
Abstract
Study design:
Cross sectional survey.
Objective:
To examine the nature and prevalence of common mental disorders among informal carers of people with Spinal Cord Injury (SCI) and the association with their leisure satisfaction.
Setting:
Christian Medical College, Vellore, Tamilnadu, India.
Methods:
A cross-sectional survey of informal carers of people SCI at the Department of Physical Medicine and Rehabilitation. Fifty-three informal carers of people with SCI were interviewed using the Revised Clinical Interview Schedule to assess psychiatric morbidity, and using the Leisure Satisfaction Scale to measure leisure and contentment. Data on carers with psychiatric morbidity were compared to those without common mental disorders using univariate and multivariate statistics.
Results:
Study reported a high morbidity (53%), with most consistent diagnoses of depression and anxiety. Carers who were spouses, women, currently married and those with lower education had greater psychiatric morbidity and lesser leisure satisfaction, even after adjusting for age and education using logistic/linear regression. Age, occupation, residence, socioeconomic status, type and duration of SCI were not associated with either morbidity or leisure satisfaction.
Conclusion:
Many carers of people with SCI suffer from psychiatric morbidity and also have low scores on leisure satisfaction.
Similar content being viewed by others

Introduction
Living with spinal cord injury (SCI), a devastating condition, requires substantial coping by patients and their carers.1, 2 The adjustment process can result in a significant psychological burden.3, 4
Leisure as an important mechanism of coping with stress5, 6 has been discussed in the literature. Studies have documented that reduction or abandonment of leisure can lead to increased psychological distress.7 In addition to the problems of coping with the consequences of paralysis of their relatives, carers of people with SCI often abandon or severely alter social and leisure aspects of their life.7, 8 However, the distinction between work and leisure are culture bound suggesting the need to examine specific issues in different cultural groups.9
Research from the West has demonstrated that men with SCI rely predominantly on their spouses for social support10 and that the spouses have significant psychological distress and social isolation.11, 12, 13, 14 Studies have recorded the disruption of sex life, wheelchair restrictions, personality change in the person with SCI and problems with bladder care were considered reasons for distress in carers.11
Methods
A cross-sectional survey was conducted of primary carers of patients with SCI admitted to the Department of Physical Medicine and Rehabilitation, Christian Medical College, Vellore, India.
Primary carers of patients with SCI, living with the patient and aged between 18 and 65 years were recruited for the study. Primary carers were defined as those relatives who provided physical care for people with SCI. Carers of patients with head injury or severe psychiatric morbidity and carers with severe cognitive difficulties and communication problems were excluded.
The following instruments were used for assessment:
Leisure Satisfaction Scale (LSS)
The Leisure Satisfaction Scale is a standard instrument to assess leisure satisfaction.15 The scale elicits information on leisure activities and provides a measure of satisfaction. The shortened version of the scale was employed in this study.16 It consists of six components or areas of need satisfaction: psychological, educational, social, relaxational, physiological and aesthetic. Each area is assessed using four statements. The answers to each statement are scored on a 5-point Likert scale. The scale was used to assess the leisure satisfaction for leisure activities chosen by the respondents. The scale has been used in the West and has been shown to have good validity and reliability.16 The scale is also employed in the institution and is useful in assessing leisure satisfaction among patients and their relatives. The general format of the statements, the scoring using a Likert scale and its application to the respondent's leisure activities makes it ideal to assess activities across different groups of people and across cultures.
The Revised Clinical Interview Schedule (CIS-R)
The Revised Clinical interview Schedule (CIS-R) is a standardized semi-structured interview to assess for common mental disorders and other non-psychotic morbidity.17 The instrument has 14 sub-sections: somatic symptoms, fatigue, concentration, sleep problems, irritability, worry about physical health, depression, depressive ideas, worry, anxiety, phobia, panic, obsessions and compulsions. Scores for sub-sections range from 0 to 4. The ratings obtained at interview provide a score for each section, which together can be summed to yield an overall score. Previous studies have shown that subjects with scores of 12 and above have common mental disorders. The schedule does not require the interviewer's clinical judgement thus minimizing observer bias. Most aspects of the interviewing style are prescribed by the interview, including the exact wording of the questions and specific rules for coding each symptom.17 The CIS-R has been shown to have high inter-rater reliability. It takes 10–20 min to administer. Algorithms have been developed to arrive at a International Classification of Diseases-10 Primary Care (ICD-10 PC)18 diagnoses. This instrument has been translated into many Indian languages and used in ethnic Indian populations.19, 20
In addition, information about socio-demographic characteristics of the carer was collected using a specially designed proforma. This information included the following: age, gender, marital status, occupation, economic status, education, place of residence and relationship to patient and clinical details of SCI.
Carers of consecutive individuals with SCI attending in-patient treatment services who satisfied the study criteria were contacted and the study was explained. Informed consent was obtained. The instruments to assess psychiatric morbidity, leisure satisfaction and socio-demographic variables were administered. The carers were interviewed alone in the hospital by the primary investigator (JTR). The average duration of the interview was 1 h.
Mean and standard deviation were used to describe continuous variables, and frequency distributions were obtained for categorical data. The χ2-test was used to assess the significance of associations for categorical variables. Student's t-test was used to test the associations for continuous data. Pearson's correlation coefficient was used to assess association among continuous variables. Linear and logistic regressions analysis were also done. The statistical software SPSS for Windows (Release 11, 0.1) was employed for the analysis.
Results
Sixty carers were contacted. Six carers did not meet inclusion for the following reasons: two were aged below 18 years and four carers were not staying with the patient. Only one carer who was eligible to participate in the study refused consent. There was no significant difference between subjects who took part in the study and those who did not on socio-demographic variables.
Table 1 shows the socio-demographic of carers and clinical profiles of patients. The psychiatric morbidity documented among carers was high (28; 53%). The common ICD-10 diagnoses were depression and mixed anxiety depression.
The factors associated with psychiatric morbidity are documented in Table 2. Carers who were spouses, women, currently married and those with lower education had greater psychiatric morbidity. These associations remained statistically significant even after adjusting for age and education using logistic regression. Age, occupation, residence, socioeconomic status, type and duration of SCI were not associated with morbidity.
Carers who were spouses (t=−2.2; df=34.0; P<0.05), women (t=−4.4; df=51; P<0.001), those currently married (t=−4.0; df=51; P<0.001) and those with lower education (t=6.3; df=50.4; P<0.001) had significantly lower scores on the leisure satisfaction scale on univariate analysis. These variables remained significantly associated with lower leisure scores when age and education were adjusted for using linear regression (spouses P<0.03; women P<0.02; currently married P<0.01; low education P<0.001). Age, occupation, residence, socio-economic status, type and duration of SCI were not significantly associated with leisure scores.
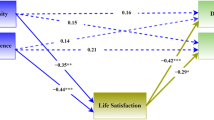
The CIS-R score significantly correlated with the leisure satisfaction scale score with lower scores among those with higher morbidity score (Pearson's correlation coefficient=−0.894; P=0.000). This remained significant after adjusting for age and education using linear regression (B=−0.36; SE of B=0.03; β=−0.86; t=−10.77; P=0.000). CIS-R scores were also found to be significantly associated with all subscales of the leisure satisfaction scale aesthetic (P=0.003); educational (P=0.000); physiological (P=0.003); psychological (P=0.000); relaxational (P=0.000) and social (P=0.000).
Discussion
This study examined the psychiatric morbidity and leisure satisfaction among carers of patients admitted to a tertiary referral center and found that a substantial proportion of carers do suffer from distress, depression and anxiety. Studies from the West have reported similar conclusions.1, 2, 3, 4, 21 The risk factors for psychiatric morbidity among carers of patients with SCI were similar to those seen among patients attending primary care. Female gender and low education were significantly related to depression and anxiety.22, 23 Being a spouse was also an important risk factor for psychiatric morbidity among carers of people with SCI.
The risk factors for poor leisure satisfaction were similar to those found for psychiatric morbidity. Other studies have also reported that household work, and child care, and family responsibilities among women who are carers often force them to abandon or severely restrict social and leisure aspects of their life.24 This study found an association between depression and anxiety and poor leisure satisfaction. However, the cross-sectional design precludes a conclusion on directionality.
This study has shown a significant relationship between the leisure satisfaction and psychiatric morbidity among carers of people with SCI. The findings suggest the need to routinely screen for psychiatric morbidity and poor leisure satisfaction among carers of people with SCI.
References
Killen JM . Role stabilization in families after spinal cord injury. Rehabil Nurs 1990; 15: 19–21.
Sullivan J . Individual and family responses to acute spinal cord injury. Crit Care Nurs Clin North Am 1990; 2: 407–414.
Strambrook M et al. Social role functioning following spinal cord injury. Paraplegia 1991; 29: 318–323.
Rintala DH, Young ME, Spencer JC, Bates PS . Family relationships and adaptation to spinal cord injury: a qualitative study. Rehabil Nurs 1996; 21: 67–74.
Trombly CA, Radomski MV . Restoring competence in leisure pursuits. In: Trombly CA (ed). Occupational Therapy for Physical Dysfunction, 5th edn. Baltimore: Williams and Wilkins 2002, pp 745–759.
Tinsley HEA, Kass RA . Leisure activities and need satisfaction: a replication and extension. J Leisure Res 1978; 10: 191–202.
Bedini LA, Phoenix TL . Addressing leisure barriers for caregivers of older adults: a model leisure wellness program. Therapeutic Recreation J 1999; 33: 222–240.
Rogers NB . Leisure and caregivers. Therapeutic Recreation J 1997; 31: 230–243.
Primeau LA . Work and leisure: transcending the dichotomy. Am J Occup Ther 1996; 50: 569–577.
Decker SD, Schultz R, Wood D . Determinants of well-being in primary caregivers of spinal cord injured persons. Rehabil Nurs 1989; 14: 6–8.
Delargy M, Parry H, Burt A . Quadriplegic care: an assessment of the impact of the carer. Int Disabil Stud 1988; 10: 145–147.
Hammell KW . Psychosocial outcome following spinal cord injury. Paraplegia 1994; 32: 771–779.
Kester BL, Rothblum ED, Lobato D, Milhaus RL . Spouse adjustment to spinal cord injury: long term medical and psychosocial factors. Rehabilitation Counselling Bulletin 1988; 32: 4–21.
Stambrook M, Moore AD, Peters LC, Zubek E, McBeath S, Friesen 1C . Head injury and spinal cord injury: differential effects on psychosocial functioning. J Clin Exp Neuropsychol 1991; 13: 521–530.
Beard JG, Ragheb MG . Measuring leisure satisfaction. J Leisure Res 1980; 12: 20–35.
Di Bona L . What are the benefits of leisure? An exploration using the leisure satisfaction scale. Br J Occupational Therapy 2000; 63: 50–58.
Lewis G, Pelosi A, Araya R, Dunn G . Measuring psychiatric disorder in the community: a standardized assessment for use by lay interviewers. Psychol Med 1992; 22: 465–486.
World Health Organization. International Classification of Diseases-10 Primary Care (ICD-10 PC). Geneva: World Health Organization 1996.
Kuruvilla A, Pothen M, Philip K, Braganza D, Joseph A, Jacob KS . The validation of the Tamil version of the 12 item General Health Questionnaire. Indian J Psychiatry 1999; 41: 217–221.
Manoharam E, John KR, Joseph A, Jacob KS . Psychiatric morbidity, patient perspectives of illness and factors associated with poor medication compliance among the tuberculous in Vellore, South India. Indian J Tuberculosis 2001; 48: 77–80.
Harris JK, Godfrey HP, Partridge FM, Knight RG . Caregiver depression following traumatic brain injury (TBI): a consequence of adverse effects on family members? Brain Inj 2001; 15: 223–238.
Pothen M, Kuruvilla A, Philip K, Joseph A, Jacob KS . Common mental disorders among primary care attenders in Vellore, South India: nature, prevalence and risk factors. Intl J Soc Psychiatry 2003; 49: 119–125.
Jacob KS, Bhugra D, Lloyd KR, Mann AH . Common mental disorders, explanatory models and consultation behaviour among ethnic Indian women in primary care. JR Soc Med 1998; 91: 66–71.
Manigandan C, Saravanan B, Macaden A, Gopalan L, Tharion G, Bhattacharji S . Psychological wellbeing among carers of people with spinal cord injury: a preliminary investigation from South India. Spinal Cord 2000; 38: 559–562.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Raj, J., Manigandan, C. & Jacob, K. Leisure satisfaction and psychiatric morbidity among informal carers of people with spinal cord injury. Spinal Cord 44, 676–679 (2006). https://doi.org/10.1038/sj.sc.3101899
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101899
Keywords
This article is cited by
-
It is a marathon rather than a sprint: an initial exploration of unmet needs and support preferences of caregivers of children with SCI
Spinal Cord (2018)
-
The impact of spinal cord injury on the quality of life of primary family caregivers: a literature review
Spinal Cord (2017)
-
Burden of care in primary caregivers of individuals with spinal cord injury in Iran: its association with sociodemographic factors
Spinal Cord (2017)
-
Psychological impact and the burden of caregiving for persons with spinal cord injury (SCI) living in the community in Fiji
Spinal Cord (2011)
-
Relationships between the psychological characteristics of youth with spinal cord injury and their primary caregivers
Spinal Cord (2011)
