
Abstract
Introduction
Although several studies have advocated the use of regional versus general anaesthesia as a means of reducing peri-operative complications from hip fracture surgery, the ideal method of anaesthesia remains controversial. Our purpose was to investigate the association between anaesthesia type and peri-operative complications in hip fracture surgery.
Methods
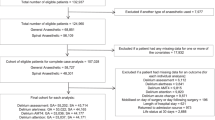
From the 2005–2011 ACS-NSQIP database, all patients with operatively treated hip fractures were identified using CPT codes, and fifteen peri-operative complications were recorded and categorized as either minor or major. Rates of minor, major, and total complications by anaesthesia type were compared using chi-square and Fischer’s exact tests. A multivariate model was used to determine odds of minor, major, and total complications between anaesthesia types. Multivariate analysis was then repeated after combining patients who received regional nerve blocks or spinal anaesthesia.
Results
A total of 7,764 hip fracture patients were included in our analysis. Spinal anaesthesia had the highest total complication rate (19.6 %), followed by general (17.9 %) and regional nerve blocks (12.6 %). Multivariate analysis demonstrated that spinal anaesthesia was associated with significantly greater odds of minor complications and total complications compared with general anaesthesia. After combining the regional nerve block and spinal anaesthesia groups, multivariate analysis again showed significantly greater odds of minor and total complications with regional versus general anaesthesia.
Conclusions
Using a large multi-centre database, we demonstrate that regional anaesthesia was associated with significantly greater odds of minor and total peri-operative complications compared with general anaesthesia. Our results challenge the notion that regional anaesthesia is the preferred method of anaesthesia for hip fractures in the elderly.
Similar content being viewed by others

References
Lyons AR (1997) Clinical outcomes and treatment of hip fractures. Am J Med 103:51S–63S, discussion S-4S
Koval KJ, Zuckerman JD (1994) Hip fractures: I. Overview and evaluation and treatment of femoral-neck fractures. J Am Acad Orthop Surg 2:141–149
Cooper C, Campion G, Melton LJ 3rd (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 2:285–289
Melton LJ 3rd, Thamer M, Ray NF et al (1997) Fractures attributable to osteoporosis: report from the National Osteoporosis Foundation. J Bone Miner Res 12:16–23
Schneider EL, Guralnik JM (1990) The aging of America. Impact on health care costs. JAMA 263:2335–2340
Roudsari BS, Ebel BE, Corso PS, Molinari NA, Koepsell TD (2005) The acute medical care costs of fall related injuries among the U.S. older adults. Injury 36:1316–1322
Vidan M, Serra JA, Moreno C et al (2005) Efficacy of a comprehensive geriatric intervention in older patients hospitalized for hip fracture: a randomized, controlled trial. J Am Geriatr Soc 53:1476–1482
Egol KA, Strauss EJ (2009) Peri-operative considerations in geriatric patients with hip fracture: what is the evidence? J Orthop Trauma 23(6):386–394
Covert CR, Fox GS (1989) Anaesthesia for hip surgery in the elderly. Can J Anaesth 36:311–319
Luger TJ, Kammerlander C, Gosch M, Luger MF, Kammerlander-Knauer U, Roth T, Kreutziger J (2010) Neuroaxial versus general anaesthesia in geriatric patients for hip fracture surgery: does it matter? Osteoporos Int 21(Suppl 4):S555–S572
Longo S (2000) Regional versus general anaesthesia. Curr Opin Anaesthesiol 13:539–543
Urwin SC, Parker MJ, Griffiths R (2000) General versus regional anaesthesia for hip fracture surgery: a meta-analysis of randomized trials. Br J Anaesth 84(4):450–455
Parker MJ, Handoll HH, Griffiths R (2004) Anaesthesia for hip fracture surgery in adults. Cochrane Database Syst Rev 4, CD000521
White SM, Moppett IK, Griffiths R (2014) Outcome by mode of anaesthesia for hip fracture surgery. An observational audit of 65 535 patients in a national dataset. Anaesthesia 69(3):224–230
Neuman MD, Silber JH, Elkassabany NM, Ludwig JM, Fleisher LA (2012) Comparative effectiveness of regional versus general anaesthesia for hip fracture surgery in adults. Anesthesiology 117(1):72–92
American College of Surgeons National Surgical Quality Improvement Program. User Guide for the 2011 Participant Use Data File. Available at: http://acsnsqip.org/main/programspecs/program_data_collection.jsp. Accessed 04 October 2013
Belmont PJ, Davey S, Orr JD, Ochoa LM, Bader JO, Schoenfeld AJ (2011) Risk factors for 30-day postoperative complications and mortality after below-knee amputation: a study of 2,911 patients from the National Surgical Quality Improvement Program. J Am Coll Surg 213(3):370–378
Martin CT, Pugely AJ, Gao Y, Wolf BR (2013) Risk factors for thirty-day morbidity and mortality following knee arthroscopy. J Bone Joint Surg Am 95(14):e98(1–10)
Pugley AJ, Martin CT, Gao Y, Mendoza-Lattes S, Callaghan JJ (2013) Differences in short-term complications between spinal and general anaesthesia for primary total knee arthroplasty. J Bone Joint Surg Am 95(3):193–199
Radcliff TA, Henderson WG, Stoner TJ, Khuri SF, Dohm M, Hutt E (2008) Patient risk factors, operative care, and outcomes among older community-dwelling male veterans with hip fracture. J Bone Joint Surg Am 90(1):34–42
Shoenfeld AJ, Ochoa LM, Bader JO, Belmont (2011) Risk factors for immediate postoperative complications and mortality following spine surgery: A study of 3475 patients from the National Surgical Quality Improvement Program. J Bone Joint Surg Am 93(17):1577–1582
Suleiman LI, Ortega G, Ong'uti SK, Gonzalez DO, Tran DD, Onyike A, Turner PL, Fullum TM (2012) Does BMI affect perioperative complications following total knee and hip arthroplasty. J Surg Res 174(1):7–11
Jones MJT, Piggott SE, Vaughan RS, Bayer AJ, Newcombe RG, Twining TC, Pathy J, Rosen M (1990) Cognitive and functional competence after anaesthesia in patients aged over 60: controlled trial of general and regional anaesthesia for elective hip or knee replacement. BMJ 300:1683–1687
Svartling N, Lehtinen AM, Tarkkanen L (1986) The effect of anaesthesia on changes in blood pressure and plasma cortisol levels induced by cementation with methylmethacrylate. Acta Anaesthesiol Scand 30:247–252
McKenzie PJ, Wishart HY, Smith G (1984) Long-term outcome after repair of fractured neck of femur; comparison of subarachnoid and general anaesthesia. Br J Anaesth 56:581–584
Le-Wendling L, Bihorac A, Baslanti TO, Lucas S, Sadasivan K, Wendling A, Heyman HJ, Boezaart (2012) A Regional anaesthesia as compared with general anaesthesia for surgery in geriatric patients with hip fracture: does it decrease morbidity, mortality, and health care costs? Results of a single-centered study. Pain Med 13(7):948–956
Parsons HM, Henderson WG, Ziegenfuss JY, Davern M, Al-Refaie WB (2011) Missing data and interpretation of cancer surgery outcomes at the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 213:379–391
Hamilton BH, Ko CY, Richards K, Hall BL (2010) Missing data in the American College of Surgeons National Surgical Quality Improvement Program are not missing at random: implications and potential impact on quality assessments. J Am Coll Surg 210(125–39):e2
Conflict of interest
Author William Obremskey has previously consulted for biometrics, done expert testimony in legal matters, has a grant from the Department of Defense, and has been a Board Member of the OTA and SEFC. For the remaining authors no conflicts of interest were declared.
Copyrighted material/consent forms
This study used no previously-copyrighted materials or signed patient consent forms.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
IRB approval
This study has approval from the Vanderbilt IRB.
Ethical review committee statement
This study was performed in accordance with the relevant regulations of the US Health Insurance Portability and Accountability Act (HIPAA) and the ethical standards of the 1964 Declaration of Helsinki.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 481 kb)
Rights and permissions
About this article

Cite this article
Whiting, P.S., Molina, C.S., Greenberg, S.E. et al. Regional anaesthesia for hip fracture surgery is associated with significantly more peri-operative complications compared with general anaesthesia. International Orthopaedics (SICOT) 39, 1321–1327 (2015). https://doi.org/10.1007/s00264-015-2735-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-015-2735-5