
Abstract
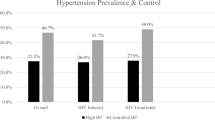
Among older people, the detection and control of hypertension is particularly important to reduce cardiovascular disease risk. This cross-sectional survey aimed to describe the detection, treatment and control of hypertension in older British adults. A total of 3059 women and 3007 men aged 60–79 years were randomly selected from general practice age/sex registers in 24 British towns and examined from 1998 to 2001. Of these, 52.6% women and 47.9% men had at least one indicator of hypertension (high blood pressure on examination, or taking antihypertensive medication or recalled a doctor diagnosis of high blood pressure). Among women, 50% of those with any indication of hypertension were on treatment and 29% were well controlled, and among men 45% were on treatment and 16% were well controlled. With the exception of alcohol use in men (adjusted odds ratio 0.67 (0.46, 0.98)), socioeconomic factors, area of residence and behavioural risk factors were not associated with good control among those with hypertension in either sex. Of those on treatment, 20.7% of women and 28% of men were on two classes of antihypertensive medication and 3.5 and 4.9%, respectively, were on three or more classes of antihypertensive medication. Among those with a doctor diagnosis of hypertension and taking antihypertensive medication, the proportion with well controlled blood pressure did not differ between those on more than one antihypertensive and those on just one in either sex. We conclude that targets of good control are rarely met in older individuals, who would benefit from the associated reduction in cardiovascular disease risk.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others


References
Lever AF, Ramsay LE . Treatment of hypertension in the elderly. J Hypertens 1995; 13 (6): 571–579.
Mulrow CD, Cornell JA, Herrera CR, Kadri A, Farnett L, Aguilar C . Hypertension in the elderly. Implications and generalizability of randomized trials. JAMA 1994; 272 (24): 1932–1938.
Perry Jr HM, Davis BR, Price TR, Applegate WB, Fields WS, Guralnik JM et al. Effect of treating isolated systolic hypertension on the risk of developing various types and subtypes of stroke: the Systolic Hypertension in the Elderly Program (SHEP). JAMA 2000; 284 (4): 465–471.
Sutton-Tyrrell K, Wildman R, Newman A, Kuller LH . Extent of cardiovascular risk reduction associated with treatment of isolated systolic hypertension. Arch Intern Med 2003; 163 (22): 2728–2731.
Wilber JA, Barrow JG . Hypertension – a community problem. Am J Med 1972; 52 (5): 653–663.
Hart JT . Rule of halves: implications of increasing diagnosis and reducing dropout for future workload and prescribing costs in primary care. Br J Gen Pract 1992; 42 (356): 116–119.
Marques-Vidal P, Tuomilehto J . Hypertension awareness, treatment and control in the community: is the ‘rule of halves’ still valid? J Hum Hypertens 1997; 11 (4): 213–220.
Duggan S, Eccles MP, Steen N, Jones S, Ford GA . Management of older patients with hypertension in primary care: improvement on the rule of halves. Age Ageing 2001; 30 (1): 73–76.
Cranney M, Barton S, Walley T . The management of hypertension in the elderly by general practitioners in Merseyside: the rule of halves revisited. Br J Gen Pract 1998; 48 (429): 1146–1150.
Primatesta P, Brookes M, Poulter NR . Improved hypertension management and control: results from the health survey for England 1998. Hypertension 2001; 38 (4): 827–832.
Weinehall L, Ohgren B, Persson M, Stegmayr B, Boman K, Hallmans G et al. High remaining risk in poorly treated hypertension: the ‘rule of halves’ still exists. J Hypertens 2002; 20 (10): 2081–2088.
Asmar R, Vol S, Pannier B, Brisac AM, Tichet J, El Hasnaoui A . High blood pressure and associated cardiovascular risk factors in France. J Hypertens 2001; 19 (10): 1727–1732.
Primatesta P, Poulter NR . Hypertension management and control among English adults aged 65 years and older in 2000 and 2001. J Hypertens 2004; 22 (6): 1093–1098.
National Centre for Social Research, Department of Epidemiology and Public Health at the Royal Free and University College Medical School, Commissioned by Department of Health. Health Survey for England 2003. The Stationery Office: London, 2003.
Lawlor DA, Whincup P, Emberson JR, Rees K, Walker M, Ebrahim S . The challenge of secondary prevention for coronary heart disease in older patients: findings from the British Women's Heart and Health Study and the British Regional Heart Study. Fam Pract 2004; 21 (5): 582–586.
Lawlor DA, Emberson JR, Ebrahim S, Whincup PH, Wannamethee SG, Walker M et al. Is the association between parity and coronary heart disease due to biological effects of pregnancy or adverse lifestyle risk factors associated with child-rearing? Findings from the British Women's Heart and Health Study and the British Regional Heart Study. Circulation 2003; 107 (9): 1260–1264.
Whincup PH, Bruce NG, Cook DG, Shaper AG . The Dinamap 1846SX automated blood pressure recorder: comparison with the Hawksley random zero sphygmomanometer under field conditions. J Epidemiol Community Health 1992; 46 (2): 164–169.
Joint Formulary Committee. British National Formulary, 48 edn. London: British Medical Association and Royal Pharmaceutical Society of Great Britain, 2004.
Williams B, Poulter NR, Brown MJ, Davis M, McInnes GT, Potter JF et al. Guidelines for management of hypertension: report of the fourth working party of the British Hypertension Society, 2004-BHS IV. J Hum Hypertens 2004; 18 (3): 139–185.
Lin HM, Hughes MD . Adjusting for regression toward the mean when variables are normally distributed. Stat Methods Med Res 1997; 6 (2): 129–146.
Morgan T, Anderson A . The effect of nonsteroidal anti-inflammatory drugs on blood pressure in patients treated with different antihypertensive drugs. J Clin Hypertens (Greenwich) 2003; 5 (1): 53–57.
Lawlor DA, Bedford C, Taylor M, Ebrahim S . Geographical variation in cardiovascular disease, risk factors, and their control in older women: British Women's Heart and Health Study. J Epidemiol Community Health 2003; 57 (2): 134–140.
National Institute for Clinical Excellence. Hypertension (Persistently High Blood Pressure) in Adults. NICE: London, 2004.
Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt D, Julius S et al. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet 1998; 351 (9118): 1755–1762.
McIntosh S, Da CD, Kenny RA, McIntosh S, Da Costa D, Kenny RA . Outcome of an integrated approach to the investigation of dizziness, falls and syncope in elderly patients referred to a ‘syncope’ clinic. Age Ageing 1993; 22 (1): 53–58.
Lindholm LH, Carlberg B, Samuelsson O, Lindholm LH, Carlberg B, Samuelsson O . Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005; 366 (9496): 1545–1553.
Campbell NC, Murchie P . Treating hypertension with guidelines in general practice. BMJ 2004; 329 (7465): 523–524.
Acknowledgements
We thank Carol Bedford, Alison Emerton, Nicola Frecknall, Karen Jones, Mark Taylor and Katherine Wornell for collecting and entering data for the BWHHS and Mary Walker, Lucy Lennon and Mary Thomas for collecting and entering data for the BRHS. We thank all of the general practitioners and their staff who have supported data collection and the women and men who have participated in the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Funding: The BWHHS and BRHS are funded by the (UK) Department of Health and British Heart Foundation. DAL is funded by a (UK) Department of Health Career Scientist Award. The views expressed in this publication are those of the authors and not necessarily those of any of the funding bodies. The funding bodies have had no influence over the scientific work or its publication.
Contributions:
RP: developed the study aim and wrote first draft of paper.
DAL: co-directs BWHHS, developed the study aim, undertook analyses, contributed to writing the paper.
PW: Co-directs BWHHS and BRHS, contributed to analyses and writing the paper.
DM: Contributed to analyses and writing the paper.
OP: Contributed to analyses and writing the paper.
PB: Contributed to development of the study aim and writing the paper.
SE: Co-directs BWHHS and BRHS, contributed to developing study aim and writing the paper.
RP, DAL and PW act as guarantors.
Conflict of interest: None.
Ethics: BWHHS and BRHS have received local and multi-centre research ethics committee approval.
Rights and permissions
About this article
Cite this article
Patel, R., Lawlor, D., Whincup, P. et al. The detection, treatment and control of high blood pressure in older British adults: cross-sectional findings from the British Women's Heart and Health Study and the British Regional Heart Study. J Hum Hypertens 20, 733–741 (2006). https://doi.org/10.1038/sj.jhh.1002064
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jhh.1002064
Keywords
This article is cited by
-
Social determinants of hypertension in high-income countries: A narrative literature review and future directions
Hypertension Research (2022)
-
Insight into rheumatological cause and effect through the use of Mendelian randomization
Nature Reviews Rheumatology (2016)
-
Mendelian Randomization: Application to Cardiovascular Disease
Current Hypertension Reports (2012)
-
The J-shape association of alcohol consumption on blood pressure levels, in elderly people from Mediterranean Islands (MEDIS epidemiological study)
Journal of Human Hypertension (2007)
