
Abstract
Aims:
To determine the monitoring and treatment of neonatal abstinence syndrome (NAS) in neonatal intensive care units (NICUs) following opiate or polydrug exposure in utero.
Methods:
A pretested questionnaire was distributed via email to the chiefs of the neonatology divisions with accredited Fellowship programs in Neonatal-Perinatal Medicine in the United States.
Results:
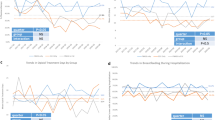
Of the 102 individuals contacted, 75 participated in the survey. In all, 41 of the respondents (54.5%) have a written policy regarding the management of neonatal NAS. The method of Finnegan is the most commonly used abstinence scoring system (49 of 75, 65%), while only three respondents use the Lipsitz tool. Opioids (tincture of opium, or morphine sulfate solution) are used most commonly for management of both opioid (63% of respondents) and polydrug (52% of respondents) withdrawal, followed by phenobarbital (32 % of respondents) for polydrug withdrawal and methadone (20% of respondents) for opioid withdrawal. In all, 53 respondents (70%) use phenobarbital, and 19 (25%) use intravenous morphine to control opioid withdrawal seizures, while 61 (81%) use phenobarbital in cases of polydrug withdrawal seizures. Only 53 respondents (70%) always use an abstinence scoring system to determine when to start, titrate, or terminate pharmacologic treatment of neonatal NAS.
Conclusion:
The management of neonatal psychomotor behavior consistent with withdrawal varies widely, with inconsistent policies to determine its presence or treatment. Only about half of NICUs have written guidelines for the management of NAS, which may preclude effective auditing of this practice. Educational interventions may be necessary to ensure changes in clinical practice.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Substance Abuse and Mental Health Services Administration, Office of Applied Studies. Preliminary Results From the 1996 National Household Survey on Drug Abuse. US Dept of Health and Human Services: Washington, DC August 1997.
American Academy of Pediatrics Committee on Drugs. Neonatal drug withdrawal. Pediatrics 1998; 101: 1079–1088.
Bodenheimer T . The American health care system. The movement for improved quality in health care. N Engl J Med 1999; 340: 488–492.
Madden JD, Chappel JN, Zuspan F, Gumpel J, Mejia A, Davis R . Observation and treatment of neonatal narcotic withdrawal. Am J Obstet Gynecol 1977; 127: 199–201.
Ostrea EM, Chavez CJ, Strauss ME . A study of factors that influence the severity of neonatal narcotic withdrawal. J Pediatr 1976; 88: 642–645.
Lipsitz PJA . Proposed narcotic withdrawal score for use with newborn infants. A pragmatic evaluation of its efficacy. Clin Pediatr 1975; 14: 592–594.
Finnegan LP, Kron RE, Connaughton JF, Emich JP . Assessment and treatment of abstinence in the infant of the drug-dependent mother. Int J Clin Pharmacol Biopharm 1975; 12: 19–32.
Morrison CL, Siney C . A survey of the management of neonatal opiate withdrawal in England and Wales. Eur J Pediatr 1996; 155: 323–326.
Micard S, Brion F . Management of the opioid withdrawal in the neonates: French and European survey. Arch Pediatr 2003; 10: 199–203.
Ambalavanan N, Kennedy K, Tyson J, Carlo WA . Survey of vitamin A supplementation for extremely-low-birth-weight infants: is clinical practice consistent with the evidence? J Pediatr 2004; 145: 304–307.
Leviton LC, Orleans CT . Promoting the uptake of evidence in clinical practice: a prescription for action. Clin Perinatol 2003; 30: 403–417.
Grol R . Implementation of evidence and guidelines in clinical practice: a new field of research? Int J Qual Health Care 2000; 12: 455–456.
Bero LA, Grilli R, Grimshaw JM, Harvey E, Oxman AD, Thomson MA . Closing the gap between research and practice: an overview of systematic reviews of interventions to promote the implementation of research findings: the Cochrane Effective Practice and Organization of Care Review Group. BMJ 1998; 317: 465–468.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies the paper on the Journal of Perinatology website (http://www.nature.com/jp).
Supplementary information
Rights and permissions
About this article
Cite this article
Sarkar, S., Donn, S. Management of neonatal abstinence syndrome in neonatal intensive care units: a national survey. J Perinatol 26, 15–17 (2006). https://doi.org/10.1038/sj.jp.7211427
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jp.7211427
Keywords
This article is cited by
-
Assessing the Eat, Sleep, Console model for neonatal abstinence syndrome management at a regional referral center
Journal of Perinatology (2023)
-
Implicit Racial Bias in Evaluation of Neonatal Opioid Withdrawal Syndrome
Journal of Racial and Ethnic Health Disparities (2023)
-
Capturing the statewide incidence of neonatal abstinence syndrome in real time: the West Virginia experience
Pediatric Research (2019)
-
Comparative effectiveness of opioid replacement agents for neonatal opioid withdrawal syndrome: a systematic review and meta-analysis
Journal of Perinatology (2019)
-
Another frontier for harm reduction: contraceptive needs of females who inject drugs in Estonia, a cross-sectional study
Harm Reduction Journal (2018)
