Article Text

Abstract
Objectives Global self-rated health (SRH) has become extensively used as an outcome measure in population health surveillance. The aim of this study was to analyse the effects of age and secular trend (year of investigation) on SRH.
Design Prospective cohort study, using population-based data from eight ongoing cohort studies, with sampling performed between 1973 and 2003.
Setting Sweden.
Participants 11 880 women and men, aged 25–99 years, providing 14 470 observations.
Primary outcome measure Global SRH.
Results In multiple ordinal logistic regression analyses, adjusted for the effects of covariates, there were independent effects of age (p<0.0001) and of year of investigation (p<0.0001) on SRH. In women the association was linear, showing lower levels of SRH with increased age, and more recent year of investigation. In men the association was curvilinear, and thus more complex. The final model explained 76.2% of the SRH variance in women and 74.5% of the variance in men.
Conclusions SRH was strongly and inversely associated with age in both sexes, after adjustment for other outcome-affecting variables. There was a strongly significant effect of year of investigation indicating a change in SRH, in women towards lower levels over calendar time, in men with fluctuations across time.
- Public Health
- Epidemiology
- Statistics & Research Methods
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
To investigate the effects of age and secular trends on self-rated health (SRH) adjusted for the effects of a wide range of potential confounders in a large population-based study of adult women and men.
Key messages
-
SRH is affected by age but differently in men and women.
-
There is a secular trend regarding SRH, such that SRH was poorer in more recent years of investigation, after controlling for age and a large number of potential confounders.
-
The secular trends differed among women and men.
Strengths and limitations of this study
-
Strengths included a large sample size and observation time which spanned three decades in men and one decade in women.
-
Limitations included that all age groups were not represented on each measurement occasion, and data were generally cross-sectional.
Introduction
Global self-rated health (SRH), a one-item simple question in which respondents are asked to rate their overall health, has predictive validity in relation to functional ability,1 healthcare utilisation,2 morbidity3 and mortality.4 ,5 Owing to the simplicity of use, and predictive validity held in relation to future health SRH has increasingly become used as an outcome measure in medical health research, and in population health surveillance.
A number of factors are known to influence SRH. The relation to age is somewhat controversial. Non-comparative SRH has been found to decrease with age,6–11 although better SRH among the oldest old 12 ,13 and no association between age and SRH,14 has also been reported.
Age reflects effects of biological processes of ageing internal to the individual, and effects of contextually determined factors of importance to health and well-being.15 ,16 Although increased knowledge concerning effects of contextually determined factors on SRH may have important public health implications, studies investigating effects of cohort or year of investigation on health are few, and results inconclusive. Poorer SRH, as well as better SRH, in more recent cohorts, and little change between cohorts in age-specific SRH, has been reported.6 ,11 ,16–19
The aim of this study was to investigate the effects of age (individual) and secular trends, measured as year of investigation (contextual), on SRH, adjusted for the effects of a wide range of potential confounders, in a large population-based study of adult women and men.
Methods
Study population
Analyses were based on data from eight ongoing Swedish cohort studies, with baseline investigations performed between 1973 and 2003. The study population has previously been described in detail.20 ,21 Briefly, random samples based on predefined specifications concerning age, sex and area of residence, were drawn from the national population register. The men born in 1913 subsample consisted of a random third of the male population aged 60 in the city of Gothenburg, Sweden, in 1973, and the men born in 1923 subsample consisted of a random 10th of the male population aged 50 in Gothenburg (table 1). Survivors in the samples were invited to re-examinations in 1980, 1988 and 1993.
Characteristics of the cohorts included in the study population
The men born in 1943 subsample consisted of a random third of 50-year-old men living in Gothenburg in 1993, re-examined in 2003, and the women and men born in 1953 subsamples consisted of a random third of women and men living in Gothenburg in 2003. The Eskil subsample consisted of a random sample of 625 men aged 30–54 and living in the city of Eskilstuna, Sweden in 1986. The Uppsala Public Health Cohort was based on random samples of 1000 men and women 25 years or older from each of the six municipalities of Uppsala County in 1993. The BEDA II subsample was based on a re-examination in 1997 of a random sample drawn in 1979 of 1746 women born during 1915–1941 and living in Gothenburg. The Uppsala-Örebro Women Study sample was based on random samples of 600 women aged 35–64 from each of the seven counties in the Uppsala-Örebro Health Care Region, Sweden.
All samples were by definition representative of their underlying general populations. No exclusions were made. The combined samples consisted of 20 160 subjects of whom 3590 were part of more than one subsample. Overall, 14 470 (71.8%) observations were obtained, based on 12 000 unique individuals. Of these 10 451 (6808 women and 3644 men) participated once, 964 men twice, 254 men three times and 330 men on four occasions. Additional information on the study population is given in table 1.
Measurements
The data used in this report were obtained by questionnaire. For the variables used here the same questionnaires were used in all studies. Educational level was classified on a four-point scale ranging from ‘compulsory education only’ (=1), to ‘college or university education’ (=4). Occupational status was measured on a four-point nominal scale as ‘gainfully employed’ (including students), ‘unemployed’, ‘on sick leave or disability pension’ or ‘old age retirement’. Marital status was classified as married/cohabiting or not (the latter including response alternatives never married, divorced and widowed).
SRH was measured using the well-being subscale of The Gothenburg Quality of Life instrument (GQL).22 Respondents were asked to rate their health on a seven-point Likert scale with response alternatives ranging from ‘very poor’ (=1) to ‘excellent, could not be better’ (=7), with no verbal labels for the intervening steps. Symptom reporting was assessed based on the Complaint score subscale of GQL, in which subjects are asked ‘Have you been troubled by any of the following symptoms during the past 3 months?’, followed by a list of 30 general symptoms with response alternatives ‘yes’ (=1) or ‘no’ (=0) for each symptom. The Complaint score was obtained as the sum across the 30 symptoms. Complaint score is not intended to measure specific diseases, but rather the tendency to report symptoms, an aspect of quality of life.
Leisure time physical activity was reported on a four-point ordinal scale with response alternatives ‘sedentary’, ‘moderately active’, ‘active’ or ‘vigorously active’.23 Smoking habits were classified as ‘current smoker’ or ‘non-smoker’ (including never smoked and ex-smoker). In addition, in some of the cohorts a five-point smoking variable was available, where smoking habits were classified as ‘never smoked’ (=1), ‘ex-smoker’ (=2), ‘currently smoking 1–14 g of tobacco per day’ (=3), ‘smoking 15–24 g/day’ (=4), or ‘smoking 25 g or more per day’, with one cigarette equalling 1 g, one cheroot 2 g, one cigar 5 g and pipe tobacco 50 g, divided by the number of days the pack lasted.23
Ethical considerations
Informed consent was obtained from all participants, verbal in the earlier studies, and written later on, as required first by the Research Ethics Committees at Gothenburg and Uppsala Universities and later by the National Research Ethics Board, that approved the study.
Statistical analyses
Data were analysed using the SAS software, V.9.2 24 Data concerning age, sex and examination year were complete, except for one individual where age was missing. Not all variables were measured in all subpopulations. The number of available observations for each variable is shown in table 2. The overall proportion of missing data in subpopulations where the variables were measured was less than 2%. Missing data were not replaced. Simple differences between groups were assessed with Student's t test or the χ2 test.
Characteristics of the study population
To make full use of SRH as a seven-level ordinal variable, multiple ordinal logistic regression was used, providing cumulative OR across the seven SRH levels for each independent variable, CI and Wald's χ2 estimates. The latter is the test parameter and may thus be used to rank the impact or importance of the independent variables on SRH.
The analyses were performed in two steps. In the first step, screening bivariate ordinal logistic regression analyses were performed to identify candidate variables for the final multiple regression model. There were no significant differences in results depending on whether the five-point ordinal smoking variable or the dichotomous smoking variable was used. Since the dichotomous variable was more complete, it was used throughout the analyses.
In the second step, two models were used, one based on age and year of investigation only and the other on all significant variables from step one entered as independent variables. The final full-scale model was based on multiple ordinal logistic regression with backward elimination of non-significant covariates. Possible non-linearity of the effects of age and year of investigation on SRH in the two models was tested by inclusion of the variables age and year of investigation, respectively, raised to the power of 2 and 3 (second-degree and third-degree polynomial functions). Moreover, potential effects of interaction between age and year of investigation were tested, but found to be non-significant.
Two measures of degree of explanation were provided by the SAS logistic procedure, one based on concordance between observed and model computed results, the other based on the receiver operator characteristics (ROC) method. The model fit between crude age and the year of investigation on SRH results and those computed in the final analytical model was assessed by scrutiny and found to be excellent.
The full-scale regression model was also tested with linear regression analysis. The results were generally the same as with ordinal logistic regression, but with somewhat lower statistical power. However, the result from the multiple linear regression model was used to compute the regression surfaces in figure 1. All tests were two-tailed. Significance levels were set at p<0.10 in the first, screening analysis step, and p<0.05 in the second, final analysis step.
{kind=link}
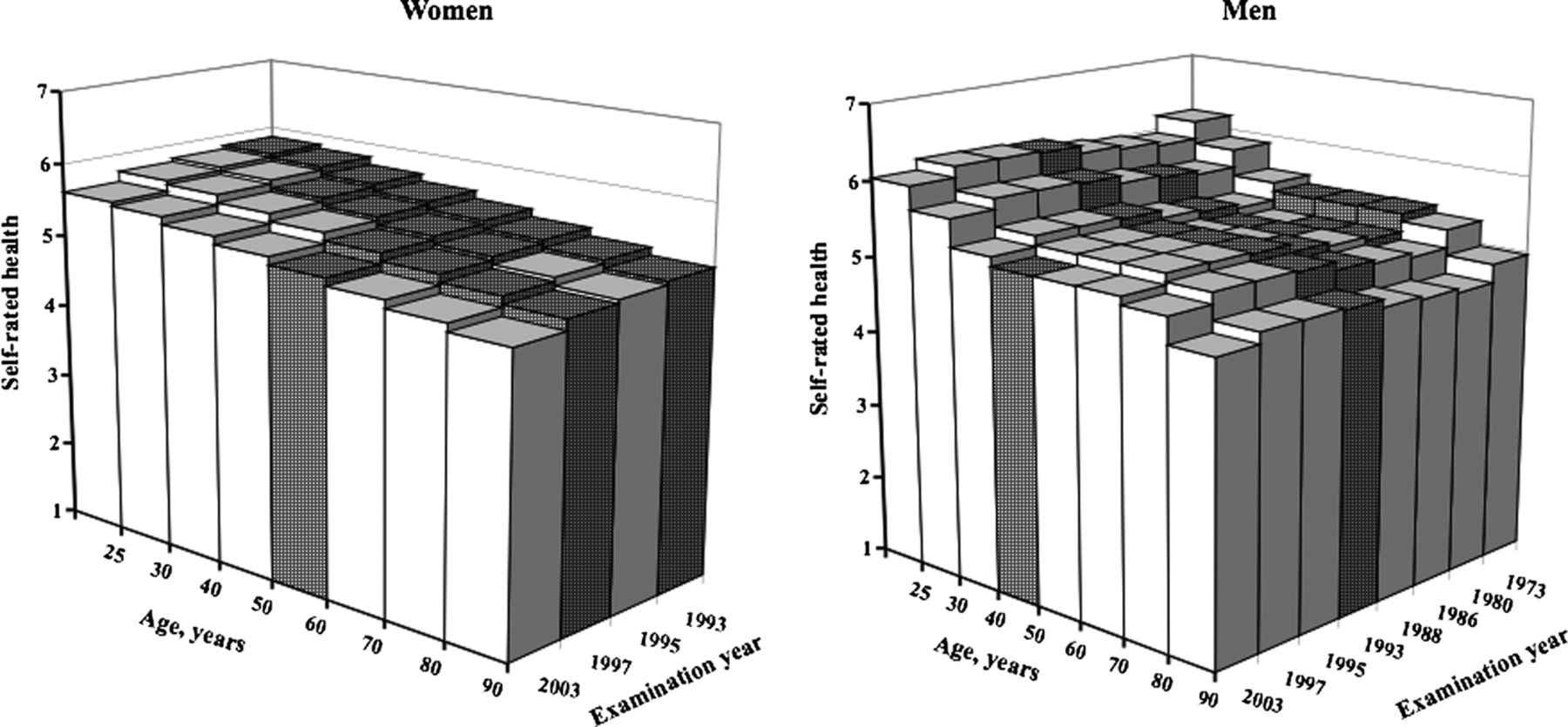
Association between age, year of investigation (proxy for secular trend) and self-rated health (SRH) in women and men, adjusted for the influence on SRH of education, physical exercise during leisure time, marital status, complaint score, on sick leave/disability pension and being unemployed. Dark bars=data available, white bars=no data available.
Results
Characteristics of the study population
Study population characteristics are presented in table 2. The mean age was 54.5 years. Approximately one-quarter of the study population reported college or university education, the majority were employed and married or cohabiting. One-quarter of the participants reported current smoking, and approximately 80% were sedentary or moderately physically active during leisure time. Mean level of SRH was 5.4 (range 1.0–7.0), and mean complaint score 6.1 (range 1.0–30.0). Women were significantly younger than men, had higher level of education, were less often married/cohabiting, less often current smokers, less physically active, reported more symptoms and had lower SRH levels than men.
Effects of age and year of investigation on SRH
In table 3, the effects on SRH of age and year of investigation are shown in women and men according to two models. In model 1, age was significantly inversely associated with SRH in both sexes (p<0.0001), as was year of investigation in women according to a second-degree and in men according to a third-degree polynomial function (non-linear relationships).
Effects of age and year of investigation on self-rated health (SRH), based on ordinal logistic regression models
In model 2, the linear association between age and SRH among women remained significant (p<0.0001), as did year of investigation, when the covariates were entered into the final model. In men, age and year of investigation, both according to a third-degree polynomial function remained significant, when the covariates were entered in the model.
Table 3 also shows Wald χ2 estimates, indicating the rank order of variable impact on SRH. In both sexes complaint score had the highest impact on SRH of all variables, followed by sick leave or disability pension, leisure time physical activity, marital status and, finally, education among women and unemployment among men. The final regression model explained 76.2% of the SRH variance in women, and 74.5% of the SRH variance in men.
Effect of participating in more than one investigation
All women participated only once, but 1548 men participated in more than one examination. An analysis was therefore made with all 1548 male observations from more than one examination, and one with the 3644 men who participated only once. The results were almost identical, the only difference being that in analyses of those participating only once age was significant but year of investigation was not (because of no intraindividual variation?) and among those participating more than once age was non-significant, while year of investigation was.
Effects of time differences
The observations on women covered a shorter time period (1993–2003) than those on men (1973–2003). To explore if this time difference could explain the difference in time trends between men and women an analysis was performed among men with data covering the time period 1993–2003. The results showed the same determinants for men as those shown in table 3 and thus a curvilinear time trend, as opposed to the linear trend in women.
Visualisation of the analysis model
In figure 1 the analysis model is visualised. In women mean SRH levels fell gradually and linearly from 5.5 among the youngest to 4.6 among the oldest women. Furthermore, mean SRH levels fell across year of investigation, from 5.2 in 1993 to 4.9 in 2003. In men, the association between age and year of investigation on the one hand, and SRH on the other followed a third-degree polynomial function with peaks at 25 years of age and at the age interval 50–70 along the age axis, as well as in 1973 and in the late 1990s along the year of investigation axis.
Discussion
In line with a majority of previous studies investigating effects of age on SRH in adult population-based studies,6 ,11 ,16 in this population-based study of 12 000 adult women and men, there was a significant, independent relationship between SRH and age in both sexes, resulting in lower SRH with increasing age. The association was independent of year of investigation and remained when adjusted for socio-demographic variables, lifestyle variables and complaint score. In women the association between SRH and age followed a linear function. In men the association was more complex. In a recent study, based on employees from the French national gas and electricity company an overall pattern of age-related gradual decline in SRH was observed, with distinctly better SRH observed in women and men during the year preceding and the year following retirement from the work force.8 In the present population-based study, no distinct changes in SRH around retirement age were observed, which suggests that the suggested associations between retirement and SRH may apply in specific populations and contexts, but not necessarily in the population as a whole.
Moreover, there was a significant association between year of investigation and SRH, which was independent of age and covariates. In women, the association between SRH and year of investigation followed a linear function, with gradually decreasing SRH levels over time, and in men the association followed a third-degree polynomial function with fluctuations but no persistent decrease over time. Results from previous studies concerning associations between year of investigation and SRH are controversial.6 ,11 ,16 ,17 However, these studies differ in terms of whether or not medical health and life-style-related variables are controlled in analyses, and also in terms of study-population characteristics. Contextually determined perceptions of health may, for example, be expected to differ between countries. Present results are in line with results from a recent study,6 in which poorer age-specific SRH in more recent years of investigation was observed in a Danish study population, but differ with regard to results from the USA, British and German study populations where no age-specific differences were observed during the same time period.
The main strength of the study concerns sample size. Data were based on eight ongoing population studies, covering more than 14 000 observations scattered over a 30-year period. The sample size was thus larger than in previous studies investigating effect of year of investigation on SRH, and observation time spanned up to three decades in men and one decade in women. The determinant variables were measured with the same instruments in all cohorts.
A further strength concerns the use of ordinal regression modelling.25 ,26 SRH is an ordered categorical variable. The majority of previous studies investigating predictors of multilevel SRH either used binary logistic regression technique, despite the reduced efficiency and the risk of bias related to choice of cut point this entails, or analytical methods requiring normally distributed SRH data, a requirement rarely satisfied.
The main limitation of the study is that all age groups were not represented on each measurement occasion, and that some model-based results were thus generated for age groups where no actual measurements were obtained, as shown in figure 1. However, this is a problem common in multiple analysis modelling, and not unique to this study.
Moreover, the data were generally cross-sectional. Even so, some of the cohorts were investigated repeatedly and thus form a truly longitudinal cohort. Results were similar for subjects who participated only once and subjects who participated on several occasions, indicating that the results concerning age and secular trends were stable, and that the design used here is equivalent to a longitudinal one.
The attrition rate was a moderate 28%. To test the potential effect of attrition on the secular trend slope, results were re-analysed based on the assumption that non-participants in the early and the late parts of the study period reported considerably lower or higher levels of SRH than participants. However, even the most unfavourable alternative from the hypothesis point of view (non-participants in the early study period reporting 5 SE units lower SRH than participants, and 5 SE units higher SRH at the end of the study period) was associated with a highly significant decrease in mean SRH over calendar time. We therefore have no reason to believe that the results are afflicted by selection or other bias to such an extent that the conclusions would be affected.
The results from this study regarding the age−SRH relationship are in line with the majority of previous studies,6–11 reporting decreasing SRH levels with age. Results concerning associations between SRH and year of investigation suggested an inverse trend in self-ratings of health over time in women, but less so in men. Previous results are controversial, some studies showing increasingly poorer SRH in more recent cohorts, others showing better SRH.12–14 16–18 Changes in SRH over time, on the one hand, may reflect changes in patterns of morbidity or, on the other hand, contextually determined differences in norms and expectations in relation to health,13 ,27 and furthermore, may or may not suggest contextually determined changes in healthcare utilisation. Concepts of health and knowledge and expectations concerning health and healthcare may change over time. One important question from a public health perspective concerns to what extent observed trends are associated with changes in morbidity, mortality and healthcare utilisation. Given that life expectancy has increased over the period it is unlikely that the decrease in SRH reflects a major deterioration in health in the population.
The relationship between age and SRH differed between women and men, as did the observed association between year of investigation and SRH. A linear decline in SRH was observed among women, and a more complex age−SRH relation observed among men. Few studies have, to date, investigated potential non-linearity of associations between age or year of investigation, and SRH.11 ,14 ,17 A non-linear association between age and SRH in women and men,11 ,14 and a linear cohort effect (measured as 10-year birth cohorts) on SRH,14 has been reported, but whether women and men differ in functional form of the observed association between age, or cohort, and SRH, was not investigated. In a study of 618 randomly sampled middle-aged women, independent, inverse, linear and quadratic age effects on SRH was reported, with poorer SRH and a more rapid decline in SRH per year in the later cohort.17
Although similar patterns of determinants of SRH have been observed in women and men,28 gender-related differences in the association between SRH and subsequent mortality have repeatedly been observed,29 ,30 and, accordingly, the relative importance of various contextually related factors of importance for health may be different for women and men.15 The present results thus underline the importance of investigating effects of contextually related factors, such as age and year of investigation on SRH separately for women and men.
The differing trends among women and men may, furthermore, be explained by the analysis modelling, since the women were less scattered over the years of investigation than men, as shown in figure 1. However, a great deal of effort was devoted to the analysis modelling, with a number of possible models tested. The model with the best fit between the model data and crude data was finally accepted. It is therefore unlikely that the differing functional form for women and men is an analytical artefact.
The results on SRH predictors were similar for women and men, and in line with previous research on determinants of SRH, in which illness, disease and disability were the strongest predictors of SRH.5 Variables included in the final ordinal regression model in the present study explained 76.2% of the variance in SRH in women, and 74.5% of the variance in SRH in men, which implies that the model captures core determinants of global SRH. In our analyses we were restricted to covariates that were available in the datasets common to all subpopulations in this study. The remaining unexplained 25% may be attributable to predictors not included in our model, perhaps different ones in women and men.
Acknowledgments
The study was supported by grants from the Swedish Research Council, the Swedish Research Council for Working Life and Social Research, the Vårdal Foundation, the Sörmland County Council and Gothenburg and Uppsala Universities, Sweden.
References
Footnotes
-
Contributors CW, TW, AR, AB, SJ, HE and KS performed the data collection in their respective datasets. CH and KS designed the analyses. JB, CH and KS contributed with SAS programming. CH and KS drafted the manuscript. All authors participated in the critical discussions of the results, identification of relevant reference literature and in the revisions of the manuscript.
-
Funding The study was supported by grants from the Swedish Research Council, the Swedish Research Council for Working Life and Social Research, the Vårdal Foundation, the Sörmland County Council and Gothenburg and Uppsala Universities, Sweden.
-
Competing interests None.
-
Ethics approval Research Ethics Committees at Gothenburg and Uppsala Universities and by the National Research Ethics Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The dataset is based on a research consort of groups in Gothenburg, Uppsala and Eskilstuna. Requests for data access may be made to Kurt Svärdsudd.
Linked Articles
- Miscellaneous
- Corrections