Article Text

Abstract
Objectives N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) is an unfavourable factor responsible for poor outcomes in the cardiovascular diseases. Nevertheless, the prognostic role of NT-pro-BNP in type B aortic dissection (TBAD) remains unclear. The aim of the current study was to investigate the relationship between NT-pro-BNP levels and in-hospital and long-term adverse prognosis in patients with TBAD.
Design A retrospective multicentre study.
Setting Liutie Central Hospital, Nanfang Hospital and Huiyang Hospital in China.
Participants A total of 657 consecutive patients with TBAD were enrolled in the study. NT-pro-BNP was measured at admission and included patients were divided into three groups according to the tertiles of NT-pro-BNP (pg/mL): <95 (n=220), 95–312 (n=218) and >312 (n=219).
Primary and secondary outcome measures Long-term mortality and in-hospital major adverse clinical events.
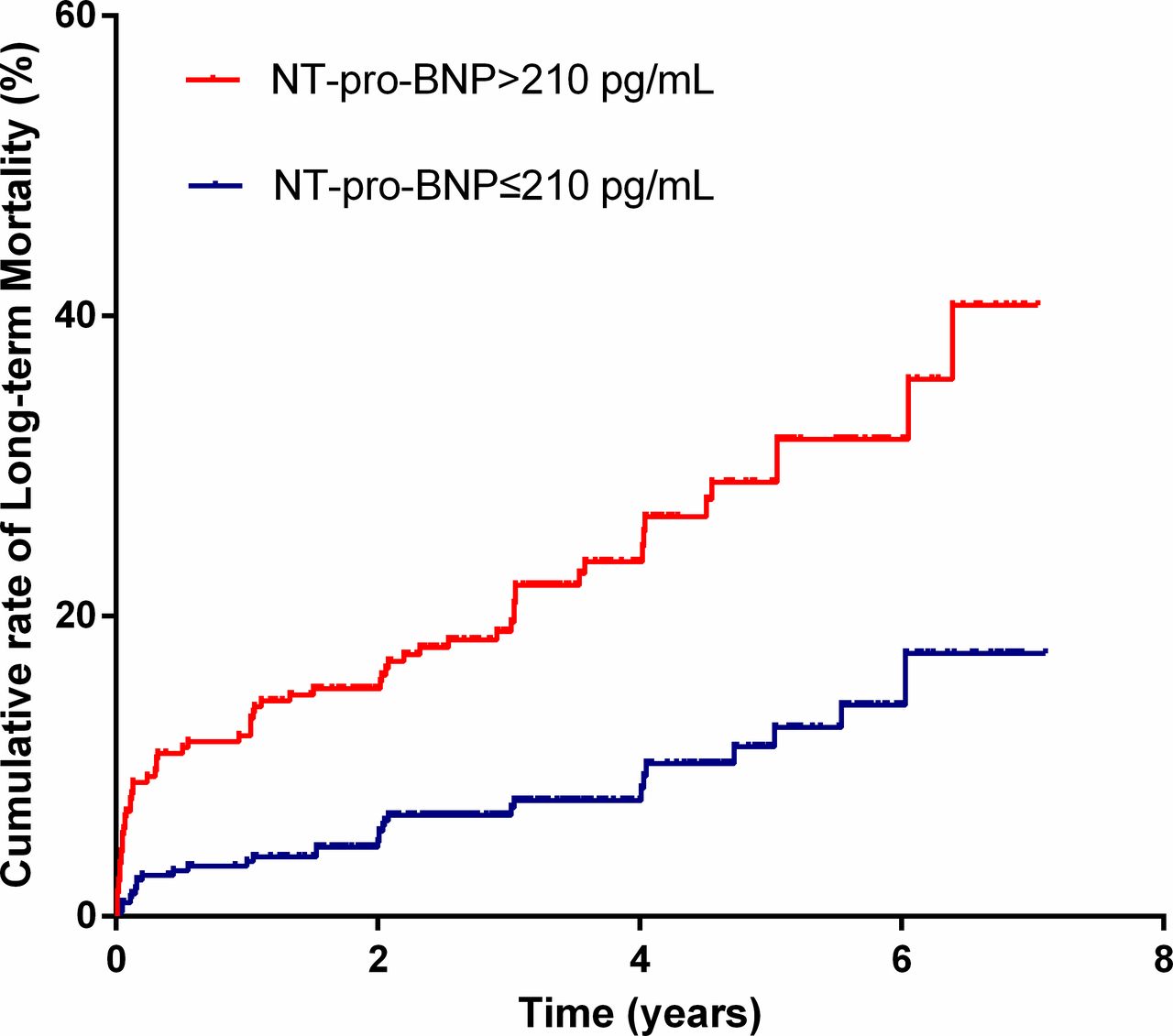
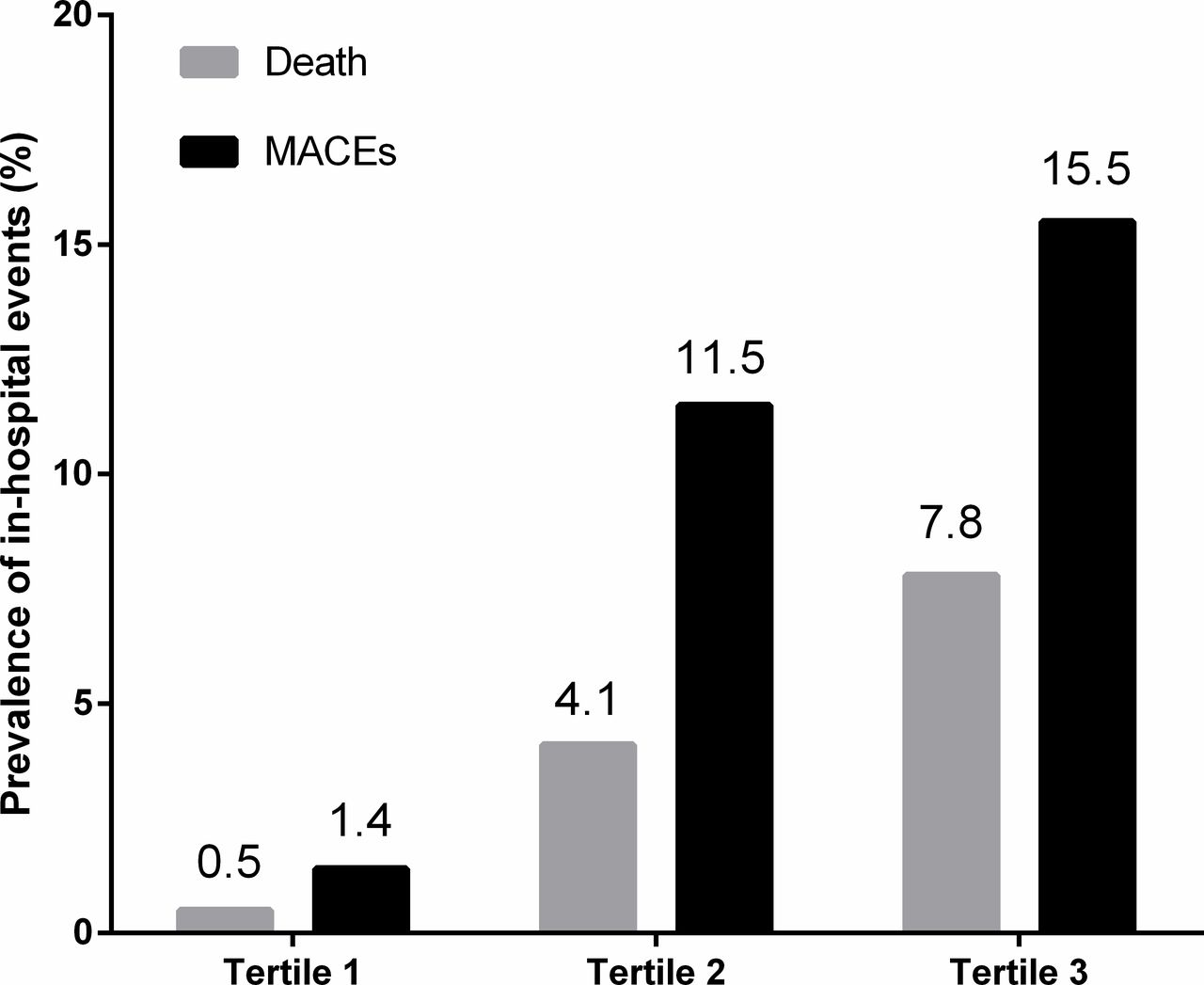
Results Overall, in-hospital death occurred in 27 patients (4.1%), which was significantly higher in upper tertiles of NT-pro-BNP (0.5% vs 4.1% vs 7.8%, p<0.001). The incident of in-hospital major adverse clinical events increased along with higher NT-pro-BNP (1.4% vs 11.5% vs 15.5%, p<0.001). NT-pro-BNP >210 pg/mL had 81.5% sensitivity and 58.6% specificity for predicting in-hospital death (area under the curve= 0.774, 95% CI 0.692 to 0.855; p<0.001). After a median of 3.1 years of follow-up, 97 (14.8%) patients died. The Kaplan-Meier analysis indicated that the long-term cumulative mortality was higher in patients with NT-pro-BNP >210 pg/mL compared with patients with NT-pro-BNP ≤210 pg/mL (log-rank=26.92, p<0.001). In multivariable Cox survival modelling, NT-pro-BNP >210 pg/mL was independently associated with long-term death (adjusted HR 2.47, 95% CI 1.45 to 4.22, p=0.001).
Conclusions NT-pro-BNP resulted as an independent predictor of adverse prognosis in patients with TBAD, thus could be used as a potential risk-stratification tool.
- Brain natriuretic peptide
- aortic dissection
- prognosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study was the first to explore the role of N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) in type B aortic dissection (TBAD) patients.
This was a multicentre study with a relatively large sample size.
This study might provide a potential risk-stratification tool in TBAD patients.
It was limited in that it was a retrospective analysis and residual risk factors may impact the present results.
The risk factors, which contributed to high NT-pro-BNP levels, were not evaluated in this study.
Introduction
Despite advances in diagnostic and therapeutic techniques, type B aortic dissection (TBAD) remains a life-threatening condition.1 Based on the epidemiological data, the in-hospital mortality of patients with TBAD treated with open surgery has been estimated to 32%, while for patients treated with thoracic endovascular aortic repair (TEVAR) it is 7% compared with 10% in patients treated only with medication.2 Mortality continues to rise during long-term follow-up, even after TEVAR.3–6 Therefore, identification of patients with a high risk of death is essential, and could assist clinicians in making accurate therapeutic plans with the aim of improving prognosis.
B-type natriuretic peptide (BNP) is a prohormone secreted by the ventricular myocardium in response to stretching,7 and is used to diagnose and to determine the severity of heart failure. N-terminal pro-BNP (NT-pro-BNP) is a more powerful predictor than BNP and has been reported as a prognostic marker for several conditions.8–12 Previous studies have indicated that patients with acute type A aortic dissection (TAAD) have significantly higher plasma NT-pro-BNP levels compared with controls.13 Also, preoperative NT-pro-BNP levels have been associated with increased risk of short-term adverse outcomes in patients with TAAD.14 15 Nevertheless, the small sample size of published studies (the largest study included 104 patients) and their lack of long-term follow-up data limit the evidence supporting the value of NT-pro-BNP as a prognostic factor in patients with aortic dissection. In addition, the prognostic value of NT-pro-BNP in TBAD remains unknown. Therefore, the aim of the present study was to investigate the relationships between NT-pro-BNP levels and in-hospital and long-term adverse prognosis in patients with TBAD on a relatively large sample size.
Materials and methods
Study population
This was a multicentre retrospective study, which included patients with TBAD treated from January 2010 to December 2015 at three hospitals in China, including Liutie Central Hospital, Nanfang Hospital and Huiyang Hospital. TBAD was diagnosed according to multidetector CT scanning. The chronic aortic dissection (onset of symptoms to treatment >90 days) was not analysed in this study.1 Patients were excluded if they had a clear aetiology, including trauma, iatrogenic injury or Marfan syndrome. Patients with a history of malignancy were also excluded. Individuals with no available admission NT-pro-BNP record were not included.
Laboratory examinations and data collection
Venous blood was collected on the admission and NT-pro-BNP was measured using a chemiluminescent immunoassay kit (Roche Diagnostics, Grenzach-Wyhlen, Germany), with a normal range of 0–125 pg/mL. Routine blood indices and serum creatinine were also tested. We calculated estimated glomerular filtration rate (eGFR) using the Chinese version of the four-variable Modification of Diet in Renal Disease equation. The demographic and clinical characteristics of study participants were collected via an electronic case report by one researcher and were randomly checked by another one. Transthoracic motion-mode, two-dimensional and Doppler echocardiographic evaluations were routinely performed within 24 hours of admission. Left ventricular ejection fraction (LVEF) was evaluated through the Simpson’s biplane method.
Thoracic endovascular aortic repair
Thoracic endovascular aortic repair (TEVAR) was performed for the patients with complicated TBAD, who presented with recurrent or refractory pain, uncontrolled hypertension despite medical treatment, rapid aortic expansion, malperfusion of the viscera or limbs, signs of rupture (haemothorax, increasing periaortic and mediastinal haematoma) or hypotension/shock.1 Other factors, such as false lumen diameter, location of the primary entry tear and retrograde component of the dissection into the aortic arch, were also considered for elective TEVAR. However, patients, who refused TEVAR due to the potential risk or cost of surgery, were treated with medication.
Patient and public involvement
Patients or public were not involved in the development of the research question and study design or conducting the present study.
Definition and endpoints
Acute TBAD was defined as time from symptom onset to hospital admission <14 days.1 Anaemia was defined as a haemoglobin value <120 g/L in men or <110 g/L in women. After discharge, all survived patients were followed up by the trained nurses via telephone interviews or visits to clinics from October 2016 to April 2017. Long-term mortality was defined as all the death causes that occurred during follow-up after a diagnosis of TBAD. The occurrences of other events, such as in-hospital death, stroke and dialysis, were also recorded. In-hospital major adverse clinical events (MACEs) were a composite endpoint, including in-hospital death, stroke and dialysis.
Statistical analyses
All data are presented as mean±SD or median (IQR) for continuous variables, or as number (percentage) for categorical variables. Continuous data were compared using analysis of variance or Wilcoxon rank-sum tests, while categorical data were evaluated using the χ2 test. Predictive value was evaluated by generating receiver operating characteristic (ROC) curves. Survival during long-term follow-up was analysed using the Kaplan-Meier curve method and compared among groups using the log-rank test. Univariate Cox survival analysis was used to determine risk factors for long-term mortality. Variables with p<0.05 in univariate analysis were included in the multivariable Cox survival model, and adjusted ORs and 95% CIs were calculated. A p<0.05 was considered statistically significant. Statistical analyses were performed using SPSS V.13.0 (SPSS).
Results
Baseline clinical characteristics
The final study population included 657 patients (mean age, 57±11 years) with admission NT-pro-BNP records, which were classified into three groups according to tertiles of NT-pro-BNP levels (pg/mL): <95 (low; n=220), 95–312 (medium; n=218) and >312 (high; n=219). The baseline clinical characteristics of the study population are presented in table 1. Patient age increased with increasing NT-pro-BNP level (53.7±9.7 vs 57.8±11.3 vs 59.5±12.1 years, in the low, medium and high group, respectively; p<0.001). The rate of acute TBAD was 87.5%, which was higher in the upper tertiles. Admission systolic blood pressure (SBP), pulse pressure, heart rate, white cell count and C reactive protein (CRP) were significantly higher in patients with high NT-pro-BNP levels, who also had lower haemoglobin, eGFR and LVEF values. In addition, there was a significantly higher prevalence of preexisting coronary heart disease, complicated TBAD, anaemia, LVEF <50% and pleural effusion among patients with levels of NT-pro-BNP in the upper tertiles.
Baseline clinical characteristics according to the tertiles of NT-pro-BNP levels
NT-pro-BNP and clinical outcomes
Overall, in-hospital death occurred in 27 patients (4.1%), and both in-hospital death (low, medium, high groups, 0.5%, 4.1% and 7.8%, respectively, p<0.001; figure 1) and in-hospital MACEs (low, medium, high groups, 1.4% vs 11.5% vs 15.5%, respectively, p<0.001) more commonly occurred in patients with levels of NT-pro-BNP in the upper tertiles; the observed differences were statistically significant. Analysis of the value of NT-pro-BNP for predicting in-hospital death yielded an area under the curve (AUC) of 0.774 (95% CI 0.692 to 0.855, p<0.001; figure 2). Moreover, the optimal cut-off NT-pro-BNP value was 210 pg/mL, with 81.5% sensitivity and 58.6% specificity. In addition, NT-pro-BNP had a similar power with D-dimer in predicting in-hospital death (AUC: 0.774 vs 0.748, p>0.05).

Prevalence of in-hospital events. MACEs, major adverse clinical events.

ROC curves of NT-pro-BNP and D-dimer for predicting in-hospital mortality. NT-pro-BNP, N-terminal pro-B-type natriuretic peptide; ROC, receiver operating characteristic.
Clinical outcome data were available for 594 patients (90.4%), with a median follow-up duration of 3.1 years. During the follow-up, 97 (14.8%) patients died. Kaplan-Meier analysis indicated that the long-term cumulative mortality was higher in patients with NT-pro-BNP >210 pg/mL compared with patients with NT-pro-BNP ≤210 pg/mL (log-rank=26.92, p<0.001; figure 3). In univariable Cox analysis, eight variables were significantly associated with long-term mortality: NT-pro-BNP, age, female, preexisting coronary heart disease, previous stroke, pulse pressure, anaemia, eGFR <60 mL/min/1.73 m2, LVEF, superior mesenteric artery affected and receiving TEVAR (table 2). In multivariable Cox survival modelling, log(NT-pro-BNP) was independently associated with long-term mortality (adjusted HR 1.77, 95% CI 1.24 to 2.52, p=0.002). Similar results were found when NT-pro-BNP >210 pg/mL replaced log(NT-pro-BNP) as a binary variable in model 2 (adjusted HR 2.47, 95% CI 1.45 to 4.22, p=0.001, table 3). ROC curve analysis showed that NT-pro-BNP had a higher predictive power for long-term death than D-dimer (AUC: 0.694 vs 0.547, p<0.001). In addition, subgroup analysis revealed that NT-pro-BNP remained as a predictor for long-term death in patients receiving TEVAR (AUC 0.682, 95% CI 0.609 to 0.754, p<0.001) or in those receiving conservative treatment (AUC 0.674, 95% CI 0.583 to 0.764, p<0.001).
{kind=link}
{kind=link}
{kind=link}
Cumulative mortality in the entire study cohort according to NT-pro-BNP cut-off. NT-pro-BNP, N-terminal pro-B-type natriuretic peptide.
Univariable COX survival analysis of factors associated with long-term mortality
Multivariable COX survival analysis of factors associated with long-term mortality
Discussion
The current study is the first to explore the prognostic value of NT-pro-BNP in patients with TBAD using a relatively large sample size. NT-pro-BNP was associated with increased risk of in-hospital and long-term mortality. In addition, NT-pro-BNP >210 pg/mL was a significant predictor of long-term mortality.
TBAD involving the descending aorta or the arch is a catastrophic condition that is most commonly treated with TEVAR. Nevertheless, studies with long-term follow-up have reported relatively high mortality rates. In this study, the long-term mortality was 10.7% in patients receiving TEVAR and 14% in those being treated only with drugs. Many factors have been identified as responsible for high mortality in these patients.16 17 However, high-risk patients have remained indistinguishable due to the different sensitivities of the previous markers. Therefore, finding a novel and simple biomarker for risk stratification is of utmost importance.
Levels of NT-pro-BNP or BNP, which are already used as prognostic factors for cardiovascular diseases, and even for some non-cardiac conditions,8–12 could be potentially used for risk stratification. To the best of our knowledge, Sbarouni et al were the first to apply NT-pro-BNP in aortic dissection. Their study included 18 patients with TAAD and 8 healthy subjects, and NT-pro-BNP levels were significantly higher in patients with TAAD.13 Subsequently, Zhang et al explored the prognostic value of NT-pro-BNP in 67 patients with TAAD and suggested that it should be considered as a predictor for in-hospital mortality.15 Another study on 104 patients with TAAD undergoing emergency surgery showed that increased preoperative NT-pro-BNP levels were associated with higher risk of short-term adverse events14; yet, the small sample sizes and lack of long-term follow-up data in previous reports limit the evidence supporting the prognostic value of NT-pro-BNP in patients with aortic dissection. If these findings were relevant to patients with TBAD remained unclear. The current study revealed that NT-pro-BNP is an independent predictor for in-hospital and long-term mortality in patients with TBAD.
Although the mechanism underlying the association of NT-pro-BNP levels and prognosis in TBAD remains unclear, the following factors may account for this finding. First, increased levels of NT-pro-BNP are a marker of renal dysfunction due to decreased excretion from the kidneys. In studies on aortic dissection, renal impairment on admission has been associated with increased risk of postoperative renal failure and with in-hospital and long-term mortality.18 19 In the present study, a linear correlation was observed between NT-pro-BNP and admission serum creatinine; however, this cannot be the only contributing factor, because the effect of NT-pro-BNP on long-term mortality was not eliminated by including renal dysfunction into multivariate Cox analysis. Second, aortic dissection is defined as the separation between the layers of the aortic wall, resulting in luminal stenosis and decreased blood supply to organs. The latter, and consequent sharp pain, further activate the sympathetic nervous and renin–angiotensin systems.20 All of these factors could cause increased blood pressure and strain on the left ventricular myocardium, leading to elevated secretion of NT-pro-BNP. Refractory hypertension has been associated with adverse outcomes in acute aortic dissection.21 22 In our analysis, we identified a significant positive association between admission SBP and increasing NT-pro-BNP concentration. NT-pro-BNP levels may reflect this high pressure load, thus indicating poor prognosis. Third, a previous study has shown that inflammation is an important risk factor in aortic dissection.23 Changes in systemic inflammatory markers, such as interleukin-6, CRP, tumour necrosis factor-a and matrix metalloproteinase-9, are associated with acute-phase reactions in aortic dissection, even when stenting has been performed.24 Inflammatory cytokines may also have direct effects on BNP transcription and translation in cardiomyocytes.25 In this analysis, we observed a trend towards a positive association between CRP and increasing NT-pro-BNP levels. Higher NT-pro-BNP was an indicator of inflammation, which contributes to poor prognosis. Finally, increased BNP also has direct adverse effects. Zhang et al have demonstrated that high BNP expression levels promote cardiomyocyte apoptosis by activating the caspase-1/interleukin-1B signalling pathway.26 BNP can also enhance mild hypoxia-induced cardiomyocyte apoptosis by downregulating the expression of Bcl2 mRNA.27
However, several limitations should be considered when seeking to generalise the results of the present study. First, though multivariable analysis was performed to eliminate possible confounding effects, residual risk factors may impact the present results due to the inherent weakness of the retrospective study design. Second, we did not evaluate the risk factors which contributed to high NT-pro-BNP levels. Third, the definite mechanism underlying the adverse effects of NT-pro-BNP in aortic dissection remains unclear and requires to be further studied. Finally, the effect of NT-pro-BNP was explored only in patients with acute and subacute TBAD; thus, it remains to be seen whether it can be extrapolated to other groups.
Conclusion
In this study, we explored the prognostic value of NT-pro-BNP levels in patients with TBAD. Increased NT-pro-BNP was associated with high risk of in-hospital and long-term mortality. These results support the routine application of NT-pro-BNP as a risk-stratification tool for patients with TBAD, while in patients with high NT-pro-BNP, it should be given additional attention.
References
Footnotes
CL, JZ and SX are joint first authors.
Contributors KF contributed to the conception or design of the study. CL, JZ, SX, ZK, JZ, YS and BQ contributed to the acquisition, analysis or interpretation of data. CL and JZ drafted the manuscript. KF and SX critically revised the manuscript. All the authors gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Funding This study was supported by projects of provincial health and family planning commission of Guangxi (no. Z2016271/Z20170024/Z20170021).
Disclaimer The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Institutional Ethics Committee of Liutie Central Hospital (2017–15), with a waiver of informed consent due to retrospective study design. The central ethic approval was applicable to the other collaborating hospitals as well.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.