Article Text

Abstract
Objective To find out if there is evidence on interventions to prevent aggression against doctors.
Design This systematic review searched the literature and reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Data sources Pubmed, Embase, Turning Research into Practice (TRIP), Cochrane and Psycharticle, GoogleScholar and www.guideline.gov were consulted.
Eligibility criteria Abstracts published in English between January 2000 and January 2018 were screened. Eligible studies focused on prevention and risk factors of type II workplace violence in general healthcare, psychiatric departments, emergency departments, emergency primary care, general practice.
Data extraction and synthesis The selected intervention studies were grouped into quantitative and qualitative studies. Systematic reviews were reported separately. For each study, the design, type of intervention and key findings were analysed. Quality rating was based on Grading of Recommendations, Assessment, Development and Evaluation (GRADE) and GRADE-Confidence in the Evidence from Reviews of Qualitative Research (CERQUAL).
Results 44 studies are included. One randomised controlled trial (RCT) provided moderate evidence that a violence prevention programme was effective in decreasing risks of violence. Major risk factors are long waiting times, discrepancy between patients’ expectations and services, substance abuse by the patient and psychiatric conditions. Appropriate workplace design and policies aim to reduce risk factors but there is no hard evidence on the effectiveness. One RCT provided evidence that a patient risk assessment combined with tailored actions decreased severe aggression events in psychiatric wards. Applying de-escalation techniques during an aggressive event is highly recommended. Postincident reporting followed by root cause analysis of the incident provides the basic input for review and optimisation of violence prevention programmes.
Conclusions This review documented interventions to prevent and de-escalate aggression against doctors. Aggression against physicians is a serious occupational hazard. There is moderate evidence that an integrated violence prevention programme decreases the risks of patient-to-worker violence. The review failed to gather sufficient numerical data to perform a meta-analysis. A large-scale cohort study would add to a better understanding of the effectiveness of interventions.
- aggression
- general practitioner
- workplace violence
- interventions
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
As compared with other reviews, this systematic review succeeded in inventorying and documenting all known interventions to prevent and de-escalate aggression against doctors.
The literature search was performed through a wide range of available medical databases. Research in this area requires quantitative as well as qualitative methodological approaches and therefore both types of publications were included, focusing on violent incidence rates and on the why and how an intervention could work.
The review failed to gather sufficient numerical data to perform a meta-analysis.
Introduction
Aggression against physicians including verbal, physical and psychological aggression is a well-known and serious occupational hazard. The prevalence of violence in healthcare is extensively documented in various settings and populations. Subjective interpretation of violent behaviour and under-reporting of workplace violence is consistently cited in literature.
A large, nationwide Australian study Balancing Employment and Life (MABEL) reported on the 12-month prevalence of verbal or written and physical aggression in Australian clinical medical practice: 70.6% of 9951 Australian doctors had experienced verbal or written aggression and 32.3% had experienced physical aggression in the previous 12 months. The 12-month prevalence of aggression towards general practitioners (GPs) was 54.9% for verbal aggression and 23.4% for physical aggression.1 In a survey in the UK 78% of all GPs experienced at least one verbal incident in the previous 2 years.2 A recent cross-sectional study among Flemish GPs showed that only about 5% never encountered aggression. In most cases, the aggression was verbal, however, about 20% of the GPs reported physical aggression and almost 8% reported sexual aggression.3
A recent nationwide German survey reported that 91% of GPs had faced aggression at least once in their career and 73% in the previous 12 months.4 Typically, the highest rates of physical aggression were found in emergency departments (EDs) and in psychiatric units. A recent systematic review and meta-analysis showed a pooled incidence of 36 of every 10 000 patient encounters in the ED of which 44% was associated with drug and alcohol exposure.5 More than a quarter of emergency physicians reported that they were victims of physical assault in the past year.6 A large randomised controlled trial (RCT) in a hospital setting identified between 8 and 15 reported violence events per 100 full-time equivalent staff members per year.7
In the healthcare setting, the most common type of workplace violence is where the aggressor is a patient or a relative of the patient. These events are categorised in literature as ‘type II workplace violence’. Exposure to workplace violence can lead to physical and psychological injury, reduced job satisfaction and detachment, and affect the quality of care.
Although the impact of workplace-related aggression is considerable and well documented, there is no systematic evidence on how to prevent, intervene and approach hazardous situations. Despite the heterogeneity in scientific and event reports about workplace-related violence, there is consensus that safety action plans should be established and implemented. Therefore, the primary research question in this study is: ‘What are interventions to prevent aggression against doctors in general and against the general practitioner in particular?’.
Methods
This systematic review is performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.8 The risk of bias for randomised controlled studies was assessed and reported using the Cochrane classification scheme for bias.9
Eligibility and inclusion criteria
Abstracts published in English between January 2000 and April 2019 were screened for inclusion. Eligible studies focused on prevention of type II workplace violence: verbal, physical and psychological aggression from a patient or a patient’s relative towards a healthcare worker. Studies focusing on ‘aggression’ by co-workers were excluded.
Qualitative and quantitative intervention studies were included. Systematic reviews and reviews on prevention strategies were included. Single case reports or opinion articles were excluded.
The target population was defined as healthcare workers in general healthcare, psychiatric departments, EDs, emergency primary care, general practice. Eligible interventions were focusing on risk factors, workplace violence prevention or strategies to reduce workplace violence. Comparison was defined as usual care and as strategy in case of reporting of a hazardous situation.
For evaluation of the effectiveness of interventions, the primary outcome was patient aggression towards healthcare workers. Secondary outcomes were risk factors, staff knowledge, staff skills and early detection of aggressive behaviour. The major findings were extracted and discussed as per the type of intervention.
Search strategy
Databases used were Pubmed, Embase, Turning Research into Practice (TRIP), Cochrane and Psycharticle with different search strategies (online supplementary appendix). The following search terms/Mesh terms were used: aggression, violence, physician, doctor, workplace, prevent*, strateg*, intervent*, general practitioner, health care. The reference list of articles was scanned additionally. A separate search was performed on Google Scholar and www.guideline.gov using the same search terms.
Supplemental material
Data collection and analysis
The selected intervention studies were grouped into two groups: quantitative and qualitative studies. Systematic reviews were reported separately. For each selected study, the design, type of intervention and key findings were analysed. A level of evidence was attributed to each quantitative study based on the Oxford 2011 Levels of Evidence.10 Quantitative studies were rated according to GRADE.11 12 For qualitative studies the GRADE-CERQUAL approach was used to assess quality.13
Patient and public involvement
Patients were not actively involved in this literature research. In a prior master thesis research, need assessment was conducted in general practice.
Results
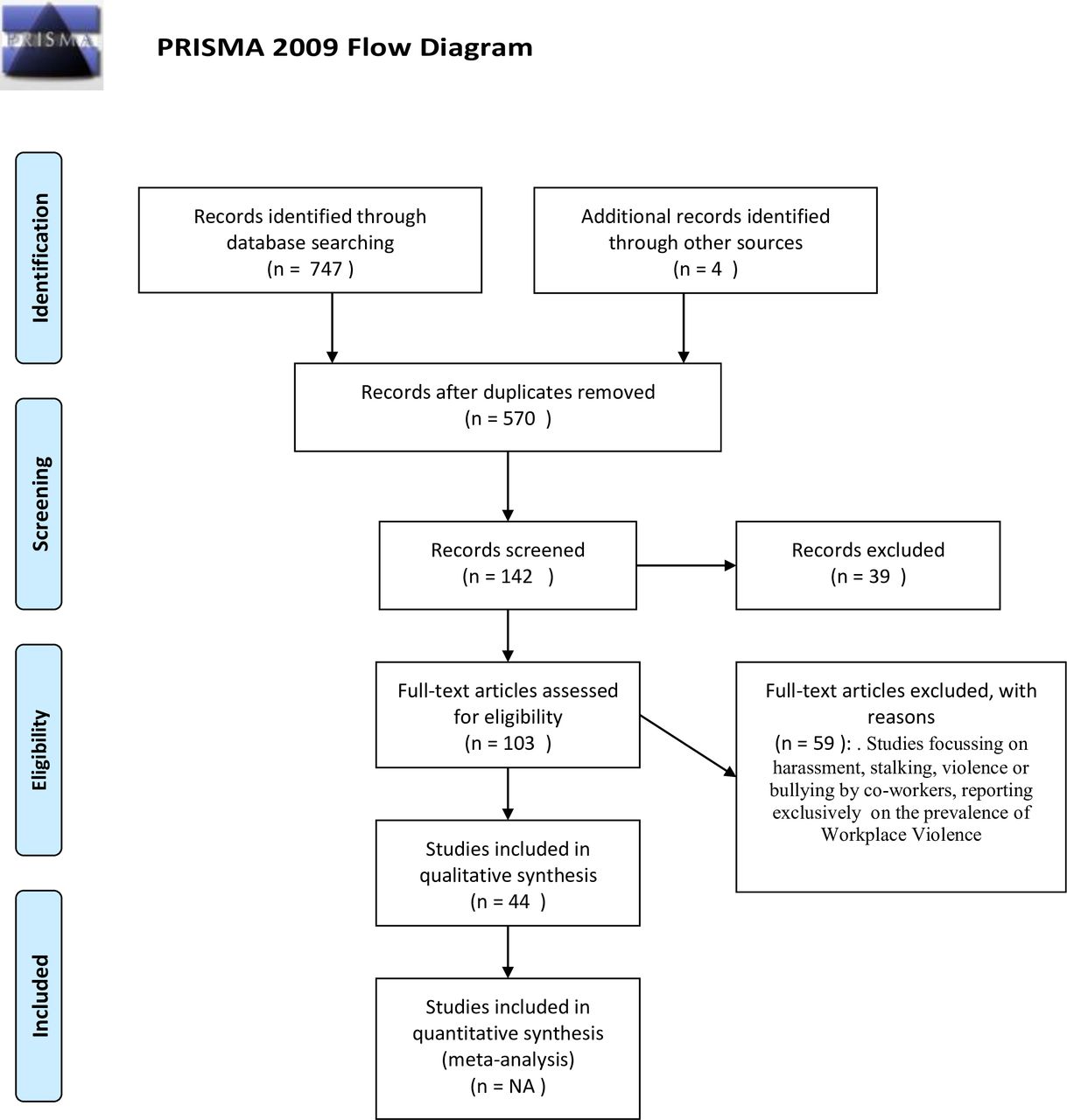
The total harvest of articles is presented in (online supplementary appendix 1). In total 105 full-text articles were read and assessed for eligibility. Forty-four studies (15 quantitative studies, 15 qualitative studies, 7 systematic reviews and 7 reviews) were included in this review (figure 1).
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of record screening and inclusion (adapted from Moher et al [8]).
Summary of results
The results of the quantitative studies are presented in table 1, the results of the qualitative studies in table 2. Table 3 summarises the systematic reviews and other reviews. Table 4 gives an overview of frequently cited guidelines. Table 5 summarises the factors that may increase the risk of workplace violence.
Summary of selected quantitative studies
Summary of selected qualitative studies GRADE-CERQual assessment
Summary of reviews and systematic reviews
Overview of relevant guidelines
Risk factors that increase the risk of occupational violence 4 18–22 30 33 52 54 56 60 68–71
Studies reporting on interventions
The interventions most frequently discussed and evaluated are grouped. The first group of interventions was labelled as pre-event preventive measures: components of an integrated violence prevention programme. The second group was labelled as interventions taking place during a violent event: applying de-escalation techniques and activating specific violence emergency procedures. The third group was labelled as postincident interventions: incident reporting followed by root cause analysis of the incident and review of the violence prevention policy.
Pre-event preventive measures
Under this label two types of interventions were identified: violence prevention programmes and risk assessment and control measures.
Violence prevention programmes
A variety of violence prevention programmes has been developed in order to prevent workplace violence and to manage and mitigate the impact of violence at work. All programmes propose an integrated approach incorporating basic elements such as a worksite risk analysis, hazard prevention and control measures, safety training and education, violent event reporting and evaluation. Some programmes explicitly apply the Plan-Do-Check-Act model of continuous quality improvement.
Arnetz et al investigated in a large RCT the effect of the Plan-Do-Check-Act model through a data-driven worksite-based intervention in 41 units across seven US hospitals over a period of 5 years.7 The study provided moderate evidence of this approach in decreasing risks of patient-to-worker violence and related injury at 6 months postintervention: the incident rate ratio (IRR) of violent events was significantly lower in intervention units compared with control units (IRR 0.48, 95% CI 0.29 to 0.80). However, this effect was not confirmed over time during the 24-month follow-up period. At that time, only violence-related injury was lower in intervention units compared with control units (IRR 0.37, 95% CI 0.17 to 0.83). Lipscomb et al evaluated in a 4-year study the impact of the implementation of the Occupational Safety and Health Administration (OSHA) guidelines and compared three intervention groups with three control groups in mental health facilities.14 Both the intervention and the control groups implemented safety preventions but the control group did not benefit from the additional support of the project team on violence prevention. The staff reported in both groups significant improvements in OSHA elements: management commitment, employee involvement and hazard assessment, and hazard control activities. Intervention facilities also reported significant improvement in the training element. There was no significant reduction in physical assaults in the intervention and the control groups. There was a significant increase in threats in the intervention group (+98%, p<0.001). The authors attribute this unexpected finding to an increased tendency to report less severe events.
Mohr et al investigated in a longitudinal study in 138 veteran healthcare facilities the impact of the implementation of a workplace violence prevention programme.15 Overall, there was no significant change in assault rates over time. Training led to a significant but moderate 5% reduction in standardised incidence rate. The authors argue that the large variation across the facilities and the under-reporting prior to the workplace violence prevention programme explain the results. Magnavita et al studied the effect of an aggression minimisation programme in a small-scale psychiatric unit in Italy. The interventions included changes in architecture and work organisation and training of employees. A stable and significant reduction in assault rate per employee from 0.24 to 0.04 per year was reported.16
Risk assessment and risk control measures
Violence risk assessment and violence management are intrinsically connected. The risk factors can be categorised based on their source of origin: workplace design, work organisation, patient factors, physician factors and social context. Numerous studies confirmed the following items as main risk factors for aggression: long waiting times, discrepancy between patients’ expectations and the services offered, alcohol or drug abuse by the patient, and psychiatric condition (table 5).
Subsequent to the specific violence risk assessment, the next step is applying appropriate risk control measures. Changes to the physical environment and work policies are based on situational crime prevention and aim to increase the effort of criminal activity, increase the risk of getting caught, reduce the rewards of criminal activity, reduce provocations and remove excuses for disruptive and violent behaviour.17
The proposed changes to physical environment vary across the different healthcare settings and include effective indoor and outdoor lighting, sufficient exit routes, physical barriers for receptionists, automatic door locks, video cameras, panic buttons, portable alarms and comfortable waiting areas to reduce stress. No concrete evidence exists on the effectiveness of these interventions.6 18–21 In some emergency departments in USA, metal detectors have been installed, and although they may theoretically mitigate violence, there is no concrete evidence to support this assumption.6
Adequate work policies include ‘zero tolerance’ policies, incident reporting, training of staff, adequate staffing, policies on drug prescription and storage, a roadmap when faced with aggressive behaviour and additional measures for out-of-hours services. Drugs, cash and prescriptions should be stored in locked places and in limited amounts. Long waiting times should be managed by expanding the staff during busy periods and by setting up courtesy message systems to alert patients about delay.20 22 Some guidelines and studies propose a ‘zero tolerance policy’ with explicit statements and warning signs stating that violence will not be tolerated. It is important to recognise verbal assault as a form of workplace violence since it is a risk factor for physical violence.20 Some authors advise to restrict or withdraw access to general practice or emergency department services for patients with a history of violence.17 However, this also might compromise the ‘equality of access to care’ principle and there is no evidence of the impact on violence reduction. GPs should take additional measures for after-hours house call services such as using a central dispatch centre or a shared visit schedule and tracking system. Additional support might be provided in certain circumstances or on request of the GP.
Ifediora et al investigated the implementation of safety measures by GPs on after-hours call services in Australia: overall 43% of the doctors adopted protection measures and for after-hours house calls, 34% used additional chaperones or security personnel. The study did not investigate the impact of these measures on violence incidents.23 Morken et al investigated in a cross-sectional study the implementation of 22 safety recommendations in 210 emergency primary care centres in Norway. The study provided evidence on the perceived usefulness and feasibility of the recommendations.24
Training of staff in communication skills, violence and de-escalation techniques should be included in a comprehensive violence prevention programme. Effective training on de-escalation should focus on cognitive, affective and practical skills based improvements in behaviour and reaction in case of an assault. Self-awareness and the ability to connect interpersonally with the aggressor are crucial. Price et al investigated in a systematic review, the cognitive and affective outcome and the effectiveness of training on violence. There is currently limited evidence that this training has an effect on de-escalation of aggressive behaviour.25 As discussed hereafter, de-escalation is a highly specialised intervention and this might explain the limited effectiveness of the training programmes.26
With respect to patient risk factors, the risk of violence is dynamic and contextual.27 Violence in medical healthcare is mostly impulsive and accompanied by the fight-flight response although premeditated aggression also occurs. Risk assessment tools focusing on patient aggression have shown to be effective as a predictor for short-term violence. Abderhalden et al investigated in an RCT the use of short-term risk assessment in 14 acute psychiatric wards in Switzerland. The intervention consisted of structured risk assessment twice a day followed by communication of risk scores and recommendation for actions tailored to the risk level. The study showed a significant reduction in severe events of patient aggression, a significant reduction in attacks and a significantly reduced need for coercive measures.28 Flagging patients with a history of violent events resulted in 90% reduction in assaults by high-risk patients in veteran healthcare hospitals in USA.29
Interventions during the event
During the event of violence the following recommendations are described in the guidelines: stay calm and apply de-escalation techniques, if de-escalation fails, take care of your own safety, go away or use self-defence techniques and activate the emergency procedure (references in table 4).
The use of restrictive interventions should only be applied in accordance with pre-established protocols and in a manner that complies with the human rights.
De-escalation is, in the medical care sector and in other settings, a highly recommended component of violence prevention. Garriga et al (Table 3) carried out a systematic review on assessment and management of agitation in psychiatry.30 After identification of possible medical causes for agitation, verbal de-escalation and environmental modification are first-choice interventions.
As established by Richmond et al, de-escalation can be successful in less than 5 min. Non-coercive de-escalation is executed in a three-step approach: first, the patient is verbally engaged, second, a collaborative relationship is established and third, the patient is verbally de-escalated out of the agitated state.31 De-escalation frequently takes the form of a verbal loop in which the clinician listens to the patient, finds a way to respond acknowledging the patient’s position and then states what he wants the patient to do. The clinician might have to repeat the loop a dozen or more times and inexperienced clinicians tend to give up.26
Similar principles of de-escalation have also been described by Kohlrieser, a psychologist and hostage negotiator.32
Postincident measures
As studied by Geoffrion et al individual and organisational factors can lead to trivialisation of workplace violence, a culture of silence and under-reporting of workplace violence. Two aspects play a role in trivialisation of workplace violence: normalisation of violence as being ‘part of the job’ and taboo by avoiding an open discussion out of fear of being stigmatised as incompetent. Colleague and employer support, training on violence, zero tolerance policy all, contribute to normalisation of violence and decrease the likelihood of taboo. Organisations should be aware of this paradox implicitly arisen by sending the message that violence is to be expected.33
Reflecting on incidents or performing a root cause analysis in team-specific workshops can identify systematic weaknesses and potential solutions, action plans and revision of the workplace violence policy.34
Organisations should provide support and assistance to victims and address short-term and long-term consequences. Schat et al investigated the effect of organisational support in reducing the negative consequences of workplace violence and found a small positive effect on emotional well-being, somatic health and job-related affect but there was no effect on fear of future violence and on job neglect.35
Discussion
Summary of main results
This review demonstrated that only few studies have been successful in providing evidence on the efficacy of interventions to prevent aggression against doctors and more specifically against the GP. Only one RCT provided moderate evidence that a violence prevention programme was effective in decreasing the risks of patient-to-worker violence and of related injury.7 In contrast, longitudinal studies showed conflicting results in assault rates after implementation of a workplace violence prevention programme.15 29 36 Appropriate workplace design and work policies aim to reduce risk factors for violence such as long waiting times and crowded waiting areas but there is a lack of evidence on the effectiveness of the interventions.6 19–21 During the event of violence or agitation, applying de-escalation techniques is a highly recommended component of violence prevention. Physical restraint should be considered as a last resort strategy.30 Postincident interventions such as incident reporting followed by a root cause analysis of the incident provides the basic input for review and optimisation of the violence prevention programme.
This review included quantitative and qualitative studies, focusing on violence incidence rates and on why and how an intervention works. Although there is a lack of hard evidence on the effectiveness of occupational health and safety management systems, there is a wide consensus that the implementation of a comprehensive health and safety prevention plan is the key to understanding, preventing and dealing with workplace violence.37 As stated by James in his book Violence Assessment and Intervention: ‘Preparation is critical as long as you accept that whatever you plan for and however you plan for it to occur, will never happen. Preparation is the ‘primer’ to get you propelled toward resolve and is important in addressing a crisis.’38
A work site-specific violence risk assessment provides the basic input for interventions. The focus of prevention and intervention goes to both the clinician and to logistics or infrastructure. Major risk factors for violence are long waiting times, discrepancy between patients’ expectations and the services offered, alcohol or drug abuse by the patient or a psychiatric condition. Specific risk control measures on the policy level to ensure adequate staffing and to reduce waiting times and training personnel in de-escalation seem rational interventions even without hard evidence.
The dynamic nature of risks feeds the issue of unintended consequences or the ‘intervention dilemma’. This dilemma states that any intervention has the capacity to either reduce the risk or not affect it or even intensify the risk.27 On the level of workplace design and work policies, 100% security will never be obtained. A balance has to be made between safety and quality of life and quality of care.38 Some interventions proposed to increase safety might be in conflict with the goals of healthcare. For example, a zero tolerance policy or flagging patients with violent history can lead to stigmatisation of the patient and can be in conflict with patient confidentiality and the right to medical care. Implementation of overt measures such as security guards or barricades between staff and patients might impair the doctor-patient relationship, which can lead to a spiral of fearfulness and suspicion and ultimately to an increased risk on violence. Evidence suggests that individuals carrying an increased risk for violent behaviour are not violent at all times or in all situations.19
De-escalation, if undertaken with a sincere commitment and with the goal of ‘helping the patient calm himself’ proved to be successful in far more cases than previously assumed and this strategy can be successful in less than 5 min.30 31 De-escalation is a complex and time-consuming intervention and this might explain the limited effectiveness of the training programmes.26
Under-reporting is a well-known issue in workplace violence management. It is partly due to normalisation of violence as being part of the job and to the taboo associated with complaining about violence. Under-reporting is also influenced by the interventions themselves and complicates research outcome and the interpretation of results.
Victims of type II workplace violence should be assisted and supported by their organisation and short-term and long term consequences should be addressed.35 A decline in frequency of assaults occurs after implementation of a peer help programme for assaulted staff.39 The unavailability of debriefing is associated with increased reports of post-traumatic stress.40 ,41
Limitations
The first limitation lies in the risk of bias across studies since mainly English and some French, German and Dutch publications were screened. Second, research on workplace violence is published in the traditional international medical scientific literature databases. The second limitation is the publication date, the literature search started in 2000. This starting time was chosen ad random. To compensate however for any loss of data before this date, the very comprehensive review of Runyan et al, published in the year 2000 was included in the analysis of this review. The third limitation lies in the risk of bias within studies. Only three RCTs are included in this review.7 28 42 Performance bias, detection bias and reporting bias are present in all studies. Due to the nature of the problem and of the interventions, allocation concealment, blinding of participants and blinding of outcome is not possible. Also as discussed in this review, under-reporting and selective reporting, a well-known issue in workplace violence, is variably present in all studies and is influenced by the intervention itself.7 Recall bias is also present due to data collection inquiring about violent events over the past 12 months.42 Finally, performance bias is present in all studies through various mechanisms: a medical care setting is a complex structure and organisational changes might have an impact on care quality and on safety performance and might interfere as a co-intervention.43 Moreover, in all RCTs, the control group will always have its own safety prevention policy.
Suggestions for further research
We believe that a large and long-term cohort study could provide more insight and evidence on effective interventions to prevent aggression against the GP. Risk factors for type II workplace violence are well known but there are insufficient data on protective factors for aggression against doctors. Analysis of large data sets of a cohort should provide insight in the protective factors and effectiveness of interventions against type II workplace violence.
A yearly audit on context of aggression incidents and on the applied safety measures per general practice will add to map effective preventive measures. Basic information about recommended safety prevention measures and training on de-escalation techniques should be offered to the cohort. With respect to postevent interventions, the GPs in the study cohort could implement a shared violence incident-reporting tool.
Conclusion
Aggression against physicians is a well-known and serious occupational hazard. There is moderate evidence that an integrated violence prevention programme can decrease the risks of patient-to-worker violence. Appropriate workplace design and work policies aiming to reduce risk factors and applying de-escalation techniques during an event of aggression are highly recommended. Considering that detection, reporting and performance bias are inherent to any RCT on interventions against type II workplace violence, we believe that a large cohort study would provide more evidence on the effectiveness of the interventions.
References
Footnotes
Contributors AR: setting up the design and method, data acquisition and analysis, interpretation of data, drafting the paper, approving the final version, accountable for the entire work. BS: delivering the research question, supporting, reviewing and revising the research process, performing data quality check, revising the manuscript for publication, accountable for both the work and the researcher.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.