
Abstract
Introduction
Chronic obstructive pulmonary disease (COPD) exacerbations are associated with systemic consequences. Data from a 4-year trial (Understanding Potential Long-term Impacts on Function with Tiotropium [UPLIFT®], n = 5,992) were used to determine risk for nonlower respiratory serious adverse events (NRSAEs) following an exacerbation.
Methods
Patients with ≥1 exacerbation were analyzed. NRSAE incidence rates (incidence rate [IR], per 100 patient-years) were calculated for the 30 and 180 days before and after the first exacerbation. NRSAEs were classified by diagnostic terms and organ classes. Maentel-Haenszel rate ratios (RR) (pre- and postexacerbation onset) along with 95% confidence intervals (CI) were computed.
Results
A total of 3,960 patients had an exacerbation. The mean age was 65 years, forced expiratory volume in 1 s (FEV1) was 38% predicted, and 74% were men. For all NRSAEs, the IRs 30 days before and after an exacerbation were 20.2 and 65.2 with RR (95% CI) = 3.22 (2.40–4.33). The IRs for the 180-day periods were 13.2 and 31.0 with RR (95% CI) = 2.36 (1.93–2.87). The most common NRSAEs by organ class for both time periods were cardiac, respiratory system (other), and gastrointestinal. All NRSAEs as well as cardiac events were more common after the first exacerbation, irrespective of whether the patient had cardiac disease at baseline.
Conclusions
The findings confirm that, after exacerbations, serious adverse events in other organ systems are more frequent, particularly those that are cardiac in nature.
Similar content being viewed by others


Introduction
Exacerbations of chronic obstructive pulmonary disease (COPD) impair health status [1, 2] and appear to accelerate the progression of the disease [3]. An exacerbation can lead to profound symptoms, disrupt the ability to engage in activities of daily living, and may take several weeks or months to resolve [4]. Of note, some patients may not fully return to baseline function following an exacerbation of COPD.
Exacerbations are associated with a considerable early mortality [5], but the frequency and severity of exacerbations are also associated with long-term mortality, independent of age, forced expiratory volume in 1 s (FEV1), body mass index, and the presence of comorbidities [6]. Comorbidities are common in people with COPD, and they may be worsened by the occurrence of an exacerbation and potentially worsen the severity and impact of the exacerbation itself.
The Understanding Potential Long-term Impacts on Function with Tiotropium (UPLIFT®) trial was designed to determine the long-term efficacy and safety of tiotropium, a once-daily, inhaled anticholinergic, in patients with COPD, with the rate of decline in FEV1 being the primary end point. Although there was no difference in the rate of FEV1 decline over the control group, patients receiving tiotropium had significant improvements in lung function and health-related quality of life and a reduced risk for exacerbations, associated hospitalizations, and episodes of respiratory failure, as well as a reduced all-cause mortality [7].
Patients who participated in the UPLIFT® study were carefully observed over a period of 4 years, and the occurrence of exacerbations and adverse events were recorded throughout the period in which patients were receiving the study drug. We therefore examined this large clinical trial database to assess the relationship between exacerbations and the occurrence of nonrespiratory morbidity recorded as adverse events.
Methods
Details of the UPLIFT® study design and results of the primary and secondary end points have been reported previously [7, 8]. All patients gave written informed consent, and the study was approved by local ethical review boards and conducted in accordance with the Declaration of Helsinki.
Study Design
The study was a 4-year, randomized, double-blind, placebo-controlled, parallel-group trial of patients with COPD. Patients received either tiotropium 18 μg once daily or a matching placebo delivered via the HandiHaler® inhalation device (Boehringer Ingelheim International GmbH, Ingelheim, Germany).
Patients were recruited from 490 investigational centers in 37 countries. Criteria for participation included diagnosis of COPD, age at least 40 years, smoking history of at least 10 pack-years, postbronchodilator FEV1 ≤70% of the predicted normal, and FEV1 ≤70% of forced vital capacity. Postrandomization clinic visits occurred at 1 and 3 months and then every 3 months throughout the 4-year treatment period. All respiratory medications, other than inhaled anticholinergics, were permitted during the trial.
Exacerbations
Exacerbations were defined as an increase in or the new onset of more than one respiratory symptom (cough, sputum, sputum purulence, wheezing, or dyspnea) lasting 3 days or more and requiring treatment with an antibiotic or a systemic corticosteroid. Data regarding exacerbations and related hospitalizations were collected on study-specific case-report forms at every visit.
Adverse Events
Adverse events, including those deemed serious and fatal, were coded using the Medical Dictionary for Regulatory Activities (MedDRA) ver. 11.1. Diagnostic terms are referred to as preferred terms. These are totaled in higher categories, including organ systems (referred to as system organ classes [SOCs]). Additional prespecified categories of preferred terms were also formed prior to unblinding of the trial, where several preferred terms described a similar clinical event. Because numerous categories exist, those that are representative of major groupings and are of significant public health concern have been chosen for display. An individual patient may contribute several terms but will be represented only once in a category, such as a SOC.
Serious adverse events were identified according to the standard definition: “A serious adverse event (experience) or reaction is any untoward medical occurrence that at any dose: results in death, is life-threatening, requires inpatient hospitalization or prolongation of existing hospitalization, results in persistent or significant disability/incapacity, or is a congenital anomaly/birth defect” [9].
Data Analysis
The population included in the current analysis was restricted to only those patients with an exacerbation of COPD. Only patients who survived their first exacerbation (i.e., the investigator indicated resolution of the exacerbation prior to a fatal event, if present) were included in order to determine the frequency of nonrespiratory events following the onset of an exacerbation.
Serious adverse event incidence rates (IRs) (per 100 patient-years) were calculated for time periods limited to 30 and 180 days before and after the first recorded exacerbation (using a standardized definition). In patients who had more than one exacerbation, the analysis was restricted to before and after the first exacerbation. IRs were calculated from the number of patients experiencing an event divided by the person-years at risk. Maentel-Haenszel rate ratios (RR) (pre- and postexacerbation onset) were computed along with the associated 95% confidence interval (CI). Only people who remained exacerbation-free for at least 30 or 180 days were included in the analyses. Events occurring on the same day as the onset of the exacerbation were included in the “after” period as they were considered to be related to the occurrence of the exacerbation. The IRs and RRs for nonlower respiratory serious adverse events (NRSAEs) were also calculated separately for patients who did or did not have a cardiac disorder present at entry into the study.
In order to examine the influence of season on the relationship between exacerbations and subsequent adverse events, the IRs and RRs before and after the first exacerbation were calculated separately according to whether the first exacerbation occurred in the winter (October–March for northern hemisphere countries and April–September for southern hemisphere countries) or summer period. For this analysis, each patient was included in the preexacerbation period for as long as he/she did not experience an exacerbation or the occurrence of the respective adverse event. Each patient was included in the postexacerbation period, starting with the onset of the first exacerbation and for as long as they were in the study until 30 days after treatment or the occurrence of the respective adverse event.
Results
Study Population
The UPLIFT® population consisted of 5,992 randomized patients who received the study drug (3,006 to placebo and 2,986 to tiotropium). The baseline demographics have been previously reported [7]. The mean age was 65 ± 8 years, 75% of the patients were men, and 30% were smoking at randomization. Mean prebronchodilator FEV1 was 1.10 ± 0.40 L (39% predicted) and postbronchodilator FEV1 was 1.32 ± 0.44 L (48% predicted). Approximately 45% of the control population prematurely discontinued placebo compared with 36% of patients treated with tiotropium. At baseline, approximately 62% of patients used an inhaled steroid, 60% used a long-acting β-agonist, and 23% used theophylline-containing preparations. Serious adverse events were reported by 52% in the tiotropium group and 50% in the placebo group [7]. Serious adverse events reported by more than 1% of patients in either study group were cardiac, respiratory, or neoplastic [7].
A total of 3,960 patients had a nonfatal exacerbation during the 4-year follow-up period. Table 1 shows the baseline characteristics of patients who had an exacerbation. Serious adverse events were reported by 52% in the tiotropium group and 50% in the placebo group [7].
The IRs (per 100 patient-years) and incidence RRs for 30 days before and after the first exacerbation for the NRSAEs by organ class where at least five people experienced an event are shown in Table 2 (sorted by the IR in the postexacerbation period). The most common prespecified adverse event categories where at least five people experienced the event during this time period are also listed in Table 2. Cardiac disorders and gastrointestinal (GI) disorders were the most commonly occurring serious nonrespiratory adverse event organ classes. In all organ classes, the RR (i.e., risk) of an event was higher after an exacerbation. For five of these 13 organ classes affected, the lower limits of the 95% CI exceeded “1.” Cardiac failure, ischemic heart disease, myocardial infarction (MI), angina, atrial fibrillation/flutter, and stroke were the most common prespecified events overall. For all nine of the categories, the risk of an event was again higher after an exacerbation, and for four of these categories (all cardiac), the lower limits of the 95% CI for the RR exceeded “1.”
The IRs (per 100 patient-years) and incidence RRs for 180 days before and after the first exacerbation for the NRSAEs by organ class where at least 10 people experienced an event during the period are shown in Table 3 (sorted by the IR in the postexacerbation period). Cardiac disorders and GI disorders were again the most commonly occurring serious nonrespiratory adverse event organ classes. In all organ classes, the risk of an event was higher after an exacerbation. For seven of these 11 organ classes affected, the lower limits of the 95% CI for the RR exceeded “1.” Cardiac failure, ischemic heart disease, MI, angina, atrial fibrillation/flutter, and stroke were again the most common prespecified events overall. For all six of the common events, the risk of an event was higher after an exacerbation, and for five of these categories (all cardiac), the lower limits of the 95% CI for the RR exceeded “1.”
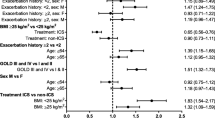
The IRs and RRs for NRSAEs in the 30 and 180 days before and after the first exacerbation according to whether patients did or did not have a cardiac disorder present at entry to the study are shown in Tables 4 and 5. Overall serious adverse events were more common in people who had cardiac disease at baseline. Ischemic heart disease, MI, angina, cardiac failure, atrial fibrillation/flutter, nonventricular tachycardia, and stroke were all more common in the 30- and 180-day periods after an exacerbation than before, irrespective of the presence of cardiac disease at baseline. In people who did not have cardiac disease at entry to the study, the lower limits of the 95% CI exceeded “1” only for ischemic heart disease and cardiac failure for the 30-day period and for ischemic heart disease, MI, angina, and cardiac failure for the 180-day period.
The IRs and RRs before and after the first exacerbation for first exacerbations that occurred in the winter and summer periods are shown in Table 6. The CIs of the RRs (before/after an exacerbation) for the two periods overlapped, indicating that the relationship between adverse events and exacerbations did not differ according to whether the exacerbation occurred in the summer or winter.
Discussion
The UPLIFT® trial was designed to assess the effect of tiotropium on the clinical course of patients with COPD who were permitted to use all respiratory medications throughout the trial, other than inhaled anticholinergics. The study showed that use of tiotropium was associated with improvements in lung function and quality of life and a reduction of 14% in the risk for an exacerbation (p < 0.001) [7]. The incidence of serious adverse events was also lower in patients receiving tiotropium.
In addition to providing data on the clinical effects of tiotropium, the UPLIFT® study provided information on the relationship between exacerbations and NRSAEs. The results of this analysis show that exacerbations were associated with an increased risk of serious events in other organ systems, most commonly cardiac. This was true in both patients treated with tiotropium and those receiving the placebo in addition to their usual medication, and in patients who did or did not have cardiac disease at entry to the study.
A previous smaller observational study of the temporal relationship between exacerbations and cardiovascular events using the Health Improvement Network database suggested a 2.3-fold increase in the risk of a MI 1-5 days after an exacerbation; however, there did not appear to be an association at any other time following an exacerbation. The risk for stroke was increased by 1.3-fold within 1-49 days following an exacerbation [10].
Exacerbations may be triggered by bacteria, viruses, and noninfective stimuli such as air pollution. These stimuli appear to amplify the inflammatory process present in the stable state [11]. Exacerbations increase the level of systemic inflammation [12, 13] and oxidative stress [14, 15], which can have adverse effects on other organs. For example, troponin T is elevated during exacerbations and is associated with increased mortality [16]. Similarly, renal endothelin-1 production is increased during exacerbations [17], which may underpin some of the vascular consequences of exacerbations. There is an increased prothrombotic state in patients with COPD during acute exacerbations, as shown by increased circulating fibrinogen levels [12], and there is evidence of increased endothelial dysfunction during and after exacerbations of COPD [18], increasing the risk of cardiovascular morbidity.
It is also possible that the factors that lead to exacerbations may also have systemic consequences. MIs, pulmonary emboli, and venous thromboses are significantly more common immediately after respiratory infections [19], which are associated with peripheral acute-phase responses, including the production and release of TNF-α, IL-6, and CRP. Particulate air pollution may also trigger a systemic inflammatory response by inducing oxidative stress in the airways [20].
In addition to the fact that exacerbations may worsen the systemic effects of COPD, the presence of systemic effects or comorbidities may also worsen the severity of an exacerbation and lead to worse outcomes. In order to study the effect of exacerbations on these effects it is important to have prospective data from large cohorts such as the UPLIFT® trial. The data provide important evidence for the relationship between exacerbations and serious nonrespiratory outcomes, although they cannot prove causality. The conclusions are strengthened by the duration of the study and the use of a standardized definition of an exacerbation. Nevertheless, there are still some potential limitations to the analysis. It could be argued that the patients who took part were selected for involvement in a clinical trial and therefore may not be fully representative of patients seen in practice, particularly with regard to disease severity and the presence of comorbidities. However, the inclusion and exclusion criteria were relatively liberal and recruitment included a broad selection of COPD patients with multiple comorbidities.
Time-based analyses are potentially subject to biases, such as the need to survive long enough to be included in the analysis, and these need to be considered when interpreting the results. Events occurring on the same day as the onset of the exacerbation were included in the “after” and, although it is possible that the adverse event in the other organ system triggered the COPD exacerbation, we believe that it is unlikely from a clinical perspective that an exacerbation would be regarded as starting on the same day. It is more likely it would be reported as starting after the nonrespiratory adverse event.
Another possible confounder is the potential for detection bias as a result of additional tests being ordered as part of an evaluation for an exacerbation or the possibility that other medical conditions are identified when the patients are admitted to hospital with an exacerbation. These factors are likely to have only a limited role given that the current analysis is based on serious adverse events and not concomitant nonserious events that may be incidental findings as part of a broader medical evaluation. The frequency of hospitalization is too low to allow a meaningful analysis of differences in the occurrence of adverse events after hospitalized and nonhospitalized exacerbations. Finally, it is also possible that the treatment given to the patient at the time of the exacerbation may have led to the development of the adverse event.
In addition to the difficulty of proving a causal link, there are other limitations to the analysis of the relationship between exacerbations and systemic effects. To be recorded as a serious adverse event, the systemic effect must lead to death or be judged life-threatening, have required inpatient hospitalization or prolongation of existing hospitalization, or result in persistent or significant disability/incapacity. While this could be considered restrictive, the advantage is that only the most clinically important events are part of the definition.
In conclusion, this analysis confirms that besides worsening respiratory outcomes, the risk of systemic events is increased after exacerbations, particularly shortly after the event. It further reinforces the importance of preventing or reducing exacerbation rates as an aim of COPD management. Treating physicians must also be vigilant for concomitant disease in other organ systems which may follow an exacerbation. Increased awareness and prompt treatment may contribute to reductions in morbidity associated with COPD.
References
Spencer S, Jones PW (2003) Time course of recovery of health status following an infective exacerbation of chronic bronchitis. Thorax 58:589–593
Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA (1998) Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 157(5 Pt 1):1418–1422
Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA (2002) Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax 57:847–852
Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA (2000) Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 161:1608–1613
Price LC, Lowe D, Hosker HS, Anstey K, Pearson MG, Roberts CM, British Thoracic Society and the Royal College of Physicians Clinical Effectiveness Evaluation Unit (CEEu) (2006) UK National COPD Audit 2003: impact of hospital resources and organisation of care on patient outcome following admission for acute COPD exacerbation. Thorax 61:837–842
Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R (2005) Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 60:925–931
Tashkin DP, Celli B, Senn S, Burkhart D, Kesten S, Menjoge S, Decramer M, UPLIFT Study Investigators (2008) A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med 359:1543–1554
Decramer M, Celli B, Tashkin DP, Pauwels RA, Burkhart D, Cassino C, Kesten S (2004) Clinical trial design considerations in assessing long-term functional impacts of tiotropium in COPD: the UPLIFT trial. COPD 1:303–312
International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (1994) Clinical safety data management: definitions and standards for expedited reporting E2A
Donaldson GC, Hurst JR, Smith CJ, Hubbard RB, Wedzicha JA (2010) Increased risk of myocardial infarction and stroke following exacerbation of COPD. Chest 137:1091–1097
Celli BR, Barnes PJ (2007) Exacerbations of chronic obstructive pulmonary disease. Eur Respir J 29:1224–1238
Wedzicha JA, Seemungal TA, MacCallum PK et al (2000) Acute exacerbations of chronic obstructive pulmonary disease are accompanied by elevations of plasma fibrinogen and serum IL-6 levels. Thromb Haemost 84:210–215
Seemungal T, Harper-Owen R, Bhowmik A et al (2001) Respiratory viruses, symptoms, and inflammatory markers in acute exacerbations and stable chronic obstructive pulmonary disease. Am J Respir Crit Care Med 164:1618–1623
Rahman I, Skwarska E, MacNee W (1997) Attenuation of oxidant/antioxidant imbalance during treatment of exacerbations of chronic obstructive pulmonary disease. Thorax 52:565–568
Drost EM, Skwarski KM, Sauleda J et al (2005) Oxidative stress and airway inflammation in severe exacerbations of COPD. Thorax 60:293–300
Brekke PH, Omland T, Holmedal SH, Smith P, Søyseth V (2008) Troponin T elevation and long-term mortality after chronic obstructive pulmonary disease exacerbation. Eur Respir J 31:563–570
Sofia M, Maniscalco M, Celentano L et al (2001) Abnormalities of renal endothelin during acute exacerbation in chronic obstructive pulmonary disease. Pulm Pharmacol Ther 14:321–327
Ozben B, Eryüksel E, Tanrikulu AM, Papila-Topal N, Celikel T, Başaran Y (2010) Acute exacerbation impairs endothelial function in patients with chronic obstructive pulmonary disease. Turk Kardiyol Dern Ars 38:1–7
Smeeth L, Cook C, Thomas S, Hall AJ, Hubbard R, Vallance P (2006) Risk of deep vein thrombosis and pulmonary embolism after acute infection in a community setting. Lancet 367:1075–1079
Gilmour PS, Rahman I, Donaldson K, MacNee W (2003) Histone acetylation regulates epithelial IL-8 release mediated by oxidative stress from environmental particles. Am J Physiol Lung Cell Mol Physiol 284:L533–L540
Acknowledgments
We gratefully acknowledge the statistical help provided by Dr. Dacheng Liu (Boehringer Ingelheim) and the editorial support of Natalie Dennis (PAREXEL).
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Halpin, D.M.G., Decramer, M., Celli, B. et al. Risk of Nonlower Respiratory Serious Adverse Events Following COPD Exacerbations in the 4-year UPLIFT® Trial. Lung 189, 261–268 (2011). https://doi.org/10.1007/s00408-011-9301-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-011-9301-8