
Abstract
Several commercial assays for SARS-CoV-2 RT-PCR are available but few of them were assessed. We evaluate the Allplex 2019-nCoV (Seegene) assay using 41 nasopharyngeal samples. The rates of agreement were 92.7% and 100% with the GeneFinder COVID-19 plus (Elitech) and the diagnosis of the infectious disease specialist respectively. Four samples display a Ct < 22.0 for the E and RdRp genes while the N gene was not detected, suggesting a variability of the viral sequence. There was no cross-reactivity with other respiratory viruses. The Allplex 2019-nCoV appears as a reliable method, but additional evaluations using more samples are needed. RT-PCR assays should probably include at least 2 viral targets.
Similar content being viewed by others


Introduction
SARS-CoV-2 has rapidly spread, infecting more than 3.9 million people and causing more than 275,000 death 19 weeks after the WHO was alerted by Chinese health authority on December 31, 2019 [1]. As the clinical presentation of the disease is nonspecific and in order to improve the management of the patients and to limit the spread of the virus, a robust and accurate diagnosis is needed. According to the WHO, laboratory confirmation is required for suspicious cases [2]. Molecular methods performed on respiratory specimen are considered the gold standard as they are specific and viral excretion appears early, before the onset of the symptoms [3].
The Allplex 2019-nCoV assay (Seegene, Seoul, South Korea) was designed for amplifying three viral targets: the E gene (specific of the subgenus Sarbecovirus), the N and the RdRP genes (both specifics of the SARS-CoV-2). The assay is approved for in vitro diagnostic in several countries as South Korea and France. The first assessment of its performances by the manufacturer demonstrates a specificity of 100% and a limit of detection of 100 RNA copies/PCR reactions. Following first manufacturer recommendations, samples with 1 or 2 viral targets were considered inconclusive and should be retested using a “higher concentration of sample” or a “gene sequencing” should be performed [4]. But, according to the revised recommendations issue in late April 2020, these profiles are considered positive. However, as the reagent was rapidly available in limited quantities and clinical laboratories were overwhelmed, no independent assessments of the assay performances were achieved. We aim to assess the performances of the Allplex 2019-nCoV assay mainly focusing on positive results for one or two viral targets.
Methods
The Allplex 2019-nCoV assay had been routinely implemented at the Hospital Foch on March 10, 2020. The performances of the kit were assessed using 41 nasopharyngeal specimen sampled on universal transport media (UTM, Copan, Mylan, Italy).
Twenty-five samples were collected prospectively from adults suspected of COVID-19. Of them, all consecutive samples positive for 1 or 2 targets (n = 20) collected from March 10 to March 25, 2020, and 5 samples positive for all three viral targets using the Allplex 2019-nCoV were included. The results of the Allplex 2019-nCoV were compared with (i) the GeneFinder COVID-19 plus assay (Elitech, Puteaux, France), and (ii) the diagnosis of the infectious disease specialist of the hospital on the basis of epidemiological exposure, clinical and laboratory examination, and chest computed tomography findings. UTM were frozen at − 70 °C before testing by the GeneFinder COVID-19 plus assay. This assay includes 3 viral genes and it is routinely used at the hospital Bichat.
In addition, a collection of 16 nasopharyngeal specimens positive to another respiratory virus was included for the evaluation of cross-reactivity. All were collected from hospitalized patients presenting with symptoms of flu or viral pneumonia. Viral agents were identified using the FilmArray RP assay (BioMérieux, Marcy-l’Etoile, France). The number of positive samples per pathogen was as follows: coronavirus (6), human metapneumovirus (3), influenza (4), and human rhinovirus (3) (Table 1).
Statistical analysis was performed using IBM SPSS Statistics version 20.0.0 (IBM Corp., Armonk, NY, USA). The results of the Allplex 2019-nCoV were compared with those of the GeneFinder COVID-2019 plus and the diagnosis of the infectious disease specialist using the agreement rate and the Kappa test.
Results
Overall, 25 and 16 samples were positive for at least a viral target and negative using the Allplex 2019-nCoV respectively.
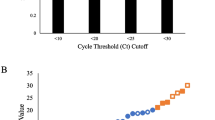
Among the 20 samples positive for 1 or 2 viral targets using the Allplex 2019-nCoV, 13 (65%) and 7 (35%) were positive for 2 and 1 viral targets respectively (Table 2). The E, RdRP, and N genes were detected in 7, 15, and 11 samples respectively. The median cycle threshold (Ct) of positivity was 18.4 (15.9–34.0) for the E gene, 36.6 (26.4–38.1) for the RdRp gene, and 38.0 (37.7–38.6) for the N gene. Four samples positive for E and RdRp genes display a Ct below 22.0 for both viral targets. Excluding these samples, the median Ct was 34.5 (34.1–34.8), 37.6 (36.6–38.3), and 38.0 (37.7–38.6) for E, RdRp, and N genes respectively. Considering the samples positive for two viral targets, the E and N gene combinations were detected in 2, the RdRp and N genes in 6, and the E and RdRp genes in 5. Except sample no. 13, all samples negative for the N gene but positive for the E and the RdRp genes display a Ct below 22.0 for both viral targets. Two out of the 6 samples positive for the N and the RdRp genes display a Ct below 35.0 for both viral targets (samples no. 6 and 7). Of the 7 samples positive for a single viral target, 4 and 3 were positive for the RdRp and the N genes respectively. All detected targets display a Ct greater than 35.0 regardless of the viral gene.
All 16 nasopharyngeal samples positive to another respiratory virus were found negative with the Allplex 2019-nCoV.
The Allplex 2019-nCoV and the GeneFinder COVID-19 plus show an overall agreement of 92.7%, and a Kappa value of 0.86. Two (15.4%) out of 13 samples positive for 2 viral targets using the Allplex 2019-nCoV were found negative using the GeneFinder COVID-19 plus assay. One of them was positive for the E (Ct = 34.5) and the RdRp (Ct = 38.1) genes while the other was positive for the RdRp (Ct = 38.2) and the N (Ct = 37.5) genes. The GeneFinder COVID-19 plus assay was negative in 1 (14.3%) over the 7 samples positive for a single viral target using the Allplex 2019-nCoV. This sample (no. 18) was positive for the RdRp gene with a Ct of 39.1. The Allplex 2019-nCoV and the diagnosis of the infectious disease specialist show an overall agreement of 100% and a Kappa value of 1.
Discussion
Our results suggest that the Allplex 2019-nCoV is a reliable method for the confirmation diagnosis of SARS-CoV-2 infection. Most samples positive for 1 or 2 viral targets could be considered positive. Several of these samples display a Ct greater than 35.0 suggesting they contain a low viral load. This finding might explain why one or two viral genes were not amplified. In contrast, 4 samples display a Ct below 22.0 for the E and the RdRp genes while the N gene was not amplified. The low Ct recovered for the E and the RdRP genes suggests a high viral load. And, we can rule out a mishandling as the premix contains all primers and probes. A deficient batch is also unlikely as the reagents were used for more than 150 positive samples and only these 4 samples display such profile. Finally, we could hypothesize variability in the viral genome sequence. Indeed, as the assay was designed at the beginning of the pandemic when few viral genomes were already sequenced, it is possible that RT-PCR designers were not able to consider sufficient sequence variability. Furthermore, higher variability of the N gene was previously reported [2, 5].
Three positive samples using the Allplex 2019-nCoV were found negative using the GeneFinder COVID-19 plus. All the patients were considered as presenting a COVID-19 by the infectious disease specialist. This finding could suggest a viral RNA degradation during sample conservation or transport rather than a nonspecific amplification. Indeed, the assay appears specific regarding the absence of cross-reaction with another respiratory virus.
Unfortunately, we were not able to perform a cross-reactive assay with sample positive for the SARS or the MERS-CoV viruses. However, in the actual context of the rapid spread of the SARS-CoV-2 and as the MERS-CoV and the SARS outbreaks are under control, a misidentification is unlikely. Furthermore, all patients infected by SARS-CoV-2, SARS, or MERS-CoV require similar infection prevention and control measures.
Molecular methods for SARS-CoV-2 identification were little assessed yet. Some in-house RT-PCR were reported as presenting a high sensitivity and specificity, but commercial assays were not evaluated [6,7,8]. However, previous reports mainly focused on false negative and low sensitivity of RT-PCR performed on respiratory samples in comparison with chest computed tomography [9,10,11,12,13]. However, these studies display several methodologic limitations. First, a few numbers of samples were included [11,12,13]. Main samples used were throat or nasal swab instead of nasopharyngeal swabs [9, 11, 12]. These latter were reported more suitable for SARS-CoV-2 infection as for flu diagnosis [14,15,16]. Finally, RT-PCR assay displays a single viral target and/or designed at the early stage of the disease when few genome sequences were available [9,10,11].
In conclusion, the Allplex 2019-nCoV assay appears accurate for the confirmation diagnosis of SARS-CoV-2 infection. Sample displaying 1 or 2 detected viral targets should be considered positive. We, therefore, emphasize the need of including at least 2 viral targets for RT-PCR. This finding is of particular concern for patients at risk of developing severe disease and healthcare workers. Independent assessments of molecular methods are mandatory.
References
ECDC (2020) 2019-ncov situation update. https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases
Wang C, Liu Z, Chen Z, Huang X, Xu M, He T, et al (2020) The establishment of reference sequence for SARS-CoV-2 and variation analysis. J. Med. Virol [cited 2020 12];jmv.25762. https://onlinelibrary.wiley.com/doi/abs/10.1002/jmv.25762
Pan Y, Zhang D, Yang P, Poon LLM, Wang Q (2020) Viral load of SARS-CoV-2 in clinical samples. Lancet Infect Dis. https://doi.org/10.1016/S1473-3099(20)30113-4
Seegene (2020) Allplex 2019-nCoV Assay Instruction for use
Ceraolo C, Giorgi FM (2020) Genomic variance of the 2019-nCoV coronavirus. J Med Virol 92:522–528. https://doi.org/10.1002/jmv.25700
Pfefferle S, Reucher S, Nörz D, Lütgehetmann M (2020) Evaluation of a quantitative RT-PCR assay for the detection of the emerging coronavirus SARS-CoV-2 using a high throughput system. Eurosurveillance 25:2000152. https://doi.org/10.2807/1560-7917.es.2020.25.9.2000152
Corman VM, Landt O, Kaiser M, Molenkamp R, Meijer A, Chu DK et al (2020) Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill 1:25. https://doi.org/10.2807/1560-7917.ES.2020.25.3.2000045
Nalla AK, Casto AM, Huang M-LW, Perchetti GA, Sampoleo R, Shrestha L, et al (2020) Comparative performance of SARS-CoV-2 detection assays using seven different primer/probe sets and one assay kit. J. Clin. Microbiol [cited 2020 18]. http://jcm.asm.org/lookup/doi/10.1128/JCM.00557-20
Ai T, Yang Z, Hou H, Zhan C, Chen C, Lv W, et al (2020) Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology 26 [cited 2020 26];200642. http://www.ncbi.nlm.nih.gov/pubmed/32101510. https://doi.org/10.1148/radiol.2020200642
Li D, Wang D, Dong J, Wang N, Huang H, Xu H, et al (2020) False-negative results of real-time reverse-transcriptase polymerase chain reaction for severe acute respiratory syndrome coronavirus 2: role of deep-learning-based ct diagnosis and insights from two cases. Korean J. Radiol [cited 2020 19];21:505. https://synapse.koreamed.org/DOIx.php?id=10.3348/kjr.2020.0146
Wang W, Xu Y, Gao R, Lu R, Han K, Wu G, et al (2020) Detection of SARS-CoV-2 in different types of clinical specimens. JAMA [cited 2020 23] http://www.ncbi.nlm.nih.gov/pubmed/32159775. https://doi.org/10.1001/jama.2020.3786
Fang Y, Zhang H, Xie J, Lin M, Ying L, Pang P, et al (2020) Sensitivity of chest CT for COVID-19: comparison to RT-PCR. Radiology [cited 2020 26];200432. http://www.ncbi.nlm.nih.gov/pubmed/32073353. https://doi.org/10.1148/radiol.2020200432
Long C, Xu H, Shen Q, Zhang X, Fan B, Wang C et al (2020) Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur J Radiol 1:126. https://doi.org/10.1016/j.ejrad.2020.108961
Spencer S, Thompson MG, Flannery B, Fry A (2019) Comparison of respiratory specimen collection methods for detection of influenza virus infection by reverse transcription-PCR: a literature review. J Clin Microbiol 57:1–6. https://doi.org/10.1128/JCM.00027-19
Zou L, Ruan F, Huang M, Liang L, Huang H, Hong Z, et al (2020) SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med cited 2020 23];382:1177–9. http://www.nejm.org/doi/10.1056/NEJMc2001737. https://doi.org/10.1056/NEJMc2001737
Huang Y, Chen S, Yang Z, Guan W, Liu D, Lin Z, et al (2020) SARS-CoV-2 Viral load in clinical samples of critically ill patients. Am J Respir Crit Care Med [cited 2020 26]. http://www.ncbi.nlm.nih.gov/pubmed/32293905. https://doi.org/10.1164/rccm.202003-0572LE
Acknowledgments
The authors wish to thank all the teams at Foch Hospital and Bichat Hospital involved in the care of patients with and without COVID-19. The members of the Sars-Cov-2 Foch Hospital study group are the following: Emilie Catherinot, Colas Tcherakian, Louis-Jean Couderc, Sylvie Colin de Verdière, Charlotte Roy, and Antoine Roux (service de pneumologie et transplantation pulmonaire); Benjamin Zuber, Mathilde Neuville, Richard Galliot, and Charles Cerf (service de réanimation); Morgan Le Guen (service d'anesthésie); Mathilde Roumier, Antoine Bizard, Felix Ackermann, David Zucman, Yoland Schoindre, David Khau, Mathieu Groh, and Romain Paule (Service de médecine interne); Marion Lecuru (service de biologie clinique); Philippe Grenier, Anne-Laure Brun, and François Mellot (service d’imagerie médicale); and Anne Verrat, Etienne Imhaus, Charlotte Rachline, and Marie-Christine Ballester (service des Urgences).
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All the procedures were in accordance with the 1964 Helsinki Declaration and its later amendments.
Informed consent
According to French Health Public Law (CSP Article L1121-1), this type of study did not require specific informed consent or ethics committee approval.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Farfour, E., Lesprit, P., Visseaux, B. et al. The Allplex 2019-nCoV (Seegene) assay: which performances are for SARS-CoV-2 infection diagnosis?. Eur J Clin Microbiol Infect Dis 39, 1997–2000 (2020). https://doi.org/10.1007/s10096-020-03930-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-020-03930-8