Article Text

Abstract
Objective To investigate the current situation of anaemia among children aged 6–23 months in a rural county in China, and to explore the influencing factors and the main causes of anaemia.
Design A cross-sectional study.
Setting Huzhu County in Qinghai Province, China
Participants We selected 38 sampled villages using Proportional to Population Size sampling method. We obtained the name list of children aged 6–23 months in each sampled village and planned to survey all the eligible children aged 6–23 months and their caregivers.
Primary and secondary outcomes measures The prevalence of anaemia, the influencing factors of anaemia, the laboratory tests for biological causes of anaemia, including serum ferritin, soluble transferrin receptor, folic acid, homocysteine and vitamin B12.
Results A total of 754 children aged 6–23 months and their caregivers were surveyed, and 183 anaemic children aged 12–23 months were collected venous blood sample. The anaemia prevalence of children aged 6–23 months in Huzhu County was 59.1%. Children of younger age (OR=0.968, 95% CI 0.940 to 0.998), Tibetan nationality (OR=3.123, 95% CI 1.473 to 6.623) and not introducing meat (OR=0.698, 95% CI 0.499 to 0.976) were more likely to be anaemic. More than 80% of children with anaemia were due to iron deficiency (ID), and 20.2% of them had both iron and folic acid deficiencies.
Conclusions The anaemia prevalence of children aged 6–23 months in Huzhu County was high and children of younger age, Tibetan nationality and not introducing meat were more likely to be anaemic. The main cause of anaemia was nutritional anaemia, with the vast majority being ID. Interventions of feeding counselling and nutrients supplements are appropriate and should be further strengthened.
Trial registration number ChiCTRPRC12002444.
- Anaemia
- iron deficiency
- nutrition
- children
- China
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
In addition to the prevalence of anaemia for young children, we also investigated the influencing factors and biological causes of anaemia through statistical analysis and laboratory tests to provide guidance for future programme implementation.
The study took place only within one rural Chinese county and caution is needed when generalising the findings from this study to other settings.
The sample size was relatively small.
Introduction
Childhood anaemia has long been a major public health problem worldwide. A systematic analysis of population-representative data suggested that anaemia prevalence in children younger than 5 years was 43% and there were 273 million children with anaemia globally in 2011.1 The national anaemia prevalence in children under five in China fluctuated between 12% and 23% between 1990 and 2005 and then decreased from 19.3% in 2005 to 12.6% in 2010.2 National Nutrition and Health Surveillance in 2013 showed that the prevalence of anaemia among children aged 0–5 years was 11.6% across the country, 10.6% in urban areas and 12.4% in rural areas, respectively. However, huge regional differences exist, with rural Qinghai province being the highest (27.5%).3 In some rural areas, anaemia prevalence in children aged 6–23 months was higher than 30%.4 5
In the public health perspective, anaemia is defined by the WHO as a haemoglobin concentration 2 SDs below the mean haemoglobin concentration for a normal population of the same gender and the same age group.6 Anaemia has irreversible adverse effects on childhood growth and development, even their working abilities in adulthood.7 Many studies suggested an association between anaemia and impaired psychomotor development; impaired cognitive functions such as concentration, intellectual status, memory and scholastic skills; psychological and behavioural disorders such as attention-deficit/hyperactivity disorder8 and autism spectrum disorder9 and decreased physical activity.10 Meanwhile, anaemia has been confirmed to be associated with impaired renal function, increased absorption of lead and impaired immunity.11 The Global Burden of Disease (GBD) 2000 report estimated that anaemia resulted in 68.4 million years lived with disability, accounting for 8.8% the total number of all cases of disability,12 and the GBD 2004 update had similar findings, which exerted a substantial economic burden.13
Our previous study in Qinghai Province found that the prevalence of anaemia in rural areas was much higher than the national average level. In 2012, the prevalence of anaemia among children aged 6–23 months in Huzhu, Minhe and Guinan County was 71.1%, 56.1% and 86.3%, respectively.14 We carried out a controlled interventional study in Huzhu and Guinan county from 2012 to 2014. And all children aged 6–23 months in the intervention county, Huzhu County, received YingYangBao (a domestically produced multiple micronutrient powders for infants and young children) and their caregivers received infant feeding counselling from trained village doctors. The study found that the anaemia prevalence significantly decreased from 71.1% to 47.8% in Huzhu County.15 WHO defines the prevalence of anaemia in the population less than 20% as a mild public health problem, 20%–40% as a moderate public health problem and the prevalence of anaemia in the population ≥40% as a serious public health problem.16 Therefore, childhood anaemia in Huzhu County is still a serious public health problem in spite of the dramatic reduction of anaemia prevalence after the study, and more efforts are needed to further decrease anaemia prevalence and improve the nutrition status of children.
There are many reasons for anaemia: acute and chronic infections that result in inflammation (including chronic blood loss caused by hookworm infection or schistosomiasis); nutritional anaemia caused by iron deficiency (ID) and other micronutrient deficiencies, especially of folic acid, vitamin B12 and vitamin A; and genetically inherited traits such as thalassemia.17 Although it is generally accepted that nutrient deficiency is the leading cause of child anaemia, proportions of anaemic causes in specific areas are usually unknown. Since interventions based on improvement of child feeding and nutrients supplements are only effective for nutritional anaemia, understanding the status of anaemia-related nutrients (iron, folic acid and vitamin B12) is crucial to estimate the potential effectiveness of nutritional interventions. The purpose of this study is to investigate the current situation of anaemia among children aged 6–23 months in Huzhu County, and to explore the influencing factors and the main causes of anaemia, so as to develop more appropriate strategies for combating this intractable public health issue.
Methods
Study design
This study was conducted as a cross-sectional survey of children aged 6–23 months and their caregivers in Huzhu County, Qinghai province. Proportional to Population Size (PPS) sampling method was used to select sampled villages in the county. We first obtained the name list of children aged 6–23 months in each sampled village and aimed to survey all the eligible children aged 6–23 months and their caregivers. The HemoCue Hb 301 analyzer (HemoCue, Lake Forest, CA, USA) was used to collect children’s fingertip peripheral blood using microcuvettes (for blood samples) to detect haemoglobin levels of children in all the sampled villages. After 4–7 days, anaemic children screened out by HemoCue Hb 301 analyzer were called to Huzhu Maternal and Child Health and Family Planning Service Centre to draw venous blood sample for further blood routine test and laboratory tests.
Study setting
Qinghai Province lies in northwest China, with an area of around 7 20 000 km2. By the end of 2017, the resident population of the province was 5 838 000, of which the resident population of rural areas was 2 808 400, accounting for 46.9%, and the ethnic minority population was 2 854 900, accounting for 47.7%. Qinghai Province has 34 counties and 439 townships. The Qinghai resident per capita disposable income in 2017 was ¥9462 (US$1363.13)18 for rural people, which was far lower than the national level (¥13 432 (US$1935.06)).19
Huzhu County is located in the northeastern part of Qinghai Province and 27.9% of its population is ethnic minorities, which includes Tu, Tibetan, Hui and other 28 ethnic minorities.20 Huzhu County covers an area of 3424 km2. The county governs 19 townships with 294 villages, with a total population of 401 540, of which the rural population accounted for 76.0%. By the end of 2017, the resident per capita disposable income in the rural area was ¥9810 (US$1414.91).21
Participants
Children aged 6–23 months and their caregivers were invited to participate in this survey. We excluded children with a structural or genetic birth defect such as neural tube defects, congenital heart disease or phenylketonuria or caregivers who refused to participate.
Survey instrument
We used the adapted WHO Maternal, Newborn and Child Health Household Survey (World Health Organization, 2009) to collect household information and infant feeding practices in each sampled village.
Sample size and sampling
The sample size required were calculated based on estimated anaemia prevalence in Huzhu County. We used the sample size calculation for proportion in single cross-sectional survey to estimate the sample for our study. Based on 35% of expected anaemia prevalence for children aged 6–23 months in Huzhu County, 5% of desired absolute precision, and 2% of design effect, we calculated the sample size of 699. Meanwhile, we also expected to draw 200 venous blood sample of anaemic children aged 12–23 months. According to the estimated anaemia prevalence of 35% in Huzhu County, we calculated that the total number of children aged 12–23 months needed was 571. We assumed that the number of children equally distributed in three age groups (6–11 months, 12–17 months and 18–23 months), and calculated that 285 children aged 6–11 months were needed. Hence, a sample size of 856 children aged 6–23 months was used in this study.
We knew the average number of children aged 6–23 months in each villages of Huzhu County from the local Maternal and Child Health Family Planning Service Centre. PPS sampling method was used to select 38 sampled villages to meet our sample size requirements in the county. We obtained the name list of children aged 6–23 months in each sampled village and planned to survey all the eligible children and their caregivers.
Training of interviewers
Staff from the Capital Institute of Paediatrics in Beijing were supervisors for this survey, and 25 students were recruited from Qinghai Institute of Health Sciences as interviewers. We provided them training for 2 days before fieldwork, which included communication skills, explanation of questionnaires, demonstration, role plays, field practice and group discussions. In addition, four of them were trained on measuring haemoglobin levels with a HemoCue Hb 301 analyzer. After the training, a half-day field practice was held in a village clinic. Any problems arising during the field practice were discussed and solved directly.
Data collection
We carried out the survey from 23rd to 27th July 2018. In every surveyed township, staff notified the village doctors of the sample villages in advance, then the village doctor called the caregivers to take their children to the village clinic for investigation. First, interviewers introduced the aim of the survey to the mothers or other caregivers and obtained written informed consent from them. Then, the interviewers questioned them following the instructions.
We used smartphones with the household survey questionnaire set up in specially developed software to record data.22 Four teams of interviewers carried out the survey, with six surveyors and one supervisor in each team. Data for each questionnaire were uploaded into an Excel database via the internet server. Once the interview was completed, the special surveyor in each team measured haemoglobin with a HemoCue Hb 301 analyzer (HemoCue, Lake Forest, CA) by drawing around 10 μL finger blood.
Children aged 12–23 months screened as anaemia by HemoCue Hb 301 analyzer were informed to go to the Huzhu County Maternal and Child Health Family Planning Service Centre for further tests from 31 July to 1 August 2018. About 4–5 mL venous blood of each children was collected by experienced nurses and placed into two tubes. The first 1–2 mL blood sample was collected into a labelled dipotassium ethylenediaminetetraacetic acid (EDTA-K2)-coated tube for blood routine test using whole blood. And the second 3 mL blood sample was collected (without removing the needle) into a labelled vacuum separating tube for serum ferritin (SF), soluble transferrin receptor (sTfR), C-reactive protein (CRP), α−1 acid glycoprotein (AGP), vitamin B12, homocysteine (HCY) and folic acid concentration using serum.
Blood routine test and blood centrifugation were completed in the local laboratory. The blood samples in labelled vacuum separating tubes were placed for 30 min, then were centrifuged at 1500 turn/min for 15 min. The serum was separated into 1, 2 and 3 cryotubes using disposable pipettes.
After the field work, all the blood samples were immediately stored at −70 °C and transported as soon as possible to National Institute for Nutrition and Health, China Centre for Disease Control and Prevention for further laboratory testing. Repeated freezing and thawing were strictly avoided during transportation and storage.
Laboratory analysis
The blood routine test was conducted using automatic blood cell analyzer (Horiba, ABX Micros 60-OT, France) in local laboratory. SF, vitamin B12 and serum folic acid were analysed by Roche Cobas e601 analyzer (Germany) using electrochemiluminescence immunoassay. sTfR, CRP and AGP were analysed by Hitachi 7600–110 chemistry autoanalyzer (Japan) using immunoturbidimetry and HCY was analysed by Hitachi 7600–110 chemistry autoanalyzer (Japan) using enzymatic cycling assay.
Data management and statistical analysis
Data of questionnaires were automatically transformed and pooled into a Microsoft Excel sheet. After the data cleaning, we converted the database into a database file for the final analysis.
We carried out statistical analysis with SAS 9.2 for Windows. The median (Q1, Q3) was used to describe the age in years of mothers and grandparents of children. Mean and SD were used to describe the values of SF and body iron (BI). Percentages were presented in binary or categorical variables. We used the Pearson X2 test and Fisher’s exact test to compare binary and categorical variables.
Moreover, we carried out a logistic regression analysis to identify factors associated with children’s anaemia in this survey. All relevant factors were first selected by univariate logistic analysis, including child’s age, child’s sex, parents’ age, parents’ nationality, parents’ education, parents’ job, whether parent worked outside the county, whether children aged 6–23 months had been given iron-rich or iron-fortified foods during last 24 hours, whether children aged 6–23 months had been given meat during last 24 hours, minimum dietary diversity, whether child had coughed, fever or diarrhoea in the past 2 weeks, and whether children aged 6–23 months had been given Ying Yang Bao (YYB) five bags or more. Only those that were significant in the final multivariate model are presented. We present ORs and 95% CIs and considered two-tailed p values of <0.05 for a significant difference.
We calculated the feeding practice indicators based on the WHO guideline ‘Indicators for Assessing Infant and Young Child Feeding Practices’,23 which based on the 24 hours recall method. And all individual haemoglobin values were adjusted using WHO recommendations based on the altitude of the surveyed villages where children lived. An adjusted haemoglobin lower than 110 g/L16 was defined as anaemia and was used to calculate the prevalence of anaemia. A haemoglobin concentration of 90–110 g/L was defined as mild anaemia,<90 g/L as moderate anaemia or severe anaemia. Cut-offs for elevated CRP and AGP were >5 and >1 mg/L, respectively.24 If one of these two indicators were elevated, the children surveyed were classified as infected children. SF concentration <12 ug/L and <30 ug/L were used to define ID in non-infected children and infected children, respectively. The children with concurrent anaemia and ID were diagnosed with ID anaemia (IDA).25 A plasma folic acid concentration of <4 ng/mL was used to define folic acid deficiency according to WHO guidelines.26 Vitamin B12 deficiency was defined as <197 pg/mL. Cut-offs for elevated sTfR and HCY were 8.327 and 14 umol/L, respectively.28
BI stores (were estimated by applying Cook’s formula as follows: BI (mg/kg) =-[log(R/F ratio)−2.82290]/0.1207. The R/F ratio was sTfR/SF.29 Among them, sTfR needs to be transformed by the following formula: sTfR=1.5 * Roche sTfR +0.35 mg/L.30 The positive value means iron surplus in stores and the negative value means iron deficit in tissues.
Participant and public involvement
The participants and the public were not involved in the design, recruitment and conduct of the study. There are no plans to disseminate the study findings to the study participants.
Results
The flowing chart of this study is shown in figure 1. Among 912 children aged 6–23 months on the name list, a total of 754 children and their caregivers were surveyed, with 444 being anaemic. There were 183 children aged 12–23 months agreed to draw venous blood for further laboratory tests, and 52 of them were found acute and/or chronic infections (CRP >5 mg/L in blood routine test and/or AGP >1 g/L in laboratory test). Besides, there was no statistical difference between 183 children aged 12–23 months who were taken venous blood and 101 children who refused to draw venous blood (online supplementary table 1).
Supplemental material

Flowchart of study procedures.
Characteristics of 754 surveyed children and their caregivers are shown in table 1. Nearly all main caregivers of the children surveyed were mothers and grandparents, and about 70% of mothers were Han nationality, followed by Tu and Tibetan nationality. More than 60% of mother attended junior high school, and the proportion of mothers who were illiterate was only 4.0%. More than half of grandparents were still illiterate. The main source of household income was working outside the county, followed by agriculture-related work such as growing crops, vegetables and animal husbandry.
Characteristics of surveyed children and their caregivers (n=754)
Table 2 shows the prevalence of anaemia and haemoglobin levels by age and severity in this survey. Most of the anaemic children were mildly anaemic, accounting for 76.9% of the total. The prevalence of anaemia in the 18-month to 23-month group was significantly lower than that in the 6-month to 11-month group (p=0.0026) and the 12-month to 17-month group (p=0.0261). The median haemoglobin levels in the 6-month to 11-month group and 12-month to 17-month group were lower than that in the 18-month to 23-month group (116 vs 121 g/L, p<0.0001 and p=0.0004, respectively).
Prevalence of anaemia and haemoglobin level by age and severity
Table 3 shows the results of an univariate logistic analysis of anaemia prevalence in this survey. Older children were less likely to suffer from anaemia than younger children (p=0.0028). The prevalence of anaemia in children of Tibetan nationality was significantly higher than those of Han nationality (p=0.0016). The prevalence of anaemia in children who consumed iron-rich or iron-fortified foods was significantly lower than that in children who did not consume these foods (p=0.0150). The prevalence of anaemia in children who were given meat was also significantly lower than that in children without meat (p=0.0077). Furthermore, the anaemia prevalence of children achieving minimum dietary diversity was significantly lower than that of children who did not meet the standard (p=0.0163).
Univariate logistic analysis of the prevalence of anaemia
The results of multivariate logistic analysis of anaemia prevalence in surveyed children are shown in table 4. Older children (OR=0.968, 95% CI 0.940 to 0.998) and those consuming meat (OR=0.698, 95% CI 0.499 to 0.976) were associated with lower anaemia levels, whereas children of Tibetan nationality (OR=3.123, 95% CI 1.473 to 6.623) were more likely to be anaemic.
Multivariate logistic analysis of anaemia prevalence
Results of the laboratory tests for 183 children are shown in table 5. There were 113 children with ID, accounting for 61.7%. The mean SF concentration in anaemic children was significantly lower than that in non-anaemic children (10.2±9.6 vs 22.6±15.9 ng/mL, p<0.0001). The BI store in anaemic children was significantly lower than that in non-anaemic children (−3.1±4.4 vs 2.1±3.3 mg/kg, p<0.0001). 32.6% of children with anaemia had elevated sTfR, significantly higher than that in children without anaemia (4.3%, p<0.0001). At the same time, the proportion of folic acid deficiency in anaemic children was also significantly higher than that in non-anaemic children (20.2% vs 5.3%, p=0.0024).There was no vitamin B12 deficiency either in anaemic or non-anaemic children.
Results of laboratory tests
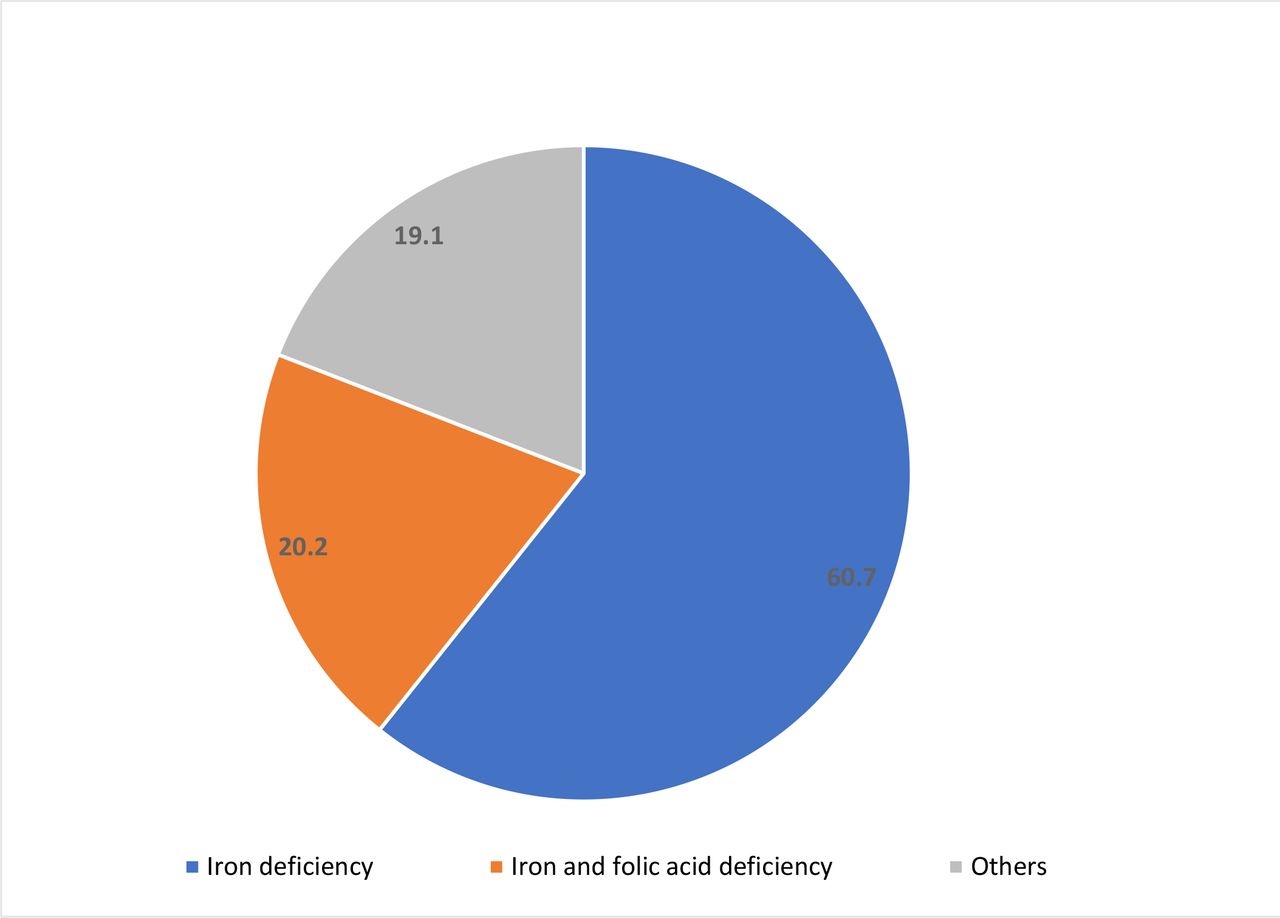
Figure 2 shows the biological causes of anaemia. 80.9% of children with anaemia were due to ID, and 20.2% of them had both iron and folic acid deficiencies. The biological causes of 19.1% anaemic children were unknown.

{kind=link}
{kind=link}
Biological causes of anaemia.
Discussion
Main findings
The anaemia prevalence of children aged 6–23 months in Huzhu County was 59.1% and most of them were mildly anaemic. The prevalence of anaemia in the 18-month to 23-month group was significantly lower than that in the 6-month to 11-month group (p=0.0026) and the 12-month to 17-month group (p=0.0261). Meanwhile, children of younger age, Tibetan nationality and not introducing meat were more likely to be anaemic. 80.9% of children with anaemia were due to ID, and 20.2% suffered from both ID and folic acid deficiency. The prevalence of ID among all children was 61.7% and 43.6% of non-anaemic children also had ID. BI stores in all children tested averaged −0.45±4.56 mg/kg. The proportion of microcytic hypochromic anaemia (mean cprpusular hemoglobin (MCH), mean corpusular volume (MCV) and mean corpuscular hemoglobin concentration (MCHC) were lower than normal value) was 13.1%. And the specificity of the combination of MCV +MCH + MCHC in the diagnosis of IDA was 100%, but its sensitivity was only 17.8%.
Influencing factors of anaemia
Children aged 6–11 months are in the transition period from exclusive breastfeeding to complementary feeding, during which the storage iron from birth is depleted and complementary foods become the main source of iron, and they were more likely to suffer from anaemia. In our study, anaemia prevalence of children at this age is the highest (64.8%).
Our analysis showed that eating meat was a protective factor of child anaemia; however, few caregivers gave meat to their children of this age due to the wrong beliefs that they could not digest meat. In addition, some caregivers did not know how to prepare meat for young infants, especially at the very beginning of complementary feeding,31 thus infant feeding counselling should include these specific issues to provide caregivers accurate knowledge and help them solve problems, such as demonstration of the preparation of meat instead of just giving information.
Compared with other nationalities, children of Tibetan nationality, who accounted for about 10% in Huzhu County, were more likely to be anaemic,14 probably because their special customs and dietary habits with the main complementary food for children being zanba (a local ethnic food consisting mainly of carbohydrates) and porridge, which contain very few irons.32 33 At the same time, poor family economic conditions would also make it unaffordable to feed animal food to their children.34
Laboratory indicators for assessment of iron status
Our study found that 80.9% of anaemic children had ID assessed by SF, but only 32.6% of these children had increased sTfR, which indicated the inconsistence of these two laboratory tests.
The WHO issued guidelines on SF cut-off for the assessment of iron status,25 which are widely used in nutrition surveys and researches in different countries. However, using sTfR to assess iron status is still controversial, as there is no internationally agreed cut-off for sTfR at present. Therefore, we mainly used ferritin to assess ID in our study.
Literatures showed that the cut-off for sTfR used in the age group of children under 3-years old are varied, such as 3.3, 4.6 and 8.3 mg/L35 36,27 A study conducted in Kenya showed that the threshold of 8.3 mg/L was better to assess the prevalence of ID in children aged 6–35 months (sensitivity 92.0%, specificity 96.0%). Therefore, we used cut-off 8.3 mg/L in our study.
Ferritin and sTfR reflect different stage of ID. We found that the results of SF and sTfR were not consistent in children aged 12–23 months. Further studies should be conducted to clarify the exact relationship between SF and sTfR in children and to explore a more effective combination of indicators to assess population iron status.
The biological causes of anaemia
The biological causes of anaemia can generally be summarised into three categories: nutritional anaemia, infectious diseases and genetic haemoglobin disorders. Nutritional anaemia results from insufficient bioavailability of hemopoietic nutrients (iron, vitamin B12, vitamin A and folic acid) needed to meet the demands of haemoglobin and erythrocyte synthesis and decreased absorption enhancers such as vitamin C. Infectious diseases include soil-transmitted helminths, malaria and schistosomiasis. Genetic haemoglobin disorders include thalassemia and haemoglobin variants, etc.17 Many previous studies have found that ID may be the most common cause of anaemia.1 6 17 37 Our study confirmed that 80.9% of anaemic children aged 12–23 months in Huzhu County were due to ID. The prevalence of ID among all children was 61.7% and BI stores in all children tested averaged only −0.45±4.56 mg/kg.
ID is a state in which iron is insufficient to maintain normal physiological functions of tissues such as blood, brain and muscle. If ID lasts too long or is serious enough, it can result in IDA.6In addition to the important role of oxygen carrier in the haeme group of haemoglobin, iron also exists in many key proteins in cells, such as cytochromes, myoglobin, neural transmitters, various enzymes and coenzymes.38 Therefore, ID not only causes anaemia, but also has many other adverse effects, especially on children in growth and development.
ID is often found in association with a deficiency of folic acid. Combined folic and ID may occur in preterm infants who are fed unfortified formula based on evaporated milk. Other study indicated that infants fed on goat's milk were also at risk.39 Our study found that 20.2% of children suffered from both ID and folic acid deficiency. Hence, attentions also need to be paid to the deficiency of folic acid. There was no vitamin B12 deficiency either in anaemic or non-anaemic children tested. However, biological causes of the remaining 19.1% of anaemic children were still unknowns and may need further explorations.
Recommendations on reducing nutritional anaemia
Deficiencies of iron and folic acid were the main biological causes of children’s anaemia in Huzhu County; therefore, feeding counselling and nutrients supplements, as biological interventions, are appropriate and should be further strengthened.
(1) Improving traditional delivery channels for infant and young child feeding (IYCF) and nutrients supplements (YYB programme).
IYCF is one of the key strategies to lower the risk of IDA in early infancy.17 40Previous studies found that inappropriate IYCF practices were common in many rural areas in China,41 42 for instance, complementary foods generally contained mainly carbohydrates and lacked protein and fat,43 or were introduced to children too early or too late, or were given in too small amounts or not frequently enough.44 45
Nutrients supplements have been commonly accepted as effective interventions in reducing child anaemia worldwide.15 46–51 In China, a domestically produced multi-nutrient powders for infants and young children called YYB was developed, and a study conducted in Gansu Province from 2001 to 2004 to test the effectiveness of this complementary food supplement showed that the use of YYB could significantly reduce the anaemia prevalence.48
The information-motivation-behaviour skills model indicates that information can be transformed into action that can motivate individuals and eventually influence their attitudes and behaviours.52 53 In China, information and knowledge about infant feeding was mainly disseminated through the traditional rural three-tier healthcare system (county–township–village). Village doctors were responsible to provide face-to-face IYCF counselling to caregivers.14 54 We conducted a controlled interventional study in Huzhu and Guinan County from 2012 to 2014, training village doctors to provide IYCF counselling and disseminating YYB to caregivers, and the results showed that the anaemia prevalence decreased more in the intervention county (receiving IYCF counselling and YYB) than in the control county (not receiving IYCF counselling and YYB, 71.1%–47.8% vs 86.3%–75.3%, respectively).15
We also found an improvement of caregivers’ feeding practice.15 Therefore, we should continue making use of the traditional health information dissemination system and measures need to be taken to further improve the quality of services, for example, conducting regular refresh training and supervision, providing monetary incentives to village doctors, and more importantly, tailoring IYCF information to the local feeding problems and special dietary habits instead of barely giving general knowledge.
(2) Exploring new channels for delivering IYCF information and disseminating YYB.
Although traditional delivery channels (mainly by village doctors) proved to be effective in our previous study, the key IYCF indicators were still low and the YYB compliance needed to be further improved47 to increase the effectiveness of the interventional programme. In addition, the sustainability of the YYB programme could also be an issue since the anaemia prevalence in Huzhu County went up from 47.8% in 2014 to 59.1% in 2018. Therefore, we need to explore new channels for delivery these interventions.
Nowadays, mobile phones and the internet have spread to millions of households in China. Data showed that, by the end of 2017, there were 1417.49 million mobile phone users and 772 million internet users, of which 753 million were smartphone internet users. The internet penetration rate reached 55.8%, of which 35.4% was in rural areas.19 Social media and smartphones have become new channels for information acquisition, and these have been widely used in many health education researches.55–57 A systematic review proved the feasibility of delivering eHealth interventions to improve health literacy skills among people with different health conditions, risk factors and socio-economic backgrounds.58 However, using eHealth or mHealth methods to deliver complementary feeding information in China is rarely reported. Therefore, further studies are needed to assess the feasibility and effectiveness of such delivery channels in improving IYCF knowledge and practice as well as YYB compliance in rural China.
Conclusions
The anaemia prevalence of children aged 6–23 months in Huzhu County was 59.1% and children of younger age, Tibetan nationality and not introducing meat were more likely to be anaemic. 80.9% of children with anaemia were due to ID, and 20.2% of them suffered from both ID and folic acid deficiency. Therefore, previous interventions of feeding counselling and nutrients supplements are appropriate and should be further strengthened.
Acknowledgments
The authors wish to thank all colleagues from the Huzhu Maternal and Child Health and Family Planning Service Center for coordination, logistic arrangements and blood routine tests, and we want to thank all students from Qinghai Institute of Health Sciences for their hard work as interviewers. We are indebted to all the mothers and caregivers who participated in our survey.
References
Footnotes
YH and LW are joint first authors.
Contributors The study was initiated, conceptualised and supervised by JH, SC and YZ. LW, YH, QW and WW collected and analysed data. LW conducted laboratory tests. YZ, YH and QW participated in the explanation and discussion of the results. The manuscript was drafted by YH, reviewed and revised by YZ, QW, SC and JH. All authors read and approved the final manuscript.
Funding The survey was funded by the United Nations Children's Fund (UNICEF). The founder was involved in study design, data interpretation, preparation of the manuscript, and decision to publish.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The study was approved by the Ethics Committee of the Capital Institute of Pediatrics (reference no.2018017). All interviewees read the Information Sheet and provided written consent on behalf of the children involved in our study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as supplementary information.