Article Text

Abstract
Introduction Cardiovascular diseases (CVD) are increasing throughout the world and cause 16.7 million deaths each year, 80% of which occur in low and middle income countries. In Argentina, Chile and Uruguay, the available data on cardiovascular risk factors come predominantly from cross-sectional studies that are principally based on self-report or studies conducted with small convenience samples. The CESCAS I study will generate reliable estimates of the prevalence and distribution of and secular trends in CVD and its risk factors in this region.
Methods and analysis CESCAS I is an observational prospective cohort study with a multistage probabilistic sample of 8000 participants aged 35–74 years from four mid-sized cities representing the Southern Cone of Latin America: Bariloche and Marcos Paz in Argentina, Temuco in Chile and Pando-Barros Blancos in Uruguay. In the first phase, baseline data regarding exposure to risk factors and prevalence of CVD will be collected in two stages: (1) in homes and (2) in health centres. Information will be gathered on medical history, risk factors, lifestyles and health utilisation through specific questionnaires, physical measurements, an ECG and an overnight, fasting blood sample to measure levels of serum lipids, glucose and creatinine. In the second phase, annual follow-up data will be obtained on the incidence rate of CVD events and the association between exposure and events.
Ethics and dissemination The protocol has obtained formal ethics approval from institutional review boards in Argentina, Chile, Uruguay and the USA. The lack of follow-up studies has prevented Argentina, Chile and Uruguay from implementing risk factor stratification and management strategies at a population level. However, the CESCAS I study data will help the development of public health strategies based on primary care intervention, thus helping to improve cardiovascular health in this region.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
To estimate the prevalence and distribution of and secular trends in major cardiovascular disease (CVD) events and risk factors in four cities in Argentina, Chile and Uruguay.
Key messages
Lack of follow-up studies prevents Argentina, Chile and Uruguay from assessing local risk estimates, obtaining reliable data on CVD burden and implementing risk factor stratification and management strategies at a population level.
There is a strong need in the region to build the capacity and infrastructure to undertake a population-based cohort study to address knowledge gaps and to inform policymakers of the impact of CVD in the Southern Cone of Latin America.
Strengths and limitations of this study
CESCAS I will be the first longitudinal study to estimate the CVD trend and risk factors in Argentina, Chile and Uruguay.
Introduction
Cardiovascular diseases (CVD) are increasing throughout the developing world and cause almost 16.7 million deaths each year, 80% of which occur in low and middle-income countries.1 Indeed, 34% of annual deaths are due to CVD.2 It has been projected that 41 million people world-wide will die in 2015 of chronic CVD unless effective concerted action is taken now.3 In low and middle-income countries, almost half of these deaths will occur in people below 70 years of age compared with only 27% in high-income countries.4 Furthermore, although in recent decades age-adjusted rates for cardiovascular mortality have decreased in developed countries, rates have increased in low and middle-income countries.1 5
In Latin America, it is estimated that between 1990 and 2020, deaths from CVD, including coronary heart disease (CHD), will increase by approximately 145% in both men and women compared with an increase of 28% in women and an increase of 50% in men in developed countries during the same period.6
Moreover, at least 75% of CVD can be explained by risk factors such as an unhealthy diet, low physical activity and tobacco use.7 In the World Health Report 2002, 26 risk factors were evaluated and ranked by their importance. Major risk factors identified for most Latin American countries were hypertension, increased body mass index (BMI), and alcohol and tobacco use.8 The Latin American INTERHEART study showed that most cardiovascular risk in the Southern Cone could be explained by tobacco use, abnormal lipids, abdominal obesity and high blood pressure.9 In Argentina, recent estimates showed that in 2005 there were more than 600 000 disability adjusted life years (DALYs) and almost 400 000 years of potential life lost due to CHD and stroke, where modifiable risk factors explained 75% of fatal and non-fatal acute CHD and stroke events, 82% of acute CHD events and 62% of strokes. Similarly, modifiable risk factors explained 76% of costs due to acute events and 71% of DALYs lost.10 In Argentina, Chile and Uruguay, the available data on CVD risk factors come mainly from cross-sectional studies that are principally based on self-report or studies conducted with small convenience samples, which do not give reliable estimates.11–13 None of the studies mentioned above included a prospective follow-up study. While the ongoing ELSA study, a recently established cohort study in Brazil, will provide data on cardiovascular events, its population is composed of employee volunteers from six Brazilian universities and thus will not be able to offer population-based estimates of the impact of CVD risk factors on the incidence of CVD.14
The CESCAS I study will generate reliable estimates of the prevalence and distribution of and secular trends in CVD and its risk factors in this region. These data will contribute to the development of public health strategies, thus helping to improve cardiovascular health in Latin America.
Methods
Study design
CESCAS I is an observational, prospective cohort study initiated in November 2010 and is composed of two phases. In the first phase, baseline data will be collected regarding exposure to risk factors and prevalence of CVD. In the second phase, annual follow-up data will be obtained on the CVD incidence rate and the association between exposure and the event.
Study population
This study entails a probabilistic sample of 8000 non-institutionalised mainly urban men and women between the ages of 35 and 74 years representing the general adult population in Argentina, Chile and Uruguay. Four mid-sized cities have been selected: two in Argentina (Bariloche and Marcos Paz), one in Chile (Temuco) and one in Uruguay (Pando-Barros Blancos).
Sampling method
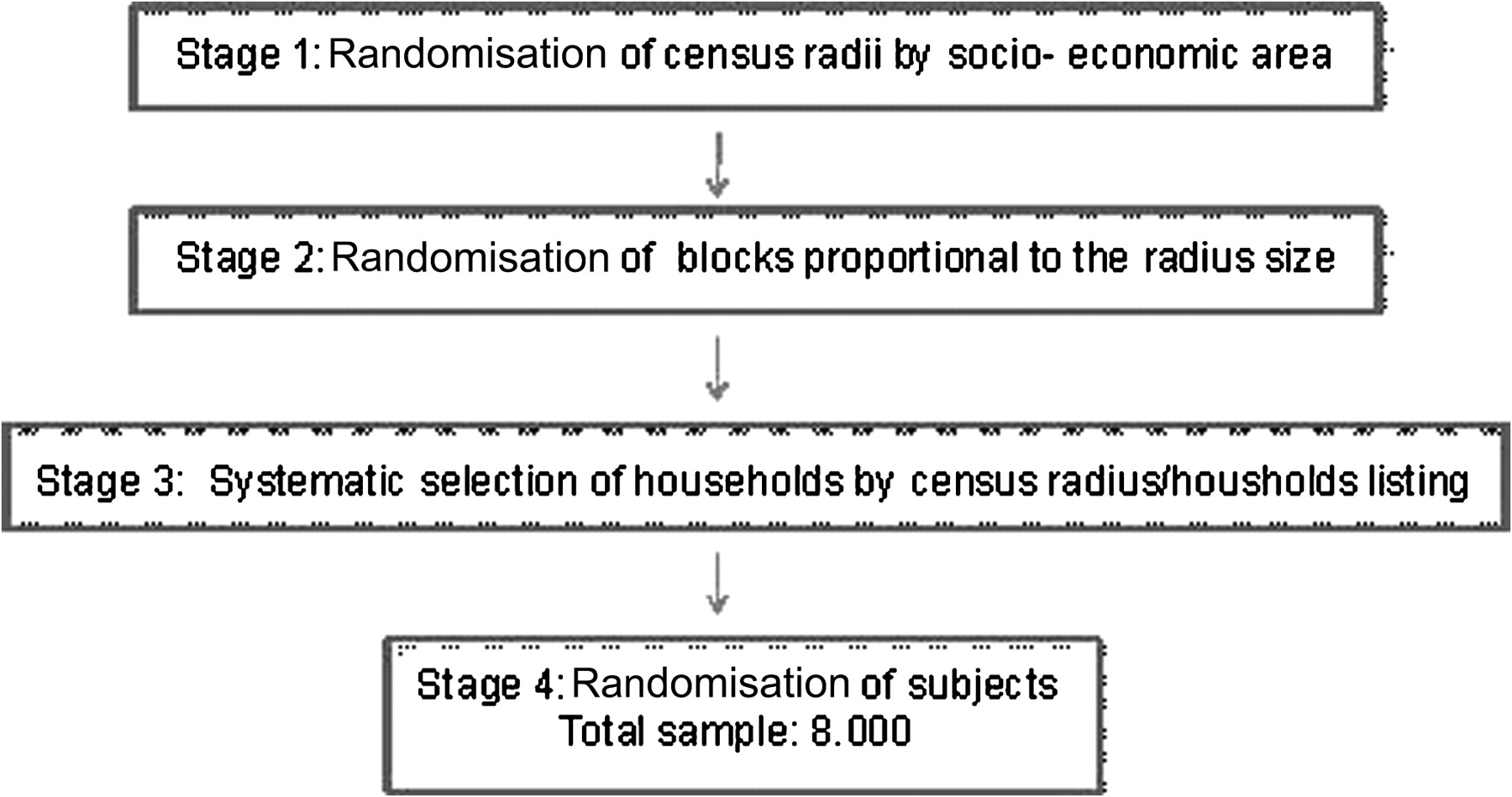
As the prevalence of CVD risk factors was considered likely to vary by age, gender and geographical area, the sampling method was stratified accordingly, following a complex sampling design that consisted of four stratified stages to obtain a representative sample from each of the four locations (figure 1). The first stage consisted of randomly sampling census radii from each location, stratified by socio-economic level. In the second stage a number of blocks proportional to the radius size were randomly selected. The third stage sampled households from each block using systematic sampling. If the selected house did not include a permanent residence (eg, offices/weekend residences, abandoned or demolished dwellings, those under construction, or addresses which were not identified), it was replaced with another house. In the selected households all members between 35 and 74 years of age were recorded to create the final sampling frame. In the fourth stage, one recorded member per household was randomly selected. The final sampling frame was composed of one subject per household, stratified by gender (50% women and 50% men) and age category (35–44, 45–54, 55–64 and 65–74 years old) constituting a total of 2000 subjects per site, all of them meeting the following criteria: a permanent resident at the location for at least 6 months per year, willing to sign a consent form to participate, not intending to relocate within the next 2 years, and able to respond autonomously to the questionnaire (without cognitive impairment or language problems). Replacement of selected participants because of refusal to participate or inability to be located was not allowed.15 16
{kind=link}
Sampling procedure in the CESCAS I study.
Recruitment plan
Participants are invited to participate through a letter from the site institution. The interviewer makes the first contact with the household and arranges an appointment for a home visit to collect questionnaire data and schedule a follow-up clinic visit. A clinic visit is scheduled to obtain physical measurements, an ECG and overnight fasting blood samples. To minimise non-participation and the potential for bias, the following measures will be taken to facilitate and encourage participation:
Travel assistance or home assessment for those unable to travel to the examination centres
Variety of appointment times to suit all members of the community
Feedback of blood test and examination results to participants.
Data collection
Baseline data collection is conducted in two stages: at home and in the health centre. In the home, an interviewer administers specific questionnaires to collect the required information. Once the survey is complete, the interviewer proceeds to arrange a visit to a health centre where the physical measurements, ECG and blood sample will be obtained.
Questionnaires
A trained interviewer will gather information regarding participant characteristics including demographic, socioeconomic and healthcare utilisation data, personal and family history of CVD, and risk factors such as high blood pressure, dyslipidaemia and diabetes, as well as current pharmacological and non-pharmacological treatment. Data will also be collected regarding intermittent claudication, cancer, respiratory disease, alcohol consumption and weight history using cross-culturally adapted questionnaires from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL).17 Physical activity will be assessed through the HCHS/SOL study questionnaire adapted from the International Physical Activity Questionnaire.18 Information about current and former cigarette smoking, including age at which smoking was initiated, years of smoking, number of cigarettes smoked per day, cessation attempts and treatments, will be assessed using the Global Adult Tobacco Survey.19 Use of other forms of tobacco, exposure to passive cigarette smoking and indoor pollution will also be assessed. Nutritional information will be collected using a semi-quantitative food frequency questionnaire adapted from the National Cancer Institute Diet History Questionnaire, which has been validated by our research team for use in Argentina, Chile and Uruguay (N Elorriaga, personal communication, 2011). Depression and anxiety will be assessed by the nine-item Patient Health Questionnaire (PHQ-9),20 which has been validated in Argentina.21 Stressful events and spirituality will be assessed through a cross-culturally adapted version of the HCHS/SOL study questionnaire.17
Locally validated versions of the SF-12 and EQ-5D will be used to measure health-related quality of life and social utilities and preferences, respectively.22 23 All questionnaires used in the study and their sources are listed in table 1.
Data collection in the CESCAS I study
Blood pressure and anthropometric measurements
Trained and certified observers will measure blood pressure during the health centre visit following the recommendations of the American Heart Association.24 According to the study protocol, before blood pressure is measured, the participant should remain seated and at rest for 5 min. Tea, mate or coffee consumption, as well as smoking or exercising, in the 30 min before testing is not permitted. A standardised mercury or aneroid sphygmomanometer with an adequate cuff size will be used. The cuff will be placed on the right arm of the participant, inflated to 10 mm Hg, and then inflated again until it reaches a pressure 30 mm Hg above the level at which the radial pulse can no longer be palpated. Three measurements will be obtained, with 30 s intervals between them. Korotkoff sounds will be recorded, and used to identify systolic and diastolic blood pressure.
Weight will be measured with the subject wearing undergarments but not shoes. Weight will be recorded in kilograms to one decimal place using standing scales supported on a steady surface. Height will be measured without shoes, in centimetres to one decimal place, on the Frankfort plane positioned at a 90° angle against a metallic metric tape measure mounted on a wall. Abdominal circumference will be measured in centimetres to one decimal place, on a horizontal plane 1 cm above the belly button which generally coincides with the narrowest waist circumference.
Laboratory measurements
Overnight fasting blood samples will be drawn by venipuncture to measure levels of serum lipids, glucose and creatinine. Samples will be processed and temporarily stored at the extraction site to be sent later for analysis and storage (in ultra freezers at −80°C) in the central laboratory at the Hospital Italiano of Buenos Aires. LDL cholesterol levels will be calculated using the Friedewald equation for participants with triglyceride levels <400 mg/dl. According to this equation, total LDL cholesterol is equal to: total cholesterol−HDL cholesterol−triglycerides/5.
Electrocardiogram
The study will employ a 12-lead electrocardiogram standardised at 25 mm/s and at 1 mV of amplitude.
Study outcomes
Hypertension is defined as a mean systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg, and/or self-report of current use of antihypertensive medications.25 Obesity is defined as BMI ≥30 kg/m2 and overweight as BMI ≥25 kg/m2.26–29 Dyslipidaemia is defined as total cholesterol ≥200 mg/dl or 11.1 mmol/l, LDL cholesterol ≥130 mg/dl or 7.2 mmol/l, or HDL cholesterol <40 mg/dl or 2.2 mmol/l.30 Diabetes mellitus is defined as fasting glucose ≥126 mg/dl or 7 mmol/l. Glucose intolerance is defined as a fasting glucose level of 110–125 mg/dl or 6.1–6.9 mmol/l.31 Current smoking is defined as smoking at least one cigarette per day at the time of the survey. Former smoking is defined as a person who has been a smoker but does not smoke at the time of the survey. Passive smoking is defined as involuntarily breathing air that is contaminated by tobacco smoke.27 32
During the follow-up a person will be categorised as having CVD if it is self-reported or their self-assigned proxy has reported any of the following conditions diagnosed by a physician: CVD death, acute myocardial infarction, angina, heart failure, cerebrovascular events, peripheral vascular disease or coronary or peripheral revascularisation. The study outcome committee will review the collected source documents related to the reported event and adjudicate on all CVD outcomes independently.
Training and quality assurance
Field work quality assurance
Data collection will be conducted according to the standardised operations manual. Between 5% and 10% of participants will have repeated measurements of arterial pressure, height, weight and waist circumference to adjust for the effect of measurement error on selected variables. All the equipment used will be certified to international standardisation norms. Periodic monitoring of data collection procedures will be performed by the coordinating centre.
Laboratory quality control
All laboratory measurements (total cholesterol, HDL, LDL, triglycerides, glucose and plasma creatinine) will be carried out by the central laboratory. Each laboratory technician will have to complete a training program.
Processing of data
The database was designed using the OpenClinica system.33 This is a computerised system of related databases with web interface. The data will be entered from each site, via the web, into electronic forms. Double data entry with independent operators will be performed to eliminate data entry errors. The data will be stored on a central server. Validation rules will be generated in accordance with the nature of the variables. Automatic queries will be generated in response to out-of-range entries to be investigated by study personnel at each site.
Statistical investigation
Sample size
The calculated sample size is 8000 participants (2000 per site) which is consistent with the recommended requirements for precision for complex surveys. This sample will be sufficient to provide precise estimates of the prevalence of major CVD risk factors by gender and site, in four age-defined categories (35–44, 45–54, 55–64 and 65–74 years old) as well as their association with the development of CVD.34–36 The proposed sample size is sufficient to comply with the precision requirements of a complex sample that assumes that the design effect is 1.5 and the prevalence of the risk factors of interest is 5% or greater (table 2).
Sample size required for different proportions and design effects
For analysis, the capacity to detect risk factors was calculated using a statistically significant α level of 0.05 and a statistical power of 85%, which will permit detection of moderate and large relative risks.
Statistical analysis
The general characteristics of the population will be described. For continuous variables, mean and median, range, standard deviation and/or quartile range will be calculated according to the distribution of each variable. In the case of categorical variables, absolute and relative frequencies will be calculated.
In order to determine the prevalence and incidence of risk factors, CVD events and the association between risk factors and CVD events, the design effect of the first stage unit of sampling will be considered. Weighting will be based on the relationship between the number of individuals finally included in the study and the population size and composition of each site according to the most recent census data. Likewise, the analysis will be carried out by socioeconomic strata, according to gender and four age categories (35–44, 45–54, 55–64 and 65–74 years old).
To assess associations between risk factors and CVD events, linear regression and simple and multiple logistic regressions will be used according to the nature of the response variables. Continuous variables that are not normally distributed will be evaluated by the application of transformations and categorisations wherever applicable.37
The secular trends in risk factors over time will be evaluated with statistical analysis methods that take account of the correlation between repeated measures. To evaluate the changes in risk factors over time by sub-groups of interest, generalised estimation equations will be used. To estimate the rate of accumulated cardiovascular incidents, the Kaplan–Meier method will be used. The log rank test will be used to compare the differences between the curves of accumulated incidence events. In order to quantify the relationship between risk factors and the incidence of CVD events, the Cox proportional hazards method will be used. Potential confounders and interactions will be explored. Appropriate diagnostics will be carried out to test goodness of fit, collinearity and atypical observations in each model. In all cases, fulfilment of assumptions in the model by means of exploration of residual behaviour will be verified.
Statistical analysis software STATA 10.0 and SAS 9.0 will be used.37–39
Ethical aspects
The study will be carried out following the guidelines for the protection of the rights of human volunteers. All investigators and personnel in the study have completed a training course, certified by the National Institutes of Health (NIH). All participants will sign an informed consent form during the initial visit. To protect participant confidentiality, the information included in the database will not contain personal identifiers.
Timeline of the study
Baseline data collection is projected to be carried out during 2011. The follow-up phase will begin in 2012 and will consist of an annual telephone interview continuing up to the fourth year with a second round of physical and biochemical measurements and an ECG performed 2–3 years after the baseline measurements.
Conclusions
Despite the increasing burden of CVD in the Southern Cone, which over the last decades has been ranked as the main cause of mortality and morbidity, national health programs and policies are still mostly focused on interventions aimed at tackling communicable diseases or perinatal or childhood conditions. Therefore, new programs should be targeted at modifying lifestyle and nutritional risk factors to reduce CVD in high risk subjects.36 However, the lack of follow-up studies prevents our countries not only from assessing local risk estimates and obtaining more reliable data on the burden of CVD, but also from implementing risk factor stratification and management strategies at a population level. Accordingly, and based on limited and imprecise evidence, there is a strong need in the region to build the capacity and infrastructure necessary to undertake a population-based cohort study to address these remaining knowledge gaps and to inform public health policymakers of the impact of CVD in our countries. The CESCAS I study data will help develop public health strategies based on the application of primary care interventions, thus helping to improve cardiovascular health in this region.
Acknowledgments
We thank Eiman Jahangir and Alisson Lee, fellows of the Fogarty International Clinical Research Fellows Program (FICRF), for careful revision of the manuscript.
References
Footnotes
Funding This work was supported by the National Heart, Lung, and Blood Institute (NHLBI) grant number HHSN268200900029C.
Competing interests None.
Ethics approval Institutional review boards from Argentina (Hospital Italiano de Buenos Aires), Chile (Universidad de la Frontera), Uruguay (Universidad de la República) and the USA approved this study.
Contributors AR, JH, VI, RP, LB, FL, JM, MC, HO, PS and JP all contributed to the conceptualisation and design of the study and all revised this manuscript critically. All authors gave final approval of the version to be published.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement Following the policy of the National Institutes of Health (NIH), we reaffirm the practice of making data used for scholarly research available to other investigators.