS in two public hospitals and one private hospital in Athens, Greece. Specifically, the purpose was primarily to assess the impact of non-medical factors such as private health insurance, potential for making informal payments, physician convenience and socio-economic status on the rate of CS deliveries. Methods: All available demographic, socio-economic and medical information from the medical records of all deliveries in the three hospitals in January 2002 were analysed. The relative importance of the variables in predicting delivery with CS rather than normal vaginal delivery was calculated in multiple logistic regression models to generate odds ratios (OR). Results: The CS rate in the public hospitals was 41.6% (52.5% for Greeks and 26% for i mmigrants), while the CS rate in the private hospital was 53% (65.2% for women with private insurance and 23.9% for women who paid directly). In the public hospitals, after controlling for demographic and medical factors, Greek ethnic background, delivery between 8 a.m. and 4 p.m., between 4 p.m. and midnight, and on Monday, Wednesday and Friday were found to increase the likelihood of CS delivery. In the private hospital, having private health insurance is the strongest predictor of CS delivery, followed by delivery between 8 a.m. and 4 p.m., between 4 p.m. and midnight, delivery on a Saturday and being a housewife. Conclusion: The results of this study lend support to the hypothesis that physicians are motivated to perform CS for financial and convenience incentives. The recent commercialization of gynaecology services in Greece is discussed, along with its implications on physicians' decisions to perform CS.
Caesarean section (CS) rates around the world have been increasing dramatically in recent decades. CSs make up a high proportion of total deliveries in Brazil (36%),1 Mexico (30%),2 Italy (31%),3 the USA (23%)3 and the UK (19%),4 with rates in most countries ranging between 15 and 25%.3 The trend is similar in OECD countries, and increasingly in less developed countries (e.g. Brazil, Mexico, Thailand5 and some Indian states6,7 ). Based on studies of medical indications, the acceptable CS level has been found to vary from 78 to 14%.9 The WHO10 states ‘there is no justification for any region to have a rate higher than 10–15%’, signifying a serious cause for concern in the majority of countries.
This concern is magnified by the economic costs and health-related risks associated with the procedure. For example, in the UK, CS deliveries significantly increase health care costs as they are reported to cost twice as much as spontaneous vaginal (V) delivery.11 Likewise, in Mexico, the large proportion of CS deliveries has created a serious burden on public health care spending.2 Moreover, it has been reported that in the USA, Netherlands and UK in the early 1990s maternal mortality was 2–4 times higher, and incidence of morbidity was 5–10 times greater12–16 for CS delivery as compared to V delivery.
Due to the newly emerged ‘epidemic’ of CS deliveries in most countries, there have been several investigations into the reasons for the rising rates. It is widely agreed that medical necessity cannot explain these increases and recent studies reveal a multitude of risk factors associated with CS delivery, ranging from medical and demographic to socio-economic and institutional factors. The most common factors include rising maternal age,13,17–25 high levels of maternal education,1,13,18,22,26–28 previous CS,29–31 obstetric complications,13,18,32 maternal request19,33,34 and high income level and social class.12,26–28,35–37
In addition, some studies, particularly in less developed countries, have assessed the impact of hospital ownership, insurance and physician factors on the proportion of CS deliveries. Higher CS rates are consistently predicted by private medical insurance or private hospitals,1,5–7,17,38–43 and associated with financial incentives,2,26 factors associated with physician convenience, such as delivery during week days and daylight hours,5,37,42,44–47 and supply-side factors such as a large number of gynaecologists.18,48
The objective of the present study was to examine the factors affecting a physician's decision to perform a CS in two public hospitals and one private hospital in Athens, Greece. The CS rate in Greece increased by almost 50% between 1983 and 1996.18 A recent study revealed that the rate exceeded 30% in a public obstetrics hospital in Athens in 1998, much higher than eight European comparators.48 The recent increase in CS deliveries in Greece may be explained by the changing composition of private sector involvement in this area. The Greek health care system is funded by a mix of private and public sources, with over 44% private financing; Greece has the highest proportion of private health care funding in the EU3 and one of the highest expenditures on health among OECD countries, spending 9.4% of GDP in 2001.9 In 2000, private medical insurance constituted 5.3% of the total health care expenditure, which is growing, whereas about 95% of private expenditure consisted of informal or direct payments to providers.49
There has been a gradual commercialization of gynaecological services in Greece, as deliveries are increasingly taking place in the private sector (i.e. 62.9% of deliveries in Athens in 1994 took place in private hospitals).50 Consistent with this trend is the increasing number of women covered by private health insurance (rising from 187 000 to 328 000 women between 1994 and 1998).50 The growth of gynaecological services in the private sector is further reflected by the total growth of 69.3% from 1997 to 2001 with an annual growth rate during this time of 14.7%, such that in 2001, 18% of the private health care market was directed to gynaecology.51 This growth may be due in part to the private hospitals being part of the stock market since the late 1990s. Additional supply factors may be contributing to increasing CS rates, as there is a large and growing number of gynaecologists in Athens. For instance, in 1997 there were 20.3 gynaecologists per 100 000 inhabitants, twice as many as in Paris, Barcelona, Liège, Amsterdam and Uppsala.48 Furthermore, between 1985 and 2000, the number of gynaecologists increased by 34%,51 while the population grew by <10%.
The private insurance system is based on reimbursement, following the indemnity model, thus there are no quality controls or preferred agreements between private insurers and providers. While women who access public hospitals are covered by public health insurance, many still have to pay hefty additional informal payments. In 1994, Greek households were paying an average of 5.66% of their total monthly expenditure on health services, which rose to 6.82% in 1999,52 representing the ‘hidden health economy’.53
While the impact of type of insurance on CS has been studied, most previous studies have been conducted in a developing country context. Thus, in addition to previously mentioned demographic and medical variables, this study will examine for the first time the impact of private health insurance, socio-economic status and potential for making informal payments derived from information on ethnic background on the rate of CS deliveries in Greece. Within the public hospitals, it is hypothesized that the CS rate would be higher for Greeks than for immigrant populations living in Greece, as the Greeks are considerably financially better off than immigrants and therefore are more able to make informal payments. Within the private hospital, it is predicted that having private medical insurance will significantly increase the odds of undergoing a CS delivery compared to direct payment by the patient. Furthermore, due to the recent commercialization of gynaecology in health care, it is hypothesized that increased pressure for financial growth in private hospitals is influencing physicians' decisions to perform CS. Thus, it is expected the CS rate would be higher in the private hospital than in the public hospitals.
Methods
This study was conducted in three hospitals in Athens: one major teaching public hospital, one specialist public gynaecology/obstetrics hospital and one private maternity hospital. The study had intended to include two private hospitals, however, access to the medical records was denied in the second private hospital once the purpose of the study was revealed. All deliveries in the three hospital settings for January 2002 were studied through manual medical chart review to record all relevant information. Selection bias was minimized as no cases were excluded in the analysis. Furthermore, the public hospitals represent the two most important obstetric hospitals in Athens, and the private hospital in this study performs the second largest proportion of private deliveries in Athens. Thus, it is likely that the proportion of the total number of births in Athens that took place in these three hospitals was high. While the hospitals may not be representative of the city or country as a whole, the objective of this study was to investigate the factors influencing physicians' practices, and not to generalize the findings on a greater scale.
All available demographic, socio-economic and medical information from the medical records was recorded. Although there was no accurate information on the income level or socio-economic status of the women, the records did detail their ethnic background, which was used as an indirect measure of their socio-economic status. For the purpose of this study, the ethnic background variable was separated into two groups: Greeks and immigrants. The majority of immigrants in this study come from Albania (65%), with the remainder from other Balkan countries as well as Pakistan, the Philippines and India. While this categorization of ethnic background is somewhat arbitrary as it does not reflect established research on social stratification in Greece, there is a paucity of available information in this area. Nonetheless, it is widely accepted that Greeks have considerably higher socio-economic status than immigrants, since the majority of immigrants are from low-income countries, and have not been in Greece long enough to establish financial security. Ethnic background is only included in the analysis of the public hospitals, since only Greek women attended the private hospital during the time frame of this study.
The relative importance of the various factors (medical and non-medical) in predicting CS rather than normal V delivery in public and private hospitals was calculated in multiple logistic regression models to generate odds ratios (ORs). The public and private hospitals were considered separately for two reasons: the patient populations are significantly different since only Greek women attended the private hospital during the study period; and payment structures differ since payment in private hospitals consists of private health insurance or direct payments, whereas public hospitals depend on public health insurance and informal payments. Marital status was left out of the analysis of the private hospital, since all women in this sample were married. The group with the lowest risk of CS delivery was used as a reference category and all variables of known importance were included in the regression model in order to control for their potential confounding effects.
Role of the funding source
The funding source had no involvement in study design; in the collection, analysis, and interpretation of data; in the writing of the report; nor in the decision to submit the paper for publication.
Results
The CS rate in the public hospitals was 41.6% (n=183), while the CS rate in the private hospital was 53% (n=193). The CS rates and crude and adjusted ORs (with 95% confidence intervals) for the public hospitals are presented in tables 1 and 2, while the private hospital results are shown in tables 3 and 4. As shown in table 1, the adjusted OR for a CS in public hospitals increases significantly with having previously had two or more births, higher maternal body mass at the time of delivery, weight gain during pregnancy >10 kg, premature deliveries, neonatal birth weight >4000 g and male neonate, but not with maternal age or marital status.
Table 2 shows that in the public hospitals, more Greek women gave birth by CS (52.5%) than V delivery, whereas only 26% of the immigrant women delivered by CS. The OR for a CS rather than a V delivery increases with the Greek ethnic group, where Greek women are significantly more likely to undergo CS than immigrant women. The time of delivery is a significant factor, where the likelihood of undergoing CS increases during working/daylight hours and, to a lesser degree, in the evenings, for >70% of CS deliveries were between 8 a.m. and 4 p.m. In addition, CS deliveries increase significantly on Mondays, Wednesdays and Fridays.
Table 3 shows that, within the private hospital, a gestational age longer than 36 weeks, first birth and birthweight >4000 g significantly predict CS delivery. As shown in table 4, having private insurance strongly predicts CS delivery in the private hospital, where women have 7.73 times the odds of undergoing CS with private insurance, compared to paying directly. In addition, housewives are more likely to undergo CS. As in the public hospitals, time and day of delivery was significant in predicting CS delivery: the odds of CS increase significantly between 8 a.m. and 4 p.m., and between 4 p.m. and midnight. Also, CS deliveries are significantly more likely on Saturdays than Sundays.
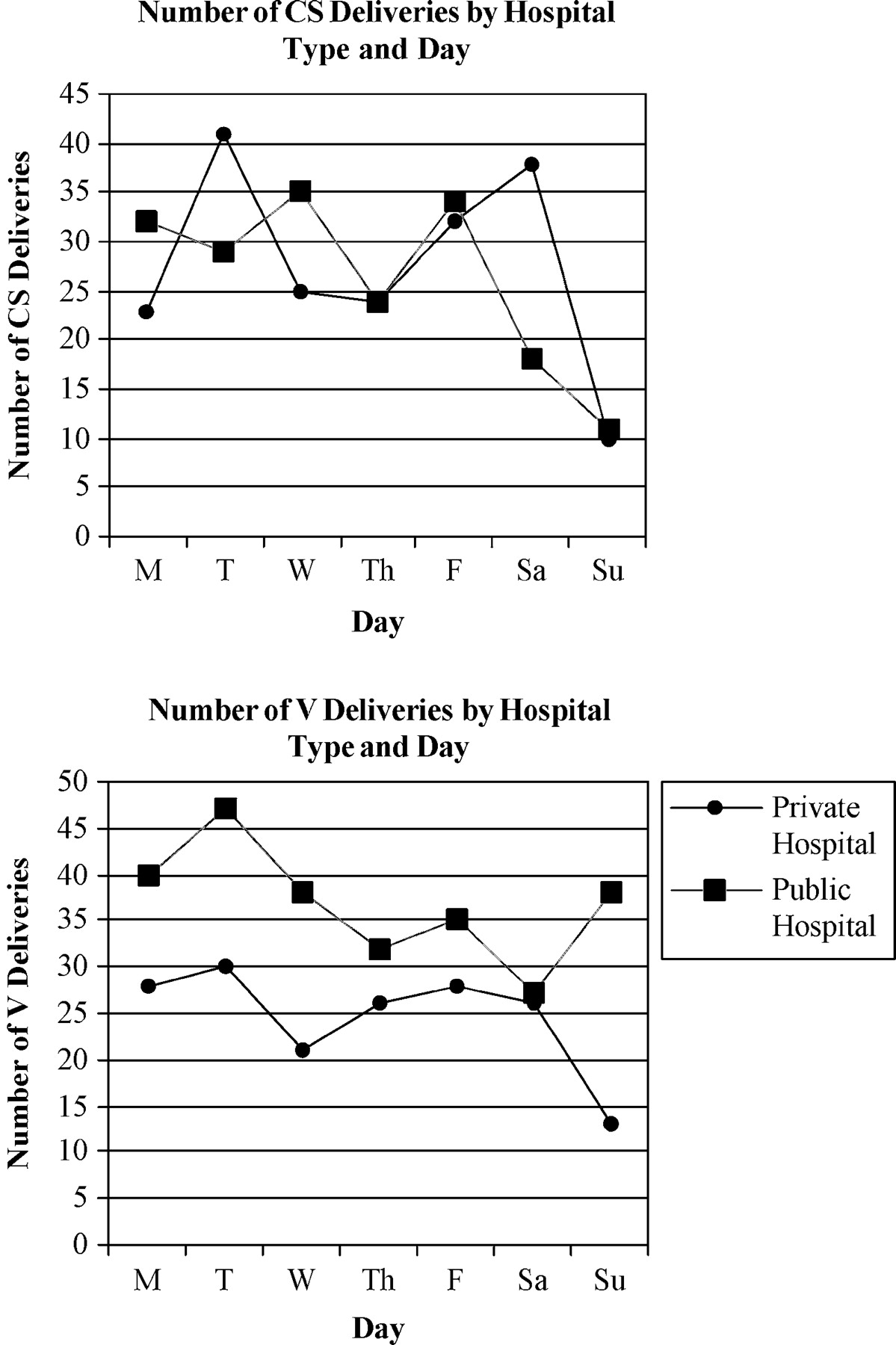
Figure 1 compares the CS and V delivery numbers per day for private and public hospitals. In the private hospital, there is a sharp decline in number of CS deliveries on Sunday, whereas in the two public hospitals there is a continuous decline in CS deliveries on the weekend. Also, there is an observable increase in CS deliveries in the private hospital on Tuesday, Friday and Saturday, compared to similar increases in public hospitals on Wednesday and Friday.
In examining the three hospitals together, there are some interesting findings. For instance, all women who had previously had a CS underwent the procedure again. Among women with a previous V delivery, 19.7% had a CS, and 80.3% had another V delivery, however, first births were divided evenly between CS and V deliveries.
The medical records revealed the most common complication indicating need for CS was cephalopelvic disproportion, followed by previous CS, breech presentation, pregnancy hypertension, alteration of heartbeat, twins or more and ‘other’ reasons, whereas no complications were reported in 91.6% of the vaginal deliveries. A puzzling finding was the reporting of myopia in the mother as a ‘complication’ leading to CS delivery in seven cases. It is likely the justifications for CS cannot necessarily be trusted as they may be for purposes of convenience. Also noteworthy is the low rate of foetal blood sampling (FBS) in labour (9.3%) prior to surgery. FBS is believed to be a necessary procedure in cases of suspected foetal acidosis, thus justifying operative delivery; rates of FBS in the UK are 44.4%.54 However, there was incomplete information on medical procedures such as ultrasound, which tend to precede FBS, therefore clinical high-risk situations or low rates of foetal acidosis symptoms may explain, in part, the relatively low rate.55 Another finding is the almost exclusive use of general anaesthesia with CS (99.2%).
Neonatal mortality is twice as great for CS compared to V delivery, for there were 16 stillbirths with CS delivery, compared to seven with V delivery. This data should be interpreted with caution as they are not adjusted for severity, complications or medical history (due to the incomplete medical records).
Information on the involvement of trainees and specialists in the deliveries was also collected from the medical records. It was revealed that the trainees (who work only in public hospitals) only take part in the vaginal deliveries, and mainly those of women in ethnic groups other than Greek. Likewise, specialists in public hospitals conduct all CS.
Discussion
Almost half of all deliveries performed in January 2002 in the three hospitals in Athens were by CS. It is important to emphasize that these findings are not meant to be generalized to the city or country as a whole. However, this rate is extremely high compared to that recommended in the literature and by the WHO.8–10 In examining the risk factors for undergoing CS delivery, it was revealed that, in addition to several medical, demographic and health service variables consistent with the literature (such as maternal body mass, weight gain during pregnancy, gestational age and birthweight), socio-economic factors also increase the likelihood of CS in both public and private hospitals.
It was found that Greek women in the public hospitals have 2.7 times greater odds of undergoing a CS than immigrant women, who are widely believed to have considerably lower socio-economic status than the Greek women. Furthermore, it was found that the rate of CS delivery among Greek women was 52.5%, compared to 26% among the other ethnic groups. Thus, as ethnic group can indirectly be a measure of socio-economic status, it is the least well off groups who have CS rates closer to the internationally accepted standards. While cultural variation may be playing a role in the differential rates, its influence is likely to be offset by the striking socio-economic differences between the groups.
Effects of private insurance on CS delivery were found in the private hospital. Among the women who delivered in the private hospital (all Greek women), those with private insurance were 7.73 times more likely to undergo CS delivery than those who paid directly. More specifically, 65% of the women with private insurance had CS delivery, compared to only 24% of the women who were not insured. It is unclear whether take-up of private insurance is related to willingness to undergo CS delivery. However, it appears that Greek women who pay directly in the private hospital are price-sensitive due to the considerably lower rates of CS among this group than those who have insurance.
These findings suggest that, similar to other studies in developing countries such as Brazil, Mexico and Thailand, non-medical factors were found to be more important than medical ones in the decision to deliver by CS. While medical complications were recorded to ‘justify’ the operation, it was revealed that they are not necessarily trustworthy and they may serve to make the operation ‘socially justifiable’.1 Similarly, there was very little use of FBS to assess medical necessity for CS in situations of foetal distress. As previously mentioned, the significant non-clinical factors found in this study were insurance type and ethnic group, revealing potential financial incentives in addition to factors associated with physician convenience (time and day of delivery).
Financial incentive factors, reflected in the predictive power of ethnic group and private insurance, can be understood within the context of the Greek health care system. As mentioned earlier, most private financing comes from informal payments taking place in public hospitals. The payments are considerably higher for CS than for V deliveries, due to the complexity of the procedure. It is believed that these payments are in part income dependent, where wealthier women pay more than poorer women.51 Thus, there are incentives affecting the decision to undergo a CS, particularly for wealthier patients. This explanation may clarify the significantly increased odds of undergoing CS as a Greek woman, who is able to pay more informally in public hospitals. Within the private hospitals, financial incentives arise from the considerably greater private health insurance reimbursement for CS than for V deliveries.
All women who had undergone previous CS underwent the procedure again. This practice of elective repeat CS is currently under debate, with increasing support for vaginal birth after CS (VBAC). The longstanding belief in the statement ‘once a caesarean, always a caesarean’ no longer applies. For, VBAC among women in the Netherlands has a success rate ranging from 60 to 80%.29 Likewise, there is less morbidity associated with VBAC than elective repeat CS.56 Current American obstetrics guidelines are also recommending VBAC, which is believed to reduce the number of repeat CS and overall CS rates.57
In examining the factors of physician convenience, the rates of CS significantly decline on Saturdays and Sundays in the public hospitals, and on Sunday in the private hospital, while rates of V deliveries increase at weekends, as shown in figure 1. Perhaps the CS rate declines on Saturdays in the public, but not the private, hospitals due to the more entrepreneurial nature of the gynaecologists in the private setting and the fact that only a small number of NHS doctors work on weekends. Private physicians work on contract and fee-for-service with the private hospital, whereas public physicians are government employees and have less incentive to work at the weekends (only on-call physicians perform deliveries). This observed decline in CS rates reflects the convenient nature of CS deliveries, and not the emergency procedure it should be. In addition, the results indicate that the risk of undergoing CS delivery increases significantly during the ‘working’ hours of the day and are least likely to occur between midnight and 8 a.m. Further qualitative research investigating physician practices would be helpful in elucidating the relationship between physician factors and CS rates.
One could also argue that the high rate of CS deliveries may result in part from maternal demand. It has been suggested that, increasingly, mothers are requesting CS to avoid the difficulties of natural labour.4 These suggestions have been put forth to explain CS rates that are <20%, whereas the present study reveals a much higher rate of almost 50%. Therefore, in light of the revealed importance of other medical and non-medical factors in determining CS, it is unlikely that maternal demand plays a significant role in the inflated CS rate in the three Greek hospitals. However, further research is needed to determine to what extent maternal preferences affect CS deliveries in Greece.
The findings of the present study may indicate the presence of supplier-induced demand for CS. The reasons behind this phenomenon can be explained in part by physician convenience and financial incentives. This study offers new insight into the rising CS trend, and the specific groups of women in Greece who are more likely undergo this operation. The results from this study differ significantly from those of a previous study of CS risk factors in Greece,18 primarily in the greater proportion of CS deliveries found in public than private hospitals in the past study, with the reverse being true in the present. More specifically, Skalkidis et al. reported a CS rate of around 30% in a public teaching hospital and around 20% in a private hospital in 1993, which has ‘changed’ to 41.6 and 53%, respectively, in the present study.18 This reverse finding was explained by the close nature of physician–patient relationship in the private institutions, however, this explanation does not apply to the current situation in Greece. Although the particular hospitals may not have been the same in each study, there are clearly important changes that have caused this reversal.
Many changes have occurred in the past decade resulting in the commercialization of gynaecology in Greece. These changes are primarily reflected by the growing involvement in the role of the private sector: increased use of private medical insurance and growing number of deliveries in private hospitals in addition to the dramatic increase in the number of gynaecologists in Greece, particularly in the private sector.50 Further pressures on private physicians, which may impact their operative decisions, stem from the recent role of the private hospital in the stock market. In the public hospitals, higher informal payments associated with CS may influence physicians' decisions. Thus, while previously CS deliveries may have been decided based on uncertainties surrounding the patient's condition, to be safe, physicians in the public and private hospitals examined in this study currently appear to be motivated to operate for financial and convenience incentives.
Number of CS and V deliveries in the private and public hospitals by day of week
Data for CS delivery of singleton babies according to demographic and reproductive variables in the public hospitals
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Age | ||||||||||||
| 14–34 | 59.9 (232) | 40.1 (155) | ||||||||||
| 35+ | 47.2 (25) | 52.8 (28) | 1.67 (0.94–2.98) | 0.079 | 1.50 (0.79–2.84) | 0.211 | ||||||
| Marital status | ||||||||||||
| Married | 57.1 (228) | 42.9 (171) | ||||||||||
| Unmarried/Divorced | 70.7 (29) | 29.3 (12) | 1.81 (0.90–3.65) | 0.097 | 2.08 (0.93–4.68) | 0.076 | ||||||
| No of live births | ||||||||||||
| 3+ | 72.2 (26) | 27.8 (10) | ||||||||||
| 2 | 50.5 (56) | 49.5 (55) | 2.55 (1.12–5.78) | 0.025 | 3.42 (1.34–8.76) | 0.010 | ||||||
| 1 | 60.7 (170) | 39.3 (110) | 1.68 (0.78–3.62) | 0.185 | 2.16 (0.88–5.30) | 0.090 | ||||||
| 1 (stillbirth) | 38.5 (5) | 61.5 (8) | 4.16 (1.09–15.78) | 0.036 | 1.74 (0.35–8.54) | 0.497 | ||||||
| BMI | ||||||||||||
| <20 | 64.9 (50) | 35.1 (27) | ||||||||||
| 20–25 | 58.7 (166) | 41.3 (117) | 1.30 (0.77–2.20) | 0.320 | 1.28 (0.72–2.27) | 0.388 | ||||||
| 25–30 | 58.5 (38) | 41.5 (27) | 1.31 (0.67–2.60) | 0.429 | 1.24 (0.56–2.65) | 0.582 | ||||||
| 30+ | 20.0 (3) | 80.0 (12) | 7.41 (1.92–28.54) | 0.004 | 13.82 (3.08–61.95) | 0.001 | ||||||
| Weight gain during pregnancy (kg) | ||||||||||||
| 0–10 | 63.5 (73) | 36.5 (42) | ||||||||||
| 11–20 | 57.4 (163) | 42.6 (121) | 1.29 (0.83–2.02) | 0.263 | 2.25 (1.30–3.90) | 0.004 | ||||||
| 21+ | 51.2 (21) | 48.8 (20) | 1.65 (0.80–3.40) | 0.170 | 2.56 (1.07–6.10) | 0.034 | ||||||
| Gestational age (weeks) | ||||||||||||
| <32 | 12.5 (2) | 87.5 (14) | 19.51 (4.13–92.17) | <0.001 | 46.27 (7.23–294.28) | <0.001 | ||||||
| 32–36 | 35.9 (14) | 64.1 (25) | 4.98 (2.23–11.13) | <0.001 | 5.07 (1.98–13.01) | 0.001 | ||||||
| 37–39 | 59.2 (174) | 40.8 (120) | 1.92 (1.14–3.24) | 0.014 | 1.96 (1.12–3.43) | 0.018 | ||||||
| 40+ | 73.6 (67) | 26.4 (24) | ||||||||||
| Birthweight (g) | ||||||||||||
| 0–2499 | 34.2 (13) | 65.8 (25) | 3.50 (1.59–7.73) | 0.002 | 1.11 (0.38–3.25) | 0.847 | ||||||
| 2500–3499 | 61.7 (171) | 38.3 (106) | 1.13 (0.70–1.83) | 0.619 | 1.26 (0.74–2.15) | 0.392 | ||||||
| 3500–3999 | 64.6 (62) | 35.4 (34) | ||||||||||
| 4000+ | 37.9 (11) | 62.1 (18) | 2.98 (1.26–7.04) | 0.013 | 2.63 (1.04–6.66) | 0.041 | ||||||
| Sex | ||||||||||||
| Boy | 54.9 (128) | 45.1 (105) | 1.35 (0.93–1.99) | 0.117 | 1.54 (1.00–2.36) | 0.047 | ||||||
| Girl | 62.3 (129) | 37.7 (78) | ||||||||||
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Age | ||||||||||||
| 14–34 | 59.9 (232) | 40.1 (155) | ||||||||||
| 35+ | 47.2 (25) | 52.8 (28) | 1.67 (0.94–2.98) | 0.079 | 1.50 (0.79–2.84) | 0.211 | ||||||
| Marital status | ||||||||||||
| Married | 57.1 (228) | 42.9 (171) | ||||||||||
| Unmarried/Divorced | 70.7 (29) | 29.3 (12) | 1.81 (0.90–3.65) | 0.097 | 2.08 (0.93–4.68) | 0.076 | ||||||
| No of live births | ||||||||||||
| 3+ | 72.2 (26) | 27.8 (10) | ||||||||||
| 2 | 50.5 (56) | 49.5 (55) | 2.55 (1.12–5.78) | 0.025 | 3.42 (1.34–8.76) | 0.010 | ||||||
| 1 | 60.7 (170) | 39.3 (110) | 1.68 (0.78–3.62) | 0.185 | 2.16 (0.88–5.30) | 0.090 | ||||||
| 1 (stillbirth) | 38.5 (5) | 61.5 (8) | 4.16 (1.09–15.78) | 0.036 | 1.74 (0.35–8.54) | 0.497 | ||||||
| BMI | ||||||||||||
| <20 | 64.9 (50) | 35.1 (27) | ||||||||||
| 20–25 | 58.7 (166) | 41.3 (117) | 1.30 (0.77–2.20) | 0.320 | 1.28 (0.72–2.27) | 0.388 | ||||||
| 25–30 | 58.5 (38) | 41.5 (27) | 1.31 (0.67–2.60) | 0.429 | 1.24 (0.56–2.65) | 0.582 | ||||||
| 30+ | 20.0 (3) | 80.0 (12) | 7.41 (1.92–28.54) | 0.004 | 13.82 (3.08–61.95) | 0.001 | ||||||
| Weight gain during pregnancy (kg) | ||||||||||||
| 0–10 | 63.5 (73) | 36.5 (42) | ||||||||||
| 11–20 | 57.4 (163) | 42.6 (121) | 1.29 (0.83–2.02) | 0.263 | 2.25 (1.30–3.90) | 0.004 | ||||||
| 21+ | 51.2 (21) | 48.8 (20) | 1.65 (0.80–3.40) | 0.170 | 2.56 (1.07–6.10) | 0.034 | ||||||
| Gestational age (weeks) | ||||||||||||
| <32 | 12.5 (2) | 87.5 (14) | 19.51 (4.13–92.17) | <0.001 | 46.27 (7.23–294.28) | <0.001 | ||||||
| 32–36 | 35.9 (14) | 64.1 (25) | 4.98 (2.23–11.13) | <0.001 | 5.07 (1.98–13.01) | 0.001 | ||||||
| 37–39 | 59.2 (174) | 40.8 (120) | 1.92 (1.14–3.24) | 0.014 | 1.96 (1.12–3.43) | 0.018 | ||||||
| 40+ | 73.6 (67) | 26.4 (24) | ||||||||||
| Birthweight (g) | ||||||||||||
| 0–2499 | 34.2 (13) | 65.8 (25) | 3.50 (1.59–7.73) | 0.002 | 1.11 (0.38–3.25) | 0.847 | ||||||
| 2500–3499 | 61.7 (171) | 38.3 (106) | 1.13 (0.70–1.83) | 0.619 | 1.26 (0.74–2.15) | 0.392 | ||||||
| 3500–3999 | 64.6 (62) | 35.4 (34) | ||||||||||
| 4000+ | 37.9 (11) | 62.1 (18) | 2.98 (1.26–7.04) | 0.013 | 2.63 (1.04–6.66) | 0.041 | ||||||
| Sex | ||||||||||||
| Boy | 54.9 (128) | 45.1 (105) | 1.35 (0.93–1.99) | 0.117 | 1.54 (1.00–2.36) | 0.047 | ||||||
| Girl | 62.3 (129) | 37.7 (78) | ||||||||||
Data for CS delivery of singleton babies according to demographic and reproductive variables in the public hospitals
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Age | ||||||||||||
| 14–34 | 59.9 (232) | 40.1 (155) | ||||||||||
| 35+ | 47.2 (25) | 52.8 (28) | 1.67 (0.94–2.98) | 0.079 | 1.50 (0.79–2.84) | 0.211 | ||||||
| Marital status | ||||||||||||
| Married | 57.1 (228) | 42.9 (171) | ||||||||||
| Unmarried/Divorced | 70.7 (29) | 29.3 (12) | 1.81 (0.90–3.65) | 0.097 | 2.08 (0.93–4.68) | 0.076 | ||||||
| No of live births | ||||||||||||
| 3+ | 72.2 (26) | 27.8 (10) | ||||||||||
| 2 | 50.5 (56) | 49.5 (55) | 2.55 (1.12–5.78) | 0.025 | 3.42 (1.34–8.76) | 0.010 | ||||||
| 1 | 60.7 (170) | 39.3 (110) | 1.68 (0.78–3.62) | 0.185 | 2.16 (0.88–5.30) | 0.090 | ||||||
| 1 (stillbirth) | 38.5 (5) | 61.5 (8) | 4.16 (1.09–15.78) | 0.036 | 1.74 (0.35–8.54) | 0.497 | ||||||
| BMI | ||||||||||||
| <20 | 64.9 (50) | 35.1 (27) | ||||||||||
| 20–25 | 58.7 (166) | 41.3 (117) | 1.30 (0.77–2.20) | 0.320 | 1.28 (0.72–2.27) | 0.388 | ||||||
| 25–30 | 58.5 (38) | 41.5 (27) | 1.31 (0.67–2.60) | 0.429 | 1.24 (0.56–2.65) | 0.582 | ||||||
| 30+ | 20.0 (3) | 80.0 (12) | 7.41 (1.92–28.54) | 0.004 | 13.82 (3.08–61.95) | 0.001 | ||||||
| Weight gain during pregnancy (kg) | ||||||||||||
| 0–10 | 63.5 (73) | 36.5 (42) | ||||||||||
| 11–20 | 57.4 (163) | 42.6 (121) | 1.29 (0.83–2.02) | 0.263 | 2.25 (1.30–3.90) | 0.004 | ||||||
| 21+ | 51.2 (21) | 48.8 (20) | 1.65 (0.80–3.40) | 0.170 | 2.56 (1.07–6.10) | 0.034 | ||||||
| Gestational age (weeks) | ||||||||||||
| <32 | 12.5 (2) | 87.5 (14) | 19.51 (4.13–92.17) | <0.001 | 46.27 (7.23–294.28) | <0.001 | ||||||
| 32–36 | 35.9 (14) | 64.1 (25) | 4.98 (2.23–11.13) | <0.001 | 5.07 (1.98–13.01) | 0.001 | ||||||
| 37–39 | 59.2 (174) | 40.8 (120) | 1.92 (1.14–3.24) | 0.014 | 1.96 (1.12–3.43) | 0.018 | ||||||
| 40+ | 73.6 (67) | 26.4 (24) | ||||||||||
| Birthweight (g) | ||||||||||||
| 0–2499 | 34.2 (13) | 65.8 (25) | 3.50 (1.59–7.73) | 0.002 | 1.11 (0.38–3.25) | 0.847 | ||||||
| 2500–3499 | 61.7 (171) | 38.3 (106) | 1.13 (0.70–1.83) | 0.619 | 1.26 (0.74–2.15) | 0.392 | ||||||
| 3500–3999 | 64.6 (62) | 35.4 (34) | ||||||||||
| 4000+ | 37.9 (11) | 62.1 (18) | 2.98 (1.26–7.04) | 0.013 | 2.63 (1.04–6.66) | 0.041 | ||||||
| Sex | ||||||||||||
| Boy | 54.9 (128) | 45.1 (105) | 1.35 (0.93–1.99) | 0.117 | 1.54 (1.00–2.36) | 0.047 | ||||||
| Girl | 62.3 (129) | 37.7 (78) | ||||||||||
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Age | ||||||||||||
| 14–34 | 59.9 (232) | 40.1 (155) | ||||||||||
| 35+ | 47.2 (25) | 52.8 (28) | 1.67 (0.94–2.98) | 0.079 | 1.50 (0.79–2.84) | 0.211 | ||||||
| Marital status | ||||||||||||
| Married | 57.1 (228) | 42.9 (171) | ||||||||||
| Unmarried/Divorced | 70.7 (29) | 29.3 (12) | 1.81 (0.90–3.65) | 0.097 | 2.08 (0.93–4.68) | 0.076 | ||||||
| No of live births | ||||||||||||
| 3+ | 72.2 (26) | 27.8 (10) | ||||||||||
| 2 | 50.5 (56) | 49.5 (55) | 2.55 (1.12–5.78) | 0.025 | 3.42 (1.34–8.76) | 0.010 | ||||||
| 1 | 60.7 (170) | 39.3 (110) | 1.68 (0.78–3.62) | 0.185 | 2.16 (0.88–5.30) | 0.090 | ||||||
| 1 (stillbirth) | 38.5 (5) | 61.5 (8) | 4.16 (1.09–15.78) | 0.036 | 1.74 (0.35–8.54) | 0.497 | ||||||
| BMI | ||||||||||||
| <20 | 64.9 (50) | 35.1 (27) | ||||||||||
| 20–25 | 58.7 (166) | 41.3 (117) | 1.30 (0.77–2.20) | 0.320 | 1.28 (0.72–2.27) | 0.388 | ||||||
| 25–30 | 58.5 (38) | 41.5 (27) | 1.31 (0.67–2.60) | 0.429 | 1.24 (0.56–2.65) | 0.582 | ||||||
| 30+ | 20.0 (3) | 80.0 (12) | 7.41 (1.92–28.54) | 0.004 | 13.82 (3.08–61.95) | 0.001 | ||||||
| Weight gain during pregnancy (kg) | ||||||||||||
| 0–10 | 63.5 (73) | 36.5 (42) | ||||||||||
| 11–20 | 57.4 (163) | 42.6 (121) | 1.29 (0.83–2.02) | 0.263 | 2.25 (1.30–3.90) | 0.004 | ||||||
| 21+ | 51.2 (21) | 48.8 (20) | 1.65 (0.80–3.40) | 0.170 | 2.56 (1.07–6.10) | 0.034 | ||||||
| Gestational age (weeks) | ||||||||||||
| <32 | 12.5 (2) | 87.5 (14) | 19.51 (4.13–92.17) | <0.001 | 46.27 (7.23–294.28) | <0.001 | ||||||
| 32–36 | 35.9 (14) | 64.1 (25) | 4.98 (2.23–11.13) | <0.001 | 5.07 (1.98–13.01) | 0.001 | ||||||
| 37–39 | 59.2 (174) | 40.8 (120) | 1.92 (1.14–3.24) | 0.014 | 1.96 (1.12–3.43) | 0.018 | ||||||
| 40+ | 73.6 (67) | 26.4 (24) | ||||||||||
| Birthweight (g) | ||||||||||||
| 0–2499 | 34.2 (13) | 65.8 (25) | 3.50 (1.59–7.73) | 0.002 | 1.11 (0.38–3.25) | 0.847 | ||||||
| 2500–3499 | 61.7 (171) | 38.3 (106) | 1.13 (0.70–1.83) | 0.619 | 1.26 (0.74–2.15) | 0.392 | ||||||
| 3500–3999 | 64.6 (62) | 35.4 (34) | ||||||||||
| 4000+ | 37.9 (11) | 62.1 (18) | 2.98 (1.26–7.04) | 0.013 | 2.63 (1.04–6.66) | 0.041 | ||||||
| Sex | ||||||||||||
| Boy | 54.9 (128) | 45.1 (105) | 1.35 (0.93–1.99) | 0.117 | 1.54 (1.00–2.36) | 0.047 | ||||||
| Girl | 62.3 (129) | 37.7 (78) | ||||||||||
Data on CS delivery of singleton babies according to socio-economic and health service variables in the public hospitals
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Ethnic group | ||||||||||||
| Greek | 47.5 (123) | 52.5 (136) | 3.15 (2.09–4.76) | <0.001 | 2.70 (1.73–4.23) | <0.001 | ||||||
| Immigrants | 74.0 (134) | 26.0 (47) | ||||||||||
| Occupational group | ||||||||||||
| Household/unemployed | 63.2 (177) | 36.8 (103) | ||||||||||
| Employed | 50.0 (80) | 50.0 (80) | 1.71 (1.16–2.55) | 0.007 | 1.16 (0.48–1.80) | 0.512 | ||||||
| Time of delivery | ||||||||||||
| 12a.m.–8a.m. | 79.5 (58) | 20.5 (15) | ||||||||||
| 8a.m.–4p.m. | 47.4 (120) | 52.6 (133) | 4.28 (2.31–7.96) | <0.001 | 4.04 (2.13–7.67) | <0.001 | ||||||
| 4p.m.–midnight | 69.3 (79) | 30.7 (35) | 1.71 (0.86–3.43) | 0.128 | 2.03 (0.99–4.18) | 0.054 | ||||||
| Day of delivery | ||||||||||||
| Monday | 55.6 (40) | 44.4 (32) | 2.76 (1.22–6.25) | 0.015 | 2.58 (1.09–6.11) | 0.031 | ||||||
| Tuesday | 61.8 (47) | 38.2 (29) | 2.13 (0.94–4.82) | 0.069 | 1.95 (0.82–4.66) | 0.131 | ||||||
| Wednesday | 52.1 (38) | 47.9 (35) | 3.18 (1.41–7.17) | 0.005 | 2.51 (1.06–5.94) | 0.035 | ||||||
| Thursday | 57.1 (32) | 42.9 (24) | 2.59 (1.10–6.09) | 0.029 | 2.27 (0.92–5.62) | 0.075 | ||||||
| Friday | 50.7 (35) | 49.3 (34) | 3.36 (1.48–7.62) | 0.004 | 2.69 (1.13–6.41) | 0.025 | ||||||
| Saturday | 60.0 (27) | 40.0 (18) | 2.30 (0.94–5.65) | 0.069 | 2.21 (0.85–5.72) | 0.102 | ||||||
| Sunday | 77.6 (38) | 22.4 (11) | ||||||||||
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Ethnic group | ||||||||||||
| Greek | 47.5 (123) | 52.5 (136) | 3.15 (2.09–4.76) | <0.001 | 2.70 (1.73–4.23) | <0.001 | ||||||
| Immigrants | 74.0 (134) | 26.0 (47) | ||||||||||
| Occupational group | ||||||||||||
| Household/unemployed | 63.2 (177) | 36.8 (103) | ||||||||||
| Employed | 50.0 (80) | 50.0 (80) | 1.71 (1.16–2.55) | 0.007 | 1.16 (0.48–1.80) | 0.512 | ||||||
| Time of delivery | ||||||||||||
| 12a.m.–8a.m. | 79.5 (58) | 20.5 (15) | ||||||||||
| 8a.m.–4p.m. | 47.4 (120) | 52.6 (133) | 4.28 (2.31–7.96) | <0.001 | 4.04 (2.13–7.67) | <0.001 | ||||||
| 4p.m.–midnight | 69.3 (79) | 30.7 (35) | 1.71 (0.86–3.43) | 0.128 | 2.03 (0.99–4.18) | 0.054 | ||||||
| Day of delivery | ||||||||||||
| Monday | 55.6 (40) | 44.4 (32) | 2.76 (1.22–6.25) | 0.015 | 2.58 (1.09–6.11) | 0.031 | ||||||
| Tuesday | 61.8 (47) | 38.2 (29) | 2.13 (0.94–4.82) | 0.069 | 1.95 (0.82–4.66) | 0.131 | ||||||
| Wednesday | 52.1 (38) | 47.9 (35) | 3.18 (1.41–7.17) | 0.005 | 2.51 (1.06–5.94) | 0.035 | ||||||
| Thursday | 57.1 (32) | 42.9 (24) | 2.59 (1.10–6.09) | 0.029 | 2.27 (0.92–5.62) | 0.075 | ||||||
| Friday | 50.7 (35) | 49.3 (34) | 3.36 (1.48–7.62) | 0.004 | 2.69 (1.13–6.41) | 0.025 | ||||||
| Saturday | 60.0 (27) | 40.0 (18) | 2.30 (0.94–5.65) | 0.069 | 2.21 (0.85–5.72) | 0.102 | ||||||
| Sunday | 77.6 (38) | 22.4 (11) | ||||||||||
Data on CS delivery of singleton babies according to socio-economic and health service variables in the public hospitals
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Ethnic group | ||||||||||||
| Greek | 47.5 (123) | 52.5 (136) | 3.15 (2.09–4.76) | <0.001 | 2.70 (1.73–4.23) | <0.001 | ||||||
| Immigrants | 74.0 (134) | 26.0 (47) | ||||||||||
| Occupational group | ||||||||||||
| Household/unemployed | 63.2 (177) | 36.8 (103) | ||||||||||
| Employed | 50.0 (80) | 50.0 (80) | 1.71 (1.16–2.55) | 0.007 | 1.16 (0.48–1.80) | 0.512 | ||||||
| Time of delivery | ||||||||||||
| 12a.m.–8a.m. | 79.5 (58) | 20.5 (15) | ||||||||||
| 8a.m.–4p.m. | 47.4 (120) | 52.6 (133) | 4.28 (2.31–7.96) | <0.001 | 4.04 (2.13–7.67) | <0.001 | ||||||
| 4p.m.–midnight | 69.3 (79) | 30.7 (35) | 1.71 (0.86–3.43) | 0.128 | 2.03 (0.99–4.18) | 0.054 | ||||||
| Day of delivery | ||||||||||||
| Monday | 55.6 (40) | 44.4 (32) | 2.76 (1.22–6.25) | 0.015 | 2.58 (1.09–6.11) | 0.031 | ||||||
| Tuesday | 61.8 (47) | 38.2 (29) | 2.13 (0.94–4.82) | 0.069 | 1.95 (0.82–4.66) | 0.131 | ||||||
| Wednesday | 52.1 (38) | 47.9 (35) | 3.18 (1.41–7.17) | 0.005 | 2.51 (1.06–5.94) | 0.035 | ||||||
| Thursday | 57.1 (32) | 42.9 (24) | 2.59 (1.10–6.09) | 0.029 | 2.27 (0.92–5.62) | 0.075 | ||||||
| Friday | 50.7 (35) | 49.3 (34) | 3.36 (1.48–7.62) | 0.004 | 2.69 (1.13–6.41) | 0.025 | ||||||
| Saturday | 60.0 (27) | 40.0 (18) | 2.30 (0.94–5.65) | 0.069 | 2.21 (0.85–5.72) | 0.102 | ||||||
| Sunday | 77.6 (38) | 22.4 (11) | ||||||||||
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Ethnic group | ||||||||||||
| Greek | 47.5 (123) | 52.5 (136) | 3.15 (2.09–4.76) | <0.001 | 2.70 (1.73–4.23) | <0.001 | ||||||
| Immigrants | 74.0 (134) | 26.0 (47) | ||||||||||
| Occupational group | ||||||||||||
| Household/unemployed | 63.2 (177) | 36.8 (103) | ||||||||||
| Employed | 50.0 (80) | 50.0 (80) | 1.71 (1.16–2.55) | 0.007 | 1.16 (0.48–1.80) | 0.512 | ||||||
| Time of delivery | ||||||||||||
| 12a.m.–8a.m. | 79.5 (58) | 20.5 (15) | ||||||||||
| 8a.m.–4p.m. | 47.4 (120) | 52.6 (133) | 4.28 (2.31–7.96) | <0.001 | 4.04 (2.13–7.67) | <0.001 | ||||||
| 4p.m.–midnight | 69.3 (79) | 30.7 (35) | 1.71 (0.86–3.43) | 0.128 | 2.03 (0.99–4.18) | 0.054 | ||||||
| Day of delivery | ||||||||||||
| Monday | 55.6 (40) | 44.4 (32) | 2.76 (1.22–6.25) | 0.015 | 2.58 (1.09–6.11) | 0.031 | ||||||
| Tuesday | 61.8 (47) | 38.2 (29) | 2.13 (0.94–4.82) | 0.069 | 1.95 (0.82–4.66) | 0.131 | ||||||
| Wednesday | 52.1 (38) | 47.9 (35) | 3.18 (1.41–7.17) | 0.005 | 2.51 (1.06–5.94) | 0.035 | ||||||
| Thursday | 57.1 (32) | 42.9 (24) | 2.59 (1.10–6.09) | 0.029 | 2.27 (0.92–5.62) | 0.075 | ||||||
| Friday | 50.7 (35) | 49.3 (34) | 3.36 (1.48–7.62) | 0.004 | 2.69 (1.13–6.41) | 0.025 | ||||||
| Saturday | 60.0 (27) | 40.0 (18) | 2.30 (0.94–5.65) | 0.069 | 2.21 (0.85–5.72) | 0.102 | ||||||
| Sunday | 77.6 (38) | 22.4 (11) | ||||||||||
Data for CS delivery of singleton babies according to demographic and reproductive variables in the private hospital
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Age | ||||||||||||
| 14–34 | 46.8 (139) | 53.2 (158) | ||||||||||
| 35+ | 48.5 (33) | 51.5 (35) | 1.07 (0.63–1.82) | 0.797 | 1.22 (0.64–2.31) | 0.540 | ||||||
| No of live births | ||||||||||||
| 3+ | 48.3 (14) | 51.7 (15) | 1.90 (0.84–4.30) | 0.124 | 1.96 (0.77–4.98) | 0.156 | ||||||
| 2 | 63.9 (78) | 36.1 (44) | ||||||||||
| 1 | 38.2 (78) | 61.8 (126) | 2.86 (1.80–4.56) | <0.001 | 4.01 (2.35–6.84) | <0.001 | ||||||
| 1 (stillbirth) | 20.0 (2) | 80.0 (8) | 7.09 (1.44–34.87) | 0.016 | 1.36 (0.21–9.00) | 0.749 | ||||||
| BMI | ||||||||||||
| <20 | 52.0 (26) | 48.0 (24) | ||||||||||
| 20–25 | 46.4 (115) | 53.6 (133) | 1.25 (0.68–2.30) | 0.468 | 1.66 (0.82–3.35) | 0.158 | ||||||
| 25–30 | 47.4 (27) | 52.6 (30) | 1.20 (0.56–2.57) | 0.633 | 1.50 (0.63–3.60) | 0.363 | ||||||
| 30+ | 40.0 (4) | 60.0 (6) | 1.62 (0.41–6.47) | 0.491 | 1.37 (0.28–6.52) | 0.694 | ||||||
| Weight gain during pregnancy (kg) | ||||||||||||
| 0–10 | 44.6 (37) | 55.4 (46) | 1.24 (0.57–2.68) | 0.579 | 2.36 (0.92–6.05) | 0.075 | ||||||
| 11–20 | 47.5 (116) | 52.5 (128) | 1.10 (0.56–2.19) | 0.778 | 2.12 (0.93–4.81) | 0.720 | ||||||
| 21+ | 50.0 (19) | 50.0 (19) | ||||||||||
| Gestational age (weeks) | ||||||||||||
| <32 | 7.7 (1) | 92.3 (12) | 29.10 (3.64–232.47) | 0.001 | 16.18 (1.42–183.78) | 0.025 | ||||||
| 32–36 | 23.3 (10) | 76.7 (33) | 8.12 (3.50–18.84) | <0.001 | 8.77 (3.29–23.33) | <0.001 | ||||||
| 37–39 | 44.3 (97) | 55.7 (122) | 3.10 (1.83–5.25) | <0.001 | 3.82 (2.13–6.85) | <0.001 | ||||||
| 40+ | 71.1 (64) | 28.9 (26) | ||||||||||
| Birthweight (g) | ||||||||||||
| 0–2499 | 13.6 (3) | 86.4 (19) | 8.90 (2.43–32.62) | 0.001 | 4.39 (0.95–20.38) | 0.059 | ||||||
| 2500–3499 | 49.6 (119) | 50.4 (121) | 1.43 (0.85–2.40) | 0.177 | 1.27 (0.71–2.28) | 0.419 | ||||||
| 3500–3999 | 58.4 (45) | 41.6 (32) | ||||||||||
| 4000+ | 19.2 (5) | 80.8 (21) | 5.91 (2.01–17.31) | 0.001 | 5.39 (1.53–18.95) | 0.009 | ||||||
| Sex | ||||||||||||
| Boy | 43.4 (76) | 56.6 (99) | 1.33 (0.88–2.01) | 0.175 | 1.47 (0.90–2.40) | 0.119 | ||||||
| Girl | 50.5 (96) | 49.5 (94) | ||||||||||
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Age | ||||||||||||
| 14–34 | 46.8 (139) | 53.2 (158) | ||||||||||
| 35+ | 48.5 (33) | 51.5 (35) | 1.07 (0.63–1.82) | 0.797 | 1.22 (0.64–2.31) | 0.540 | ||||||
| No of live births | ||||||||||||
| 3+ | 48.3 (14) | 51.7 (15) | 1.90 (0.84–4.30) | 0.124 | 1.96 (0.77–4.98) | 0.156 | ||||||
| 2 | 63.9 (78) | 36.1 (44) | ||||||||||
| 1 | 38.2 (78) | 61.8 (126) | 2.86 (1.80–4.56) | <0.001 | 4.01 (2.35–6.84) | <0.001 | ||||||
| 1 (stillbirth) | 20.0 (2) | 80.0 (8) | 7.09 (1.44–34.87) | 0.016 | 1.36 (0.21–9.00) | 0.749 | ||||||
| BMI | ||||||||||||
| <20 | 52.0 (26) | 48.0 (24) | ||||||||||
| 20–25 | 46.4 (115) | 53.6 (133) | 1.25 (0.68–2.30) | 0.468 | 1.66 (0.82–3.35) | 0.158 | ||||||
| 25–30 | 47.4 (27) | 52.6 (30) | 1.20 (0.56–2.57) | 0.633 | 1.50 (0.63–3.60) | 0.363 | ||||||
| 30+ | 40.0 (4) | 60.0 (6) | 1.62 (0.41–6.47) | 0.491 | 1.37 (0.28–6.52) | 0.694 | ||||||
| Weight gain during pregnancy (kg) | ||||||||||||
| 0–10 | 44.6 (37) | 55.4 (46) | 1.24 (0.57–2.68) | 0.579 | 2.36 (0.92–6.05) | 0.075 | ||||||
| 11–20 | 47.5 (116) | 52.5 (128) | 1.10 (0.56–2.19) | 0.778 | 2.12 (0.93–4.81) | 0.720 | ||||||
| 21+ | 50.0 (19) | 50.0 (19) | ||||||||||
| Gestational age (weeks) | ||||||||||||
| <32 | 7.7 (1) | 92.3 (12) | 29.10 (3.64–232.47) | 0.001 | 16.18 (1.42–183.78) | 0.025 | ||||||
| 32–36 | 23.3 (10) | 76.7 (33) | 8.12 (3.50–18.84) | <0.001 | 8.77 (3.29–23.33) | <0.001 | ||||||
| 37–39 | 44.3 (97) | 55.7 (122) | 3.10 (1.83–5.25) | <0.001 | 3.82 (2.13–6.85) | <0.001 | ||||||
| 40+ | 71.1 (64) | 28.9 (26) | ||||||||||
| Birthweight (g) | ||||||||||||
| 0–2499 | 13.6 (3) | 86.4 (19) | 8.90 (2.43–32.62) | 0.001 | 4.39 (0.95–20.38) | 0.059 | ||||||
| 2500–3499 | 49.6 (119) | 50.4 (121) | 1.43 (0.85–2.40) | 0.177 | 1.27 (0.71–2.28) | 0.419 | ||||||
| 3500–3999 | 58.4 (45) | 41.6 (32) | ||||||||||
| 4000+ | 19.2 (5) | 80.8 (21) | 5.91 (2.01–17.31) | 0.001 | 5.39 (1.53–18.95) | 0.009 | ||||||
| Sex | ||||||||||||
| Boy | 43.4 (76) | 56.6 (99) | 1.33 (0.88–2.01) | 0.175 | 1.47 (0.90–2.40) | 0.119 | ||||||
| Girl | 50.5 (96) | 49.5 (94) | ||||||||||
Data for CS delivery of singleton babies according to demographic and reproductive variables in the private hospital
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Age | ||||||||||||
| 14–34 | 46.8 (139) | 53.2 (158) | ||||||||||
| 35+ | 48.5 (33) | 51.5 (35) | 1.07 (0.63–1.82) | 0.797 | 1.22 (0.64–2.31) | 0.540 | ||||||
| No of live births | ||||||||||||
| 3+ | 48.3 (14) | 51.7 (15) | 1.90 (0.84–4.30) | 0.124 | 1.96 (0.77–4.98) | 0.156 | ||||||
| 2 | 63.9 (78) | 36.1 (44) | ||||||||||
| 1 | 38.2 (78) | 61.8 (126) | 2.86 (1.80–4.56) | <0.001 | 4.01 (2.35–6.84) | <0.001 | ||||||
| 1 (stillbirth) | 20.0 (2) | 80.0 (8) | 7.09 (1.44–34.87) | 0.016 | 1.36 (0.21–9.00) | 0.749 | ||||||
| BMI | ||||||||||||
| <20 | 52.0 (26) | 48.0 (24) | ||||||||||
| 20–25 | 46.4 (115) | 53.6 (133) | 1.25 (0.68–2.30) | 0.468 | 1.66 (0.82–3.35) | 0.158 | ||||||
| 25–30 | 47.4 (27) | 52.6 (30) | 1.20 (0.56–2.57) | 0.633 | 1.50 (0.63–3.60) | 0.363 | ||||||
| 30+ | 40.0 (4) | 60.0 (6) | 1.62 (0.41–6.47) | 0.491 | 1.37 (0.28–6.52) | 0.694 | ||||||
| Weight gain during pregnancy (kg) | ||||||||||||
| 0–10 | 44.6 (37) | 55.4 (46) | 1.24 (0.57–2.68) | 0.579 | 2.36 (0.92–6.05) | 0.075 | ||||||
| 11–20 | 47.5 (116) | 52.5 (128) | 1.10 (0.56–2.19) | 0.778 | 2.12 (0.93–4.81) | 0.720 | ||||||
| 21+ | 50.0 (19) | 50.0 (19) | ||||||||||
| Gestational age (weeks) | ||||||||||||
| <32 | 7.7 (1) | 92.3 (12) | 29.10 (3.64–232.47) | 0.001 | 16.18 (1.42–183.78) | 0.025 | ||||||
| 32–36 | 23.3 (10) | 76.7 (33) | 8.12 (3.50–18.84) | <0.001 | 8.77 (3.29–23.33) | <0.001 | ||||||
| 37–39 | 44.3 (97) | 55.7 (122) | 3.10 (1.83–5.25) | <0.001 | 3.82 (2.13–6.85) | <0.001 | ||||||
| 40+ | 71.1 (64) | 28.9 (26) | ||||||||||
| Birthweight (g) | ||||||||||||
| 0–2499 | 13.6 (3) | 86.4 (19) | 8.90 (2.43–32.62) | 0.001 | 4.39 (0.95–20.38) | 0.059 | ||||||
| 2500–3499 | 49.6 (119) | 50.4 (121) | 1.43 (0.85–2.40) | 0.177 | 1.27 (0.71–2.28) | 0.419 | ||||||
| 3500–3999 | 58.4 (45) | 41.6 (32) | ||||||||||
| 4000+ | 19.2 (5) | 80.8 (21) | 5.91 (2.01–17.31) | 0.001 | 5.39 (1.53–18.95) | 0.009 | ||||||
| Sex | ||||||||||||
| Boy | 43.4 (76) | 56.6 (99) | 1.33 (0.88–2.01) | 0.175 | 1.47 (0.90–2.40) | 0.119 | ||||||
| Girl | 50.5 (96) | 49.5 (94) | ||||||||||
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Age | ||||||||||||
| 14–34 | 46.8 (139) | 53.2 (158) | ||||||||||
| 35+ | 48.5 (33) | 51.5 (35) | 1.07 (0.63–1.82) | 0.797 | 1.22 (0.64–2.31) | 0.540 | ||||||
| No of live births | ||||||||||||
| 3+ | 48.3 (14) | 51.7 (15) | 1.90 (0.84–4.30) | 0.124 | 1.96 (0.77–4.98) | 0.156 | ||||||
| 2 | 63.9 (78) | 36.1 (44) | ||||||||||
| 1 | 38.2 (78) | 61.8 (126) | 2.86 (1.80–4.56) | <0.001 | 4.01 (2.35–6.84) | <0.001 | ||||||
| 1 (stillbirth) | 20.0 (2) | 80.0 (8) | 7.09 (1.44–34.87) | 0.016 | 1.36 (0.21–9.00) | 0.749 | ||||||
| BMI | ||||||||||||
| <20 | 52.0 (26) | 48.0 (24) | ||||||||||
| 20–25 | 46.4 (115) | 53.6 (133) | 1.25 (0.68–2.30) | 0.468 | 1.66 (0.82–3.35) | 0.158 | ||||||
| 25–30 | 47.4 (27) | 52.6 (30) | 1.20 (0.56–2.57) | 0.633 | 1.50 (0.63–3.60) | 0.363 | ||||||
| 30+ | 40.0 (4) | 60.0 (6) | 1.62 (0.41–6.47) | 0.491 | 1.37 (0.28–6.52) | 0.694 | ||||||
| Weight gain during pregnancy (kg) | ||||||||||||
| 0–10 | 44.6 (37) | 55.4 (46) | 1.24 (0.57–2.68) | 0.579 | 2.36 (0.92–6.05) | 0.075 | ||||||
| 11–20 | 47.5 (116) | 52.5 (128) | 1.10 (0.56–2.19) | 0.778 | 2.12 (0.93–4.81) | 0.720 | ||||||
| 21+ | 50.0 (19) | 50.0 (19) | ||||||||||
| Gestational age (weeks) | ||||||||||||
| <32 | 7.7 (1) | 92.3 (12) | 29.10 (3.64–232.47) | 0.001 | 16.18 (1.42–183.78) | 0.025 | ||||||
| 32–36 | 23.3 (10) | 76.7 (33) | 8.12 (3.50–18.84) | <0.001 | 8.77 (3.29–23.33) | <0.001 | ||||||
| 37–39 | 44.3 (97) | 55.7 (122) | 3.10 (1.83–5.25) | <0.001 | 3.82 (2.13–6.85) | <0.001 | ||||||
| 40+ | 71.1 (64) | 28.9 (26) | ||||||||||
| Birthweight (g) | ||||||||||||
| 0–2499 | 13.6 (3) | 86.4 (19) | 8.90 (2.43–32.62) | 0.001 | 4.39 (0.95–20.38) | 0.059 | ||||||
| 2500–3499 | 49.6 (119) | 50.4 (121) | 1.43 (0.85–2.40) | 0.177 | 1.27 (0.71–2.28) | 0.419 | ||||||
| 3500–3999 | 58.4 (45) | 41.6 (32) | ||||||||||
| 4000+ | 19.2 (5) | 80.8 (21) | 5.91 (2.01–17.31) | 0.001 | 5.39 (1.53–18.95) | 0.009 | ||||||
| Sex | ||||||||||||
| Boy | 43.4 (76) | 56.6 (99) | 1.33 (0.88–2.01) | 0.175 | 1.47 (0.90–2.40) | 0.119 | ||||||
| Girl | 50.5 (96) | 49.5 (94) | ||||||||||
Data for CS delivery of singleton babies according to socio-economic and health service variables in the private hospital
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Payment method | ||||||||||||
| Out-of-pocket | 76.1 (83) | 23.9 (26) | ||||||||||
| Private insurance | 34.8 (89) | 65.2 (167) | 5.99 (3.60–9.98) | <0.001 | 7.73 (4.46–13.39) | <0.001 | ||||||
| Occupational group | ||||||||||||
| Household/unemployed | 44.1 (64) | 55.9 (81) | 1.22 (0.80–1.86) | 0.354 | 1.69 (1.04–2.74) | 0.034 | ||||||
| Employed | 49.1 (108) | 50.9 (112) | ||||||||||
| Time of delivery | ||||||||||||
| 12a.m.–8a.m. | 64.2 (34) | 35.8 (19) | ||||||||||
| 8a.m.–4p.m. | 43.8 (102) | 56.2 (131) | 2.30 (1.24–4.26) | 0.008 | 2.90 (1.48–5.69) | 0.002 | ||||||
| 4p.m.–midnight | 45.6 (36) | 54.4 (43) | 2.14 (1.05–4.37) | 0.037 | 2.53 (1.16–5.51) | 0.020 | ||||||
| Day of delivery | ||||||||||||
| Monday | 54.9 (28) | 45.1 (23) | 1.07 (0.40–2.88) | 0.897 | 1.24 (0.42–3.63) | 0.700 | ||||||
| Tuesday | 42.3 (30) | 57.7 (41) | 1.78 (0.69–4.59) | 0.235 | 2.17 (0.77–6.15) | 0.144 | ||||||
| Wednesday | 45.7 (21) | 54.3 (25) | 1.55 (0.56–4.24) | 0.396 | 1.44 (0.48–4.32) | 0.510 | ||||||
| Thursday | 52.0 (26) | 48.0 (24) | 1.20 (0.44–3.24) | 0.719 | 1.14 (0.39–3.36) | 0.802 | ||||||
| Friday | 46.7 (28) | 53.3 (32) | 1.49 (0.56–3.91) | 0.423 | 1.84 (0.64–5.33) | 0.258 | ||||||
| Saturday | 40.6 (26) | 59.4 (38) | 1.90 (0.72–4.98) | 0.192 | 2.58 (0.89–7.48) | 0.080 | ||||||
| Sunday | 56.5 (13) | 43.5 (10) | ||||||||||
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Payment method | ||||||||||||
| Out-of-pocket | 76.1 (83) | 23.9 (26) | ||||||||||
| Private insurance | 34.8 (89) | 65.2 (167) | 5.99 (3.60–9.98) | <0.001 | 7.73 (4.46–13.39) | <0.001 | ||||||
| Occupational group | ||||||||||||
| Household/unemployed | 44.1 (64) | 55.9 (81) | 1.22 (0.80–1.86) | 0.354 | 1.69 (1.04–2.74) | 0.034 | ||||||
| Employed | 49.1 (108) | 50.9 (112) | ||||||||||
| Time of delivery | ||||||||||||
| 12a.m.–8a.m. | 64.2 (34) | 35.8 (19) | ||||||||||
| 8a.m.–4p.m. | 43.8 (102) | 56.2 (131) | 2.30 (1.24–4.26) | 0.008 | 2.90 (1.48–5.69) | 0.002 | ||||||
| 4p.m.–midnight | 45.6 (36) | 54.4 (43) | 2.14 (1.05–4.37) | 0.037 | 2.53 (1.16–5.51) | 0.020 | ||||||
| Day of delivery | ||||||||||||
| Monday | 54.9 (28) | 45.1 (23) | 1.07 (0.40–2.88) | 0.897 | 1.24 (0.42–3.63) | 0.700 | ||||||
| Tuesday | 42.3 (30) | 57.7 (41) | 1.78 (0.69–4.59) | 0.235 | 2.17 (0.77–6.15) | 0.144 | ||||||
| Wednesday | 45.7 (21) | 54.3 (25) | 1.55 (0.56–4.24) | 0.396 | 1.44 (0.48–4.32) | 0.510 | ||||||
| Thursday | 52.0 (26) | 48.0 (24) | 1.20 (0.44–3.24) | 0.719 | 1.14 (0.39–3.36) | 0.802 | ||||||
| Friday | 46.7 (28) | 53.3 (32) | 1.49 (0.56–3.91) | 0.423 | 1.84 (0.64–5.33) | 0.258 | ||||||
| Saturday | 40.6 (26) | 59.4 (38) | 1.90 (0.72–4.98) | 0.192 | 2.58 (0.89–7.48) | 0.080 | ||||||
| Sunday | 56.5 (13) | 43.5 (10) | ||||||||||
Data for CS delivery of singleton babies according to socio-economic and health service variables in the private hospital
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Payment method | ||||||||||||
| Out-of-pocket | 76.1 (83) | 23.9 (26) | ||||||||||
| Private insurance | 34.8 (89) | 65.2 (167) | 5.99 (3.60–9.98) | <0.001 | 7.73 (4.46–13.39) | <0.001 | ||||||
| Occupational group | ||||||||||||
| Household/unemployed | 44.1 (64) | 55.9 (81) | 1.22 (0.80–1.86) | 0.354 | 1.69 (1.04–2.74) | 0.034 | ||||||
| Employed | 49.1 (108) | 50.9 (112) | ||||||||||
| Time of delivery | ||||||||||||
| 12a.m.–8a.m. | 64.2 (34) | 35.8 (19) | ||||||||||
| 8a.m.–4p.m. | 43.8 (102) | 56.2 (131) | 2.30 (1.24–4.26) | 0.008 | 2.90 (1.48–5.69) | 0.002 | ||||||
| 4p.m.–midnight | 45.6 (36) | 54.4 (43) | 2.14 (1.05–4.37) | 0.037 | 2.53 (1.16–5.51) | 0.020 | ||||||
| Day of delivery | ||||||||||||
| Monday | 54.9 (28) | 45.1 (23) | 1.07 (0.40–2.88) | 0.897 | 1.24 (0.42–3.63) | 0.700 | ||||||
| Tuesday | 42.3 (30) | 57.7 (41) | 1.78 (0.69–4.59) | 0.235 | 2.17 (0.77–6.15) | 0.144 | ||||||
| Wednesday | 45.7 (21) | 54.3 (25) | 1.55 (0.56–4.24) | 0.396 | 1.44 (0.48–4.32) | 0.510 | ||||||
| Thursday | 52.0 (26) | 48.0 (24) | 1.20 (0.44–3.24) | 0.719 | 1.14 (0.39–3.36) | 0.802 | ||||||
| Friday | 46.7 (28) | 53.3 (32) | 1.49 (0.56–3.91) | 0.423 | 1.84 (0.64–5.33) | 0.258 | ||||||
| Saturday | 40.6 (26) | 59.4 (38) | 1.90 (0.72–4.98) | 0.192 | 2.58 (0.89–7.48) | 0.080 | ||||||
| Sunday | 56.5 (13) | 43.5 (10) | ||||||||||
| Variable | V Rate | CS Rate | Crude OR | Adjusted OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (n) | % (n) | (95% CI) | P-value | (95% CI) | P-value | |||||||
| Payment method | ||||||||||||
| Out-of-pocket | 76.1 (83) | 23.9 (26) | ||||||||||
| Private insurance | 34.8 (89) | 65.2 (167) | 5.99 (3.60–9.98) | <0.001 | 7.73 (4.46–13.39) | <0.001 | ||||||
| Occupational group | ||||||||||||
| Household/unemployed | 44.1 (64) | 55.9 (81) | 1.22 (0.80–1.86) | 0.354 | 1.69 (1.04–2.74) | 0.034 | ||||||
| Employed | 49.1 (108) | 50.9 (112) | ||||||||||
| Time of delivery | ||||||||||||
| 12a.m.–8a.m. | 64.2 (34) | 35.8 (19) | ||||||||||
| 8a.m.–4p.m. | 43.8 (102) | 56.2 (131) | 2.30 (1.24–4.26) | 0.008 | 2.90 (1.48–5.69) | 0.002 | ||||||
| 4p.m.–midnight | 45.6 (36) | 54.4 (43) | 2.14 (1.05–4.37) | 0.037 | 2.53 (1.16–5.51) | 0.020 | ||||||
| Day of delivery | ||||||||||||
| Monday | 54.9 (28) | 45.1 (23) | 1.07 (0.40–2.88) | 0.897 | 1.24 (0.42–3.63) | 0.700 | ||||||
| Tuesday | 42.3 (30) | 57.7 (41) | 1.78 (0.69–4.59) | 0.235 | 2.17 (0.77–6.15) | 0.144 | ||||||
| Wednesday | 45.7 (21) | 54.3 (25) | 1.55 (0.56–4.24) | 0.396 | 1.44 (0.48–4.32) | 0.510 | ||||||
| Thursday | 52.0 (26) | 48.0 (24) | 1.20 (0.44–3.24) | 0.719 | 1.14 (0.39–3.36) | 0.802 | ||||||
| Friday | 46.7 (28) | 53.3 (32) | 1.49 (0.56–3.91) | 0.423 | 1.84 (0.64–5.33) | 0.258 | ||||||
| Saturday | 40.6 (26) | 59.4 (38) | 1.90 (0.72–4.98) | 0.192 | 2.58 (0.89–7.48) | 0.080 | ||||||
| Sunday | 56.5 (13) | 43.5 (10) | ||||||||||
This paper investigates whether private health insurance (PMI), physician convenience and socio-economic status (derived from ethnic background) increase the odds of Caesarean Section (CS) in Greece.
Important non-medical predictors of CS include: Greek ethnicity, day-time and week-day delivery (public hospitals); PMI, day-time and Saturday delivery (private hospital).
The results of this study suggest that physicians are motivated to perform CS for financial and convenience incentives.
This study was financed by the LSE Health and Social Care, London School of Economics and Political Science.
Conflicts of Interest
None
References
Gomes UA, Silva AAM, Bettiol H, Barbieri MA. Risk factors for the increasing caesarean section rate in Southeast Brazil: a comparison of two birth cohorts, 1978–1979 and 1994.
Gonzalez-Perez GJ, Vega-Lopez MG, Cabrera-Pivaral C, Munoz A, Valle A. Caesarean sections in Mexico: are there too many?
Hanvoravongchai P, Letiendumrong J, Teerawattanon Y, Tangcharoensathien V. Implications of private practice on the caesarean section rate in Thailand.
Padmadas SS, Kumar S, Nair SB, Kumari KR. Caesarean section delivery in Kerala, India: evidence from a National Family Health Survey.
Mishra US, Ramanathan M. Delivery-related complications and determinants of caesarean section rates in India.
Francome C, Savage W. Caesarean section in Britain and the United States—12% or 24% is either the right rate?
Joffe M, Chapple J, Paterson C, Beard RW. What is the optimal caesarean section rate? An outcome based study on the existing variation.
Petrou S, Glazener C. The economic costs of alternate modes of delivery during the first two months postpartum: results from a Scottish observational study.
Lilford RJ, van Coeverden de Groot HA, Morre P, Bingham P. The relative risks of caesarean section (intrapartum and elective) and vaginal delivery: a detailed analysis to exclude the effects of medical disorders and other acute pre-existing physiological disturbances.
Schuitemaker N, van Roosmalen H, van Dongen P, van Geijn H, Gravenhorst JB. Maternal mortality after caesarean section in the Netherlands.
Guihard P, Blondel B. Trends in risk factors for caesarean sections in France between 1981 and 1995: lessons for reducing the rates in the future.
Skalkidis Y, Petridou E, Papathoma E, Revinthi K, Tong D, Trichopoulos D. Are operative delivery procedures in Greece socially conditioned?
Wilkinson C, McIlwaine G, Boulton-Jones C, Cole S. Is a rising caesarean section rate inevitable?
Kirsop R, Jenkins GJ, Saunders DM, Houghton RS. The influence of maternal age on caesarean section rates.
Zahniser SC, Kendrick JS, Franks AL, Saftlas AF. Trends in obstetric operative procedures, 1980–1987.
Parazzini F, Pirotta N, La Vecchia C, Fedele L. Determinants of caesarean section rates in Italy.
Adashek JA, Peaceman AM, Lopez-Zeno JA, Minogue JP, Socol ML. Factors contributing to the increased caesarean birth rate in older parturient women.
Kirz DS, Dorchester W, Freeman RK. Advanced maternal age: the mature gravida.
Naeye RL. Maternal age, obstetric complications and the outcome of pregnancy.
Tatar M, Gunalp S, Somunoglu S, Demirol A. Women's perceptions of caesarean section: reflections from a Turkish teaching hospital.
Hurst M, Sumney PS. Childbirth and social class: the case of caesarean delivery.
Spaans WA, Sluijs MB, Van Roosmalen J, Bleker O. Risk factors at caesarean section and failure of subsequent trial of labour.
Lynch CM, Kearney R, Turner MJ. Maternal morbidity after elective repeat caesarean section after two or more previous procedures.
Signorelli C, Cattaruzza MS, Osborn JF. Risk factors for caesarean section in Italy: results of a multicentre study.
Bernstein IM, Catalano PM. Examination of factors contributing to risk of caesarean delivery in women with gestational diabetes.
Mould TA, Chong S, Spencer JAD, Gallivan S. Women's involvement with the decision preceding their caesarean section and their degree of involvement.
Barros FC, Vaughan JP, Victora CG, Huttly SR. Epidemic of caesarean sections in Brazil.
Bertollini R, DiLallo D, Spadea T, Perucci C. Caesarean section rates in Italy by hospital payment mode: An analysis based on birth certificates.
Signorelli C, Elliot P, Cattaruzza MS, Osborn J. Trend of caesarean section in Italy: An examination of national data 1980–1985.
Robert CL, Tracy S, Peat B. Rates for obstetric intervention among private and public patients in Australia: population based descriptive study.
Haynes de Regt R, Minkoff HL, Feldman J, Schwartz RH. Relation of private or clinic care on caesarean birth rate.
Placek PJ, Taffel SM, Moien M. C-Section rise: VBACs inch upward.
Kizer KW, Ellis A. C-sections rate related to payment source [letter].
David S, Mamelle N, Riviere O. Estimation of an expected caesarean section rate taking into account case mix of a maternity hospital. Analysis from the AUDIPOG Sentinelle Network (France).
Keeler EB, Brodie M. Economic incentives in the choice between vaginal delivery and caesarean section.
Goyert GL, Bottoms SF, Treadwell MC, Nehra P. The physician factor in caesarean birth rates.
Elferinck-Stinkens PM, Brand R, Van Hemel OJS. Trends in caesarean section rates among high- and medium-risk pregnancies in the Netherlands 1983–1992.
Shelton Brown H. Physician demand for leisure: implications for caesarean section rates.
Burns LR, Geller SE, Wholey DR. The effect of physician factors on the caesarean section decision.
Alran S, Sibony O, Oury JF, Luton D, Blot P. Differences in management and results in term-delivery in nine European referral hospitals: descriptive study.
Mossialos E, Davaki K. Health care developments in Greece: Looking back to see forward? London: LSE Health and Social Care,
Niakas D. Gynaecological services in Greece. In: Matsaganis M, Editor. The economics of gynaecological services in Greece. Athens: Kritiki,
National Statistical Service. Household budget survey 1998/99. Athens: National Statistical Service,
Liaropoulos L, Tragakes E. Public/private financing in the Greek health care system: implications for equity.
Thomas J, Paranjothy S. Royal College of Obstetricians and Gynaecologists Clinical Effectiveness Support Unit. National Sentinel Caesarean Section Audit Report. RCOG Press,
Jibodua OA, Arulkumaranb S. Intrapartum fetal surveillance.
Mastrobattista JM. Vaginal birth after caesarean delivery.

{kind=link}
{kind=link}
Comments