
Abstract
OBJECTIVE: Recent reports have linked calcium channel blockers (CCBs) with an increased risk of acute myocardial infarction (AMI). We sought to determine to what extent physicians relinquished CCBs following these adverse reports and if there were differences in the use of CCBs and other AMI therapies across 3 levels of specialist involvement: generalist attendings, collaborative care (generalist with cardiologist consultation), and cardiologist attendings.
DESIGN: We measured use of CCBs during hospitalization for AMI before (1992–1993) and after (1995–1996) the adverse CCB reports, controlling for hospital-, physician-, and patient-level variables. We also examined use of effective medications (aspirin, β-blockers, thrombolytic therapy) and ineffective AMI treatments (lidocaine).
SETTING: Thirty-seven community-based hospitals in Minnesota.
PATIENTS: Population-based sample of 5,347 patients admitted with AMI.
MEASUREMENTS: The primary outcome was prescription of a CCB at the time of discharge from hospital. Secondary outcomes included use of other effective and ineffective AMI therapies during hospitalization and at discharge.
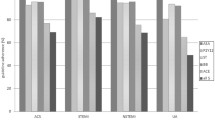
MAIN RESULTS: Compared with cardiologists, generalist attendings were less likely to use aspirin (37% vs 68%; adjusted odds ratio [OR], 0.58; 95% confidence interval [95% CI], 0.42 to 0.80) and thrombolytics (29% vs 64%; adjusted OR, 0.18; 95% CI, 0.13 to 0.25), but not β-blockers (20% vs 46%; adjusted OR, 0.93; 95% CI, 0.66 to 1.31). From 1992-1993 to 1995-1996, the use of CCBs in patients with AMI decreased from 24% to 10%, the net result of physicians starting CCBs less often and discontinuing them more often. In multivariate models, the odds of CCB relinquishment after the adverse reports (adjusted OR, 0.33; 95% CI, 0.27 to 0.39) were independent of, and not modified by, the involvement of a cardiologist.
CONCLUSIONS: Compared with cardiologists, generalist physicians were less likely to adopt some effective AMI therapies, particularly those associated with risk such as thrombolytic therapy. However, generalists were as likely as cardiologists to relinquish CCBs after the adverse reports. This pattern of practice may be the generalist physicians’ response to an expanding, but increasingly risky and uncertain, pharmacopoeia.
Similar content being viewed by others


References
Donohoe MT. Comparing generalist and specialist care: discrepancies, deficiencies, and excesses. Arch Intern Med. 1998;58:1596–608.
Turner BJ, McKee L, Fanning T, Markson LE. AIDS specialist versus generalist ambulatory care for advanced HIV infection and impact on hospital use. Med Care. 1994;32:902–16.
Markson LE, Cosler LE, Turner BJ. Implications of generalists’ slow adoption of zidovudine in clinical practice. Arch Intern Med. 1994;154:1497–504.
Hirth RA, Fendrick AM, Chernew ME. Specialist and generalist physicians’ adoption of antibiotic therapy to eradicate Helicobacter pylori infection. Med Care. 1996;34:1199–204.
Thamer M, Ray NF, Henderson SC, Rinehart CS, Sherman CR, Ferguson JH. Influence of the NIH Consensus Conference on Helicobacter pylori on physician prescribing among a Medicaid Population. Med Care. 1998;36:646–60.
Ayanian JZ, Hauptman PJ, Guadagnoli E, Artman EM, Pashos CL, McNeil BJ. Knowledge and practices of generalist and specialist physicians regarding drug therapy for acute myocardial infarction. N Engl J Med. 1994;331:1136–42.
Ayanian JZ, Guadagnoli E, McNeil BJ, Cleary PD. Treatment and outcomes of acute myocardial infarction among patients of cardiologists and generalist physicians. Arch Intern Med. 1997;157:2570–6.
Jollis JG, DeLong ER, Peterson ED, et al. Outcome of acute myocardial infarction according to the specialty of the admitting physician. N Engl J Med. 1996;335:1880–7.
Willison DJ, Soumerai SB, McLaughlin TJ, et al. Consultation between cardiologists and generalists in the management of acute myocardial infarction: implications for quality of care. Arch Intern Med. 1998;158:1778–83.
Nash IS, Corrato RR, Dlutowski MJ, O’Connor JP, Nash DB. Generalist versus specialist care for acute myocardial infarction. Am J Cardiol. 1999;83:650–4.
Schreiber TL, Elkhatib A, Grines CL, O’Neill WW. Cardiologist versus internist management of patients with unstable angina: treatment patterns and outcomes. J Am Coll Cardiol. 1995;26:577–82.
Goldman L. The value of cardiology. N Engl J Med. 1996;355:1918–9.
Mitchell JR. But will it help my patients with myocardial infarction? The implications of recent trials for everyday country folk. Br Med J (Clin Res Ed). 1982;285:1140–8.
Greer AL. The state of the art versus the state of the science. The diffusion of new medical technologies into practice. Int J Technol Assess Health Care. 1988;4:5–26.
Dixon AS. The evolution of clinical policies. Med Care. 1990;28:201–20.
Miao LL. Gastric freezing: an example of the evaluation of medical therapy by randomized clinical trials. In: Bunker JP, Barnes BA, Mosteller F, eds. Costs, Risks, and Benefits of Surgery. New York: Oxford University Press; 1977:198–211.
Eisenberg JM. Doctors’ Decisions and the Cost of Medical Care. Ann Arbor, Mich: Health Administration Press Perspectives; 1986.
Soumerai SB, Majumdar SR, Lipton HL. Evaluating and improving physician prescribing. In: Pharmacoepidemiology. 3rd ed. Strom BL, ed. Chichester: John Wiley and Sons; 1999.
Tanenbaum SJ. What physicians know. N Engl J Med. 1993;329:1268–71.
Davis P, Gribben B. Rational prescribing and interpractitioner variation. A multilevel approach. Int J Technol Assess Health Care. 1995;11:428–42.
Wennberg JE. Dealing with medical practice variations: a proposal for action. Health Aff (Millwood). 1984;3:6–32.
Avorn J, Chen M, Hartley R. Scientific versus commercial sources of influence on the prescribing behavior of physicians. Am J Med. 1982;73:4–8.
Schwartz RK, Soumerai SB, Avorn J. Physician motivations for nonscientific drug prescribing. Soc Sci Med. 1989;28:577–82.
Manolio TA, Cutler JA, Furberg CD, Psaty BM, Whelton PK, Applegate WB. Trends in pharmacologic management of hypertension in the United States. Arch Intern Med. 1995;155: 829–37.
Mapes RE. Physicians’ drug innovation and relinquishment. Soc Sci Med. 1977;11:619–24.
Eddy DM. Practice policies: where do they come from? JAMA. 1990;263:1265–75.
Leape LL. Unnecessary surgery. Annu Rev Publ Health. 1992;13:363–83.
Duffy SQ, Farley DE. The protracted demise of medical technology. The case of intermittent positive pressure breathing. Med Care. 1992;30:718–36.
Rogers EM. Diffusion of Innovations. 4th ed. New York: The Free Press; 1995.
Hennekens CH, Albert CM, Godfried SL, Gaziano JM, Buring JE. Adjunctive drug therapy of acute myocardial infarction—evidence from clinical trials. N Engl J Med. 1996;335:1660–7.
Yusuf S. Calcium antagonists in coronary artery disease and hypertension. Time for a reevaluation? Circulation. 1995;92:1079–82.
Rogers WJ, Bowlby LJ, Chandra NC, et al. Treatment of myocardial infarction in the United States (1990 to 1993). Observations from the National Registry of Myocardial Infarction. Circulation. 1994;90:2103–14.
McCormick D, Gurwitz JH, Savageau J, Yarzebski J, Gore JM, Goldberg RJ. Differences in discharge medication after acute myocardial infarction in patients with HMO and fee-for service medical insurance. J Gen Intern Med. 1999;14:73–81.
Psaty BM, Heckbert SR, Koepsell TD, et al. The risk of incident myocardial infarction associated with antihypertensive drug therapies. Circulation. 1995;91:925 Abstract.
Psaty BM, Heckbert SR, Koepsell TD, et al. The risk of myocardial infarction associated with antihypertensive drug therapies. JAMA. 1995;274:620–5.
Furberg CD, Psaty BM, Meyer JV. Nifedipine. Dose-related increase in mortality in patients with coronary heart disease. Circulation. 1995;92:1326–31.
Parmley WW. Sensationalism and the news media. J Am Coll Card. 1995;26:836–7.
Buring JE, Glynn RJ, Hennekens CH. Calcium channel blockers and myocardial infarction. A hypothesis formulated but not yet tested. JAMA. 1995;274:654–5.
Opie LH, Messerli FH. Nifedipine and mortality. Grave defects in the dossier. Circulation. 1995;92:1068–73.
Maclure M, Dormuth C, Naumann T, et al. Influences of educational interventions and adverse news about calcium-channel blockers on first-line prescribing of antihypertensive drugs to elderly people in British Columbia. Lancet. 1998;352:943–8.
Brunt M, Murray MD, Kesterson J, Tierney WM. Does media coverage of medical research influence prescribing? J Gen Intern Med. 1999;14(suppl. 2):89 abstract.
Soumerai SB, McLaughlin TJ, Gurwitz JH, et al. Effect of local opinion leaders on quality of care for acute myocardial infarction: a randomized controlled trial. JAMA. 1998;279:1358–63.
Greenfield S, Apolone G, McNeil BJ, Cleary PD. The importance of co-existent disease in the occurrence of postoperative complications and one-year recovery in patients undergoing total hip replacement. Med Care. 1993;31:141–54.
McLaughlin TJ, Soumerai SB, Willison DJ, et al. The effect of comorbidity on use of thrombolysis or aspirin in patients with acute myocardial infarction eligible for treatment. J Gen Intern Med. 1997;12:1–6.
Allison JJ, Kiefe CI, Cook EF, Gerrity MS, Orav EJ, Centor R. The association of physician attitudes about uncertainty and risk-taking with resource use in a Medicare HMO. Med Decis Making. 1998;18:320–9.
Diggle PJ, Liang KY, Zeger SL. Analysis of Longitudinal Data. New York: Oxford University Press; 1996.
Divine GW, Brown JT, Frazier LM. The unit of analysis error in studies about physicians’ patient care behavior. J Gen Intern Med. 1992;7:623–9.
Hershey JC, Baron J. Clinical reasoning and cognitive processes. Med Decis Making. 1987;7:203–11.
Yates JF. Judgement and Decision Making. Englewood Cliffs, NJ: Prentice Hall; 1990.
Feinstein AR. The “chagrin factor” and qualitative decision analysis. Arch Intern Med. 1985;145:1257–9.
Ayanian JZ, Berwick DM. Do physicians have a bias towards action? A classic study revisited. Med Decis Making. 1991;11:154–8.
MacMahon S, Collins R, Peto R, Koster RW, Yusuf S. Effects of prophylactic lidocaine in suspected acute myocardial infarction. An overview of results from randomized controlled trials. JAMA. 1988;260:1910–6.
Echt DS, Liebson PR, Mitchell LB, et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N Engl J Med. 1991;324:781–8.
ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group. ISIS-4: a randomized factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. Lancet. 1995;345:669–75.
Author information
Authors and Affiliations
Additional information
This work was supported by grants from The Agency for Health Care Policy and Research (HSO7357), The National Institute on Aging (AG14474), The Health Care Education and Research Foundation, and The Harvard Pilgrim Health Care Foundation. Dr. Majumdar was the recipient of a National Research Service Award (PE 11001-10).
Rights and permissions
About this article
Cite this article
Majumdar, S.R., Inui, T.S., Gurwitz, J.H. et al. Influence of physician specialty on adoption and relinquishment of calcium channel blockers and other treatments for myocardial infarction. J GEN INTERN MED 16, 351–359 (2001). https://doi.org/10.1046/j.1525-1497.2001.016006351.x
Issue Date:
DOI: https://doi.org/10.1046/j.1525-1497.2001.016006351.x