Article Text

Abstract
Objectives The objectives of our study were (1) to investigate the association between gender of the general practitioner (GP) and the quality of primary care in Hungary with respect to process indicators for GP performance and (2) to assess the size of the gender impact.
Study design A nation-wide cross-sectional study was performed in 2016.
Setting and participants The study covered all general medical practices in Hungary (n=4575) responsible for the provision of primary healthcare (PHC) for adults. All GPs in their private practices are solo practitioners.
Main outcome measures Multilevel logistic regression models were used to analyse the association between GP gender and process indicators of PHC, and attributable proportion (AP) was calculated.
Results 48% of the GPs (n=2213) were women in the study. The crude rates of care provided by female GPs were significantly higher for seven out of eight evaluated indicators than those provided by male GPs. Adjusted for practice, physician and patient factors, GP gender was associated with the haemoglobin A1c (HbA1c) measurement: OR=1.18, 95% CI (1.14 to 1.23); serum creatinine measurement: OR=1.14, 95% CI (1.12 to 1.17); lipid measurement: OR=1.14, 95% CI (1.11 to 1.16); eye examination: OR=1.06, 95% CI (1.03 to 1.08); mammography screening: OR=1.05, 95% CI (1.03 to 1.08); management of patients with chronic obstructive pulmonary disease: OR=1.05, 95% CI (1.01 to 1.09) and the composite indicator: OR=1.08, 95% CI (1.07 to 1.1), which summarises the number of care events and size of target populations of each indicator. The AP at the specific indicators varied from 0.97% (95% CI 0.49% to 1.44%) of influenza immunisation to 8.04% (95% CI 7.4% to 8.67%) of eye examinations.
Conclusion Female GP gender was an independent predictor of receiving higher quality of care. The actual size of the gender effect on the quality of services seemed to be notable. Factors behind the gender effect should receive more attention in quality improvement particularly in countries where the primary care is organised around solo practices.
- PRIMARY CARE
- Process indicators
- General practitioner
- Quality of care
- Gender
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The nation-wide study on process indicators of primary healthcare (PHC) covered all general medical practices in Hungary responsible for the provision to adults, avoided selection bias.
Our investigation could estimate the population-level impact of the general practitioner (GP) gender effect.
Although the analyses were controlled for several factors (GP age; patient age, gender, relative education; and practice size, types of settlement and regional location) influencing the quality of PHC, by involving other potential confounding factors (such as onset/duration of a chronic diseases, preferences and conditions of patients), reliability of our estimations for risks and impacts could be further improved.
Introduction
The gender composition of physicians has changed in the last decades in all organisation for economic co-operation and development (OECD) countries. The proportion of female physicians has increased from 38% (in 2000) to 46% (in 2015), and this trend is expected to continue.1 The Central and Eastern European countries showed the highest share of female physicians in 2015. Extremes of this share were observed in Latvia (74.4%) and in Estonia (74.6%), but the strongest growing trend was in the Netherlands, where the proportion of female physicians increased from 35.3% to 52.6% from 2000 to 2015. However, changes in gender proportions are not homogeneous in the different medical specialties; some, such as family medicine, are more affected.1–4
According to the international literature, there is solid evidence that the physician’s gender influences the effectiveness of medical care in primary healthcare (PHC).5–9 Female physicians in primary care tend to deliver more preventive services,10–18 they have better adherence to guidelines of chronic diseases8 19 and they achieve better intermediate treatment outcomes (blood pressure, haemoglobin A1c (HbA1c) and cholesterol level), compared with their male colleagues.20 21
Several arguments could partially explain the existing differences between the quality of services provided by the two genders. Female physicians more often use patient-centred approach; moreover, they effectively facilitate patient participation in the medical exchange.8 22 23 According to studies in clinical practice, female physicians spend significantly more time with their patients and have longer consultations.6 24–26 Others have underlined the significance of the patient-centred communication style, which is more frequently applied by female physicians.8 27 28 Empathy is a further aspect of physicians’ behaviour associated with better patient compliance and outcomes in chronic disease care23 29–31 and a higher level of empathy is a well-known characteristic of women.32 33 Additionally, the level of empathy seems to have an impact on career choices; individuals with higher empathy tend to prefer the primary care specialty.30 33 34 Similar specialty preference was found among both medical students and physicians.30
The association between the gender of the provider (especially general practitioners (GPs)) and the effectiveness of the service is well demonstrated in many settings, but the exploration of how the gender of the physician actually affects the care practices and assessments of the size of the effect are insufficient.
Hungary provides an ideal field to examine the gender effect at the level of primary care in detail. The country has one of the highest shares of female physicians of general medicine and paediatrics, with a total share of 55.9% in 20151 and 56.2% in 2017.35 In Hungary, the gender of the GP can be used as a potential factor affecting general medical practice (GMP)-level performance indicators because each individual GP works in their own primary care district with a territorial supply obligation (municipalities are responsible for the provision of primary care for the local population within their territory). Since 2009, the performance of providers has been monitored for quality indicators by the National Institute of Health Insurance Fund Management (NIHIFM), which have contracts with all GPs in the country. This monitoring exclusively applies process indicators to assess the quality of chronic disease management in primary care. The evaluation of GMPs and the provision of financial incentives are based on reaching desired target values for these indicators.36
The objectives of our study were (1) to investigate the association between GP gender and the quality of primary care with respect to various process indicators for GMP performance and (2) to assess the size of the gender impact.
Methods
Setting
The healthcare system in Hungary is based on compulsory health insurance with universal coverage. Primary care services are provided by GPs working in solo practices; therefore, one GMP is owned and operated by one GP. In vacant GMPs, the services are provided by temporary GPs with restricted availability in time and place. The GPs are contracted with the NIHIFM, and they have territorial supply obligation, but patients can choose and change their primary care provider without any restriction.37
Study design
A nation-wide cross-sectional study was performed, which covered all GMPs in Hungary responsible for the adult primary care in 2016 (n=4852). Demographic data of 7 207 186 clients (above 18 years) and 4575 GPs, the GMPs’ organisational characteristics and data on performance indicators for GMPs were provided by NIHIFM. Vacant GMPs without a permanent GP during the study period (5.71%, n=277) were excluded, as this secondary analysis aimed to evaluate the influence of GPs’ gender on PHC indicators.
Patient and public involvement
Patients and the public were not involved in this study.
Patient-level, physician-level and organisational characteristics of GMPs
Patient-specific and GMP-specific data were provided by NIHIFM. The number of adults registered in each GMP was determined by gender and age groups of 18–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, 85–89, and 90 years and above in the database. The age group of 65–69 (and 60–64 where 65 years and above patients were not available) was used as a reference. The age of the GP was a continuous variable. The male gender of GPs and patients were used as a reference in the analyses.
GMPs were categorised by the practice size (number of insured people registered in each GMP as follows:<800, 801–1200, 1201–1600, 1601–2000 and >2000; the categories are defined by NIHIFM), and types of settlement (rural and urban). The regional location of each GMP was described by the county (Baranya, Bács-Kiskun, Békés, Borsod-Abaúj-Zemplén, Csongrád, Fejér, Győr-Moson-Sopron, Hajdú-Bihar, Heves, Komárom-Esztergom, Nógrád, Pest, Somogy, Szabolcs-Szatmár-Bereg, Jász-Nagykun-Szolnok, Tolna, Vas, Veszprém and Zala counties) and the capital city (Budapest). The practice size of 1201–1600, the rural settlement and Budapest were used as reference categories.
The relative education was used to indicate the educational attainment of adults registered in each GMP. This indicator was calculated using gender, age group (7–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, 85–89 and 90 years and above), and settlement-specific data from 2011 Hungarian Census data provided by the Hungarian Central Statistical Office. The summarised length of education was calculated for each settlement. The expected number of school years was determined for adults in each settlement by the demographic characteristics of the settlement and the national reference values. The ratio of observed and expected values, representing the settlement-specific relative education, was used to express the relative education of adults living in a certain settlement compared with the national reference level. A weighted settlement-specific relative education variable was calculated for GMPs providing care for patients from more than one settlement.38
Performance indicators for GMPs
Each routine indicator of NIHIFM on immunisation, cancer screening and chronic disease management were used to assess the performance of GMPs: (1) proportion of patients with influenza immunisation; (2) proportion of patients who participated in screening mammography; (3) proportion of patients with hypertension with serum creatinine measurements; (4) proportion of patients with diabetes and/or hypertension with lipid profile measurements; (5) proportion of beta-blocker use among patients with ischaemic heart disease; (6) proportion of patients with diabetes with HbA1c measurements; (7) proportion of patients with diabetes who attended eye examination and (8) proportion of patients with chronic obstructive pulmonary disease (COPD) who participated in pulmonary functional testing. A composite indicator (proportion of patients who received recommended care) was calculated by summarising the number of care events and the size of the target groups by each studied indicator. Indicators reflect the proportion of patients who received the care in each GMP. Details about the target groups and definitions of the assessed process indicators are shown in table 1.
Definition and the target group of the studied PHC indicators
Statistical analysis
Differences between baseline characteristics of GMPs were evaluated by the Pearson χ2 test for categorical variables and two-sample t-test for continuous variables.
We used multilevel logistic regression models because of the binary outcome variables and in order to account for the clustering effect of patients within physicians. The models were adjusted for characteristics of patients (age and gender), GPs (age) and GMPs (practice size, types of settlement, geographical location and relative education) to assess the effect of the gender of the GP on their performance in case of each indicator. ORs with the corresponding 95% CIs, and robust standard errors were estimated. We presented intraclass correlation coefficient, which shows the proportion of total variance explained by the physician as grouping factor. The Hosmer-Lemeshow test was used to determine the goodness of fit of the model (by comparing predicted and observed outcomes in deciles of predicted risk), which verified the adequacy of the model.
We calculated the missed care events, that is the number of care events not meeting the number of events which would be expected if the care was provided by female GP. The expected number of care events was calculated for GMPs with male GPs, using the demographic composition of adults belong to GMPs and considering female GPs as a reference, to describe the gender impact on service use in the whole country. Both observed and expected number of events were summarised for the whole country. The differences between the summarised observed and expected number of care events were calculated for GMPs with male GPs to quantify the differences in the number of care events compared with female GPs. Attributable proportion (AP) with 95% CI was also calculated by the summarised number of events to show the percentage of care events that can be attributed to the male GP gender.
Statistical significance was considered p<0.05. Statistical analyses were performed using STATA IC V.13.0 software.
Results
Descriptive statistics
The studied 4575 GPs (providing care for adults) consisted of 2213 (48.4%) women, and 2362 (51.6%) men (p<0.001). Female GPs were younger (55.3 years vs 57.8 years; p<0.001), more likely to work in urban regions (75.8% vs 62.0%; p<0.001) and had smaller sized GMPs (p<0.001). Patients of female physicians were more likely to be female (54.6% vs 52.31%; p<0.001). The mean relative education was higher in GMPs with female GPs (1.026 vs 0.989; p<0.001). The patient, physician and organisational characteristics of GMPs are summarised in table 2.
Patient-level, physician-level and organisational characteristics of GMPs
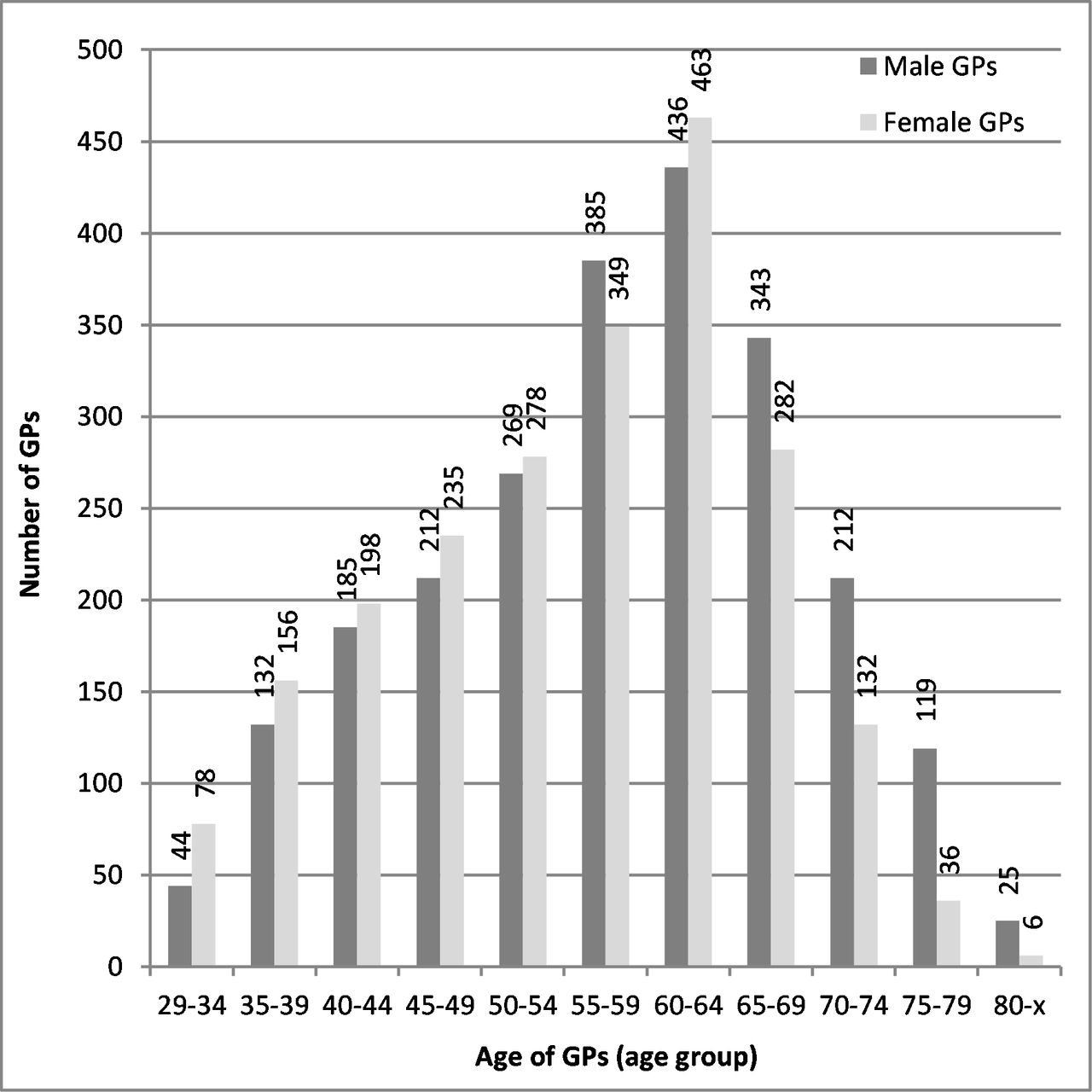
Female GPs were younger. In the group of female GPs under 55 years and male GPs above 65 years were over-represented ( figure 1 ).
{kind=link}
The age and gender distribution of Hungarian GPs responsible for the adult primary healthcare in 2016. GPs, general practitioners.
According to the crude values of the PHC indicators (aggregated by the gender of the GP), statistically significant differences were found between male and female physicians. Patients of female GPs were more likely to have had serum creatinine (70.9% vs 66.5%; p<0.001), lipid (64.5% vs 59.7%; p<0.001) and HbA1c (80.6% vs 76.8%; p<0.001) measurements; ophthalmological examinations (41.3% vs 38.2%; p<0.001); and mammography screening (46.7% vs 44.7%; p<0.001). They were also more likely to be managed properly in cases of COPD (79.1% vs 77.3%; p<0.001). Although there was statistically significant differences between genders related to vaccination against influenza (p=0.004), the size of difference was negligible (20.1% vs 19.9%). Patients with male GPs were more likely to receive beta-blockers (52.3% vs 53.5%; p<0.001) (table 3).
The number of patients received the care, the number of people in the target groups and the proportion of patients received the care in 2016 for the whole country by gender of GPs with 95% CIs
Multilevel analyses
According to the multilevel logistic regression analysis, patients of female GPs were significantly more likely to receive care according to guidelines. The female gender of GPs was associated with hypertension and diabetes care-related indicators (HbA1c measurement, serum creatinine measurement, lipid measurement and eye examination), mammography screening, management of COPD patients and the composite indicator. No association was observed between influenza immunisation, beta-blocker application and GP gender. The proportion of total variability attributable to physician after adjusting for characteristics of physician, patient and practice varied between 2.4% and 17.9% across the indicators (table 4). Gender had one of the strongest effects among all studied variables on hypertension and diabetes care indicators (HbA1c, serum creatinine and lipid measurement). Results of the regression models are presented in Supplementary Table 1-2.
Influence of female gender of GPs (OR, 95% CIs, robust standard errors) on the primary healthcare indicators according to multilevel logistic regression analysis controlled for age of GP, age and gender of the patients, relative education of patients, practice size, types of settlement and regional location of GMP in 2016 and the ICC of tested models
Population-level impact
Overall, 5.9% (95% CI 5.77% to 6.02%) of missed care events are attributable to male GP gender, which corresponds to 144 871 care events in the country per year. Restricting this summary to indicators with a significant association with GP gender (omitting influenza vaccination and beta-blocker application), the missed number of interventions was 144 373.
Compared with the GMPs with female GPs, the highest AP was observed for lipid measurement (AP=7.93%, 95% CI 7.71% to 8.16%), whereas the lowest AP was observed for influenza immunisation (AP=0.97%, 95% CI 0.49% to 1.44%). A notable percentage of missed care events was attributed to GPs’ male gender in the case of serum creatinine measurement (AP=6.4%, 95% CI 6.18% to 6.61%), eye examinations (AP=8.04%, 95% CI 7.4% to 8.67%) and HbA1c measurements (AP=5.09%, 95% CI 4.65% to 5.54%). Mammography screening was not performed for 4.36% (95% CI 4.00% to 4.71%) of women in the target group, whereas COPD management was missed for 2.33% (95% CI 1.61% to 3.04%) of patients if the GP was male. Only beta-blocker application showed more care events that were attributed to male gender of GPs (AP=2.42%, 95% CI 1.53% to 3.31%) (table 5).
Number of observed and expected care events in 2016, with absolute differences and attributable proportion estimations (with 95% CI) in Hungary among 3 762 869 patients provided by male GPs
Discussion
Main findings
Our results showed that GP gender was independently associated with quality of care with respect to process indicators for cancer screening and the management of chronic diseases (hypertension, diabetes and COPD). Patients of female GPs were more likely to have their HbA1c levels, serum creatinine, lipid measured, as well as their ophthalmological examination and pulmonary function testing implemented for monitoring purposes. Moreover, female patients of female GPs received significantly more mammography. Gender effect seems to have a clinical relevance mostly on hypertension and diabetes care-related indicators, considering both the higher effect of the GP's gender (HbA1c measurement: OR=1.18, 95% CI 1.14 to 1.23, serum creatinine: OR=1.14, 95% CI 1.12 to 1.17 and lipid measurement: OR=1.14, 95% CI 1.11 to 1.16) and size of the affected population compared with other indicators (mammography screening, eye examination and management of COPD) where we also found statistically significant differences. A lack of gender influence was observed only for influenza immunisation and for beta-blocker usage.
The size of this gender effect proved to be notable. A high proportion (ARtotal=5.9%) of missed care events could be attributed to this gender effect. More than 144 000 care events per year were missed (out of 2 600 827 expected events) due to gender effect among patients of male GPs in Hungary. Primarily, missed lipid (59 723 missed laboratory investigations) and serum creatinine measurements (52 130 missed laboratory investigations) were responsible for this impact. Missed examinations among patients with diabetes mellitus (9801 missed HbA1c measurements and 7686 missed eye examinations) and missed breast cancer screenings (13 285 screening tests) had a secondary, but significant, contribution.
Comparison with other studies
Others found similar gender differences in the management of diabetes8 20 21 39 40 and cancer8 41 screening. In addition, several studies have found an association between the management of hypertension and the gender of the physician. Female GPs tend to reach the blood pressure and lipid-level treatment goals more often42 43 and tend to focus better on cardiovascular risk factor control.15 39 42 43 Altogether, a positive association was observed between female gender and better quality of PHC in our investigation, in line with international experiences. Besides, our findings are consistent with other studies found that relatively low percentage of the variance is attributable to physicians on process measures after adjusting for characteristics of the physician, patient and practice.44 45
Strength and limitations
A strength of this study was that it covered the entire Hungarian population, avoiding selection bias in the analysis of the association between GP gender and PHC indicators and resulting in the representativeness of our results for the whole Hungarian PHC population. As a consequence, the main strength of our investigation was that it could estimate the population-level impact of the GP gender effect, which has rarely been investigated as reflected by a scarcity of relevant publications.
A limitation of the study is that we were not able to monitor the changes over time due to the cross-sectional design.
The relative educational level, which was used to indicate the educational attainment for GMPs, cannot be considered as a year-specific and GMP-specific indicator. The information on education was not available for the investigated year, and the relative educational level of the adults living in the settlement (settlement-specific) was considered, regardless of the number of GPs in one settlement.
Additionally, the fact that the range of variables in the NIHIFM database which could be included in the analysis is limited, careful interpretation is required. Although the analyses were controlled for GPs’ and patients’ age and gender, educational attainment, GMP practice size, types of settlement and regional location, there were confounding factors that were not included in our models, limiting the reliability of the presented risk measures. Selection of the GP may be affected by patients preferences and expectations, as patients have free choice of healthcare provider in Hungary. Since most of the GPs in Hungary are self-employed workers organising the provision on their own authority, the length of their working hours, the length of the consultation time and the availability of support staff were not measurable. The availability of support staff in solo practices or work in group practice could be an important factor in determining whether and how a patient will be treated.
Our analysis, which was based on data on solo GP practices, may differ from findings in group GP practices where professional cooperation with other providers may mitigate the effects of any non-clinical factors (eg, gender of GP).
Further research need
Our findings on impact of GP gender (mainly for HbA1c, serum creatinine and lipid measurement) suggest that further consideration of the effect is needed to identify the details and mechanisms behind the gender effect to improve the adequacy of targeted interventions. Patients with early stage diabetes mellitus are more cooperative with female GPs, but patients with advanced stages of the disease, realising the seriousness of the consequences, are more sensitive to male GP directions. The onset/duration of a chronic disease and accordingly the complex needs of patients may modify the gender effect.46 Therefore, it would be worthwhile to investigate the potential influences on performance indicators that are differentiated according to the preferences47–49 and type of their health problem.50
Furthermore, there is a possible extension of our presented investigation. Analysing outcome indicators on the prognosis of patients with chronic diseases in PHC is obviously required to more convincingly describe the public health impact of the GP gender effect.
Implications
Poor-quality healthcare services put a great burden on payers and society everywhere.51 The effective utilisation of experiences of high-income countries52 addressing gender differences in provision is crucial in low-income and middle-income countries such as Hungary. High-quality PHC is a shared goal of the patients, the GPs and the state.
According to our observations, a possible way to improve the quality of PHC is to raise awareness about the significance of the GPs’ gender effect and its underlying causes. Keeping in mind that large sample size can detect even the smallest differences, the interpretation needs to consider that these small differences may have limited importance at population level; our results indicate the significance and urge the expansion of interventions aiming at improved communication skills of medical students and GPs, and at shifting the attitude of GPs. Incorporating practical knowledge on how the communication strategies and empathy in clinical practice influence the quality of services (which is often overlooked by medical students and practitioners) may facilitate the development of a patient-centred care culture.
It is well demonstrated that a behaviour change targeting improved patient outcomes is feasible by training physicians and medical students.23 Since teaching patient-oriented communication skills to medical students increases their competency, as well as patients’ satisfaction and health outcomes. Training in effective communication skills, embedded into the medical school curriculum, is widely recommended.53–56 Our results suggest that the scope of this training should be supplemented by gender-related attitudes and behavioural features.
These findings can be utilised in gender impact assessment regarding the feminisation of the primary care physician workforce.57 58
Conclusions
Our results suggest the existence of a gender effect in Hungary on performance of GPs working in solo practices. Provision of guideline-recommended care was observed more often in patients of female GPs. The actual impact of the gender effect on the quality of services was found to be notable, emphasising that the communication style and attitude associated with female gender should be considered as factors influencing the quality of PHC and should be targeted accordingly in training of medical students and GPs. However, further studies involving a broader range of clinical and non-clinical factors are needed to allow more precise assessment of gender differences.
Supplemental material
Supplemental material
Acknowledgments
The authors thank the support of Zsófia Falusi and László Pál for providing the data for this study.
References
Footnotes
Contributors NK, LK and JS performed and designed the study. LK participated in the database preparation. NK, AP, VS and AN analysed and interpreted the data. NK and OV prepared the manuscript. RÁ and JS provided professional instruction on the subject and approved the final version to be submitted. JS revised the manuscript. All authors read and approved the final manuscript.
Funding The reported study was carried out in the framework of the 'Public Health Focused Model Programme for Organising Primary Care Services Backed by a Virtual Care Service Centre' (SH/8/1). The Model Programme is funded by the Swiss Government via the Swiss Contribution Programme (SH/8/1) in agreement with the Government of Hungary. Additional source of funding was from GINOP-2.3.2-15-2016-00005 project which was co-financed by the European Union and the European Regional Development Fund, and from EFOP-3.6.3-VEKOP-16-2017-00009 co-financed by EU and the European Social Fund. This work was also supported by the Portugal/Hungary Bilateral Project FCT/NKFIH - (TÉT_16-1-2016-0093) and the János Bolyai Scholarship of the Hungarian Academy of Sciences (MTA) to O.V.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The databases that we analysed were anonymised. The research protocol was reviewed and permitted by and performed in concordance with the Internal Data Safety and Patient Rights Board of the National Institute of Health Insurance Fund Management (E01/317-1/2014).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.