Article Text

Abstract
Objectives Depression has been reported to be a risk factor of cardiovascular disease in the western world, but the association has not yet been studied among Asian populations. The aim of this study was to investigate whether depression increases the risk of developing atherosclerotic cardiovascular disease (ASCVD) in a large Korean cohort study.
Design Population based cohort study.
Setting Database of National Health Insurance System, Republic of Korea.
Participants 481 355 Koreans (260 695 men and 220 660 women) aged 40–80 years who had a biennial health check-up between 2002 and 2005.
Main outcome measure The main outcome in this study was the first ASCVD event (hospital admission or death).
Results Depression increased the risk of developing ASCVD by 41% for men and 48% for women. In men, 3–4 outpatient visits for depression increased the risk of angina pectoris by 2.12 times (95% CI 1.55 to 2.90) and acute myocardial infarction by 2.29 times (95% CI 1.33 to 3.95). Depression was also associated with stroke in men (HR 1.29, 95% CI 1.19 to 1.39) and in women (HR 1.37, 95% CI 1.29 to 1.46). However, no increased risk of ASCVD was found for men who received 10 or more depressive treatments, compared with those without any outpatient visit for depression.
Conclusions In this cohort, depressed people were at increased risk of ASCVD incidence. Therefore, individuals with depression may need routine monitoring of heart health that may prevent their future CVD risk.
- depression
- cardiovascular disease
- body mass index
- socioeconomic status
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Depression was defined as the presence of objective data such as outpatient visit and antidepressant prescription rather than categorisation by self-reported questionnaire scores.
The usage of mean value of multiple measurements allowed us to minimise measurement error of exposure variables.
This prospective study is the virtually complete follow-up for fatal and non-fatal events identified from national insurance claims.
Since non-fatal events are insurance claim data, their accuracy has been controversial.
Findings of this study may not be generalisable to other ethnic groups.
Introduction
Depression or depressive symptoms have been linked to increased cardiovascular disease (CVD), including coronary heart disease and stroke.1–4 A growing body of evidence suggests that the impact of depressive symptoms on CVD may differ by race, with depressive symptoms conferring an elevated risk for CVD in African-Americans, compared with whites.5 6 However, less is known about the experiences of people from Asian countries.
Depression is an increasingly common illness in Korea, with a gradual increase in the prevalence of depression over the past decade (2001, 4.3%; 2011, 6.7%).7 8 This might be due to the fact that Korea has undergone unprecedented economic growth and faced multiple changes since 2000. In fact, Korea has the second highest suicide rate among developed countries.9 Despite the potential relevance of depression as a risk factor for CVD risk in Korean population, few studies have examined the association between depression and important clinical endpoints, such as CVD mortality.
The importance of psychosocial factors of CVD risk among persons with low socioeconomic status (SES) has also been increasingly appreciated.10–12 In the Reasons for Geographic and Racial Differences in Stroke study, participants with both depressive symptoms and stress had the greatest risk of incident CVD events and death only for those with low income (<$35 000) and not with higher income.12
Using data from a large-scale cohort study, we examined whether depression increases the risk of atherosclerotic CVD (ASCVD) independently of existing cardiac risk factors. We also assessed whether SES modifies the association between depression and ASCVD risk.
Methods
Study Population
The study population is a representative sub-sample of subjects who undertook national health screening programme provided by National Health Insurance System (NHIS). NHIS has provided repeat health screenings every 2 years to 500 000 people who received health screenings between 2002 and 2003. Among these 500 000, the study selected 481 355 participants who were repeatedly screened between 2004 and 2005. Participants were excluded from the analyses if they had a record of admission or outpatient for CVD from 2002 to 2005. Hospital diagnoses were reported to the study and coded to the WHO’s International Classification of Diseases, 10th Revision (ICD-10) (WHO, 1992).
Measurement variables
Height and body weight were measured as anthropometric variables. Body mass index (BMI) was calculated by dividing body weight (kg) by the square of height (m). Blood pressure was measured by a trained technician using an automatic sphygmomanometer or mercury sphygmomanometer. All those who participated in the national health screening provided by NHIS were asked to be fasted until the morning after dinner the previous day. The variables measured through fasting blood were total cholesterol, blood glucose and liver function tests. For those who had multiple measurements for the same continuous variables, we used their mean measurement to reduce measurement error. Each health examination centre had internal and external quality control procedures directed by the Korean Association of Laboratory Quality Control. Agreement for each biomedical marker across individual hospital was high (correlations coefficients range 0.96–0.99).13
Participants completed a questionnaire that included questions on their health status and life style factors such as smoking status, alcohol drinking and exercise. We examined smoking status using the first survey data, or where there was missing in the first survey, the second survey data. In this study, medical premiums were regarded as a proxy for SES because, in Korea, medical insurance premiums are given in proportion to social and economic levels. Depression was defined as the hospital outpatient use and diagnosis of depression (ICD-10 codes F32-F33) or history of medication for depression.
Assessment of depression
Participants were classified as depressed if they had at least one outpatient visit due to depression (ICD-10 codes F32-F33) or were prescribed depression medication at more than three visits. Between 2002 and 2005, 13 antidepressants were listed in the medication database at the health insurance review and assessment service: the medications included sertraline, paroxetine, fluvoxamine, citalopram, mirtazapine, trazodone, phenelzine imipramine, amitriptyline, nortriptyline, amoxapine, lofrepramine and tianeptine.
Outcomes
We defined incident ASCVD as the first hospital admission with a diagnosis of ASCVD (ICD-10 codes), or, where there was no relevant hospital admission, death due to ASCVD as the underlying cause (ICD-10 codes). The detailed outcomes used in this study include ischaemic heart disease (IHD) (ICD-10 codes I20-I25), stroke (ICD-10 codes I60-I69) and other CVD (ICD-10 I10-I15, I70-I74, R96, I50, I51, I44-I49). IHD was further divided into angina pectoris and acute myocardial infarction. Stroke was divided into ischaemic and haemorrhagic stroke.
All ASCVD events or detailed outcome data for hospital records were available from NHIS for participants at baseline (2002–2005) from 1 January 2006 to 31 December 2013. Information on causes of death for the participants was confirmed by the National Statistical Office.
A validation study was conducted in collaboration with the Korean Society of Cardiology through the formation of the Event Validation Committee (July 2008–May 2009). For participants who provided written permission for the use of their personal information, 673 coronary heart disease events between 1994 and 2007 were confirmed with individual hospital medical records, and 73% of the cases of myocardial infarction were validated.14 Another study reported that 83% of stroke diagnoses were validated among a sample of 626 stroke patients.15
Statistical analysis
First, descriptive analyses of distribution of depression by general characteristics and cardiac risk factors were conducted in men and women.
Second, the age-adjusted incidence rate of ASCVD per 100 000 person-years was calculated by the number of outpatient visits due to depression (None, 1–2, 3–4, 5–9 and 10 or more). The incidence rate was standardised to the age distribution of Korean national population in 2000.
Third, Cox regression models were used to estimate hazard ratios (HRs) and the 95% cCIs. The independent effects of depression on ASCVD were analysed by adjusting for known risk factors for ASCVD: age, smoking status, hypertension, hypercholesterolaemia, diabetes and chronic renal failure. We also evaluated the proportional hazards assumption based on Schoenfeld residuals test. In order to avoid reverse causation bias attributable to underlying diseases, we analysed the events after excluding the first 2 years of follow-up.
Lastly, we investigated the effect of the interaction between depression and SES on the development of ASCVD events. Participants were classified into six groups reflecting psychosocial risk at baseline: (1) no depression and high SES, (2) no depression and middle SES, (3) no depression and low SES, (4) depression and high SES, (5) depression and middle SES and (6) depression and low SES. Analyses were conducted using SAS software V.9.4 (SAS institute).
Patient and public involvement
Neither patients nor members of the public were involved in this study.
Results
General characteristics
Table 1 summarises the characteristics of the study population at baseline by sex and depression. In this study, 4.9% of males and 10.0% of females had at least one outpatient visit for depression during baseline years or were prescribed depression medication at more than three visits (table 1). The majority of participants (96.9%) had no outpatient visit. The most frequent outpatient visit was 1–2 times (1.64%), followed by 3–4 times (0.43%), 5–9 times (0.42%) and at least 10 and more visits (0.61%) (data not shown).
General characteristics of study participants at baseline (2002–2005)
The overall mean age was 52.8 years (52.0 years for men and 53.7 years for women). The mean age of the participants with depression was higher in both men and women than that of those with no depression. The mean BMI was 24.0 kg/m2 for both men and women. There was no difference in BMI by depression status. The levels of systolic blood pressure, diastolic blood pressure and fasting blood glucose were higher in men, whereas women had higher total cholesterol levels than men. In men and women, the prevalence of diabetes mellitus was higher in those with depression. The overall current smoking rate was 24.2% (42.4% for men and 2.8% for women).
Depression and ASCVD risk
During a median follow-up of 8 years (3 557 303 person years), 40 813 ASCVD (5570 fatal), 16 915 IHD (1645 fatal) and 17 846 stroke (2584 fatal) occurred. Participants with depression at baseline had a higher risk of developing heart disease during the 8-year follow-up period (see online supplementary figures 1 and 2) than those with no depression. Table 2 shows the risk of developing ASCVD by the number of depression outpatient use in men. Overall, the risk of ASCVD was 41% higher among men with at least one outpatient visit for depression compared with those with no outpatient visit at baseline (HR=1.41; 95% CI 1.34 to 1.48). The risk of ASCVD increased with increasing number of outpatient visits but not for those with ≥10 visits. In particular, 3–4 outpatient visits for depression had the strongest effects on developing angina pectoris (HR=2.12; 95% CI 1.55 to 2.90) and acute myocardial infarction (HR=2.29; 95% CI 1.33 to 3.95), compared with no visit history. Similar to the overall ASCVD, the risk of developing angina pectoris was lower (but still significant) in participants who had 10 or more visits for depression, compared with those who had nine or less visits. While there was no association of depression with haemorrhagic stroke, the association appeared to be significant with total stroke (HR=1.29; 95% CI 1.19 to 1.39) and ischaemic stroke (HR=1.05; 95% CI 1.03 to 1.07).
Supplemental material
Age-adjusted incidence rate per 100 000 person-year and HR for various cardiovascular events by depression level in Korean men, 2006–2013
Table 3 shows the results for women. The overall results were similar to those of men. The overall risks of total stroke or ischaemic stroke were significantly higher in depressed patients. Likewise, there was no association with haemorrhagic stroke.
Age-adjusted incidence rate per 100 000 person-year and HR for various cardiovascular events by depression level in Korean women, 2006–2013
Depression and ASCVD risk by SES
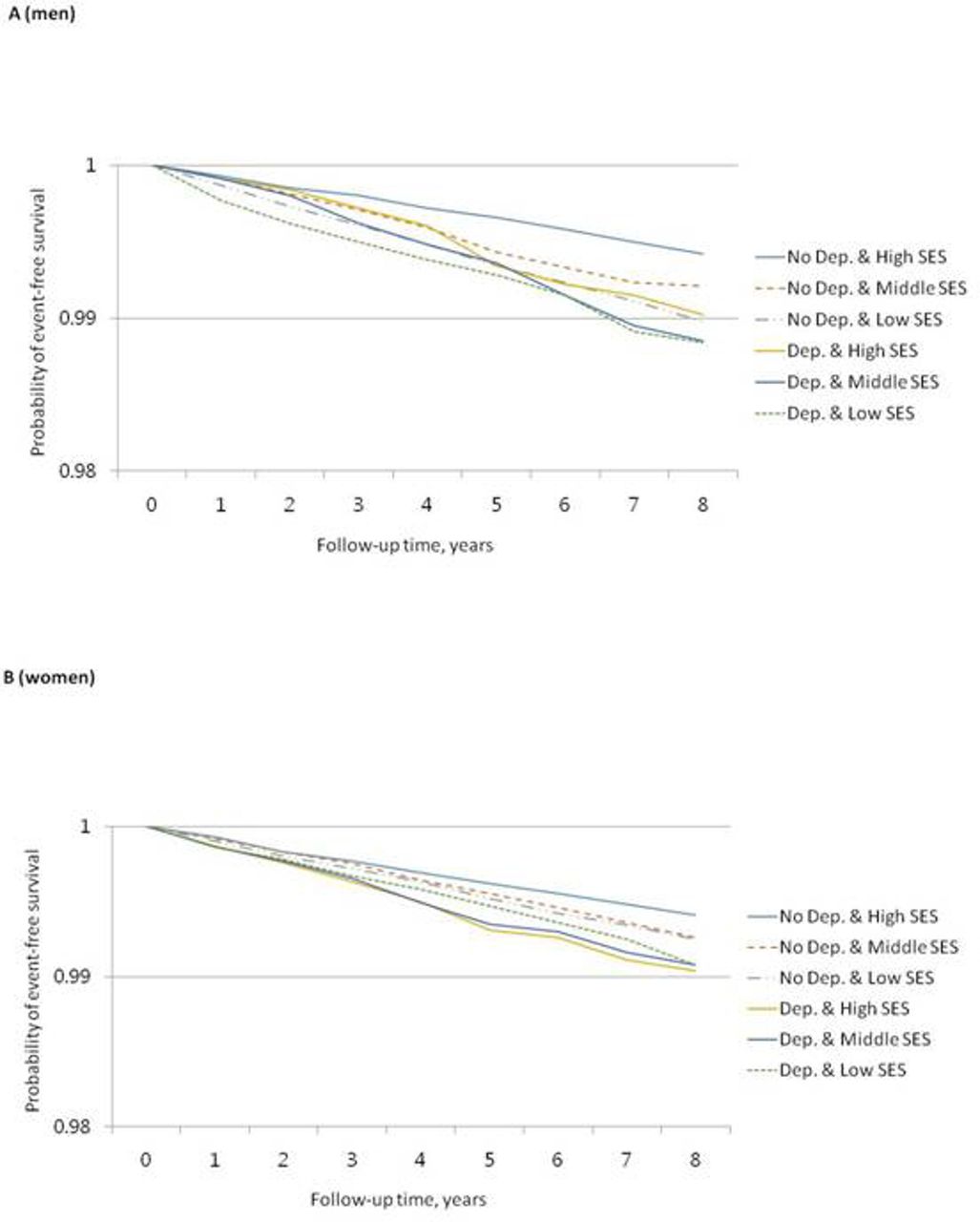
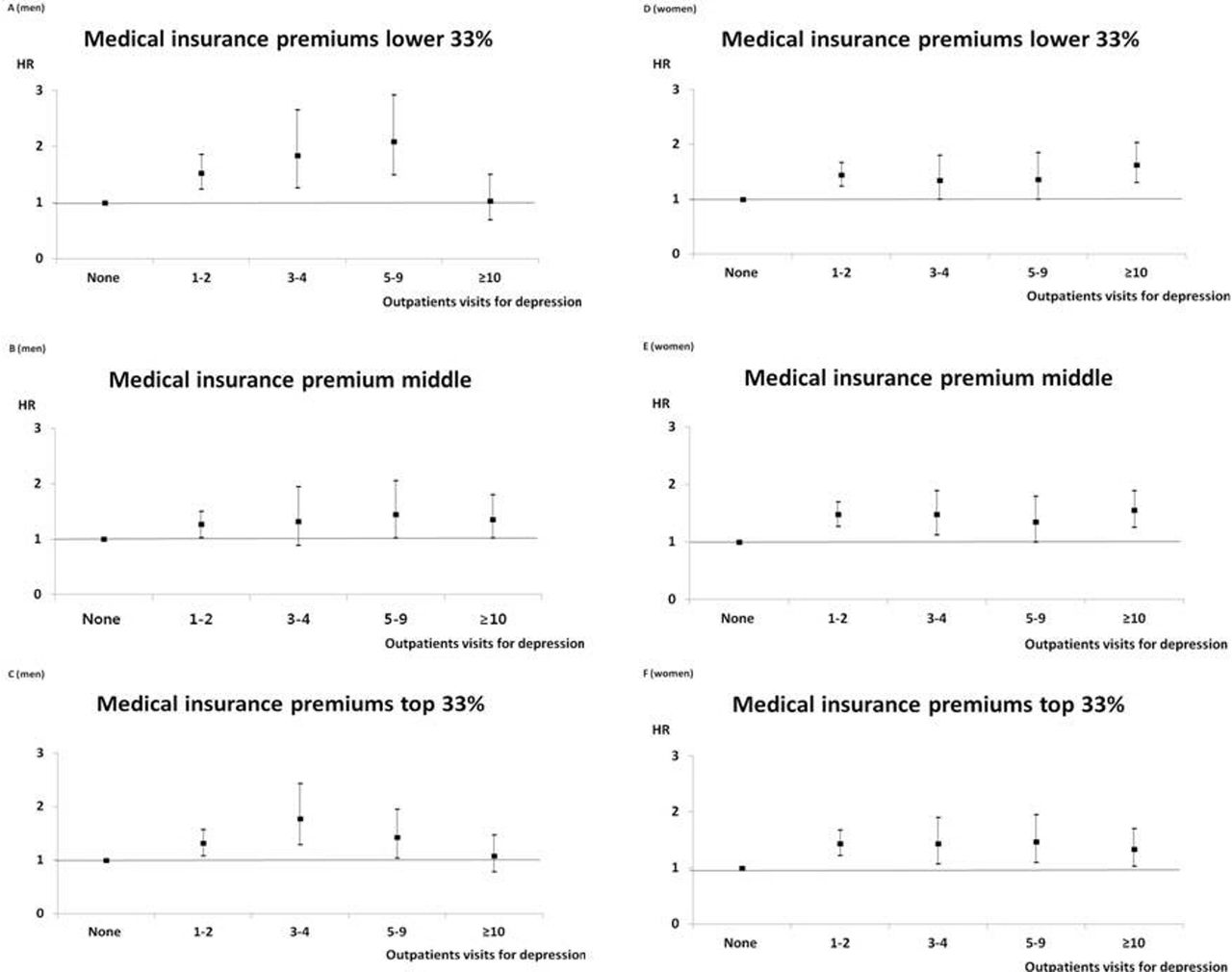
Figure 1 shows how medical insurance premium as a surrogate for SES modifies the association between depression and the risk of developing ASCVD in men and women. For men with low (bottom tertile) or high (top tertile) SES, the risk of ASCVD increased with increasing number of outpatient visits but flattened. In these SES groups, the ASCVD risk did not reach statistical significance when the number of outpatient visits was 10 or more. Women who had at least one outpatient visit were at high risk of ASCVD in all SES groups. Figure 2 shows combination effects of depression and SES at baseline on the development of heart disease. In men, depression-free group had a reduced survival in low SES group, while depressed group showed a reduced survival in middle or low SES group. Depressed women showed a reduced survival, regardless of their SES at baseline.

Depression treatment frequency and atherosclerotic cardiovascular disease risks according to socioeconomic level. The socioeconomic level is divided into three levels according to the level of medical insurance premiums.
{kind=link}
{kind=link}
Probability of atherosclerotic cardiovascular disease event-free survival according to depression and socioeconomic level. The socioeconomic level is divided into three levels according to the level of medical insurance premiums. SES, socioeconomic status.
Discussion
The study found that depression in general population of Korea increased the risk of ASCVD with about 40%. In men, depression increased the risk of angina pectoris and acute myocardial infarction by up to twofold. However, even if participants had depression at baseline, the risk of developing ASCVD was not increased as long as they had at least 10 outpatient visits for depression. This finding was similarly observed in low or high SES group in men. However, the risk of ASCVD was high in women with depression in all SES groups.
Overall, the results of this study were consistent with previous studies. The main finding of our study was that the risk of heart disease was not increased when men received 10 or more depressive treatments during the follow-up periods. In women, however, the risk of ASCVD was high in those with depression, regardless of the number of visits or SES levels. A possible explanation for this finding is that most women in the study were postmenopausal women (with mean age of 52.8 years at baseline) who were at increased risk of CVD. The results suggest that the risk of ASCVD may not be modified by the number of outpatients or SES levels in depressed middle-aged women.
Depression has been linked with various behavioural risk factors such as smoking, obesity, diabetes and metabolic syndrome.16 17 A comprehensive review concluded that obesity, hyperlipidaemia, hypertension and diabetes are now perceived as important comorbid conditions in depressed patients.18 It is also known that patients with depression are less likely to adhere to medical recommendations, contributing to poor health outcomes.19 20 In addition, depressed people have maladaptive coping style, social isolation and chronic life stress.21–23
The mechanisms underlying the association between depression and cardiovascular risk remain poorly understood. Increased platelet reactivity has been associated in cross-sectional studies.24 A cross-sectional study revealed that depression and anxiety enhanced platelet aggregation, which can cause recurrent acute coronary syndrome in secondary prevention.25 Further research is needed to determine whether depression directly increases these cardiovascular events or whether this association is mediated by the risk factors of CVD, such as elevated blood pressure, cholesterol or blood glucose.
In our study, only 4.9% of males and 10.0% of females visited outpatients for depression during baseline period (2002–2005). Similarly, the prevalence of depression with Patient Health Questionnaire 9 was 4.2% for males and 9.1% for females according to the Nationally Representative Survey of Korea National Health and Nutrition Examination Survey.25 ,26 The prevalence of depression is low in Korea, and even if people are aware of their depression, the actual rate of treatment is likely to be very low. Moreover, the rate of continuing treatment of depression is expected to be even lower. We therefore suggest that regular outpatient visits may serve as a basis for the prevention of the risk of developing ASCVD. Further studies are needed to verify the true association between depression and ASCVD with long-term follow-up.
The main strength of this prospective study is the virtually complete follow-up for diseases and deaths in a large study population. Moreover, the usage of mean value of multiple measurements allowed us to minimise measurement error of exposure variables. Another strength of this study is the presence of objective data such as outpatient visit and antidepressant prescription for defining depression rather than categorisation by self-reported questionnaire scores.
Nonetheless, this study has some limitations. In this study, events of CVD were confirmed by NHIS hospitalisation data. Since these data are insurance claim data, their accuracy has been controversial. We have conducted two studies on the validity of the data for heart disease and stroke. According to previous validation studies, the validity of acute myocardial infarction was higher than 90%, and that of stroke was 83%.14 15 However, validity study of angina has not yet been reported. Therefore, we believe that classification errors for the outcome may still exist. In general, if classification errors exist, the association of exposure variables and outcomes tends to toward the null. In this study, whether the weak association with stroke was genuinely relevant or due to classification errors should be carefully examined. Another limitation of our study is that the number of visits with depression ICD-10 code is being used as a proxy for severity of depression. In fact, more visits could actually mean better treated depression, which may be why greater than 10 or more outpatient visits does not correspond to increased ASCVD risk in our study. On the other hand, the lack of increased risk may indicate proper treatment of depression reduces ASCVD risk, and 10 or more visits for depression is a surrogate endpoint of treatment compliance, of attending the follow-up visits with their doctor and in general of proper mental treatment. However, further studies with longer term follow-up should be conducted to elucidate an exact endpoint of proper mental treatment.
Conclusions
In this large Korean cohort, depression increased the risk of ASCVD incidence by around 40%. Therefore, men and women with depression may need routine monitoring of heart health that may prevent their future CVD risk.
Acknowledgments
The authors thank the staff of the Korean National Health Insurance Service.
References
Footnotes
Contributors Substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work: YHJ, HYC, SHJ and KJJ. Drafting the work or revising it critically for important intellectual content: YHJ, HYC. Final approval of the version to be published: KJJ. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: YHJ, HYC, SHJ and KJJ.
Funding This study was funded by a grant of the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (HI14C2686).
Competing interests None declared.
Ethics approval All study participants provided general consent to take part in the study at the time of their health screening. International review board approval was provided by Severance hospital (4- 2017-0051).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Patient consent for publication Not required.