
Abstract
Background
Autosomal dominant polycystic kidney disease (ADPKD) is the most common hereditary renal disease. The course and progression of the disease is highly variable. In this study, we aimed to investigate the impact of clinical characteristics and basic biochemical parameters on progression of chronic kidney disease (CKD) in ADPKD patients.
Materials and methods
A total of 323 consecutive patients with ADPKD were enrolled into the study and followed with a mean duration of 100 ± 38 months. Patients were grouped as rapid progressors (RP) and slow progressors (SP) according to median rates of decline in glomerular filtration rate (ΔGFR) per year, namely 1 ml/min/year.
Results
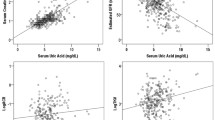
History of macroscopic hematuria, urinary stone and smoking were more common in male patients; hepatic and other organ cysts were more common in female patients. ∆GFR/year was similar between males and females [0.95 (0–3.02) vs. 1.11 (0.10–2.74) ml/min/year, p = 0.21]. History of smoking and pack-year of cigarettes smoked were significantly higher in the RP compared to the SP group (36 vs. 18 %, p = 0.01 and 5.24 ± 1.20 vs. 3 ± 1.32 pack-year, p = 0.02, respectively). Baseline 24 h-proteinuria was found to be significantly correlated with the percent decline of GFR (∆%GFR) per year (r = 0.303, 0.001). In Cox regression analysis for predicting the progression of CKD, age, hypertension, urinary stone and proteinuria were retained as the significant independent factors predicting progression of CKD in the model.
Conclusion
Baseline proteinuria was significantly correlated with ∆%GFR per year. Hypertension and proteinuria were found to be the major treatable risk factors for the progression of CKD in ADPKD patients.

Similar content being viewed by others


References
Ecder T, Fick-Brosnahan GM, Schrier RW. Polycystic kidney disease. In: Schrier RW, editors. Diseases of the kidney and urinary tract. 8th ed. Philadelphia: Lippincott, Williams & Wilkins; 2007.
Sessa A, Righetti M, Battini G. Autosomal recessive and dominant polycystic kidney diseases. Minerva Urol Nefrol. 2004;56:329–38.
Pei Y. Molecular genetics of autosomal dominant polycystic kidney disease. Clin Invest Med. 2003;26:252–8.
Fall PJ, Prisant LM. Polycystic kidney disease. J Clin Hypertens. 2005;7:617–9.
Grantham JJ. Autosomal dominant polycystic kidney disease. N Engl J Med. 2008;359:1477–85.
Chapman AB, Johnson AM, Gabow PA, Schrier RW. Overt proteinuria and micro-albuminuria in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1994;5:1349–54.
Pei Y, Obaji J, Dupuis A, Paterson AD, Magistroni R, Dicks E, Parfrey P, Cramer B, Coto E, Torra R, San Millan JL, Gibson R, Breuning M, Peters D, Ravine D. Unified criteria for ultrasonographic diagnosis of ADPKD. J Am Soc Nephrol. 2009;20(1):205–12.
Chapman AB, Schrier RW. Pathogenesis of hypertension in autosomal dominant polycystic kidney disease. Semin Nephrol. 1991;11:653–60.
Fick GM, Johnson AM, Hammond WS, Gabow PA. Causes of death in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1995;5:2048–56.
Schrier RW. Optimal care of autosomal dominant polycystic kidney disease patients. Nephrology. 2006;11:124–30.
Chapman AB, Gabow PA. Hypertension in autosomal dominant polycystic kidney disease. Kidney Int. 1997;52(Suppl 61):S71–3.
Kazancioglu R, Ecder T, Altintepe L, Altiparmak MR, Tuglular S, Uyanik A, Cavdar C, Ecder SA, Tokgoz B, Duman N, Duzova A, Turkish Society of Nephrology Polycystic Kidney Disease Working Group. Demographic and clinical characteristics of patients with autosomal dominant polycystic kidney disease: a multicenter experience. Nephron Clin Pract. 2011;117(3):c270–5.
Taylor M, Johnson AM, Tison M, Fain P, Schrier R. Earlier diagnosis of autosomal dominant polycystic kidney disease: importance of family history and implications for cardiovascular and renal complications. Am J Kidney Dis. 2005;46:415–23.
Ecder T, Schrier RW. Hypertension in autosomal-dominant poly cystic kidney disease: early occurrence and unique aspects. J Am Soc Nephrol. 2001;12:194–200.
Gabow PA, Johnson AM, Kaehny WD, Kimberling WJ, Lezotte DC, Duley IT, Jones RH. Factors affecting the progression of renal disease in autosomal-dominant polycystic kidney disease. Kidney Int. 1992;41:1311–9.
Schrier RW, McFann K, Johnson AM. Epidemiological study of kidney survival in autosomal dominant polycystic kidney disease. Kidney Int. 2003;63:678–85.
Ecder T, Edelstein CL, Chapman AB, Johnson AM, Tison L, Gill EA, Brosnahan GM, Schrier RW. Reversal of left ventricular hypertrophy with angiotensin converting enzyme inhibition in hypertensive patients with autosomal dominant polycystic kidney disease. Nephrol Dial Transplant. 1999;14:1113–6.
Klahr S, Breyer JA, Beck GJ, Dennis VW, Hartman JA, Roth D, Steinman TI, Wang SR, Yamamoto ME. Dietary protein restriction, blood pressure control, and the progression of polycystic kidney disease. Modification of Diet in Renal Disease Study Group. J Am Soc Nephrol. 1995;5:2037–47.
Schrier RW, McFann K, Johnson A, Chapman A, Edelstein C, Brosnahan G, Ecder T. Cardiac and renal effects of standard versus rigorous blood pressure control in autosomal-dominant polycystic kidney disease: results of a seven-year prospective randomized study. J Am Soc Nephrol. 2002;13:1733–9.
Ecder T, Edelstein CL, Fick-Brosnahan GM, Johnson AM, Chapman AB, Gabow PA, Schrier RW. Diuretics versus angiotensin-converting enzyme inhibitors in autosomal dominant polycystic kidney disease. Am J Nephrol. 2001;21(2):98–103.
Nutahara K, Higashihara E, Horie S, Kamura K, Tsuchiya K, Mochizuki T, Hosoya T, Nakayama T, Yamamoto N, Higaki Y, Shimizu T. Calcium channel blocker versus angiotensin II receptor blocker in autosomal dominant polycystic kidney disease. Nephron Clin Pract. 2005;99(1):c18–23.
Jafar TH, Stark PC, Schmid CH, Strandgaard S, Kamper AL, Maschio G, Becker G, Perrone RD, ACE Inhibition in Progressive Renal Disease (AIPRD) Study Group. The effect of angiotensin-converting-enzyme inhibitors on progression of advanced polycystic kidney disease. Kidney Int. 2005;67(1):265–71.
Bae K, Zhu F, Chapman A, Torres V, Grantham J, Guay-Woodford L, Baumgarten D, King BF, Wetzel LH, Kenney P, Brummer M, Bennett W, Klahr S, Meyers C, Zhang X, Thompson P, Miller J. Magnetic resonance imaging (MRI) evaluation of hepatic cysts in early autosomal dominant polycystic kidney disease (ADPKD): the Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP) Cohort. Clin J Am Soc Nephrol. 2006;1:64–9.
Choukroun G, Itakura Y, Albouze G, Christophe JL, Man NK, Grünfeld JP, Jungers P. Factors influencing progression of renal failure in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1995;6(6):1634–42.
Gabow PA, Duley I, Johnson AM. Clinical profiles of gross hematuria in autosomal dominant polycystic kidney disease. Am J Kidney Dis. 1992;20:140–3.
Gibson P, Watson ML. Cyst infection in polycystic kidney disease: a clinical challenge. Nephrol Dial Transplant. 1998;13:2455–7.
Grampsas SA, Chandhoke PS, Fan J, Glass MA, Townsed R, Johnson AM, Gabow P. Anatomic and metabolic risk factors for nephrolithiasis in patients with autosomal dominant polycystic kidney disease. Am J Kidney Dis. 2000;36:53–7.
Torres VE, Wilson DM, Hattery RR, Segura JW. Renal stone disease in autosomal polycystic kidney disease. Am J Kidney Dis. 1993;22:513–9.
Orth SR, Stockman A, Conradt C, Ritz E, Ferro M, Kreusser W, Piccoli G, Rambausek M, Roccatello D, Schafer K, Sieberth HG, Wanner C, Watschinger B, Zucchelli P. Smoking as a risk factor for end-stage renal failure in men with primary renal disease. Kidney Int. 1998;54:926–31.
Hallan SI, Orth SR. Smoking is a risk factor in the progression to kidney failure. Kidney Int. 2011;80:516–23.
Higashihara E, Horie S, Muto S, Mochizuki T, Nishio S, Nutahara K. Renal disease progression in autosomal dominant polycystic kidney disease. Clin Exp Nephrol. 2012;16(4):622–8.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Ozkok, A., Akpinar, T.S., Tufan, F. et al. Clinical characteristics and predictors of progression of chronic kidney disease in autosomal dominant polycystic kidney disease: a single center experience. Clin Exp Nephrol 17, 345–351 (2013). https://doi.org/10.1007/s10157-012-0706-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-012-0706-3