





Abstract
Aims To describe atrial fibrillation (AF) management in member countries of the European Society of Cardiology (ESC) and to verify cardiology practices against guidelines.
Methods and results Among 182 hospitals in 35 countries, 5333 ambulant and hospitalized AF patients were enrolled, in 2003 and 2004. AF was primary or secondary diagnosis, and was confirmed on ECG in the preceding 12 months. Clinical type of AF was reported to be first detected in 978, paroxysmal in 1517, persistent in 1167, and permanent in 1547 patients. Concomitant diseases were present in 90% of all patients, causing risk factors for stroke to be also highly prevalent (86%). As many as 69% of patients were symptomatic at the time of the survey; among asymptomatic patients, 54% were previously experienced symptoms. Oral anticoagulation was prescribed in 67 and 49% of eligible and ineligible patients, respectively. A rhythm control strategy was applied in 67% of currently symptomatic patients and in 44% of patients who never experienced symptoms.
Conclusion This survey provides a unique snapshot of current AF management in ESC member countries. Discordance between guidelines and practice was found regarding several issues on stroke prevention and antiarrhythmic therapy.
See for the editorial comment on this article (doi:10.1093/eurheartj/ehi489)
Introduction
Atrial fibrillation (AF) is associated with an increased mortality.1,2 In addition, AF causes a five-fold rise in stroke risk and frequently coexists with heart failure, both leading to an even further increase in mortality.3–6 Altogether, AF causes a significant economic burden which has grown in the past decades and is expected to grow even further in the upcoming period with the increasing trend in AF prevalence and hospitalizations.7–9 Therefore, an adequate treatment strategy is warranted.
In the past decades, treatment modalities of AF have been studied extensively. Two arrhythmia strategies for the treatment of AF are actually proposed: rate control and rhythm control. Rate control aims at slowing the ventricular rate during AF, whereas rhythm control targets termination of AF and maintenance of sinus rhythm. Recent randomized studies indicated that there is no significant difference in long-term outcome between both treatments.10–15 For stroke prevention, numerous trials showed a beneficial effect of anticoagulation above aspirin or placebo in patients with a high risk for stroke, although the risk for bleeding is increased.16,17 In patients with a low risk for stroke, the bleeding risk of anticoagulation therapy outweighs the benefit of stroke prevention, but aspirin is recommended in these patients.17,18
Owing to the variety of clinical presentations and treatment options for AF, heterogeneity in ‘real-life’ management of AF is expected. The European Society of Cardiology (ESC), the American Heart Association (AHA), and the American College of Cardiology (ACC) recognized the need to review the currently available information on AF, and produced guidelines for AF management (ACC/AHA/ESC guidelines on AF).19 The guidelines have been distributed from 2001, but it remains unclear how well clinicians adhere to them.
Several population-based studies provided information on the incidence, prevalence, and outcome of AF in the general population.1,2,8,20–26 AF management has also been described by national and local surveys and registries in general practices,27–29 and hospitals.30–32 However, there are no prospective data so far regarding the frequency and outcome of the different types of AF in the clinical setting for the total spectrum of ESC member countries. Furthermore, it is unknown whether the actual clinical management and therapy of AF in the member countries conform to the ACC/AHA/ESC guidelines. Therefore, the Euro Heart Survey (EHS) committee of the ESC decided to perform a survey on the management of AF to verify practice against AF guidelines, to compare AF patients in clinical studies with AF patients in clinical practice, and to compare different management strategies in relation to outcome.
The first results of the Euro Heart Survey on Atrial Fibrillation are presented here.
Methods
The Euro Heart Survey on Atrial Fibrillation is a multi-centre prospective observational study among cardiology practices in ESC member countries. For each country, the national coordinator supplied a list of centres that would be suitable to participate in the survey, aiming on a composition of university and non-university centres, and specialized centres that would be representative for local medical practice. Consecutive patients per site of enrolment were requested from the following sites: outpatient clinic, cardiology ward, first (heart) aid, electrical cardioversion department, electrophysiology laboratory, pacemaker and ICD implantation department, and cardiac surgery. All patients were managed according to the usual local institutional practice. Each centre filled in an electronic questionnaire on local infrastructure for AF care.
Patients were enrolled if they were 18 years or older and had AF on ECG or Holter recording during the qualifying admission/consultation, or in the preceding 12 months. Patients with only atrial flutter on their ECGs were excluded. Enrolment started on 19 September 2003 and continued till 16 July 2004. Data collection was finished on 11 August 2004. Patients were enrolled in 182 centres from 35 ESC member countries. Participating countries were divided among three regions (Table 1).
Data collection and validation
In each centre, data were collected using an electronic case report form (CRF: www.euroheartsurvey.org). Data were transferred through Internet to the central database in the European Heart House. Data were either entered online or offline with frequent data transfer.
By using a validation plan, integrated in the data entry software, data were checked for missing or contradictory entries and values out of the normal range. Additional edit checks were performed by the EHS staff at the European Heart House and by the EHS-AF Data Analysis Centre at the University Hospital Maastricht. Patient identification was registered in the participating centres, but was not transferred to the central database.
Data analysis
Data analysis was performed with SPSS statistical software (SPSS, Inc., release 12.01). Continuous variables are reported as mean (standard deviation), and categorical variables as number of observed patients (percentage). Owing to incomplete answers, missing variables and multiple answering options, observed numbers and percentages do not always add up to exactly 100%. Tables are presented according to type of AF. Differences for continuous variables were tested with t-test when comparing two groups and with ANOVA when comparing the four clinical types of AF, and categorical variables were tested with χ2 statistic. Because of the large population sample, comparisons that are reported as different had P<0.001 in all instances.
Results
Patient enrolment
We enrolled 5333 AF patients in 35 countries; 1354 in western, 1530 in central, and 2449 in Mediterranean countries. Details of centre participation and patient enrolment per country and per region are shown in Table 1. Patient enrolment varied significantly among participating countries, with Spain, Italy, and the Netherlands as very high contributors. Nevertheless, the proportion of enrolled patients in relation to all prevalent AF patients in the participating countries appeared to be comparable among the three regions.33 Of 182 participating centres, 141 centres (78%) enrolled more than 10 patients. Almost half of the participating centres (46%) were a university centre, and within centres the vast majority of patients was enrolled at the cardiology ward (56%) or cardiology outpatient clinic (34%). An electrophysiology department was present in 101 centres (56%), and 114 centres (63%) had an outpatient clinic for anticoagulation monitoring.
Patients were categorized into a clinical type of AF, based on the physician's perception of the AF at the time of presentation for the survey (for definitions of clinical AF types, see Appendix A). First detected AF was reported in 978 patients, paroxysmal AF in 1517 patients, persistent AF in 1167 patients, permanent AF in 1541 patients, and unknown AF in 130 patients. The four clinical types of AF were equally often enrolled in the different types of centres, but permanent AF patients were more often enrolled at the outpatient cardiology clinic (Table 2).
Patient characteristics
Patients with permanent AF as their qualifying arrhythmia were older and more often had heart failure, valvular heart disease, or a previous stroke/TIA (Table 3). In addition, artificial pacemakers were more prevalent in these patients. Paroxysmal and first detected AF were more often idiopathic than the other two AF types. Patients with an unknown AF type were comparable to permanent AF patients regarding age [70 (13) years], gender (55% males), previous pharmacological conversion (16%), electrical cardioversion (21%) and catheter ablation (2%). However, prevalence of heart failure (34%) and a previous stroke/TIA (10%) were more comparable with persistent AF, whereas idiopathic AF was even equally often present as in paroxysmal AF (15%).
Hypertension was by far the most prevalent associated medical condition. Coronary artery disease and heart failure were present in one out of three patients. Combinations of associated diseases were found in 60% of patients, of which hypertension with coronary artery disease and hypertension with heart failure (both 24%) were the most frequent ones. Altogether, 90% of AF patients in this survey had at least one associated medical condition. Besides hypertension, other risk factors for coronary artery disease were remarkably frequent, because 18% of all patients was diabetic and 25% severely obese (BMI >30 kg/m2). Of permanent AF patients, 9% previously suffered from a stroke, in contrast to 4% of the other AF patients. Previous pharmacological conversion was most often performed in paroxysmal AF patients and electrical cardioversion most often in persistent AF patients. After first detected AF, permanent AF patients had fewest previous cardioversions. As many as 10–15% of patients participated in a clinical trial. These patients were more frequently categorized as paroxysmal AF (37 vs. 28%), far more often enrolled in a specialized centre (40 vs. 11%), but were of similar age [67 (13) vs. 65 (13) years] compared with patients not participating in a clinical trial.
Patient characteristics on admission or at consultation
Logically the most frequent reason for the qualifying admission or consultation was AF, but it was often accompanied by other reasons, especially in patients with permanent AF (Table 4). The majority of patients reported current AF symptoms (69%) or had suffered from AF symptoms in the past (54% of currently asymptomatic patients), with relatively the lowest symptom burden in permanent AF. Paroxysmal AF patients were currently least frequent in AF. Patients with a first detected episode had a higher ventricular rate on admission. In accordance with the highest prevalence of heart failure, permanent AF patients more often had NYHA functional class III or IV and a broader QRS complex. An increased left atrial diameter was seen in persistent AF and is more pronounced in permanent AF. Duration of the current AF episode was reported to be longer than 7 days in 61 (4%) patients classified as paroxysmal AF, and 3% of patients classified as permanent AF were not currently in AF.
Diagnostics and interventions
The vast majority of patients underwent a transthoracic echocardiogram and a chest X-ray (Table 5). Either a transthoracic or transesophageal echocardiogram was done in 86% of patients. The patients who did not undergo echocardiography were older [69 (14) vs. 66 (13) years], presented more frequently as first detected AF (28 vs. 17%), were more often enrolled in a non-university centre (49 vs. 37%), or enrolled in Western European countries (35 vs. 24%). The other diagnostic procedures were most often used in paroxysmal AF patients, except for transesophageal echocardiography, which was relatively frequently used in persistent AF patients. Of all current transesophageal echocardiograms, 71% was used in connection with a current or planned electrical cardioversion. Thyroid hormone levels were reported in only half of the patients. Patients without assessment of thyroid function were of similar age [66 (13) vs. 67 (12) years], more often male (61 vs. 54%), presented more frequently with first detected (21 vs. 16%) and permanent AF (34 vs. 25%), and were more often enrolled in a university centre (50 vs. 44%), a specialized centre (17 vs. 10%), or in a Central European country (35 vs. 22%), compared with patients with thyroid function assessment. In the subset of patients currently on amiodarone thyroid hormone levels, measurement was performed at least once or planned in 60% of patients, which is just slightly more often than the application in patients not currently on amiodarone (56%).
Pharmacological conversions were mainly applied in first detected and paroxysmal AF, whereas electrical cardioversions were preferred in persistent AF. A minority of patients that had been classified as having permanent AF underwent pharmacological or electrical cardioversion. Catheter ablation was infrequently applied, predominantly in paroxysmal and persistent AF. Catheter ablation was related to pacemaker implantation in five paroxysmal, three persistent, and seven permanent AF patients.
Drug therapy
Drug therapy at discharge or end of visit was known for 5157 patients. Oral anticoagulation (OAC) was prescribed in the majority of AF patients, especially in persistent and permanent AF (Table 6). Few patients did not receive any antithrombotic treatment.
Of all patients, 40% received antiarrhythmic medication, 65% rate control medication, and 12% neither of these. Type IA drugs (Vaughan Williams classification34) were hardly used. Type IC antiarrhythmic drugs were mainly prescribed in patients with paroxysmal or persistent AF. Of note, 3% of paroxysmal and persistent AF patients were on a type IC antiarrhythmic drug despite having coronary artery disease or heart failure. Beta-blockers were used for an antiarrhythmic indication in approximately 30% of patients with almost equal distribution across all subgroups. Type IV antiarrhythmic drugs and digitalis were most frequently prescribed in permanent AF. Type III antiarrhythmic drugs were given in 15% of permanent AF patients, of which 13% amiodarone and 2% sotalol.
Rate and rhythm control
In the majority of patients with current AF symptoms, rhythm control was applied (67%), but still 27% had exclusively rate control (Figure 1). Most symptomatic patients suffered from palpitations and/or syncope (75%). Of note, in 44% of patients who never had experienced symptoms, a rhythm control strategy was applied. In previously symptomatic patients (symptoms suppressed or spontaneously disappeared), a rhythm control strategy was equally often applied (46%) as in the group that had never experienced symptoms.
Of all patients with paroxysmal or persistent AF, 77% was under rhythm control, 18% on exclusive rate control, and 5% did not receive any treatment or information was incomplete. Of all patients with first detected AF, 72% underwent rhythm control. Of these patients, 79% (n=553) were symptomatic with their AF.
Among all rhythm control patients, 54% was also on typical rate control drugs (digitalis, beta-blocker, verapamil, or diltiazem) and 52% was on amiodarone or sotalol, which are known to also have rate control properties. Taken together, 84% of patients had some type of rate control besides the rhythm control treatment.
Average resting ventricular rate was comparable in patients on solely typical rate control drugs [88 (27) b.p.m.] and patients on solely sotalol or amiodarone [89 (33) b.p.m.], but was higher in patients who were on a combination of amiodarone or sotalol with one or more of the typical rate control drugs [100 (32) b.p.m.].
Stroke prevention
According to the ACC/AHA/ESC guidelines, 86% of this survey population had at least one risk factor for stroke for which they should receive OAC (Table 7), and an additional 4% of patients without such a stroke risk factor should receive OAC to reduce risk for stroke during a procedure for restoring sinus rhythm. Only a minority of all patients was known with a major bleeding (2%) or malignancy (5%) as possible contraindications. Figure 2 shows that 67% of eligible and 49% of ineligible patients received OAC. The exclusion of patients known with a major bleeding or malignancy did not alter the prescription rates. Only 7% of eligible patients did not receive any antithrombotic treatment.
Discussion
The Euro Heart Survey on Atrial Fibrillation provides a unique snapshot of the characteristics and management of AF patients in cardiology departments among ESC member countries. Management guideline application may be suboptimal regarding several issues. Data derived from this survey can be used as a baseline for outcome analysis at follow-up, and as a benchmark for future European surveys on AF management.
This survey provides unique data on AF management from a wide array of medical centres in ESC member countries. Nevertheless, enrolment was not equally divided among participating countries, and in addition an overrepresentation of highly specialized and AF interested centres is suspected. Therefore, one has to keep in mind that these data are representative for the participating centres and may not be representative for all centres in ESC member countries.
Patient characteristics in this survey stress the importance of recognizing AF as a disease that is generally associated with many other cardiac and non-cardiac problems. In accordance with other surveys and registries, hypertension is established as the primary associated cardiovascular disease in AF patients.1,27,28 In addition, the majority of patients suffered from a combination of associated medical conditions. As a consequence, cardiologists should realize that the vast majority of AF patients they encounter in clinical practice have at least one stroke risk factor. The latter was also observed in previous studies.35–41 To improve prognosis in AF patients, the high prevalence of stroke risk factors in this survey mandates that one should first focus on antithrombotic treatment and management of associated conditions before embarking on rhythm control treatment.
AF has been reported in clinical studies to be idiopathic or lone in 15% of persistent AF and in even 60% of paroxysmal AF patients.42 In contrast, in population-based studies the prevalence of idiopathic or lone AF was much lower, between 7.643 and 11%,44 and even as low as 2.7% in a population younger than 60 years.45 In this survey, the overall prevalence of idiopathic AF amounted to 10%, with an expected highest value in paroxysmal AF (15%). The fact that prevalence is lower in this survey compared with previous clinical studies probably relates to the higher average age in clinical practice compared with clinical trials. In addition, over the years the awareness of associated disease has grown, especially hypertension and left ventricular dysfunction being recognized as important associated conditions.1,6 Especially echocardiography contributed in this respect.
Classification of the type of AF into first detected, paroxysmal, persistent, and permanent (3P classification)19,46 is of importance for choosing appropriate therapy. Overall, misclassifications were not very frequent. Patients registered as having first detected AF could have had a previous arrhythmia intervention if the first episode was diagnosed before the current admission or consultation, and no recurrence was seen since. In this survey, it appeared that only 2% of first detected patients had more than one previous arrhythmia intervention, suggesting paroxysmal or persistent AF rather than first detected. Similarly, among patients classified as paroxysmal AF, only 4% should have been classified as persistent AF based on a current AF duration longer than 7 days. In contrast, 11% of patients classified by the investigators as permanent AF should be considered as having persistent AF, because these patients currently underwent a cardioversion, received a type IA or IC antiarrhythmic drug, or were reported not be in AF on ECG. If the use of type III antiarrhythmic drugs also is considered in the permanent group, then an additional 11% could have been classified as persistent AF. Therefore, especially the classification permanent AF might have been regularly confused with persistent AF. The latter is supported by the observation that the group with unknown AF type mostly showed a mix of persistent and permanent AF patient characteristics.
Misclassification may relate to unfamiliarity with definitions of the various AF classes, or that the 3P classification is not used in a uniform manner due to interpretation differences. Bearing in mind the relatively short time that these definitions are being used now, it may very well be that physicians are not yet used to apply them in clinical practice. Nevertheless, we saw significant and clinically important differences concerning treatments among the different types of AF, indicating that management was directed by type of AF. Considering the above, we feel that the 3P classification is useful and feasible, and satisfies a clinical need in the diagnosis of AF patients. It also helps to identify patients for clinical studies.
A relatively high proportion of patients had first detected AF which could not be explained by site of inclusion, as the proportion was similar for outpatients vs. inpatients as well as for acute vs. non-acute patients (Table 2). In addition, there was no difference in proportion first detected AF between patients with a primary or secondary AF diagnosis. Apparently, relatively many patients seen by ESC cardiologists have only one overt episode of AF which presents right away as persistent or permanent in 75% of cases (Table 3). The profile of these patients is not dissimilar from the persistent and permanent AF groups, indicating that underlying heart diseases is more important than the ‘AF begets AF’ principle.47Therefore, primary prevention, especially treatment of high blood pressure rather than secondary suppression of the arrhythmia, seems indicated to ameliorate the epidemic of AF.
Minimal evaluation as required by the guidelines is well implemented, as the vast majority of patients underwent an echocardiogram and a chest X-ray.19 Transesophageal echocardiography does not seem to play a large role, as it was performed mainly in relation to electrical cardioversion. First detected AF patients and elderly had a lower chance of undergoing echocardiography. This is remarkable and should receive the attention of cardiologists, because these subgroups are at highest risk of stroke or other complications such as heart failure. Improving routines of early echocardiography seem important to prevent early AF-related morbidity.
Thyroid hormone levels were never measured in half of these patients, although this is highly recommended to exclude thyroid dysfunction as the underlying cause of AF. Surprisingly, patients receiving amiodarone did not have a higher chance of undergoing thyroid function tests, while thyroid function monitoring is especially warranted in these patients.
The high prevalence of previous and current pharmacological conversions in paroxysmal AF reflects appropriate clinical practice, as pharmacological conversion is preferred above electrical cardioversion in these patients. The same holds for the most frequent use of electrical cardioversions in persistent AF, because this is more effective than pharmacological conversion. Prior pharmacological conversions were performed in many persistent and permanent AF patients, suggesting that they had paroxysmal AF before progressing to more persistent forms of AF.
In fair agreement with the guidelines, 67% of currently symptomatic patients received a rhythm control strategy. Note that the symptomatic patients formed the largest group in the survey (69%) and most rhythm-controlled patients suffered from arrhythmia symptoms rather than complaints due to associated cardiac disease. This indicates that available rhythm control strategies are inadequate and that there is at present an unmet need for safe and efficacious antiarrhythmic drugs for control of AF.
Within the group of patients who never experienced any symptoms, rhythm control was applied in 44% of cases despite the absence of AF symptoms. In these patients, rate control to prevent late onset heart failure is probably sufficient, and may also help to avoid possible adverse effects of rhythm control.10,11 The ACC/AHA/ESC guidelines state that rhythm control should be applied only in symptomatic patients.19 This advice is supported by the findings from the large rate vs. rhythm trials which showed that compared with the existing rhythm control strategies, rate control seems safer and as effective as rhythm control.10,11
To our knowledge, this survey found one of the highest OAC prescription rates in the clinical setting until now.35,40,48–53 Besides increased knowledge about antithrombotic treatment for stroke prevention, this relatively high prevalence may also relate to the fact that the majority of patients came from university and specialized centres. In addition, 63% of participating centres had an anticoagulation clinic to monitor INR values. Nevertheless, there is still room for improvement, because 33% of patients with an indication for anticoagulation is not treated as such. In contrast, among the eligible patients who did not receive OAC, a significant number may have had contraindications to OAC other than major bleeding or malignancy, which prevents reaching 100% in eligible patients. We believe that this gap between guidelines and practice is not completely attributable to the presence of contraindications, because previous studies found a prevalence of contraindications in around 15% of clinical AF patients.32,41,54,55
A remarkable finding is that among patients without an indication for OAC, half of these patients received OAC. This may relate to patient preference due to, e.g. fear of disabling stroke which was also discussed as such by the latest ACCP guidelines on management of stroke in younger AF patients.56 Altogether, it seems that in daily practice selection of stroke prevention therapy is not strongly determined by the clinical indications as recommended by the guidelines.
Surprisingly as many as 10–15% of patients had participated in any one or more clinical trials, mainly in specialized centres. This might indicate high activity regarding AF research in Europe, but it is also likely to reflect the participation of specialized centres with a specific interest in research on AF in this survey.
Limitations
We intended to collect data from a broad sample of cardiology centres from member countries of the ESC that were willing to participate, to present a broad view on daily practice. However, relatively many centres were university and specialized centres, and also the results point towards an overrepresentation of centres that were highly specialized and interested in AF. In addition, patient enrolment was not equally divided among participating countries. Therefore, these results are representative for the participating centres in the survey, but cannot automatically be extrapolated to all centres in ESC member countries. Data were contributed on a voluntary basis, which may cause incompleteness or inconsistency of data. Data were however quite complete. Among key variables, a maximum of 2% of missing data points was found. In addition, we checked for inconsistencies by applying logical checks within the database. Inconsistencies were checked with the investigators by issuing queries.
Conclusions
Most patients visiting cardiovascular specialist in ESC member countries have one or multiple associated medical conditions and specific stroke risk factors. In addition, most patients are symptomatic with their arrhythmia despite treatment. This survey shows that application of the ESC AF guideline may be suboptimal regarding several issues including inappropriate application of rhythm control in asymptomatic patients and the contraindicated or needless use of antiarrhythmic drugs in both rate and rhythm control patients. The survey also illustrates the unmet need for new safe and effective antiarrhythmic drugs to suppress symptoms in paroxysmal and persistent AF. Although the use of OAC was the highest ever reported, stroke risk assessment according to the guidelines just marginally seems to drive the decision to anticoagulate or not. New antithrombotic drugs or strategies including education of the public might help to improve matters. The long-term follow-up of the patients in this survey may indicate whether guideline adherence is associated with better outcomes compared with guideline deviant management.
Appendix A. Definitions
Numerous definitions were used in this survey, with the aim of standardizing data entry. Definitions were given in a short text file attached to the data entry point in the electronic case report form so that this information was readily available. The most important definitions for this manuscript are reported here.
First detected episode of AF: The first detected episode is AF diagnosed for the first time by a physician, in which it is important to distinguish whether it is symptomatic or self-limiting, recognizing that there may be uncertainty about the duration of the episode and about previous undetected episodes.
Paroxysmal AF: Recurrent AF that terminates spontaneously and lasts ≤7 days (mostly <24 h).
Persistent AF: Recurrent AF or sustained AF lasting >7 days. Termination of AF by pharmacological therapy or electrical cardioversion does not change the designation. In other words, cardioversion does not necessarily differentiate between paroxysmal and persistent AF, as pharmacological and electrical cardioversions are used in both conditions.
Permanent AF: AF has been present for a long time, cardioversion has not been indicated, or one or several attempts have failed to restore reliable sinus rhythm.
Hypertension: Systolic blood pressure above 160 mmHg, diastolic blood pressure above 90 mmHg, or receiving blood-pressure-lowering drugs.
Idiopathic AF: No previously or currently diagnosed hypertension, coronary artery disease, heart failure, valvular heart disease, tachycardiomyopathy, sick sinus syndrome, chronic obstructive pulmonary disease, or thyroid disease.
Symptomatic AF: The presence of one or more of the following symptoms in relation to AF: palpitations, dyspnoea, chest pain, syncope, dizziness, fatigue, or other non-specified symptoms.
Rhythm control strategy: Currently applying or planning a pharmacological conversion or electrical cardioversion, or prescribing a class IA, IC, or III antiarrhythmic drug (Vaughan Williams classification).34 Of note, rhythm control patients may be on typical rate control drugs, because the latter drugs are frequently unavoidable as background therapy in rhythm control patients.
Rate control strategy: Prescribing digitalis, class II, or class IV antiarrhythmic drugs, and not currently applying or planning any of the ‘rhythm control’ procedures and not prescribing a class IA, IC, or III antiarrhythmic drug.
Eligible for anticoagulation: According to the ACC/AHA/ESC guidelines, patients are eligible for anticoagulation when they undergo pharmacological or electrical cardioversion for AF lasting >48 h, or when one of the following characteristics are present: risk factors for stroke are here: age≥60 years with diabetes or coronary artery disease, age≥75 years, heart failure, left ventricular ejection fraction≤0.35, hypertension, mitral valve stenosis, valve surgery, or prior thromboembolism. In addition, patients undergoing catheter ablation are also considered to be eligible for anticoagulation.
Not eligible for anticoagulation: When none of the above-mentioned indications for anticoagulation are present.
Appendix B. Organization of the survey
Atrial Fibrillation Expert Committee and Consultants: Harry Crijns (Survey Chairman), The Netherlands; Robby Nieuwlaat (research fellow), The Netherlands; Dieter Andresen, Germany; A. John Camm, UK; Alessandro Capucci, Italy; Wynn Davies, UK; Samuel Lévy, France; Bertil Olsson, Sweden; Etienne Aliot, France; Günter Breithardt, Germany; Stuart Cobbe, UK; Jean-Yves Le Heuzey, France; Massimo Santini, Italy; Panos Vardas, Greece.
Euro Heart Survey Team (European Heart House, France): Malika Manini, Operations Manager; Claire Bramley, Data Monitor; Valérie Laforest, Data Monitor; Charles Taylor, Database Administrator; Susan Del Gaiso, Administrator.
Main Investigator Centre (Maastricht, The Netherlands): Harry Crijns (Survey Chairman), Robby Nieuwlaat (Research Coordinator).
National Coordinators: Austria, Kurt Huber; Belgium, Guy De Backer; Bulgaria, Vera Sirakova; Czech Republic, Roman Cerbak; Denmark, Per Thayssen; Finland, Seppo Lehto; France, Jean-Jacques Blanc, François Delahaye; Georgia, Bondo Kobulia; Germany, Uwe Zeymer; Greece, Dennis Cokkinos; Hungary, Kristof Karlocai; Ireland, Ian Graham, Emer Shelley; Israel, Shlomo Behar; Italy, Aldo Maggioni; Lithuania, Virginija Grabauskiene; The Netherlands, Jaap Deckers; Norway, Inger Asmussen; Poland, Janina Stepinska; Portugal, Lino Gonçalves; Russia, Vyacheslav Mareev; Serbia and Montenegro, Zorana Vasiljevic; Slovakia, Igor Riecansky; Slovenia, Miran F. Kenda; Spain, Angeles Alonso, José Luis Lopez-Sendon; Sweden, Annika Rosengren; Switzerland, Peter Buser; Turkey, Tugrul Okay; Ukraine, Oleg Sychov; UK, Kevin Fox, Peter Schofield.
There was no national coordinator in the participating countries which are not mentioned in the above list.
Euro Heart Survey Board Committee (2000–2004): Maarten Simoons (Chairman), The Netherlands, David Wood (past-chairman), United Kingdom; Angeles Alonso, Spain; Alex Battler, Israel; Shlomo Behar, Israel; Eric Boersma, The Netherlands; Harry Crijns, The Netherlands; Kim Fox, UK; Michel Komajda, France; Malika Manini, France; Keith McGregor, France; Barbara Mulder, The Netherlands; Sylvia Priori, Italy; Lars Rydén, Sweden; Luigi Tavazzi, Italy; Alec Vahanian, France; Panos Vardas, Greece; William Wijns, Belgium; Uwe Zeymer, Germany.
Industry sponsors: main sponsor: AstraZeneca; major sponsor: Sanofi-Aventis; sponsor: Eucomed.
List of Institutions: Austrian Heart Foundation, Austrian Society of Cardiology, French Federation of Cardiology, Hellenic Cardiological Society, Netherlands Heart Foundation, Portuguese Society of Cardiology, Spanish Cardiac Society, Swedish Heart and Lung Foundation and individual centres.
Participating Centres, Investigators, and Data Collection Officers: Armenia: S.V. Grigoryan, I. Apetyan, S. Aroyan, L. Azarapetyan; Austria: Anahit Anvari, Michael Gottsauner-Wolf, Stefan Pfaffenberger, Kurt Huber, Kadriye Aydinkoc, Karim Kalla, Martina Penka, Heinz Drexel, Peter Langer; Belgium: Luc A. Pierard, Victor Legrand, Dominique Blommaert, E. Schroeder, Isabelle Mancini, William Wijns, P. Geelen, P. Brugada, Marc De Zutter, Christiaan Vrints, Marc Vercammen, Marielle Morissens; Bulgaria: Borislav Boyanov Borisov, Valentin Asenov Petrov, Maria Marinova Alexandrova, Assen Rachev Goudev, Vera Sirakova, Yavor Peychev, Vassil Stoyanovsky, Evgeni Stoynev; Croatia: Stjepan Kranjcevic; Cyprus: Joseph Moutiris, Marios Ioannides; Switzerland: Dominique Evequoz; Czech Republic: Jaroslava Spacilova, Roman Cerbak, Miroslav Novak, Martin Eisenberger, Jolana Mullerova, Josef Kautzner, Lucie Riedlbauchova, Jan Petrù, Milos Taborsky; Denmark: Per Thayssen, Helle Cappelen; Egypt: Yasser A. Sharaf, B.S.S. Ibrahim, Khalid Tammam, Aly Saad, Helmy Elghawaby, Hamed Zaky Sherif, Heba Farouk; Germany: D. Andresen, Arlett Mielke, Gunter Breithardt, Markus Engelen, Paulus Kirchhof, Pia Zimmermann; Spain: F. Fernandez Aviles, Jeronimo Rubio, F. Malpartida, M. Corona, Luis Tercedor Sanchez, Jose Miguel Lozano Herrera, Aurelio Quesada, Antonio J. Munoz Garcia, Carlos Sanchez Gonzalez, M. Soledad Alcasena Juango, Jesus Berjon-Reyero, Josep M. Alegret, J.M. Cruz Fernandez, Cesar Carrascosa Rosillo, Antonio Fernandez Romero, Miguel González Lara, José L. Lopez Sendon, José Juan Gomez de Diego, Luis Sosa Martin, Maria Irurita, Norbero Herrera Guttierez, Juan Ramon Siles Rubio, Isabel Antorrena, Alicia Bautista Paves, Antonio Salvador, Maria Dolores Orriach, A. Alonso Garcia, Francisco Epelde, Vicente Bertomeu Martinez, Antonio Berruezo Sanchez, Carlos Pinero Galvez, Rafael Fernandez Rivero, Antonio Hernandez Madrid, Gonzalo Baron-Esquivias, Rafael Peinado, José Antonio Gomez Guindal, Tomas Ripoll Vera, Emilio Luengo Fernandez, Ricardo Gayan, Javier Garcia, Andres Bodegas, Jesus Toril Lopez, Julio Martinez Florez, Cristobal Lozano Cabezas, Eduardo Vazquez Ruiz de Castroviejo, Juan Munoz Bellido, Maria Eugenia Ruiz; Finland: Seppo Lehto, Kirsti Savolainen, Markku Nieminen, Lauri Toivonen, Mikko Syvanne, Mervi Pietila; France: Daniel Galley, Christine Beltra, Samuel Lévy, Alain Gay, J.C. Daubert, Guillaume Lecocq, Christine Poulain; United Kingdom: J.G.F.C. Cleland, Rhidian Shelton, G.Y.H. Lip, A. Choudhury; Georgia: Gulnara Abuladze, Irina Jashi; Greece: Dennis V. Cokkinos, Anastasia Tsiavou, G. Giamouzis, N. Dagres, A. Kostopoulou, Domproglou, Tsoutsanis, Ch. Stefanadis, George Latsios, Ioannis Vogiatzis, Alexandros Gotsis, Paraskevi Bozia, Maria Karakiriou, Spyridon Koulouris, John Parissis, George Kostakis, Nikos Kouris, Dimitra Kontogianni, Koutroubas Athanasios, Alexandros Douras, Themistoklis Tsanakis, Panos Vardas, Mary Marketou, Nikolaos Patsourakos; Hungary: Laszlo Czopf, Robert Halmosi, Istvan Préda, Eva Csoti, Andrea Badics; Israel: Boris Strasberg, Nahum A. Freedberg, Amos Katz, Eli Zalzstein, Aviva Grosbard, E. Goldhammer, Menachem Nahir, Menashe Epstein, Ida Vider, David Luria, Lori Mandelzweig; Italy: Bruno Aloisi, Alfio Cavallaro, Emanuele Antonielli, Baldassarre Doronzo, Diego Pancaldo, Carlo Mazzola, Liliana Buontempi, Valeria Calvi, Giuseppe Giuffrida, Antonino Figlia, Francesco Ippolito, Gian-Paolo Gelmini, N. Gaibazzi, Virgilio Ziacchi, Francesco De Tommasi, Federico Lombardi, Cesare Fiorentini, Paolo Terranova, Pietro Maiolino, Muhamad Albunni, Plinio Pinna-Pintor, Stefano Fumagalli, Guilio Masotti, Lorenzo Boncinelli, Domenico Rossi, Giovanni Maria Santoro, Massimo Fioranelli, Franco Naccarella, Stefano Sdringola Maranga, Giovannina Lepera, Barbara Bresciani, Elena Seragnoli, Mara Cantelli Forti, Valentina Cortina, Giacinto Baciarello, Paolo Cicconetti, Antonio Lax, Federica Vitali, Diran Igidbashian, Luisa Scarpino, Sergio Terrazzino, Luigi Tavazzi, Francesco Cantu, Francesco Pentimalli, Salvatore Novo, Giuseppe Coppola, Gianluca Zingarini, Giuseppe Ambrozio, Paolo Moruzzi, Sergio Callegari, Gabriele Saccomanno, Paolo Russo, Emanuele Carbonieri, Anna Paino, Marco Zanetta, Enzo Barducci, Roberto Cemin, Werner Rauhe, Walter Pitscheider, Marina Meloni, Sergio Mariano Marchi, Marco Di Gennaro, Sergio Calcagno, Paola Squaratti, Francesco Quartili, Patrizia Bertocchi, Mario De Martini, Giuseppe Mantovani, Roman Komorovsky, Alessandro Desideri, Leopoldo Celegon, Luigi Tarantini, Giuseppe Catania, Donata Lucci, Francesca Bianchini; Lithuania: Aras Puodziukynas, Ausra Kavoliuniene, Vilija Barauskiene, Audrius Aidietis, Jurate Barysiene, Vitas Vysniauskas, Irena Zukauskiene, Nijole Kazakeviciene; Macedonia: Ljubica Georgievska-Ismail, Lidija Poposka; Moldova: Eleonora Vataman, Aurel A. Grosu; The Netherlands: Wilma Scholte op Reimer, Esther de Swart, Mattie Lenzen, Jaap Deckers, Chris Jansen, Ritzo Brons, Henriette Tebbe, D.C.A van Hoogenhuyze, M.J. Veerhoek, Maria Kamps, D. Haan, Nitolanda van Rijn, Annette Bootsma, Leo Baur, Adrie van den Dool, Harry Crijns, Robby Nieuwlaat, Heidi Fransen, Luc Eurlings, Joan Meeder, M.J. De Boer, Jobst Winter, Herman Broers, Chris Werter, M. Bijl, Saskia Versluis; Poland: Malgorzata Milkowska, Beata Wozakowska-Kaplon, Marianna Janion, Lidia Lepska, Grazyna Swiatecka, Piotr Kokowicz, Jacek Cybulski, Aleksandr Gorecki, Marcin Szulc, Jerzy Rekosz, Rafal Manczak, Anna-Maria Wnuk-Wojnar, M. Trusz-Gluza, Anna Rybicka-Musialik, Jaroslaw Myszor, Michal Szpajer, Krzysztof Cymerman, Jerzy Sadowski, Maria Sniezek-Maciejewska, Mariola Ciesla-Dul, Izabela Gorkiewicz-Kot, Tomasz Grodzicki, Krzysztof Rewiuk, Leszek Kubik, Jacek Lewit; Portugal: Joao Manuel Frazao Rodrigues de Sousa, Rafael Ferreira, Antonio Freitas, Joao Carlos Araujo Morais, Rui Pires, M.J. Veloso Gomes, Paula Gago, Rui Alexandre C. Candeias, Luis Nunes, Joao Vitor Miranda Sa, Miguel Ventura, Mario de Oliveira, Luis Brandao Alves; Romania: Ioan Bostaca, Codin T. Olariu, G.A. Dan, Anca Dan, Cristian Podoleanu, Attila Frigy, George I.M. Georgescu, Catalina Arsenescu, Cristian Statescu, Radu Sascau, Dan L. Dimitrascu, Raluca Rancea; Russian Federation: Yuri V. Shubik, Dmitry Duplyakov, Marina Shalak, Vyacheslav Mareev, Marine Danielyan, Albert Galyavich, Venera Zakirova; Slovakia: Robert Hatala, Gabriela Kaliska, Jan Kmec; Slovenia: Igor Zupan, Jerneja Tasiè, Damijan Vokac; Sweden: Nils Edvardsson, Dritan Poci; Tunisia: Habib Gamra, Hichem Denguir; Turkey: Tugrul Okay, Ahmet Sepetoglu, Alev Arat-Ozkan; Ukraine: Mariya Orynchak, Elena Paliy, I. Vakalyuk, Oleg Sychov, David Malidze, Rostyslav Prog, Myckola Ivanovich Yabluchansky, Nataliya Volodimirovna Makienko; Serbia and Montenegro: Tatjana Potpara, Sofija Knezevic, Miomir Randjelovic.
Conflict of interest: none declared.
Figure 1 Heart rhythm management strategy in patients who were symptomatic at the time of the survey, in patients who were not symptomatic at the time of the survey but who had been symptomatic in the past, and in patients who had never experienced any symptoms. Definitions for rhythm control, rate control, and symptomatic AF are given in Appendix A. No treatment: none of the procedures and drugs mentioned under ‘rhythm control’ and ‘rate control’ were applied; uncertain: not enough information available to determine the treatment strategy.
Figure 2 Antithrombotic therapy at discharge or end of visit, in patients considered to be eligible or ineligible for OAC according to the ACC/AHA/ESC guidelines for AF management. Descriptions of stroke risk factors are given in Appendix A. Antiplatelet: aspirin, clopidogrel, ticlopidin or dipyridamole; other antithrombotic: heparin or non-specified antithrombotic agent. *In the absence of OAC. #In the absence of OAC and antiplatelet drugs.
Geographical distribution of centre participation and patient enrolment
| Participation | Patients | Site of enrolment | Clinical type of AF | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Centres | Centres enrolling >10 patients | University centre | Non-university centre | Specialized centre | Outpatient cardiology clinic | Cardiology ward | First (heart) aid | Other site | First detected AF | Paroxysmal AF | Persistent AF | Permanent AF | ||
| Western | 34 | 30 (88) | 14 (41) | 19 (56) | 1 (3) | 1354 | 684 (51) | 502 (37) | 85 (6) | 83 (6) | 184 (14) | 493 (36) | 233 (17) | 380 (28) |
| Austria | 3 | 3 | 1 | 1 | 1 | 119 | 76 | 37 | 5 | 1 | 25 | 32 | 29 | 19 |
| Belgium | 5 | 3 | 4 | 1 | 0 | 61 | 16 | 29 | 1 | 15 | 21 | 14 | 17 | 9 |
| Denmark | 1 | 1 | 1 | 0 | 0 | 26 | 0 | 26 | 0 | 0 | 3 | 13 | 6 | 3 |
| Finland | 2 | 2 | 2 | 0 | 0 | 68 | 51 | 17 | 0 | 0 | 3 | 37 | 14 | 13 |
| France | 4 | 2 | 1 | 3 | 0 | 51 | 10 | 40 | 0 | 1 | 13 | 15 | 6 | 17 |
| Germany | 2 | 2 | 1 | 1 | 0 | 192 | 34 | 128 | 0 | 30 | 15 | 88 | 23 | 63 |
| Sweden | 1 | 1 | 1 | 0 | 0 | 40 | 32 | 8 | 0 | 0 | 2 | 25 | 5 | 8 |
| Switzerland | 1 | 1 | 0 | 1 | 0 | 52 | 4 | 18 | 14 | 16 | 4 | 3 | 5 | 33 |
| The Netherlands | 13 | 13 | 2 | 11 | 0 | 714 | 430 | 199 | 65 | 16 | 96 | 256 | 115 | 209 |
| United Kingdom | 2 | 2 | 1 | 1 | 0 | 31 | 31 | 0 | 0 | 0 | 2 | 10 | 13 | 6 |
| Central | 53 | 42 (79) | 30 (57) | 9 (17) | 14 (26) | 1530 | 250 (16) | 1149 (75) | 36 (2) | 95 (6) | 265 (17) | 485 (32) | 357 (23) | 402 (26) |
| Armenia | 1 | 1 | 0 | 0 | 1 | 51 | 0 | 50 | 1 | 0 | 1 | 42 | 6 | 2 |
| Bulgaria | 5 | 4 | 2 | 2 | 1 | 107 | 1 | 66 | 1 | 39 | 25 | 22 | 19 | 40 |
| Croatia | 1 | 0 | 1 | 0 | 0 | 8 | 7 | 1 | 0 | 0 | 1 | 1 | 2 | 3 |
| Czech Republic | 4 | 4 | 2 | 1 | 1 | 176 | 39 | 119 | 12 | 6 | 24 | 45 | 39 | 65 |
| Georgia | 1 | 1 | 0 | 0 | 1 | 30 | 12 | 18 | 0 | 0 | 14 | 7 | 2 | 2 |
| Hungary | 3 | 2 | 1 | 1 | 1 | 82 | 0 | 80 | 0 | 2 | 29 | 22 | 10 | 21 |
| Lithuania | 4 | 4 | 2 | 2 | 0 | 118 | 23 | 91 | 1 | 3 | 13 | 43 | 46 | 15 |
| Macedonia | 1 | 0 | 1 | 0 | 0 | 2 | 0 | 2 | 0 | 0 | 1 | 0 | 1 | 0 |
| Moldova | 1 | 1 | 0 | 0 | 1 | 36 | 5 | 31 | 0 | 0 | 8 | 22 | 6 | 0 |
| Poland | 11 | 8 | 6 | 1 | 4 | 267 | 41 | 182 | 22 | 22 | 39 | 106 | 56 | 63 |
| Romania | 6 | 4 | 5 | 0 | 1 | 168 | 8 | 147 | 0 | 13 | 31 | 34 | 45 | 55 |
| Russia | 4 | 4 | 2 | 1 | 1 | 115 | 45 | 70 | 0 | 0 | 20 | 46 | 5 | 41 |
| Serbia & Montenegro | 2 | 1 | 1 | 1 | 0 | 30 | 1 | 29 | 0 | 0 | 14 | 4 | 10 | 1 |
| Slovakia | 4 | 4 | 3 | 0 | 1 | 121 | 20 | 95 | 0 | 0 | 18 | 35 | 45 | 23 |
| Slovenia | 1 | 1 | 1 | 0 | 0 | 32 | 29 | 3 | 0 | 0 | 3 | 22 | 3 | 4 |
| Ukraine | 4 | 3 | 3 | 0 | 1 | 187 | 19 | 165 | 0 | 3 | 24 | 34 | 62 | 67 |
| Mediterranean | 94 | 69 (73) | 39 (41) | 44 (47) | 11 (12) | 2449 | 859 (35) | 1336 (55) | 78 (3) | 176 (7) | 529 (22) | 539 (22) | 577 (24) | 759 (31) |
| Cyprus | 2 | 1 | 0 | 2 | 0 | 20 | 8 | 12 | 0 | 0 | 4 | 15 | 1 | 0 |
| Egypt | 3 | 3 | 3 | 0 | 0 | 133 | 28 | 91 | 2 | 12 | 22 | 30 | 14 | 60 |
| Greece | 10 | 10 | 1 | 7 | 2 | 323 | 51 | 261 | 7 | 4 | 79 | 105 | 57 | 70 |
| Israel | 7 | 1 | 6 | 1 | 0 | 59 | 22 | 32 | 0 | 5 | 25 | 12 | 16 | 5 |
| Italy | 32 | 24 | 6 | 23 | 3 | 843 | 334 | 432 | 36 | 41 | 145 | 184 | 290 | 206 |
| Portugal | 9 | 7 | 2 | 5 | 2 | 154 | 23 | 101 | 5 | 25 | 46 | 29 | 25 | 53 |
| Spain | 29 | 21 | 20 | 6 | 3 | 848 | 384 | 349 | 27 | 88 | 165 | 150 | 166 | 361 |
| Tunisia | 1 | 1 | 1 | 0 | 0 | 50 | 1 | 49 | 0 | 0 | 33 | 9 | 7 | 1 |
| Turkey | 1 | 1 | 0 | 0 | 1 | 19 | 8 | 9 | 1 | 1 | 10 | 5 | 1 | 3 |
| Overall | 181 | 141 (78) | 83 (46) | 72 (40) | 26 (14) | 5333 | 1793 (34) | 2987 (56) | 199 (4) | 350 (7) | 978 (18) | 1517 (28) | 1167 (22) | 1541 (29) |
| Participation | Patients | Site of enrolment | Clinical type of AF | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Centres | Centres enrolling >10 patients | University centre | Non-university centre | Specialized centre | Outpatient cardiology clinic | Cardiology ward | First (heart) aid | Other site | First detected AF | Paroxysmal AF | Persistent AF | Permanent AF | ||
| Western | 34 | 30 (88) | 14 (41) | 19 (56) | 1 (3) | 1354 | 684 (51) | 502 (37) | 85 (6) | 83 (6) | 184 (14) | 493 (36) | 233 (17) | 380 (28) |
| Austria | 3 | 3 | 1 | 1 | 1 | 119 | 76 | 37 | 5 | 1 | 25 | 32 | 29 | 19 |
| Belgium | 5 | 3 | 4 | 1 | 0 | 61 | 16 | 29 | 1 | 15 | 21 | 14 | 17 | 9 |
| Denmark | 1 | 1 | 1 | 0 | 0 | 26 | 0 | 26 | 0 | 0 | 3 | 13 | 6 | 3 |
| Finland | 2 | 2 | 2 | 0 | 0 | 68 | 51 | 17 | 0 | 0 | 3 | 37 | 14 | 13 |
| France | 4 | 2 | 1 | 3 | 0 | 51 | 10 | 40 | 0 | 1 | 13 | 15 | 6 | 17 |
| Germany | 2 | 2 | 1 | 1 | 0 | 192 | 34 | 128 | 0 | 30 | 15 | 88 | 23 | 63 |
| Sweden | 1 | 1 | 1 | 0 | 0 | 40 | 32 | 8 | 0 | 0 | 2 | 25 | 5 | 8 |
| Switzerland | 1 | 1 | 0 | 1 | 0 | 52 | 4 | 18 | 14 | 16 | 4 | 3 | 5 | 33 |
| The Netherlands | 13 | 13 | 2 | 11 | 0 | 714 | 430 | 199 | 65 | 16 | 96 | 256 | 115 | 209 |
| United Kingdom | 2 | 2 | 1 | 1 | 0 | 31 | 31 | 0 | 0 | 0 | 2 | 10 | 13 | 6 |
| Central | 53 | 42 (79) | 30 (57) | 9 (17) | 14 (26) | 1530 | 250 (16) | 1149 (75) | 36 (2) | 95 (6) | 265 (17) | 485 (32) | 357 (23) | 402 (26) |
| Armenia | 1 | 1 | 0 | 0 | 1 | 51 | 0 | 50 | 1 | 0 | 1 | 42 | 6 | 2 |
| Bulgaria | 5 | 4 | 2 | 2 | 1 | 107 | 1 | 66 | 1 | 39 | 25 | 22 | 19 | 40 |
| Croatia | 1 | 0 | 1 | 0 | 0 | 8 | 7 | 1 | 0 | 0 | 1 | 1 | 2 | 3 |
| Czech Republic | 4 | 4 | 2 | 1 | 1 | 176 | 39 | 119 | 12 | 6 | 24 | 45 | 39 | 65 |
| Georgia | 1 | 1 | 0 | 0 | 1 | 30 | 12 | 18 | 0 | 0 | 14 | 7 | 2 | 2 |
| Hungary | 3 | 2 | 1 | 1 | 1 | 82 | 0 | 80 | 0 | 2 | 29 | 22 | 10 | 21 |
| Lithuania | 4 | 4 | 2 | 2 | 0 | 118 | 23 | 91 | 1 | 3 | 13 | 43 | 46 | 15 |
| Macedonia | 1 | 0 | 1 | 0 | 0 | 2 | 0 | 2 | 0 | 0 | 1 | 0 | 1 | 0 |
| Moldova | 1 | 1 | 0 | 0 | 1 | 36 | 5 | 31 | 0 | 0 | 8 | 22 | 6 | 0 |
| Poland | 11 | 8 | 6 | 1 | 4 | 267 | 41 | 182 | 22 | 22 | 39 | 106 | 56 | 63 |
| Romania | 6 | 4 | 5 | 0 | 1 | 168 | 8 | 147 | 0 | 13 | 31 | 34 | 45 | 55 |
| Russia | 4 | 4 | 2 | 1 | 1 | 115 | 45 | 70 | 0 | 0 | 20 | 46 | 5 | 41 |
| Serbia & Montenegro | 2 | 1 | 1 | 1 | 0 | 30 | 1 | 29 | 0 | 0 | 14 | 4 | 10 | 1 |
| Slovakia | 4 | 4 | 3 | 0 | 1 | 121 | 20 | 95 | 0 | 0 | 18 | 35 | 45 | 23 |
| Slovenia | 1 | 1 | 1 | 0 | 0 | 32 | 29 | 3 | 0 | 0 | 3 | 22 | 3 | 4 |
| Ukraine | 4 | 3 | 3 | 0 | 1 | 187 | 19 | 165 | 0 | 3 | 24 | 34 | 62 | 67 |
| Mediterranean | 94 | 69 (73) | 39 (41) | 44 (47) | 11 (12) | 2449 | 859 (35) | 1336 (55) | 78 (3) | 176 (7) | 529 (22) | 539 (22) | 577 (24) | 759 (31) |
| Cyprus | 2 | 1 | 0 | 2 | 0 | 20 | 8 | 12 | 0 | 0 | 4 | 15 | 1 | 0 |
| Egypt | 3 | 3 | 3 | 0 | 0 | 133 | 28 | 91 | 2 | 12 | 22 | 30 | 14 | 60 |
| Greece | 10 | 10 | 1 | 7 | 2 | 323 | 51 | 261 | 7 | 4 | 79 | 105 | 57 | 70 |
| Israel | 7 | 1 | 6 | 1 | 0 | 59 | 22 | 32 | 0 | 5 | 25 | 12 | 16 | 5 |
| Italy | 32 | 24 | 6 | 23 | 3 | 843 | 334 | 432 | 36 | 41 | 145 | 184 | 290 | 206 |
| Portugal | 9 | 7 | 2 | 5 | 2 | 154 | 23 | 101 | 5 | 25 | 46 | 29 | 25 | 53 |
| Spain | 29 | 21 | 20 | 6 | 3 | 848 | 384 | 349 | 27 | 88 | 165 | 150 | 166 | 361 |
| Tunisia | 1 | 1 | 1 | 0 | 0 | 50 | 1 | 49 | 0 | 0 | 33 | 9 | 7 | 1 |
| Turkey | 1 | 1 | 0 | 0 | 1 | 19 | 8 | 9 | 1 | 1 | 10 | 5 | 1 | 3 |
| Overall | 181 | 141 (78) | 83 (46) | 72 (40) | 26 (14) | 5333 | 1793 (34) | 2987 (56) | 199 (4) | 350 (7) | 978 (18) | 1517 (28) | 1167 (22) | 1541 (29) |
Data are presented as observed number. Percentages were calculated within rows.
Geographical distribution of centre participation and patient enrolment
| Participation | Patients | Site of enrolment | Clinical type of AF | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Centres | Centres enrolling >10 patients | University centre | Non-university centre | Specialized centre | Outpatient cardiology clinic | Cardiology ward | First (heart) aid | Other site | First detected AF | Paroxysmal AF | Persistent AF | Permanent AF | ||
| Western | 34 | 30 (88) | 14 (41) | 19 (56) | 1 (3) | 1354 | 684 (51) | 502 (37) | 85 (6) | 83 (6) | 184 (14) | 493 (36) | 233 (17) | 380 (28) |
| Austria | 3 | 3 | 1 | 1 | 1 | 119 | 76 | 37 | 5 | 1 | 25 | 32 | 29 | 19 |
| Belgium | 5 | 3 | 4 | 1 | 0 | 61 | 16 | 29 | 1 | 15 | 21 | 14 | 17 | 9 |
| Denmark | 1 | 1 | 1 | 0 | 0 | 26 | 0 | 26 | 0 | 0 | 3 | 13 | 6 | 3 |
| Finland | 2 | 2 | 2 | 0 | 0 | 68 | 51 | 17 | 0 | 0 | 3 | 37 | 14 | 13 |
| France | 4 | 2 | 1 | 3 | 0 | 51 | 10 | 40 | 0 | 1 | 13 | 15 | 6 | 17 |
| Germany | 2 | 2 | 1 | 1 | 0 | 192 | 34 | 128 | 0 | 30 | 15 | 88 | 23 | 63 |
| Sweden | 1 | 1 | 1 | 0 | 0 | 40 | 32 | 8 | 0 | 0 | 2 | 25 | 5 | 8 |
| Switzerland | 1 | 1 | 0 | 1 | 0 | 52 | 4 | 18 | 14 | 16 | 4 | 3 | 5 | 33 |
| The Netherlands | 13 | 13 | 2 | 11 | 0 | 714 | 430 | 199 | 65 | 16 | 96 | 256 | 115 | 209 |
| United Kingdom | 2 | 2 | 1 | 1 | 0 | 31 | 31 | 0 | 0 | 0 | 2 | 10 | 13 | 6 |
| Central | 53 | 42 (79) | 30 (57) | 9 (17) | 14 (26) | 1530 | 250 (16) | 1149 (75) | 36 (2) | 95 (6) | 265 (17) | 485 (32) | 357 (23) | 402 (26) |
| Armenia | 1 | 1 | 0 | 0 | 1 | 51 | 0 | 50 | 1 | 0 | 1 | 42 | 6 | 2 |
| Bulgaria | 5 | 4 | 2 | 2 | 1 | 107 | 1 | 66 | 1 | 39 | 25 | 22 | 19 | 40 |
| Croatia | 1 | 0 | 1 | 0 | 0 | 8 | 7 | 1 | 0 | 0 | 1 | 1 | 2 | 3 |
| Czech Republic | 4 | 4 | 2 | 1 | 1 | 176 | 39 | 119 | 12 | 6 | 24 | 45 | 39 | 65 |
| Georgia | 1 | 1 | 0 | 0 | 1 | 30 | 12 | 18 | 0 | 0 | 14 | 7 | 2 | 2 |
| Hungary | 3 | 2 | 1 | 1 | 1 | 82 | 0 | 80 | 0 | 2 | 29 | 22 | 10 | 21 |
| Lithuania | 4 | 4 | 2 | 2 | 0 | 118 | 23 | 91 | 1 | 3 | 13 | 43 | 46 | 15 |
| Macedonia | 1 | 0 | 1 | 0 | 0 | 2 | 0 | 2 | 0 | 0 | 1 | 0 | 1 | 0 |
| Moldova | 1 | 1 | 0 | 0 | 1 | 36 | 5 | 31 | 0 | 0 | 8 | 22 | 6 | 0 |
| Poland | 11 | 8 | 6 | 1 | 4 | 267 | 41 | 182 | 22 | 22 | 39 | 106 | 56 | 63 |
| Romania | 6 | 4 | 5 | 0 | 1 | 168 | 8 | 147 | 0 | 13 | 31 | 34 | 45 | 55 |
| Russia | 4 | 4 | 2 | 1 | 1 | 115 | 45 | 70 | 0 | 0 | 20 | 46 | 5 | 41 |
| Serbia & Montenegro | 2 | 1 | 1 | 1 | 0 | 30 | 1 | 29 | 0 | 0 | 14 | 4 | 10 | 1 |
| Slovakia | 4 | 4 | 3 | 0 | 1 | 121 | 20 | 95 | 0 | 0 | 18 | 35 | 45 | 23 |
| Slovenia | 1 | 1 | 1 | 0 | 0 | 32 | 29 | 3 | 0 | 0 | 3 | 22 | 3 | 4 |
| Ukraine | 4 | 3 | 3 | 0 | 1 | 187 | 19 | 165 | 0 | 3 | 24 | 34 | 62 | 67 |
| Mediterranean | 94 | 69 (73) | 39 (41) | 44 (47) | 11 (12) | 2449 | 859 (35) | 1336 (55) | 78 (3) | 176 (7) | 529 (22) | 539 (22) | 577 (24) | 759 (31) |
| Cyprus | 2 | 1 | 0 | 2 | 0 | 20 | 8 | 12 | 0 | 0 | 4 | 15 | 1 | 0 |
| Egypt | 3 | 3 | 3 | 0 | 0 | 133 | 28 | 91 | 2 | 12 | 22 | 30 | 14 | 60 |
| Greece | 10 | 10 | 1 | 7 | 2 | 323 | 51 | 261 | 7 | 4 | 79 | 105 | 57 | 70 |
| Israel | 7 | 1 | 6 | 1 | 0 | 59 | 22 | 32 | 0 | 5 | 25 | 12 | 16 | 5 |
| Italy | 32 | 24 | 6 | 23 | 3 | 843 | 334 | 432 | 36 | 41 | 145 | 184 | 290 | 206 |
| Portugal | 9 | 7 | 2 | 5 | 2 | 154 | 23 | 101 | 5 | 25 | 46 | 29 | 25 | 53 |
| Spain | 29 | 21 | 20 | 6 | 3 | 848 | 384 | 349 | 27 | 88 | 165 | 150 | 166 | 361 |
| Tunisia | 1 | 1 | 1 | 0 | 0 | 50 | 1 | 49 | 0 | 0 | 33 | 9 | 7 | 1 |
| Turkey | 1 | 1 | 0 | 0 | 1 | 19 | 8 | 9 | 1 | 1 | 10 | 5 | 1 | 3 |
| Overall | 181 | 141 (78) | 83 (46) | 72 (40) | 26 (14) | 5333 | 1793 (34) | 2987 (56) | 199 (4) | 350 (7) | 978 (18) | 1517 (28) | 1167 (22) | 1541 (29) |
| Participation | Patients | Site of enrolment | Clinical type of AF | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Centres | Centres enrolling >10 patients | University centre | Non-university centre | Specialized centre | Outpatient cardiology clinic | Cardiology ward | First (heart) aid | Other site | First detected AF | Paroxysmal AF | Persistent AF | Permanent AF | ||
| Western | 34 | 30 (88) | 14 (41) | 19 (56) | 1 (3) | 1354 | 684 (51) | 502 (37) | 85 (6) | 83 (6) | 184 (14) | 493 (36) | 233 (17) | 380 (28) |
| Austria | 3 | 3 | 1 | 1 | 1 | 119 | 76 | 37 | 5 | 1 | 25 | 32 | 29 | 19 |
| Belgium | 5 | 3 | 4 | 1 | 0 | 61 | 16 | 29 | 1 | 15 | 21 | 14 | 17 | 9 |
| Denmark | 1 | 1 | 1 | 0 | 0 | 26 | 0 | 26 | 0 | 0 | 3 | 13 | 6 | 3 |
| Finland | 2 | 2 | 2 | 0 | 0 | 68 | 51 | 17 | 0 | 0 | 3 | 37 | 14 | 13 |
| France | 4 | 2 | 1 | 3 | 0 | 51 | 10 | 40 | 0 | 1 | 13 | 15 | 6 | 17 |
| Germany | 2 | 2 | 1 | 1 | 0 | 192 | 34 | 128 | 0 | 30 | 15 | 88 | 23 | 63 |
| Sweden | 1 | 1 | 1 | 0 | 0 | 40 | 32 | 8 | 0 | 0 | 2 | 25 | 5 | 8 |
| Switzerland | 1 | 1 | 0 | 1 | 0 | 52 | 4 | 18 | 14 | 16 | 4 | 3 | 5 | 33 |
| The Netherlands | 13 | 13 | 2 | 11 | 0 | 714 | 430 | 199 | 65 | 16 | 96 | 256 | 115 | 209 |
| United Kingdom | 2 | 2 | 1 | 1 | 0 | 31 | 31 | 0 | 0 | 0 | 2 | 10 | 13 | 6 |
| Central | 53 | 42 (79) | 30 (57) | 9 (17) | 14 (26) | 1530 | 250 (16) | 1149 (75) | 36 (2) | 95 (6) | 265 (17) | 485 (32) | 357 (23) | 402 (26) |
| Armenia | 1 | 1 | 0 | 0 | 1 | 51 | 0 | 50 | 1 | 0 | 1 | 42 | 6 | 2 |
| Bulgaria | 5 | 4 | 2 | 2 | 1 | 107 | 1 | 66 | 1 | 39 | 25 | 22 | 19 | 40 |
| Croatia | 1 | 0 | 1 | 0 | 0 | 8 | 7 | 1 | 0 | 0 | 1 | 1 | 2 | 3 |
| Czech Republic | 4 | 4 | 2 | 1 | 1 | 176 | 39 | 119 | 12 | 6 | 24 | 45 | 39 | 65 |
| Georgia | 1 | 1 | 0 | 0 | 1 | 30 | 12 | 18 | 0 | 0 | 14 | 7 | 2 | 2 |
| Hungary | 3 | 2 | 1 | 1 | 1 | 82 | 0 | 80 | 0 | 2 | 29 | 22 | 10 | 21 |
| Lithuania | 4 | 4 | 2 | 2 | 0 | 118 | 23 | 91 | 1 | 3 | 13 | 43 | 46 | 15 |
| Macedonia | 1 | 0 | 1 | 0 | 0 | 2 | 0 | 2 | 0 | 0 | 1 | 0 | 1 | 0 |
| Moldova | 1 | 1 | 0 | 0 | 1 | 36 | 5 | 31 | 0 | 0 | 8 | 22 | 6 | 0 |
| Poland | 11 | 8 | 6 | 1 | 4 | 267 | 41 | 182 | 22 | 22 | 39 | 106 | 56 | 63 |
| Romania | 6 | 4 | 5 | 0 | 1 | 168 | 8 | 147 | 0 | 13 | 31 | 34 | 45 | 55 |
| Russia | 4 | 4 | 2 | 1 | 1 | 115 | 45 | 70 | 0 | 0 | 20 | 46 | 5 | 41 |
| Serbia & Montenegro | 2 | 1 | 1 | 1 | 0 | 30 | 1 | 29 | 0 | 0 | 14 | 4 | 10 | 1 |
| Slovakia | 4 | 4 | 3 | 0 | 1 | 121 | 20 | 95 | 0 | 0 | 18 | 35 | 45 | 23 |
| Slovenia | 1 | 1 | 1 | 0 | 0 | 32 | 29 | 3 | 0 | 0 | 3 | 22 | 3 | 4 |
| Ukraine | 4 | 3 | 3 | 0 | 1 | 187 | 19 | 165 | 0 | 3 | 24 | 34 | 62 | 67 |
| Mediterranean | 94 | 69 (73) | 39 (41) | 44 (47) | 11 (12) | 2449 | 859 (35) | 1336 (55) | 78 (3) | 176 (7) | 529 (22) | 539 (22) | 577 (24) | 759 (31) |
| Cyprus | 2 | 1 | 0 | 2 | 0 | 20 | 8 | 12 | 0 | 0 | 4 | 15 | 1 | 0 |
| Egypt | 3 | 3 | 3 | 0 | 0 | 133 | 28 | 91 | 2 | 12 | 22 | 30 | 14 | 60 |
| Greece | 10 | 10 | 1 | 7 | 2 | 323 | 51 | 261 | 7 | 4 | 79 | 105 | 57 | 70 |
| Israel | 7 | 1 | 6 | 1 | 0 | 59 | 22 | 32 | 0 | 5 | 25 | 12 | 16 | 5 |
| Italy | 32 | 24 | 6 | 23 | 3 | 843 | 334 | 432 | 36 | 41 | 145 | 184 | 290 | 206 |
| Portugal | 9 | 7 | 2 | 5 | 2 | 154 | 23 | 101 | 5 | 25 | 46 | 29 | 25 | 53 |
| Spain | 29 | 21 | 20 | 6 | 3 | 848 | 384 | 349 | 27 | 88 | 165 | 150 | 166 | 361 |
| Tunisia | 1 | 1 | 1 | 0 | 0 | 50 | 1 | 49 | 0 | 0 | 33 | 9 | 7 | 1 |
| Turkey | 1 | 1 | 0 | 0 | 1 | 19 | 8 | 9 | 1 | 1 | 10 | 5 | 1 | 3 |
| Overall | 181 | 141 (78) | 83 (46) | 72 (40) | 26 (14) | 5333 | 1793 (34) | 2987 (56) | 199 (4) | 350 (7) | 978 (18) | 1517 (28) | 1167 (22) | 1541 (29) |
Data are presented as observed number. Percentages were calculated within rows.
Distribution of participation and patient enrolment per clinical type of AF
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Type of centre | |||||
| University | 481 (49) | 669 (44) | 572 (49) | 731 (48) | |
| Non-university | 344 (35) | 596 (39) | 457 (39) | 619 (40) | |
| Specialised | 149 (15) | 247 (16) | 136 (12) | 188 (12) | |
| Site of inclusion | |||||
| Cardiology ward | 622 (64) | 842 (56) | 711 (61) | 750 (49) | * |
| Outpatient clinic | 209 (21) | 524 (35) | 371 (32) | 633 (41) | * |
| First (heart) aid | 54 (6) | 83 (6) | 32 (3) | 25 (2) | * |
| Other site | 93 (9) | 67 (4) | 53 (5) | 132 (9) | * |
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Type of centre | |||||
| University | 481 (49) | 669 (44) | 572 (49) | 731 (48) | |
| Non-university | 344 (35) | 596 (39) | 457 (39) | 619 (40) | |
| Specialised | 149 (15) | 247 (16) | 136 (12) | 188 (12) | |
| Site of inclusion | |||||
| Cardiology ward | 622 (64) | 842 (56) | 711 (61) | 750 (49) | * |
| Outpatient clinic | 209 (21) | 524 (35) | 371 (32) | 633 (41) | * |
| First (heart) aid | 54 (6) | 83 (6) | 32 (3) | 25 (2) | * |
| Other site | 93 (9) | 67 (4) | 53 (5) | 132 (9) | * |
Data are presented as observed number (%) within type of AF.
*Difference with P<0.001 among the four AF types.
Distribution of participation and patient enrolment per clinical type of AF
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Type of centre | |||||
| University | 481 (49) | 669 (44) | 572 (49) | 731 (48) | |
| Non-university | 344 (35) | 596 (39) | 457 (39) | 619 (40) | |
| Specialised | 149 (15) | 247 (16) | 136 (12) | 188 (12) | |
| Site of inclusion | |||||
| Cardiology ward | 622 (64) | 842 (56) | 711 (61) | 750 (49) | * |
| Outpatient clinic | 209 (21) | 524 (35) | 371 (32) | 633 (41) | * |
| First (heart) aid | 54 (6) | 83 (6) | 32 (3) | 25 (2) | * |
| Other site | 93 (9) | 67 (4) | 53 (5) | 132 (9) | * |
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Type of centre | |||||
| University | 481 (49) | 669 (44) | 572 (49) | 731 (48) | |
| Non-university | 344 (35) | 596 (39) | 457 (39) | 619 (40) | |
| Specialised | 149 (15) | 247 (16) | 136 (12) | 188 (12) | |
| Site of inclusion | |||||
| Cardiology ward | 622 (64) | 842 (56) | 711 (61) | 750 (49) | * |
| Outpatient clinic | 209 (21) | 524 (35) | 371 (32) | 633 (41) | * |
| First (heart) aid | 54 (6) | 83 (6) | 32 (3) | 25 (2) | * |
| Other site | 93 (9) | 67 (4) | 53 (5) | 132 (9) | * |
Data are presented as observed number (%) within type of AF.
*Difference with P<0.001 among the four AF types.
Patient characteristics
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age, years | 65 (14) | 64 (13) | 66 (12) | 71 (11) | * |
| Female gender | 418 (43) | 652 (43) | 451 (39) | 668 (43) | |
| Concomitant disease | |||||
| Hypertension | 620 (63) | 942 (62) | 772 (66) | 984 (64) | |
| Coronary artery disease | 309 (32) | 514 (34) | 338 (29) | 543 (36) | |
| Acute infarction | 65 (7) | 32 (2) | 24 (2) | 41 (3) | * |
| Old infarction | 124 (13) | 228 (15) | 142 (12) | 259 (17) | |
| Previous PCI / CABG | 102 (11) | 187 (12) | 136 (12) | 166 (11) | |
| Angina | 179 (19) | 350 (23) | 172 (15) | 304 (20) | * |
| Heart failure | 255 (26) | 341 (23) | 401 (35) | 754 (49) | * |
| Valvular heart disease | 203 (21) | 287 (19) | 276 (24) | 607 (40) | * |
| Cardiomyopathy | 79 (8) | 101 (7) | 148 (13) | 243 (16) | * |
| Tachycardiomyopathy | 9 (1) | 4 (0) | 28 (2) | 14 (1) | * |
| Hypertrophic | 25 (3) | 34 (2) | 24 (2) | 21 (1) | |
| Dilated | 38 (4) | 49 (3) | 73 (6) | 152 (10) | * |
| Other type | 7 (1) | 14 (1) | 23 (2) | 56 (4) | * |
| Sick sinus syndrome | 9 (1) | 93 (6) | 55 (5) | 82 (5) | * |
| Chronic obstructive pulmonary disease | 103 (11) | 185 (12) | 133 (12) | 272 (18) | * |
| Thyroid disease | 61 (7) | 148 (11) | 132 (12) | 149 (11) | |
| Idiopathic AFa | 130 (14) | 226 (15) | 112 (10) | 61 (4) | * |
| Cardiovascular risk factors | |||||
| Diabetes mellitus | 187 (19) | 232 (15) | 186 (16) | 336 (22) | * |
| Hyperlipidemia | 309 (32) | 588 (40) | 413 (36) | 518 (34) | |
| Current smoker | 181 (19) | 204 (14) | 128 (11) | 120 (8) | * |
| No regular exercise | 484 (51) | 596 (42) | 488 (44) | 785 (53) | * |
| Family history of CAD | 111 (14) | 291 (23) | 195 (20) | 252 (20) | * |
| Comorbidities | |||||
| Previous thromboembolism | 87 (9) | 158 (11) | 122 (11) | 273 (18) | * |
| Stroke | 41 (4) | 64 (4) | 51 (4) | 135 (9) | * |
| TIA | 28 (3) | 83 (6) | 56 (5) | 98 (6) | |
| Other thromboembolism | 24 (3) | 25 (2) | 27 (2) | 72 (5) | * |
| Prior major bleeding | 6 (1) | 19 (1) | 16 (1) | 45 (3) | * |
| Malignancy | 49 (5) | 73 (5) | 54 (5) | 97 (6) | |
| Peripheral vascular disease | 59 (6) | 97 (7) | 77 (7) | 162 (11) | * |
| Renal failure | 41 (4) | 84 (6) | 60 (5) | 119 (8) | |
| Previous interventions | |||||
| Pharmacological conversion | 106 (11) | 733 (49) | 435 (37) | 291 (19) | * |
| Electrical cardioversion | 39 (4) | 388 (26) | 436 (38) | 324 (21) | * |
| Catheter ablation | 0 (0) | 78 (5) | 45 (4) | 24 (2) | * |
| Pacemaker implantation | 19 (2) | 88 (6) | 51 (4) | 145 (9) | * |
| ICD implantation | 4 (0) | 23 (2) | 11 (1) | 18 (1) | |
| Surgery for AF | 2 (2) | 12 (1) | 9 (1) | 6 (0) | |
| Miscellaneous | |||||
| Clinical trial | 96 (10) | 229 (15) | 136 (12) | 163 (11) | * |
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age, years | 65 (14) | 64 (13) | 66 (12) | 71 (11) | * |
| Female gender | 418 (43) | 652 (43) | 451 (39) | 668 (43) | |
| Concomitant disease | |||||
| Hypertension | 620 (63) | 942 (62) | 772 (66) | 984 (64) | |
| Coronary artery disease | 309 (32) | 514 (34) | 338 (29) | 543 (36) | |
| Acute infarction | 65 (7) | 32 (2) | 24 (2) | 41 (3) | * |
| Old infarction | 124 (13) | 228 (15) | 142 (12) | 259 (17) | |
| Previous PCI / CABG | 102 (11) | 187 (12) | 136 (12) | 166 (11) | |
| Angina | 179 (19) | 350 (23) | 172 (15) | 304 (20) | * |
| Heart failure | 255 (26) | 341 (23) | 401 (35) | 754 (49) | * |
| Valvular heart disease | 203 (21) | 287 (19) | 276 (24) | 607 (40) | * |
| Cardiomyopathy | 79 (8) | 101 (7) | 148 (13) | 243 (16) | * |
| Tachycardiomyopathy | 9 (1) | 4 (0) | 28 (2) | 14 (1) | * |
| Hypertrophic | 25 (3) | 34 (2) | 24 (2) | 21 (1) | |
| Dilated | 38 (4) | 49 (3) | 73 (6) | 152 (10) | * |
| Other type | 7 (1) | 14 (1) | 23 (2) | 56 (4) | * |
| Sick sinus syndrome | 9 (1) | 93 (6) | 55 (5) | 82 (5) | * |
| Chronic obstructive pulmonary disease | 103 (11) | 185 (12) | 133 (12) | 272 (18) | * |
| Thyroid disease | 61 (7) | 148 (11) | 132 (12) | 149 (11) | |
| Idiopathic AFa | 130 (14) | 226 (15) | 112 (10) | 61 (4) | * |
| Cardiovascular risk factors | |||||
| Diabetes mellitus | 187 (19) | 232 (15) | 186 (16) | 336 (22) | * |
| Hyperlipidemia | 309 (32) | 588 (40) | 413 (36) | 518 (34) | |
| Current smoker | 181 (19) | 204 (14) | 128 (11) | 120 (8) | * |
| No regular exercise | 484 (51) | 596 (42) | 488 (44) | 785 (53) | * |
| Family history of CAD | 111 (14) | 291 (23) | 195 (20) | 252 (20) | * |
| Comorbidities | |||||
| Previous thromboembolism | 87 (9) | 158 (11) | 122 (11) | 273 (18) | * |
| Stroke | 41 (4) | 64 (4) | 51 (4) | 135 (9) | * |
| TIA | 28 (3) | 83 (6) | 56 (5) | 98 (6) | |
| Other thromboembolism | 24 (3) | 25 (2) | 27 (2) | 72 (5) | * |
| Prior major bleeding | 6 (1) | 19 (1) | 16 (1) | 45 (3) | * |
| Malignancy | 49 (5) | 73 (5) | 54 (5) | 97 (6) | |
| Peripheral vascular disease | 59 (6) | 97 (7) | 77 (7) | 162 (11) | * |
| Renal failure | 41 (4) | 84 (6) | 60 (5) | 119 (8) | |
| Previous interventions | |||||
| Pharmacological conversion | 106 (11) | 733 (49) | 435 (37) | 291 (19) | * |
| Electrical cardioversion | 39 (4) | 388 (26) | 436 (38) | 324 (21) | * |
| Catheter ablation | 0 (0) | 78 (5) | 45 (4) | 24 (2) | * |
| Pacemaker implantation | 19 (2) | 88 (6) | 51 (4) | 145 (9) | * |
| ICD implantation | 4 (0) | 23 (2) | 11 (1) | 18 (1) | |
| Surgery for AF | 2 (2) | 12 (1) | 9 (1) | 6 (0) | |
| Miscellaneous | |||||
| Clinical trial | 96 (10) | 229 (15) | 136 (12) | 163 (11) | * |
Data are presented as mean (standard deviation) or observed number (%) within type of AF.
*Difference with P<0.001 among the four AF types.
aNone of the reported concomitant diseases.PCI, percutaneous coronary intervenion; CABG, coronary artery bypass grafting; CAD, coronary artery disease; TIA, transient ischaemic attack; ICD, implantable cardioverter defibrillator.
Patient characteristics
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age, years | 65 (14) | 64 (13) | 66 (12) | 71 (11) | * |
| Female gender | 418 (43) | 652 (43) | 451 (39) | 668 (43) | |
| Concomitant disease | |||||
| Hypertension | 620 (63) | 942 (62) | 772 (66) | 984 (64) | |
| Coronary artery disease | 309 (32) | 514 (34) | 338 (29) | 543 (36) | |
| Acute infarction | 65 (7) | 32 (2) | 24 (2) | 41 (3) | * |
| Old infarction | 124 (13) | 228 (15) | 142 (12) | 259 (17) | |
| Previous PCI / CABG | 102 (11) | 187 (12) | 136 (12) | 166 (11) | |
| Angina | 179 (19) | 350 (23) | 172 (15) | 304 (20) | * |
| Heart failure | 255 (26) | 341 (23) | 401 (35) | 754 (49) | * |
| Valvular heart disease | 203 (21) | 287 (19) | 276 (24) | 607 (40) | * |
| Cardiomyopathy | 79 (8) | 101 (7) | 148 (13) | 243 (16) | * |
| Tachycardiomyopathy | 9 (1) | 4 (0) | 28 (2) | 14 (1) | * |
| Hypertrophic | 25 (3) | 34 (2) | 24 (2) | 21 (1) | |
| Dilated | 38 (4) | 49 (3) | 73 (6) | 152 (10) | * |
| Other type | 7 (1) | 14 (1) | 23 (2) | 56 (4) | * |
| Sick sinus syndrome | 9 (1) | 93 (6) | 55 (5) | 82 (5) | * |
| Chronic obstructive pulmonary disease | 103 (11) | 185 (12) | 133 (12) | 272 (18) | * |
| Thyroid disease | 61 (7) | 148 (11) | 132 (12) | 149 (11) | |
| Idiopathic AFa | 130 (14) | 226 (15) | 112 (10) | 61 (4) | * |
| Cardiovascular risk factors | |||||
| Diabetes mellitus | 187 (19) | 232 (15) | 186 (16) | 336 (22) | * |
| Hyperlipidemia | 309 (32) | 588 (40) | 413 (36) | 518 (34) | |
| Current smoker | 181 (19) | 204 (14) | 128 (11) | 120 (8) | * |
| No regular exercise | 484 (51) | 596 (42) | 488 (44) | 785 (53) | * |
| Family history of CAD | 111 (14) | 291 (23) | 195 (20) | 252 (20) | * |
| Comorbidities | |||||
| Previous thromboembolism | 87 (9) | 158 (11) | 122 (11) | 273 (18) | * |
| Stroke | 41 (4) | 64 (4) | 51 (4) | 135 (9) | * |
| TIA | 28 (3) | 83 (6) | 56 (5) | 98 (6) | |
| Other thromboembolism | 24 (3) | 25 (2) | 27 (2) | 72 (5) | * |
| Prior major bleeding | 6 (1) | 19 (1) | 16 (1) | 45 (3) | * |
| Malignancy | 49 (5) | 73 (5) | 54 (5) | 97 (6) | |
| Peripheral vascular disease | 59 (6) | 97 (7) | 77 (7) | 162 (11) | * |
| Renal failure | 41 (4) | 84 (6) | 60 (5) | 119 (8) | |
| Previous interventions | |||||
| Pharmacological conversion | 106 (11) | 733 (49) | 435 (37) | 291 (19) | * |
| Electrical cardioversion | 39 (4) | 388 (26) | 436 (38) | 324 (21) | * |
| Catheter ablation | 0 (0) | 78 (5) | 45 (4) | 24 (2) | * |
| Pacemaker implantation | 19 (2) | 88 (6) | 51 (4) | 145 (9) | * |
| ICD implantation | 4 (0) | 23 (2) | 11 (1) | 18 (1) | |
| Surgery for AF | 2 (2) | 12 (1) | 9 (1) | 6 (0) | |
| Miscellaneous | |||||
| Clinical trial | 96 (10) | 229 (15) | 136 (12) | 163 (11) | * |
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age, years | 65 (14) | 64 (13) | 66 (12) | 71 (11) | * |
| Female gender | 418 (43) | 652 (43) | 451 (39) | 668 (43) | |
| Concomitant disease | |||||
| Hypertension | 620 (63) | 942 (62) | 772 (66) | 984 (64) | |
| Coronary artery disease | 309 (32) | 514 (34) | 338 (29) | 543 (36) | |
| Acute infarction | 65 (7) | 32 (2) | 24 (2) | 41 (3) | * |
| Old infarction | 124 (13) | 228 (15) | 142 (12) | 259 (17) | |
| Previous PCI / CABG | 102 (11) | 187 (12) | 136 (12) | 166 (11) | |
| Angina | 179 (19) | 350 (23) | 172 (15) | 304 (20) | * |
| Heart failure | 255 (26) | 341 (23) | 401 (35) | 754 (49) | * |
| Valvular heart disease | 203 (21) | 287 (19) | 276 (24) | 607 (40) | * |
| Cardiomyopathy | 79 (8) | 101 (7) | 148 (13) | 243 (16) | * |
| Tachycardiomyopathy | 9 (1) | 4 (0) | 28 (2) | 14 (1) | * |
| Hypertrophic | 25 (3) | 34 (2) | 24 (2) | 21 (1) | |
| Dilated | 38 (4) | 49 (3) | 73 (6) | 152 (10) | * |
| Other type | 7 (1) | 14 (1) | 23 (2) | 56 (4) | * |
| Sick sinus syndrome | 9 (1) | 93 (6) | 55 (5) | 82 (5) | * |
| Chronic obstructive pulmonary disease | 103 (11) | 185 (12) | 133 (12) | 272 (18) | * |
| Thyroid disease | 61 (7) | 148 (11) | 132 (12) | 149 (11) | |
| Idiopathic AFa | 130 (14) | 226 (15) | 112 (10) | 61 (4) | * |
| Cardiovascular risk factors | |||||
| Diabetes mellitus | 187 (19) | 232 (15) | 186 (16) | 336 (22) | * |
| Hyperlipidemia | 309 (32) | 588 (40) | 413 (36) | 518 (34) | |
| Current smoker | 181 (19) | 204 (14) | 128 (11) | 120 (8) | * |
| No regular exercise | 484 (51) | 596 (42) | 488 (44) | 785 (53) | * |
| Family history of CAD | 111 (14) | 291 (23) | 195 (20) | 252 (20) | * |
| Comorbidities | |||||
| Previous thromboembolism | 87 (9) | 158 (11) | 122 (11) | 273 (18) | * |
| Stroke | 41 (4) | 64 (4) | 51 (4) | 135 (9) | * |
| TIA | 28 (3) | 83 (6) | 56 (5) | 98 (6) | |
| Other thromboembolism | 24 (3) | 25 (2) | 27 (2) | 72 (5) | * |
| Prior major bleeding | 6 (1) | 19 (1) | 16 (1) | 45 (3) | * |
| Malignancy | 49 (5) | 73 (5) | 54 (5) | 97 (6) | |
| Peripheral vascular disease | 59 (6) | 97 (7) | 77 (7) | 162 (11) | * |
| Renal failure | 41 (4) | 84 (6) | 60 (5) | 119 (8) | |
| Previous interventions | |||||
| Pharmacological conversion | 106 (11) | 733 (49) | 435 (37) | 291 (19) | * |
| Electrical cardioversion | 39 (4) | 388 (26) | 436 (38) | 324 (21) | * |
| Catheter ablation | 0 (0) | 78 (5) | 45 (4) | 24 (2) | * |
| Pacemaker implantation | 19 (2) | 88 (6) | 51 (4) | 145 (9) | * |
| ICD implantation | 4 (0) | 23 (2) | 11 (1) | 18 (1) | |
| Surgery for AF | 2 (2) | 12 (1) | 9 (1) | 6 (0) | |
| Miscellaneous | |||||
| Clinical trial | 96 (10) | 229 (15) | 136 (12) | 163 (11) | * |
Data are presented as mean (standard deviation) or observed number (%) within type of AF.
*Difference with P<0.001 among the four AF types.
aNone of the reported concomitant diseases.PCI, percutaneous coronary intervenion; CABG, coronary artery bypass grafting; CAD, coronary artery disease; TIA, transient ischaemic attack; ICD, implantable cardioverter defibrillator.
Admission/consultation information
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Reason admission/consultation | |||||
| AF only | 446 (46) | 709 (47) | 577 (50) | 361 (24) | * |
| AF and other reason | 375 (38) | 559 (37) | 472 (41) | 772 (50) | * |
| Other reason only | 156 (16) | 247 (16) | 116 (10) | 404 (26) | * |
| Symptoms | |||||
| Current AF symptomsa | 749 (77) | 1167 (77) | 854 (73) | 848 (55) | * |
| Previous AF symptoms | 62 (7) | 235 (16) | 173 (15) | 287 (20) | * |
| Never AF symptoms | 150 (16) | 86 (6) | 119 (10) | 293 (21) | * |
| Heart failure NYHA class III/IV | 162 (17) | 113 (8) | 170 (15) | 382 (25) | * |
| Physical examination | |||||
| BMI (kg/m2) | 28 (6) | 28 (9) | 28 (9) | 27 (5) | |
| Systolic BP (mmHg) | 135 (23) | 136 (22) | 136 (22) | 136 (22) | |
| Diastolic BP (mmHg) | 80 (14) | 81 (13) | 82 (13) | 79 (13) | * |
| ECG | |||||
| Atrial fibrillation | 736 (75) | 816 (54) | 867 (74) | 1486 (97) | * |
| LVH | 160 (17) | 272 (19) | 234 (21) | 344 (23) | * |
| Left BBB | 58 (6) | 101 (7) | 82 (7) | 144 (10) | * |
| Right BBB | 60 (6) | 101 (7) | 73 (6) | 148 (10) | * |
| Heart rate (bpm) | 103 (34) | 91 (32) | 90 (29) | 87 (26) | * |
| QRS duration (ms) | 93 (25) | 97 (28) | 99 (27) | 104 (31) | * |
| TTEb | |||||
| LA diameter, (mm) | 43 (8) | 43 (7) | 46 (8) | 51 (17) | * |
| LVEF (%) | 52 (14) | 53 (14) | 51 (15) | 51 (15) | |
| LVH | 249 (34) | 380 (33) | 336 (36) | 401 (35) | |
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Reason admission/consultation | |||||
| AF only | 446 (46) | 709 (47) | 577 (50) | 361 (24) | * |
| AF and other reason | 375 (38) | 559 (37) | 472 (41) | 772 (50) | * |
| Other reason only | 156 (16) | 247 (16) | 116 (10) | 404 (26) | * |
| Symptoms | |||||
| Current AF symptomsa | 749 (77) | 1167 (77) | 854 (73) | 848 (55) | * |
| Previous AF symptoms | 62 (7) | 235 (16) | 173 (15) | 287 (20) | * |
| Never AF symptoms | 150 (16) | 86 (6) | 119 (10) | 293 (21) | * |
| Heart failure NYHA class III/IV | 162 (17) | 113 (8) | 170 (15) | 382 (25) | * |
| Physical examination | |||||
| BMI (kg/m2) | 28 (6) | 28 (9) | 28 (9) | 27 (5) | |
| Systolic BP (mmHg) | 135 (23) | 136 (22) | 136 (22) | 136 (22) | |
| Diastolic BP (mmHg) | 80 (14) | 81 (13) | 82 (13) | 79 (13) | * |
| ECG | |||||
| Atrial fibrillation | 736 (75) | 816 (54) | 867 (74) | 1486 (97) | * |
| LVH | 160 (17) | 272 (19) | 234 (21) | 344 (23) | * |
| Left BBB | 58 (6) | 101 (7) | 82 (7) | 144 (10) | * |
| Right BBB | 60 (6) | 101 (7) | 73 (6) | 148 (10) | * |
| Heart rate (bpm) | 103 (34) | 91 (32) | 90 (29) | 87 (26) | * |
| QRS duration (ms) | 93 (25) | 97 (28) | 99 (27) | 104 (31) | * |
| TTEb | |||||
| LA diameter, (mm) | 43 (8) | 43 (7) | 46 (8) | 51 (17) | * |
| LVEF (%) | 52 (14) | 53 (14) | 51 (15) | 51 (15) | |
| LVH | 249 (34) | 380 (33) | 336 (36) | 401 (35) | |
Data are presented as mean (standard deviation) or observed number (%) within type of AF.
BMI, body mass index; BP, blood pressure; LVH, left ventricular hypertrophy; BBB, bundle branch block; TTE, transthoracic echocardiography; LA, left atrium; LVEF, left ventricular ejection fraction.
*Difference with P<0.001 among the four AF types.
aIncludes palpitations, syncope, dyspnea, chest pain, dizziness, fatigue, and non-specified symptoms.
bPerformed during qualifying admission/visit, or maximally 1 year prior to inclusion.
Admission/consultation information
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Reason admission/consultation | |||||
| AF only | 446 (46) | 709 (47) | 577 (50) | 361 (24) | * |
| AF and other reason | 375 (38) | 559 (37) | 472 (41) | 772 (50) | * |
| Other reason only | 156 (16) | 247 (16) | 116 (10) | 404 (26) | * |
| Symptoms | |||||
| Current AF symptomsa | 749 (77) | 1167 (77) | 854 (73) | 848 (55) | * |
| Previous AF symptoms | 62 (7) | 235 (16) | 173 (15) | 287 (20) | * |
| Never AF symptoms | 150 (16) | 86 (6) | 119 (10) | 293 (21) | * |
| Heart failure NYHA class III/IV | 162 (17) | 113 (8) | 170 (15) | 382 (25) | * |
| Physical examination | |||||
| BMI (kg/m2) | 28 (6) | 28 (9) | 28 (9) | 27 (5) | |
| Systolic BP (mmHg) | 135 (23) | 136 (22) | 136 (22) | 136 (22) | |
| Diastolic BP (mmHg) | 80 (14) | 81 (13) | 82 (13) | 79 (13) | * |
| ECG | |||||
| Atrial fibrillation | 736 (75) | 816 (54) | 867 (74) | 1486 (97) | * |
| LVH | 160 (17) | 272 (19) | 234 (21) | 344 (23) | * |
| Left BBB | 58 (6) | 101 (7) | 82 (7) | 144 (10) | * |
| Right BBB | 60 (6) | 101 (7) | 73 (6) | 148 (10) | * |
| Heart rate (bpm) | 103 (34) | 91 (32) | 90 (29) | 87 (26) | * |
| QRS duration (ms) | 93 (25) | 97 (28) | 99 (27) | 104 (31) | * |
| TTEb | |||||
| LA diameter, (mm) | 43 (8) | 43 (7) | 46 (8) | 51 (17) | * |
| LVEF (%) | 52 (14) | 53 (14) | 51 (15) | 51 (15) | |
| LVH | 249 (34) | 380 (33) | 336 (36) | 401 (35) | |
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Reason admission/consultation | |||||
| AF only | 446 (46) | 709 (47) | 577 (50) | 361 (24) | * |
| AF and other reason | 375 (38) | 559 (37) | 472 (41) | 772 (50) | * |
| Other reason only | 156 (16) | 247 (16) | 116 (10) | 404 (26) | * |
| Symptoms | |||||
| Current AF symptomsa | 749 (77) | 1167 (77) | 854 (73) | 848 (55) | * |
| Previous AF symptoms | 62 (7) | 235 (16) | 173 (15) | 287 (20) | * |
| Never AF symptoms | 150 (16) | 86 (6) | 119 (10) | 293 (21) | * |
| Heart failure NYHA class III/IV | 162 (17) | 113 (8) | 170 (15) | 382 (25) | * |
| Physical examination | |||||
| BMI (kg/m2) | 28 (6) | 28 (9) | 28 (9) | 27 (5) | |
| Systolic BP (mmHg) | 135 (23) | 136 (22) | 136 (22) | 136 (22) | |
| Diastolic BP (mmHg) | 80 (14) | 81 (13) | 82 (13) | 79 (13) | * |
| ECG | |||||
| Atrial fibrillation | 736 (75) | 816 (54) | 867 (74) | 1486 (97) | * |
| LVH | 160 (17) | 272 (19) | 234 (21) | 344 (23) | * |
| Left BBB | 58 (6) | 101 (7) | 82 (7) | 144 (10) | * |
| Right BBB | 60 (6) | 101 (7) | 73 (6) | 148 (10) | * |
| Heart rate (bpm) | 103 (34) | 91 (32) | 90 (29) | 87 (26) | * |
| QRS duration (ms) | 93 (25) | 97 (28) | 99 (27) | 104 (31) | * |
| TTEb | |||||
| LA diameter, (mm) | 43 (8) | 43 (7) | 46 (8) | 51 (17) | * |
| LVEF (%) | 52 (14) | 53 (14) | 51 (15) | 51 (15) | |
| LVH | 249 (34) | 380 (33) | 336 (36) | 401 (35) | |
Data are presented as mean (standard deviation) or observed number (%) within type of AF.
BMI, body mass index; BP, blood pressure; LVH, left ventricular hypertrophy; BBB, bundle branch block; TTE, transthoracic echocardiography; LA, left atrium; LVEF, left ventricular ejection fraction.
*Difference with P<0.001 among the four AF types.
aIncludes palpitations, syncope, dyspnea, chest pain, dizziness, fatigue, and non-specified symptoms.
bPerformed during qualifying admission/visit, or maximally 1 year prior to inclusion.
Diagnostics and interventions
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Diagnosticsa | |||||
| TTE | 757 (78) | 1275 (84) | 1025 (88) | 1332 (87) | * |
| Chest X-ray | 803 (82) | 1155 (77) | 923 (80) | 1321 (86) | * |
| Holter monitoring | 135 (14) | 549 (36) | 323 (28) | 511 (31) | * |
| Exercise test | 126 (13) | 442 (29) | 234 (20) | 263 (17) | * |
| TEE | 114 (12) | 173 (11) | 227 (20) | 166 (11) | * |
| Electrophysiology | 14 (1) | 143 (10) | 81 (7) | 66 (4) | * |
| Event recorder | 20 (2) | 36 (2) | 19 (2) | 11 (1) | |
| Thyroid hormone levels measurement | 394 (40) | 782 (52) | 644 (55) | 609 (40) | * |
| Interventionsb | |||||
| Pharmacological conversion | 378 (39) | 496 (33) | 213 (18) | 41 (3) | * |
| Electrical cardioversion | 191 (20) | 216 (14) | 424 (36) | 69 (5) | * |
| Catheter ablation | 0 (0) | 75 (5) | 43 (4) | 16 (1) | * |
| Pacemaker implantation | 14 (1) | 54 (4) | 29 (3) | 101 (7) | * |
| ICD implantation | 0 (0) | 4 (0) | 9 (1) | 14 (1) | |
| AF surgery | 0 (0) | 4 (0) | 2 (0) | 1 (0) | |
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Diagnosticsa | |||||
| TTE | 757 (78) | 1275 (84) | 1025 (88) | 1332 (87) | * |
| Chest X-ray | 803 (82) | 1155 (77) | 923 (80) | 1321 (86) | * |
| Holter monitoring | 135 (14) | 549 (36) | 323 (28) | 511 (31) | * |
| Exercise test | 126 (13) | 442 (29) | 234 (20) | 263 (17) | * |
| TEE | 114 (12) | 173 (11) | 227 (20) | 166 (11) | * |
| Electrophysiology | 14 (1) | 143 (10) | 81 (7) | 66 (4) | * |
| Event recorder | 20 (2) | 36 (2) | 19 (2) | 11 (1) | |
| Thyroid hormone levels measurement | 394 (40) | 782 (52) | 644 (55) | 609 (40) | * |
| Interventionsb | |||||
| Pharmacological conversion | 378 (39) | 496 (33) | 213 (18) | 41 (3) | * |
| Electrical cardioversion | 191 (20) | 216 (14) | 424 (36) | 69 (5) | * |
| Catheter ablation | 0 (0) | 75 (5) | 43 (4) | 16 (1) | * |
| Pacemaker implantation | 14 (1) | 54 (4) | 29 (3) | 101 (7) | * |
| ICD implantation | 0 (0) | 4 (0) | 9 (1) | 14 (1) | |
| AF surgery | 0 (0) | 4 (0) | 2 (0) | 1 (0) | |
Data are presented as observed number (%) within type of AF.
TEE, transesophageal echocardiography; ICD, implantable cardioverter defibrillator.
*Difference with P<0.001 among the four AF types.
aPrior to, or during qualifying admission/consultation.
bDuring qualifying admission or consultation.
Diagnostics and interventions
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Diagnosticsa | |||||
| TTE | 757 (78) | 1275 (84) | 1025 (88) | 1332 (87) | * |
| Chest X-ray | 803 (82) | 1155 (77) | 923 (80) | 1321 (86) | * |
| Holter monitoring | 135 (14) | 549 (36) | 323 (28) | 511 (31) | * |
| Exercise test | 126 (13) | 442 (29) | 234 (20) | 263 (17) | * |
| TEE | 114 (12) | 173 (11) | 227 (20) | 166 (11) | * |
| Electrophysiology | 14 (1) | 143 (10) | 81 (7) | 66 (4) | * |
| Event recorder | 20 (2) | 36 (2) | 19 (2) | 11 (1) | |
| Thyroid hormone levels measurement | 394 (40) | 782 (52) | 644 (55) | 609 (40) | * |
| Interventionsb | |||||
| Pharmacological conversion | 378 (39) | 496 (33) | 213 (18) | 41 (3) | * |
| Electrical cardioversion | 191 (20) | 216 (14) | 424 (36) | 69 (5) | * |
| Catheter ablation | 0 (0) | 75 (5) | 43 (4) | 16 (1) | * |
| Pacemaker implantation | 14 (1) | 54 (4) | 29 (3) | 101 (7) | * |
| ICD implantation | 0 (0) | 4 (0) | 9 (1) | 14 (1) | |
| AF surgery | 0 (0) | 4 (0) | 2 (0) | 1 (0) | |
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Diagnosticsa | |||||
| TTE | 757 (78) | 1275 (84) | 1025 (88) | 1332 (87) | * |
| Chest X-ray | 803 (82) | 1155 (77) | 923 (80) | 1321 (86) | * |
| Holter monitoring | 135 (14) | 549 (36) | 323 (28) | 511 (31) | * |
| Exercise test | 126 (13) | 442 (29) | 234 (20) | 263 (17) | * |
| TEE | 114 (12) | 173 (11) | 227 (20) | 166 (11) | * |
| Electrophysiology | 14 (1) | 143 (10) | 81 (7) | 66 (4) | * |
| Event recorder | 20 (2) | 36 (2) | 19 (2) | 11 (1) | |
| Thyroid hormone levels measurement | 394 (40) | 782 (52) | 644 (55) | 609 (40) | * |
| Interventionsb | |||||
| Pharmacological conversion | 378 (39) | 496 (33) | 213 (18) | 41 (3) | * |
| Electrical cardioversion | 191 (20) | 216 (14) | 424 (36) | 69 (5) | * |
| Catheter ablation | 0 (0) | 75 (5) | 43 (4) | 16 (1) | * |
| Pacemaker implantation | 14 (1) | 54 (4) | 29 (3) | 101 (7) | * |
| ICD implantation | 0 (0) | 4 (0) | 9 (1) | 14 (1) | |
| AF surgery | 0 (0) | 4 (0) | 2 (0) | 1 (0) | |
Data are presented as observed number (%) within type of AF.
TEE, transesophageal echocardiography; ICD, implantable cardioverter defibrillator.
*Difference with P<0.001 among the four AF types.
aPrior to, or during qualifying admission/consultation.
bDuring qualifying admission or consultation.
Drug therapy at discharge/end of visit
| First detected (n=960) | Paroxysmal (n=1509) | Persistent (n=1155) | Permanent (n=1515) | P-value | |
|---|---|---|---|---|---|
| Antithrombotic | |||||
| Oral anticoagulation | 495 (53) | 744 (51) | 898 (80) | 1134 (76) | * |
| Aspirin | 340 (36) | 535 (36) | 236 (21) | 379 (25) | * |
| Othera | 145 (16) | 188 (13) | 99 (9) | 169 (11) | * |
| Combination of the above | 157 (17) | 165 (11) | 145 (13) | 225 (15) | * |
| None | 124 (13) | 183 (12) | 46 (4) | 65 (4) | * |
| Antiarrhythmic/rate controlb | |||||
| Type IAc | 4 (0) | 14 (1) | 6 (1) | 1 (0) | |
| Type ICd | 56 (6) | 260 (17) | 151 (13) | 22 (2) | * |
| Type IIe | 278 (29) | 438 (29) | 339 (30) | 443 (30) | |
| Type IIIf | 317 (33) | 551 (37) | 483 (43) | 224 (15) | * |
| Type IVg | 71 (8) | 126 (8) | 89 (8) | 177 (12) | * |
| Digitalish | 159 (17) | 207 (14) | 260 (23) | 743 (50) | * |
| None | 213 (23) | 215 (15) | 128 (11) | 280 (19) | * |
| Other medication | |||||
| ACE-inhibitor | 446 (48) | 660 (45) | 590 (52) | 795 (53) | * |
| AT II antagonist | 105 (11) | 177 (12) | 162 (14) | 205 (14) | |
| Beta-blockeri | 140 (15) | 202 (14) | 160 (14) | 236 (16) | |
| Dihydropyridin calcium channel blocker | 107 (12) | 215 (15) | 151 (13) | 166 (11) | |
| Diuretic | 406 (44) | 570 (39) | 579 (51) | 1043 (70) | * |
| Nitrate | 146 (16) | 256 (17) | 146 (13) | 310 (21) | * |
| Statin | 221 (24) | 414 (28) | 286 (25) | 362 (24) | |
| Diabetic therapy | 137 (15) | 166 (11) | 128 (11) | 252 (17) | * |
| Thyroid therapy | 31 (3) | 94 (6) | 85 (8) | 80 (5) | * |
| First detected (n=960) | Paroxysmal (n=1509) | Persistent (n=1155) | Permanent (n=1515) | P-value | |
|---|---|---|---|---|---|
| Antithrombotic | |||||
| Oral anticoagulation | 495 (53) | 744 (51) | 898 (80) | 1134 (76) | * |
| Aspirin | 340 (36) | 535 (36) | 236 (21) | 379 (25) | * |
| Othera | 145 (16) | 188 (13) | 99 (9) | 169 (11) | * |
| Combination of the above | 157 (17) | 165 (11) | 145 (13) | 225 (15) | * |
| None | 124 (13) | 183 (12) | 46 (4) | 65 (4) | * |
| Antiarrhythmic/rate controlb | |||||
| Type IAc | 4 (0) | 14 (1) | 6 (1) | 1 (0) | |
| Type ICd | 56 (6) | 260 (17) | 151 (13) | 22 (2) | * |
| Type IIe | 278 (29) | 438 (29) | 339 (30) | 443 (30) | |
| Type IIIf | 317 (33) | 551 (37) | 483 (43) | 224 (15) | * |
| Type IVg | 71 (8) | 126 (8) | 89 (8) | 177 (12) | * |
| Digitalish | 159 (17) | 207 (14) | 260 (23) | 743 (50) | * |
| None | 213 (23) | 215 (15) | 128 (11) | 280 (19) | * |
| Other medication | |||||
| ACE-inhibitor | 446 (48) | 660 (45) | 590 (52) | 795 (53) | * |
| AT II antagonist | 105 (11) | 177 (12) | 162 (14) | 205 (14) | |
| Beta-blockeri | 140 (15) | 202 (14) | 160 (14) | 236 (16) | |
| Dihydropyridin calcium channel blocker | 107 (12) | 215 (15) | 151 (13) | 166 (11) | |
| Diuretic | 406 (44) | 570 (39) | 579 (51) | 1043 (70) | * |
| Nitrate | 146 (16) | 256 (17) | 146 (13) | 310 (21) | * |
| Statin | 221 (24) | 414 (28) | 286 (25) | 362 (24) | |
| Diabetic therapy | 137 (15) | 166 (11) | 128 (11) | 252 (17) | * |
| Thyroid therapy | 31 (3) | 94 (6) | 85 (8) | 80 (5) | * |
Data are presented as observed number (%) within type of AF.
*Difference with P<0.001 among the four AF types.
aClopidogrel, ticlopidin, dipyridamole, heparin, or non-specified.
bAntiarrhythmic drugs according to the Vaughan Williams classification (33), if possible.
cBepridil, cibenzoline, disopyramide, procainamide, quinidine.
dFlecainide, propafenone.
eBeta-blocker for antiarrhythmic indication.
fAmiodarone, sotalol.
gDiltiazem, verapamil.
hDigoxin, digitoxin.
iBeta-blocker not for antiarrhythmic indication.
Drug therapy at discharge/end of visit
| First detected (n=960) | Paroxysmal (n=1509) | Persistent (n=1155) | Permanent (n=1515) | P-value | |
|---|---|---|---|---|---|
| Antithrombotic | |||||
| Oral anticoagulation | 495 (53) | 744 (51) | 898 (80) | 1134 (76) | * |
| Aspirin | 340 (36) | 535 (36) | 236 (21) | 379 (25) | * |
| Othera | 145 (16) | 188 (13) | 99 (9) | 169 (11) | * |
| Combination of the above | 157 (17) | 165 (11) | 145 (13) | 225 (15) | * |
| None | 124 (13) | 183 (12) | 46 (4) | 65 (4) | * |
| Antiarrhythmic/rate controlb | |||||
| Type IAc | 4 (0) | 14 (1) | 6 (1) | 1 (0) | |
| Type ICd | 56 (6) | 260 (17) | 151 (13) | 22 (2) | * |
| Type IIe | 278 (29) | 438 (29) | 339 (30) | 443 (30) | |
| Type IIIf | 317 (33) | 551 (37) | 483 (43) | 224 (15) | * |
| Type IVg | 71 (8) | 126 (8) | 89 (8) | 177 (12) | * |
| Digitalish | 159 (17) | 207 (14) | 260 (23) | 743 (50) | * |
| None | 213 (23) | 215 (15) | 128 (11) | 280 (19) | * |
| Other medication | |||||
| ACE-inhibitor | 446 (48) | 660 (45) | 590 (52) | 795 (53) | * |
| AT II antagonist | 105 (11) | 177 (12) | 162 (14) | 205 (14) | |
| Beta-blockeri | 140 (15) | 202 (14) | 160 (14) | 236 (16) | |
| Dihydropyridin calcium channel blocker | 107 (12) | 215 (15) | 151 (13) | 166 (11) | |
| Diuretic | 406 (44) | 570 (39) | 579 (51) | 1043 (70) | * |
| Nitrate | 146 (16) | 256 (17) | 146 (13) | 310 (21) | * |
| Statin | 221 (24) | 414 (28) | 286 (25) | 362 (24) | |
| Diabetic therapy | 137 (15) | 166 (11) | 128 (11) | 252 (17) | * |
| Thyroid therapy | 31 (3) | 94 (6) | 85 (8) | 80 (5) | * |
| First detected (n=960) | Paroxysmal (n=1509) | Persistent (n=1155) | Permanent (n=1515) | P-value | |
|---|---|---|---|---|---|
| Antithrombotic | |||||
| Oral anticoagulation | 495 (53) | 744 (51) | 898 (80) | 1134 (76) | * |
| Aspirin | 340 (36) | 535 (36) | 236 (21) | 379 (25) | * |
| Othera | 145 (16) | 188 (13) | 99 (9) | 169 (11) | * |
| Combination of the above | 157 (17) | 165 (11) | 145 (13) | 225 (15) | * |
| None | 124 (13) | 183 (12) | 46 (4) | 65 (4) | * |
| Antiarrhythmic/rate controlb | |||||
| Type IAc | 4 (0) | 14 (1) | 6 (1) | 1 (0) | |
| Type ICd | 56 (6) | 260 (17) | 151 (13) | 22 (2) | * |
| Type IIe | 278 (29) | 438 (29) | 339 (30) | 443 (30) | |
| Type IIIf | 317 (33) | 551 (37) | 483 (43) | 224 (15) | * |
| Type IVg | 71 (8) | 126 (8) | 89 (8) | 177 (12) | * |
| Digitalish | 159 (17) | 207 (14) | 260 (23) | 743 (50) | * |
| None | 213 (23) | 215 (15) | 128 (11) | 280 (19) | * |
| Other medication | |||||
| ACE-inhibitor | 446 (48) | 660 (45) | 590 (52) | 795 (53) | * |
| AT II antagonist | 105 (11) | 177 (12) | 162 (14) | 205 (14) | |
| Beta-blockeri | 140 (15) | 202 (14) | 160 (14) | 236 (16) | |
| Dihydropyridin calcium channel blocker | 107 (12) | 215 (15) | 151 (13) | 166 (11) | |
| Diuretic | 406 (44) | 570 (39) | 579 (51) | 1043 (70) | * |
| Nitrate | 146 (16) | 256 (17) | 146 (13) | 310 (21) | * |
| Statin | 221 (24) | 414 (28) | 286 (25) | 362 (24) | |
| Diabetic therapy | 137 (15) | 166 (11) | 128 (11) | 252 (17) | * |
| Thyroid therapy | 31 (3) | 94 (6) | 85 (8) | 80 (5) | * |
Data are presented as observed number (%) within type of AF.
*Difference with P<0.001 among the four AF types.
aClopidogrel, ticlopidin, dipyridamole, heparin, or non-specified.
bAntiarrhythmic drugs according to the Vaughan Williams classification (33), if possible.
cBepridil, cibenzoline, disopyramide, procainamide, quinidine.
dFlecainide, propafenone.
eBeta-blocker for antiarrhythmic indication.
fAmiodarone, sotalol.
gDiltiazem, verapamil.
hDigoxin, digitoxin.
iBeta-blocker not for antiarrhythmic indication.
ACC/AHA/ESC stroke risk factors
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Stroke risk factors | |||||
| Age ≥75 years | 255 (26) | 325 (21) | 271 (23) | 591 (38) | * |
| Heart failure or LVEF ≤35% | 291 (30) | 415 (28) | 454 (39) | 796 (52) | * |
| Hypertension | 620 (63) | 942 (62) | 772 (66) | 984 (63) | |
| Mitral stenosis | 34 (4) | 37 (3) | 62 (5) | 188 (13) | * |
| Valve surgery | 27 (3) | 75 (5) | 72 (6) | 172 (11) | * |
| Stroke/TIA | 70 (7) | 143 (10) | 101 (9) | 228 (15) | * |
| Age 60–74 years, and diabetes or CAD | 212 (22) | 292 (19) | 230 (20) | 334 (22) | |
| At least one of the above | 808 (83) | 1200 (79) | 1010 (87) | 1447 (94) | * |
| Contraindications | |||||
| Major bleeding | 7 (1) | 26 (2) | 23 (2) | 54 (4) | * |
| Malignancy | 49 (5) | 73 (5) | 54 (5) | 97 (6) | |
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Stroke risk factors | |||||
| Age ≥75 years | 255 (26) | 325 (21) | 271 (23) | 591 (38) | * |
| Heart failure or LVEF ≤35% | 291 (30) | 415 (28) | 454 (39) | 796 (52) | * |
| Hypertension | 620 (63) | 942 (62) | 772 (66) | 984 (63) | |
| Mitral stenosis | 34 (4) | 37 (3) | 62 (5) | 188 (13) | * |
| Valve surgery | 27 (3) | 75 (5) | 72 (6) | 172 (11) | * |
| Stroke/TIA | 70 (7) | 143 (10) | 101 (9) | 228 (15) | * |
| Age 60–74 years, and diabetes or CAD | 212 (22) | 292 (19) | 230 (20) | 334 (22) | |
| At least one of the above | 808 (83) | 1200 (79) | 1010 (87) | 1447 (94) | * |
| Contraindications | |||||
| Major bleeding | 7 (1) | 26 (2) | 23 (2) | 54 (4) | * |
| Malignancy | 49 (5) | 73 (5) | 54 (5) | 97 (6) | |
Data are presented as observed number (%) within type of AF.
LVEF, left ventricular ejection fraction; TIA, transient ischaemic attack; CAD, coronary artery disease; TEE, transesophageal echocardiography.
*Difference with P<0.001 among the four AF types.
ACC/AHA/ESC stroke risk factors
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Stroke risk factors | |||||
| Age ≥75 years | 255 (26) | 325 (21) | 271 (23) | 591 (38) | * |
| Heart failure or LVEF ≤35% | 291 (30) | 415 (28) | 454 (39) | 796 (52) | * |
| Hypertension | 620 (63) | 942 (62) | 772 (66) | 984 (63) | |
| Mitral stenosis | 34 (4) | 37 (3) | 62 (5) | 188 (13) | * |
| Valve surgery | 27 (3) | 75 (5) | 72 (6) | 172 (11) | * |
| Stroke/TIA | 70 (7) | 143 (10) | 101 (9) | 228 (15) | * |
| Age 60–74 years, and diabetes or CAD | 212 (22) | 292 (19) | 230 (20) | 334 (22) | |
| At least one of the above | 808 (83) | 1200 (79) | 1010 (87) | 1447 (94) | * |
| Contraindications | |||||
| Major bleeding | 7 (1) | 26 (2) | 23 (2) | 54 (4) | * |
| Malignancy | 49 (5) | 73 (5) | 54 (5) | 97 (6) | |
| First detected (n=978) | Paroxysmal (n=1517) | Persistent (n=1167) | Permanent (n=1541) | P-value | |
|---|---|---|---|---|---|
| Stroke risk factors | |||||
| Age ≥75 years | 255 (26) | 325 (21) | 271 (23) | 591 (38) | * |
| Heart failure or LVEF ≤35% | 291 (30) | 415 (28) | 454 (39) | 796 (52) | * |
| Hypertension | 620 (63) | 942 (62) | 772 (66) | 984 (63) | |
| Mitral stenosis | 34 (4) | 37 (3) | 62 (5) | 188 (13) | * |
| Valve surgery | 27 (3) | 75 (5) | 72 (6) | 172 (11) | * |
| Stroke/TIA | 70 (7) | 143 (10) | 101 (9) | 228 (15) | * |
| Age 60–74 years, and diabetes or CAD | 212 (22) | 292 (19) | 230 (20) | 334 (22) | |
| At least one of the above | 808 (83) | 1200 (79) | 1010 (87) | 1447 (94) | * |
| Contraindications | |||||
| Major bleeding | 7 (1) | 26 (2) | 23 (2) | 54 (4) | * |
| Malignancy | 49 (5) | 73 (5) | 54 (5) | 97 (6) | |
Data are presented as observed number (%) within type of AF.
LVEF, left ventricular ejection fraction; TIA, transient ischaemic attack; CAD, coronary artery disease; TEE, transesophageal echocardiography.
*Difference with P<0.001 among the four AF types.
References
Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates.
Vidaillet H, Granada JF, Chyou PH, Maassen K, Ortiz M, Pulido JN, Sharma P, Smith PN, Hayes J. A population-based study of mortality among patients with atrial fibrillation or flutter.
Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: epidemiology, pathophysiology, and rationale for therapy.
Wolf PA, Dawber TR, Thomas HE Jr, Kannel WB. Epidemiologic assessment of chronic atrial fibrillation and risk of stroke: the Framingham study.
Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: a major contributor to stroke in the elderly. The Framingham Study.
Wang TJ, Larson MG, Levy D, Vasan RS, Leip EP, Wolf PA, D'Agostino RB, Murabito JM, Kannel WB, Benjamin EJ. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study.
Stewart S, Murphy N, Walker A, McGuire A, McMurray JJ. Cost of an emerging epidemic: an economic analysis of atrial fibrillation in the UK.
Wattigney WA, Mensah GA, Croft JB. Increasing trends in hospitalization for atrial fibrillation in the United States, 1985 through 1999: implications for primary prevention.
Le Heuzey JY, Paziaud O, Piot O, Said MA, Copie X, Lavergne T, Guize L. Cost of care distribution in atrial fibrillation patients: the COCAF study.
Van Gelder IC, Hagens VE, Bosker HA, Kingma JH, Kamp O, Kingma T, Said SA, Darmanata JI, Timmermans AJ, Tijssen JG, Crijens HJ. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation.
Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, Kellen JC, Greene HL, Mickel MC, Dalquist JE, Corley SD. A comparison of rate control and rhythm control in patients with atrial fibrillation.
Opolski G, Torbicki A, Kosior DA, Szulc M, Wozakowska-Kaplon B, Kolodziej P, Achremczyk P. Rate control vs rhythm control in patients with nonvalvular persistent atrial fibrillation: the results of the Polish How to Treat Chronic Atrial Fibrillation (HOT CAFE) Study.
Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation—pharmacological intervention in atrial fibrillation (PIAF): a randomised trial.
Carlsson J, Miketic S, Windeler J, Cuneo A, Haun S, Micus S, Walter S, Tebbe U. Randomized trial of rate-control versus rhythm-control in persistent atrial fibrillation: the strategies of treatment of atrial fibrillation (STAF) study.
de Denus S, Sanoski CA, Carlsson J, Opolski G, Spinler SA. Rate vs rhythm control in patients with atrial fibrillation: a meta-analysis.
Saxena R, Koudstaal PJ. Anticoagulants versus antiplatelet therapy for preventing stroke in patients with nonrheumatic atrial fibrillation and a history of stroke or transient ischemic attack. The Cochrane Database of Systematic Reviews
Segal JB, McNamara RL, Miller MR, Powe NR, Goodman SN, Robinson KA, Bass EB. Anticoagulants or antiplatelet therapy for non-rheumatic atrial fibrillation and flutter. The Cochrane Database of Systematic Reviews
Benavente O, Hart R, Koudstaal P, Laupacis A, McBride R. Antiplatelet therapy for preventing stroke in patients with non-valvular atrial fibrillation and no previous history of stroke or transient ischemic attacks. The Cochrane Database of Systematic Reviews
Fuster V, Ryden LE, Asinger RW, Cannom DS, Crijns HJ, Frye RL, Halperin JL, Kay GN, Klein WW, Levy S, McNamara RL, Prystowsky EN, Wann LS, Wyse DG. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to develop guidelines for the management of patients with atrial fibrillation) developed in collaboration with the North American Society of Pacing and Electrophysiology.
Friberg J, Scharling H, Gadsboll N, Jensen GB. Sex-specific increase in the prevalence of atrial fibrillation (The Copenhagen City Heart Study).
Goudevenos JA, Vakalis JN, Giogiakas V, Lathridou P, Katsouras C, Michalis LK, Sideris DA. An epidemiological study of symptomatic paroxysmal atrial fibrillation in northwest Greece.
Kerr CR, Boone J, Connolly SJ, Dorian P, Green M, Klein G, Newman D, Sheldon R, Talajic M. The Canadian Registry of Atrial Fibrillation: a noninterventional follow-up of patients after the first diagnosis of atrial fibrillation.
Krahn AD, Manfreda J, Tate RB, Mathewson FA, Cuddy TE. The natural history of atrial fibrillation: incidence, risk factors, and prognosis in the Manitoba Follow-Up Study.
Stewart S, Hart CL, Hole DJ, McMurray JJ. Population prevalence, incidence, and predictors of atrial fibrillation in the Renfrew/Paisley study.
Wandell PE. A survey of subjects with present or previous atrial fibrillation in a Swedish community.
Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study.
Levy S, Maarek M, Coumel P, Guize L, Lekieffre J, Medvedowsky JL, Sebaoun A. Characterization of different subsets of atrial fibrillation in general practice in France: the ALFA study. The College of French Cardiologists.
Lip GY, Golding DJ, Nazir M, Beevers DG, Child DL, Fletcher RI. A survey of atrial fibrillation in general practice: the West Birmingham Atrial Fibrillation Project.
Majeed A, Moser K, Carroll K. Trends in the prevalence and management of atrial fibrillation in general practice in England and Wales, 1994–1998: analysis of data from the general practice research database.
Carlsson J, Tebbe U, Rox J, Harmjanz D, Haerten K, Neuhaus KL, Seidel F, Niederer W, Miketic S. Cardioversion of atrial fibrillation in the elderly. ALKK-Study Group. Arbeitsgemeinschaft Leitender Kardiologischer Krankenhausaerzte.
Santini M, De Ferrari GM, Pandozi C, Alboni P, Capucci A, Disertori M, Gaita F, Lombardi F, Maggioni AP, Mugelli A, Salerno-Uriarte JA, Sermasi S, Schwartz PJ. Atrial fibrillation requiring urgent medical care: approach and outcome in the various departments of admission. Data from the atrial Fibrillation/flutter Italian REgistry (FIRE).
Frykman V, Beerman B, Ryden L, Rosenqvist M. Management of atrial fibrillation: discrepancy between guideline recommendations and actual practice exposes patients to risk for complications.
Statistics by Country for Atrial Fibrillation. http://www.wrongdiagnosis.com/a/atrial_fibrillation/stats-country.htm (24 May
Vaughan Williams EM. A classification of antiarrhythmic actions reassessed after a decade of new drugs.
Laguna P, Martn A, del Arco C, Gargantilla P. Risk factors for stroke and thromboprophylaxis in atrial fibrillation: what happens in daily clinical practice? The GEFAUR-1 study.
Ang SY, Peterson GM, Friesen WT, Vial JH. Review of antithrombotic drug usage in atrial fibrillation.
Albers GW, Yim JM, Belew KM, Bittar N, Hattemer CR, Phillips BG, Kemp S, Hall EA, Morton DJ, Vlasses PH. Status of antithrombotic therapy for patients with atrial fibrillation in university hospitals.
Adhiyaman V, Kamalakannan D, Oke A, Shah IU, White AD. Underutilization of antithrombotic therapy in atrial fibrillation.
Anderson DR, Gardner MJ, Putnam W, Jassal D, Brownell B, Flowerdew G, Nagpal S, Thompson K, Cox JL. Population-based evaluation of the management of antithrombotic therapy for atrial fibrillation.
Jackson SL, Peterson GM, Vial JH, Daud R, Ang SY. Outcomes in the management of atrial fibrillation: clinical trial results can apply in practice.
Kalra L, Yu G, Perez I, Lakhani A, Donaldson N. Prospective cohort study to determine if trial efficacy of anticoagulation for stroke prevention in atrial fibrillation translates into clinical effectiveness.
Furberg CD, Psaty BM, Manolio TA, Gardin JM, Smith VE, Rautaharju PM. Prevalence of atrial fibrillation in elderly subjects (the Cardiovascular Health Study).
Brand FN, Abbott RD, Kannel WB, Wolf PA. Characteristics and prognosis of lone atrial fibrillation: 30-year follow-up in the Framingham Study.
Kopecky SL, Gersh BJ, McGoon MD, Whisnant JP, Holmes DR Jr, Ilstrup DM, Frye RL. The natural history of lone atrial fibrillation: a population-based study over three decades.
Wijffels MC, Kirchhof CJ, Dorland R, Allessie MA. Atrial fibrillation begets atrial fibrillation: a study in awake chronically instrumented goats.
Frost L, Johnsen SP, Pedersen L, Toft E, Husted S, Sorensen HT. Atrial fibrillation or flutter and stroke: a Danish population-based study of the effectiveness of oral anticoagulation in clinical practice.
Gage BF, Boechler M, Doggette AL, Fortune G, Flaker GC, Rich MW, Radford MJ. Adverse outcomes and predictors of underuse of antithrombotic therapy in medicare beneficiaries with chronic atrial fibrillation.
Go AS, Hylek EM, Borowsky LH, Phillips KA, Selby JV, Singer DE. Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: the anticoagulation and risk factors in atrial fibrillation (ATRIA) study.
Perez I, Melbourn A, Kalra L. Use of antithrombotic measures for stroke prevention in atrial fibrillation.
Scott PA, Pancioli AM, Davis LA, Frederiksen SM, Eckman J. Prevalence of atrial fibrillation and antithrombotic prophylaxis in emergency department patients.
Weisbord SD, Whittle J, Brooks RC. Is warfarin really underused in patients with atrial fibrillation?
Bravata DM, Rosenbeck K, Kancir S, Brass LM. The use of warfarin in veterans with atrial fibrillation.
Whittle J, Wickenheiser L, Venditti LN. Is warfarin underused in the treatment of elderly persons with atrial fibrillation?


{kind=link}
{kind=link}
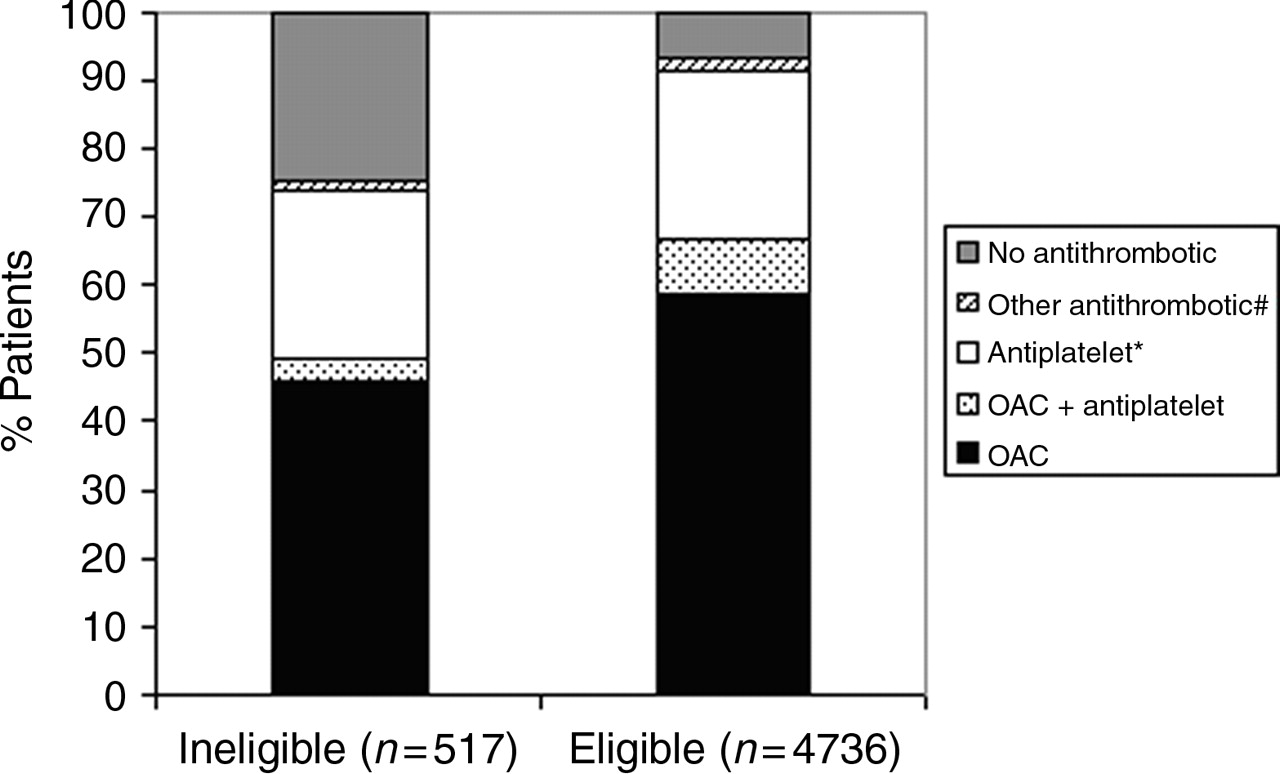{kind=link}
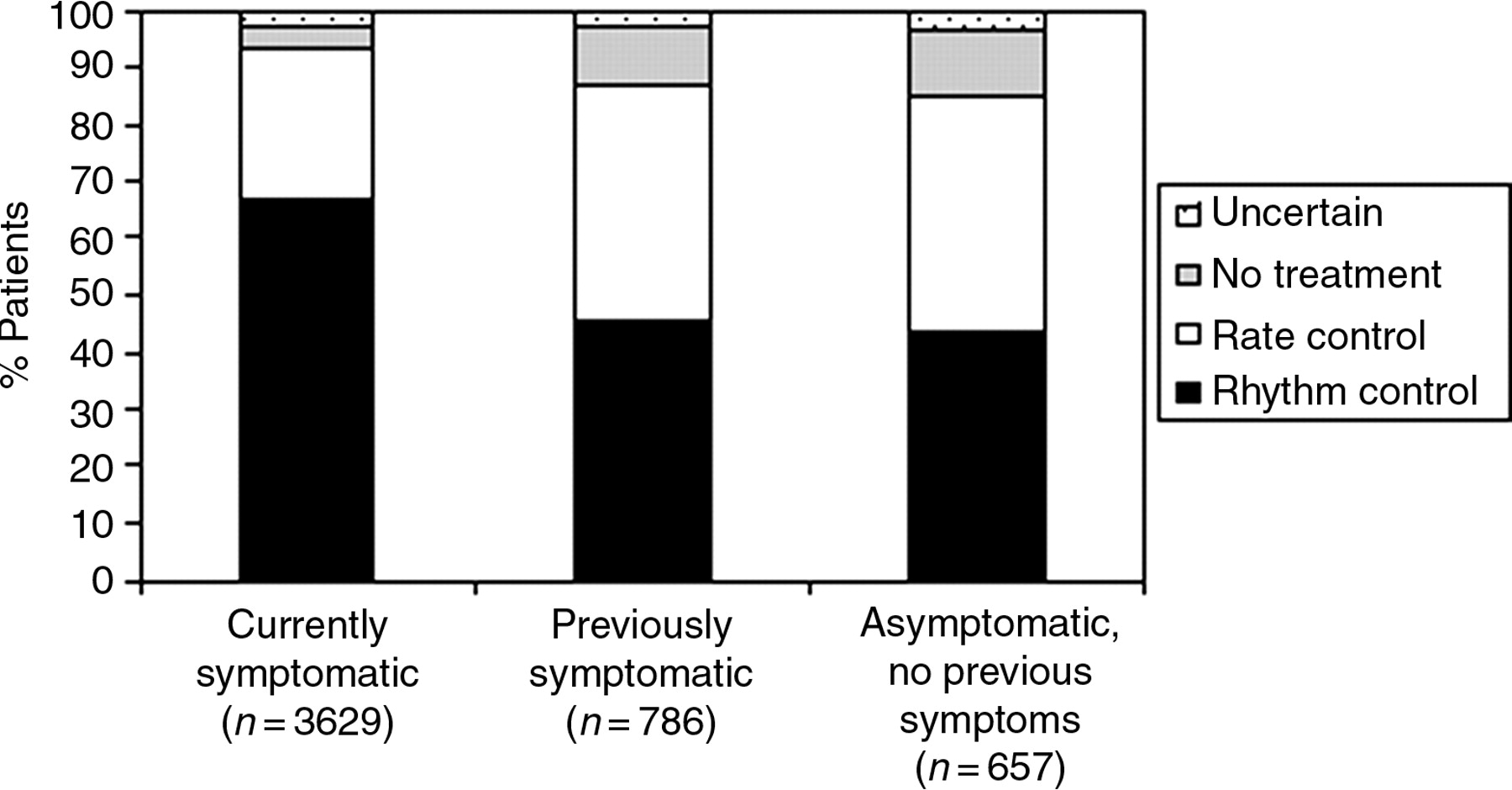{kind=link}