
Purpose:
To compare acute gastrointestinal (GI) and genitourinary (GU) toxicity between patient groups with localized prostate adenocarcinoma, treated with conventionally fractionated (CFRT) and hypofractionated (HFRT) three-dimensional conformal external-beam radiotherapy (3D-CRT).
Patients and Methods:
91 patients were enrolled into a randomized study with a minimum follow-up of 3 months. 44 men in the CFRT arm were irradiated with 74 Gy in 37 fractions at 2 Gy per fraction for 7.5 weeks. 47 men in the HFRT arm were treated with 57 Gy in 17 fractions for 3.5 weeks, given as 13 fractions of 3 Gy plus four fractions of 4.5 Gy. The clinical target volume (CTV) included the prostate and the base of seminal vesicles. The CTV-to-PTV (planning target volume) margin was 8–10 mm. Study patients had portal imaging and/or simulation performed on the first fractions and repeated at least weekly.
Results:
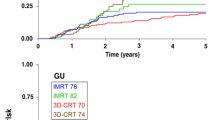
No acute grade 3 or 4 toxicities were observed. The grade 2 GU acute toxicity proportion was significantly lower in the HFRT arm: 19.1% versus 47.7% (χ2-test, p = 0.003). The grade 2 GU acute toxicity-free survival was significantly better in the HFRT arm (log-rank test, p = 0.008). The median duration of overall GI acute toxicity was shorter with HFRT: 3 compared to 6 weeks with CFRT (median test, p = 0.017).
Conclusion:
In this first evaluation, the HFRT schedule is feasible and induces acceptable or even lower acute toxicity compared with the toxicities in the CFRT schedule. Extended follow-up is needed to justify this fractionation schedule’s safety in the long term.
Ziel:
Es soll die Frage beantwortet werden, ob bei der Behandlung des lokalisierten Adenokarzinoms der Prostata ein hypofraktioniertes Schema (HFRT) die gleichen Tumorkontroll- und Nebenwirkungsraten zeigt wie ein konventionelles Schema (CFRT). Hier wird uber die ersten Ergebnisse zu den Nebenwirkungen berichtet.
Patienten und Methodik:
91 Patienten wurden im Rahmen einer Studie randomisiert behandelt, die minimale Nachbeobachtungszeit lag bei 3 Monaten. Im CFRT-Arm (44 Patienten) betrug die Dosis 74 Gy (37 × 2 Gy/d), im HFRT-Arm (47 Patienten) 57 Gy (17 × 3 Gy/d, 4 × 4,5 Gy/d). Das klinische Zielvolumen (CTV) umfasste die Prostata und die Basis der Samenblaschen, der Sicherheitsrand um das CTV betrug 8–10 mm. Verifikationsaufnahmen (EPI ["electronic portal imaging"]) wurden zu Beginn der Behandlung und danach wochentlich angefertigt.
Ergebnisse:
Nebenwirkungen der Grade 3 und 4 wurden nicht beobachtet. Die Rate an urologischen Grad-2-Nebenwirkungen war fur die HFRT mit 19,1% im Vergleich zu 47,7% bei der CFRT signifikant geringer (χ2-Test, p = 0,003). Auserdem traten die Grad-2-Nebenwirkungen im HFRT-Arm deutlich spater auf als im CFRT-Arm (Log-Rank-Test, p = 0,008). Gastrointestinale Grad-2-Nebenwirkungen hielten bei der HFRT im Median 3 Wochen, bei der CFRT 6 Wochen an (Mediantest, p = 0,017).
Schlussfolgerung:
In der ersten Auswertung zeigen sich Vorteile fur das HRFT-Schema in Bezug auf die Frequenz und die Dauer der Grad-2-Toxizitaten. Es ist aber eine langere Nachbeobachtungszeit notwendig, um dieses Schema als sicher akzeptieren zu konnen.
Similar content being viewed by others


References
Bohrer M, Schröder P, Welzel G, et al. Reduced rectal toxcity with ultrasound-based image guided radiotherapy using BAT? (B-mode acquisition and targeting system) for prostata cancer. Strahlenther Onkol 2008;184:674–678.
Brenner DJ, Martinez AA, Edmundson GK, et al. Direct evidence that prostate tumors show high sensitivity to fractionation (low α/β ratio) comparable to late-responding normal tissue. Int J Radiat Oncol Biol Phys 2 2002;52:6–13.
Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys 1995;31:1341–1346.
Dorr W, Jaal J, Zips D. Prostate cancer: biological dose considerations and constraints in tele- and brachytherapy. Strahlenther Onkol 2007;183:Suppl 2:14–15.
Fowler JF, Harari PM, Leborgne F, et al. Acute radiation reactions in oral and pharyngeal mucosa: tolerable levels in altered fractionation schedules. Radiother Oncol 2003;69:161–168.
Guckenberger M, Flentje M. Intensity-modulated radiotherapy (IMRT) of localized prostate cancer. A review and future perspectives. Strahlenther Onkol 2007;183:57–62.
Haustermans K, Fowler JF. A comment on proliferation rates in human prostate cancer [Letter]. Int J Radiat Oncol Biol Phys 2000;48:297.
Jereczek-Fossa BA, Cattani F, Garibaldi C, et al. Transabdominal ultrasonography, computed tomography and electronic portal imaging for 3-dimensional conformal radiotherapy for prostate cancer. Strahlenther Onkol 2007;183:610–6.
Joiner MC, Bentzen SM Baumann M. Time-dose relationships: the linearquadratic approach and the model in clinical practice. In: Steel GG, ed. Basic clinical radiobiology, 3rd edn. London: Arnold, 2002:120–146.
Junius S, Haustermans K, Bussels B, et al. Hypofractionated intensity modulated irradiation for localized prostate cancer: results from a phase I/II feasibility study. Radiat Oncol 2007;2:29–36.
Kitamura K, Shirato H, Shinohara N, et al. Reduction in acute morbidity using hypofractionated intensity-modulated radiation therapy assisted with a fluoroscopic real-time tumor-tracking system for prostate cancer: preliminary results of a phase I/II study. Cancer J 2003;9:268–276.
Kupelian PA, Reddy CA, Klein EA. Short-course intensity-modulated radiotherapy (70 Gy at 2.5 Gy per fraction) for localized prostate cancer: preliminary results on late toxicity and quality of life. Int J Radiat Oncol Biol Phys 2001;51:988–993.
Kupelian PA, Willoughby TR, Reddy CA. Hypofractionated intensity modulated radiotherapy (70 Gy at 2.5 Gy per fraction) for localized prostate cancer: Cleveland Clinic experience. Int J Radiat Oncol Biol Phys 2007;63:1424–1430.
Leborgne F, Fowler J. Acute toxicity after hypofractionated conformal radiotherapy for localized prostate cancer: nonrandomized contemporary comparison with standard fractionation. Int J Radiat Oncol Biol Phys 2008:72:770–776.
Lukka H, Hayter C, Warde P. A randomized trial comparing two fractionation schedules for patients with localized prostate cancer. Int J Radiat Oncol Biol Phys 2003;57:S126.
Madsen BL, His RA, Pham HT. Stereotactic hypofractionated accurate radiotherapy of the prostate (SHARP), 33.4 Gy in five fractions for localized disease: first clinical trial results. Int J Radiat Oncol Biol Phys 2007;67:1099–1105.
Martin JM, Bayley A, Bristow R. A prospective study of hypofractionated radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys 2006;66:S35–S36.
Martin JM, Rosewall TL, Bayley A, et al. Phase II trial of hypofractionated image-guided intensity-modulated radiotherapy for localized prostate adenocarcinoma. Int J Radiat Oncol Biol Phys 2007;69:1084–1089.
Polat B, Guenther I, Wilbert J, et al. Intra-fractional uncertainties in image-guided intensity-modulated radiotherapy (IMRT) of prostate cancer. Strahlenther Onkol 2008;184:668–673.
Pollack A, Hanlon AL, Horwitz EM, et al. Dosimetry and preliminary acute toxicity in the first 100 men treated for prostate cancer on a randomized hypofractionation dose escalation trial. Int J Radiat Oncol Biol Phys 2006;64:518–526.
Ritter MA, Forman JD, Kupelian PA, et al. A phase I/II trial of dose-per-fraction escalation for prostate cancer. Int J Radiat Oncol Biol Phys 2007;69:S174.
Siegel S, Castellan NJ Jr. Nonparametric statistics for the behavioral sciences, 2nd edn. New York: McGraw-Hill, 1988.
Soete G, Arcangeli S, De Meerleer G. Phase II study of a four-week hypofractionated external beam radiotherapy regimen for prostate cancer: report on acute toxicity. Radiother Oncol 2006;80:78–81.
van Tol-Geerdink JJ, Stalmeier PF, Pasker-de Jong PC, et al. Systematic review of the effect of radiation dose on tumor control and morbidity in the treatment of prostate cancer by 3D-CRT. Int J Radiat Oncol Biol Phys 2006;64:534–543.
Weiss W, Horninger W, Forthuber BC, et al. Single-institution results of primary external-beam radiation for the treatment of T1–T3 prostate cancer. Strahlenther Onkol 2007;183:321–326.
Yeoh EE, Fraser RJ, McGowan RE. Evidence for efficacy without increased toxicity of hypofractionated radiotherapy for prostate carcinoma: early results of a phase III randomized trial. Int J Radiat Oncol Biol Phys 2003;55:943–955.
Zelefsky MJ, Fuks Z, Hunt M, et al. High dose radiation delivered by intensity modulated conformal radiotherapy improves the outcome of localized prostate cancer. J Urol 2001;166:876–881.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Norkus, D., Miller, A., Kurtinaitis, J. et al. A Randomized Trial Comparing Hypofractionated and Conventionally Fractionated Three-Dimensional External-Beam Radiotherapy for Localized Prostate Adenocarcinoma. Strahlenther Onkol 185, 715–721 (2009). https://doi.org/10.1007/s00066-009-1982-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-009-1982-z