Article Text

Abstract
Introduction Androgen deficiency of the ageing male is a clinical syndrome resulting from the low production of androgens (testosterone levels <6.9 nmol/L) with symptoms including decline in lean mass, muscle strength, increases in body mass and overall fat mass. The aim of the study is to examine the effect of a 12 week strength training intervention on body composition, physical function, muscle cellular and molecular and selected biochemical markers of metabolic health in hypogonadal patients.
Methods and analysis The study is three-group controlled 12-week experiment to assess the effect of strength training on hypogonadal patients with testosterone replacement therapy and newly diagnosed males without testosterone replacement therapy. Age matched healthy eugonadal males are also engaged in strength training. Lean mass is used to determine sample size indicating, that 22 subjects per group will be sufficient to detect intervention related changes at the power of 0.90. All outcomes are collected before the intervention (pre-intervention assessments) and after the intervention (post-intervention assessments). Clinical outcomes are body composition (lean mass, fat mass and total body mass) measured by dual-energy X-ray absorptiometry, physical functioning assessed by physical tests and psychosocial functioning. The most important haematological and biochemical parameters included are glucose, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, testosterone, luteinizing hormone, follicle-stimulating hormone, sexhormone-binding globulin, insulin and prostate-specific antigen. Muscle cellular and molecular outcomes are muscle fibre size and regulators of muscle fibre size. Muscle cellular outcomes are measured from muscle biopsies obtained from musculus vastus lateralis.
Ethics and dissemination This trial is approved by Ethics Committee of the University Hospital in Bratislava, Slovakia, (ref. trial number: 127/2017) and all subjects will be fully informed on the rationale, risks and benefits of the study and sign the written informed consent prior to entering the study. Results will be published in peer-reviewed journals and presented in scientific conferences.
Trial registration number NCT03282682
- hypogonadism
- testosterone deficiency
- strength training
- testosterone
- physical activity
- aging male
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
To the best of our knowledge this trial represents the first study in hypogonadal males focusing on possible physiological and metabolic mechanisms of strength training at circulating, cellular and molecular level.
Wide spectrum of clinical outcomes with high-standard methods of assessments (dual-energy X-ray absorptiometry, muscle biopsies).
The major limitation of this trial is small sample size, caused by limited number of detected patients.
Another limitation is that the participants will be asked to not change their habitual dietary intake during the intervention, but the actual intake is not monitored.
Introduction
Testosterone is one of the most potent naturally secreted androgenic-anabolic hormone, and its biological effects include, among others, promotion of skeletal muscle growth.1 Testosterone stimulates protein synthesis, inhibits protein degradation and these effects account for the promotion of muscle hypertrophy by testosterone.2 Ageing beyond 35 to 40 years is associated with a decline of 1% to 3% per year in circulating testosterone concentration (1.6% in total and 2% to 3% in bioavailable testosterone) in men. This reduction can eventually lead to very low resting concentrations of circulating testosterone, a condition that has been termed andropause.3–6 Although the lower limit of normal total testosterone is not clearly defined, American Association of Clinical Endocrinologists suggests 6.9 nmol/L as lower limit of normal testosterone levels, other societies suggest 8 nmol/L and even up to 10 nmol/L7 as a limit below which patients can be considered as hypogonadal. The Endocrine Society defines male hypogonadism as a clinical syndrome resulting from failure of the testis to produce physiological levels of testosterone (androgen deficiency) and normal number of spermatozoa. Hypogonadism (primary, secondary or mixed) is caused by disruption of one or more levels of the hypothalamic–pituitary–gonadal axis.8 All the causes of male hypogonadism can be found in table 1.9–11 Due to complexity of the diagnosis of hypogonadism, there are several alternative names for male hypogonadism, but for a purpose of this trial, the term ADAM was chosen.
Causes of male hypogonadism
Symptoms of hypogonadism
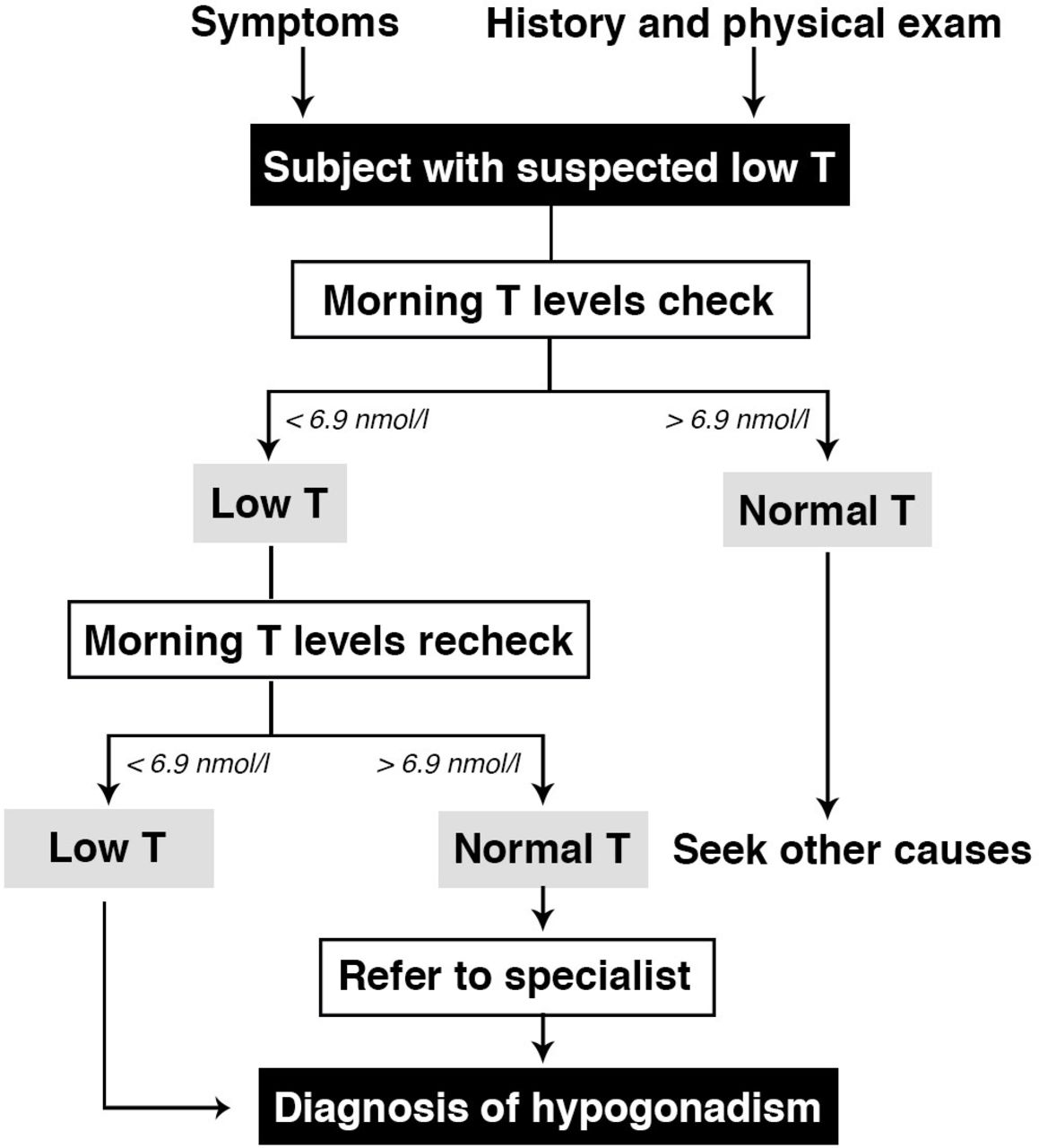
Total testosterone is a reliable marker for the initial screening of men presenting symptoms of hypogonadism,12–14 (figure 1), but for better understanding of the ADAM syndrome it is sometimes required to analyse also free or bioavailable testosterone.15 Most testosterone circulates tightly bound to sex hormone-binding globulin (SHBG) or weakly bound to albumin. A minor amount circulates as free testosterone, and it is believed that this is the metabolically active fraction. Therefore, measurements of free testosterone is important in the diagnosis of disorders of androgen deficiency in men.16

Symptoms of male hypogonadism include decline in lean mass (LM), muscle strength, adiposity, libido and erectile dysfunction, depressed mood, decreased energy or vitality, increased fatigue, osteoporosis or low bone mass, increases in body mass and overall fat mass.8 17 Studies of hypogonadal men shows, that there are increases in body mass and overall body fat mass as well as decreases in LM with declining androgen levels.17 Androgens also have a direct impact on bone mineral density since testosterone and oestrogens both play a vital role in bone health and low testosterone levels can cause an increase in osteoclast induced bone resorption.18 Other sources also state direct correlation between low testosterone levels and increased risk of aortic atherosclerosis independent of age, increased body mass index (BMI), total cholesterol or diabetes.19
These symptoms may affect men earlier in life, already in their late third decade of life.20 If untreated, chronic lower than normal testosterone level dramatically increases risk of many diseases later in life. Studies have suggested a link between hypogonadism and cardiovascular disease, which is not surprising given the relationship with hypogonadism and the metabolic syndrome.10 21 Testosterone is a hormone regulating several pathways affecting many other syndromes, for example locomotive syndrome.22 There is a likely causal relationship between low androgen levels and ageing, as well as its association with increased risk and the occurrence of cardiovascular events and progression of cardiovascular diseases.23 On a metabolic level, men with lower androgen levels have demonstrated higher glucose and insulin levels, higher rates of obesity and increased incidence of type 2 diabetes and other diseases.24–28
Testosterone replacement therapy
For decades hypogonadism, has been treated by testosterone replacement therapy (TRT) lifelong, as this helps to prevent some of the adverse health effects.29–31 Restoration of testosterone levels to the normal range improves libido, sexual function and mood, reduces fat body mass, increases lean body mass and improves bone mineral density.3
Among the published trials on the role of testosterone in older men, not all report increased muscle strength with testosterone replacement therapy. The studies reporting significant strength gains were performed in hypogonadal subjects and employed a higher dose of testosterone for a longer duration.32 Nair et al 33 described in their report treatment of a group of hypogonadal men with a transdermal testosterone at a dose of 35 mg/week for 24 months and found no increase in strength. However, 35 mg/week is less than a replacement dose and resulted in only a 30% increase in the circulating testosterone concentration. Some other studies34–37 also report small or no increases in muscle strength with TRT. Maintenance of the musculoskeletal system by increased bone density will contribute to increased physical fitness, reflected by increased strength and endurance,38 and the treatment outcome is strongly influenced by age and training.38 Lašaitė et al 39 observed that 2 year testosterone replacement therapy in young and middle-aged hypogonadal men had beneficial effect on cognitive functioning (improved attention and visual scanning ability, executive function and psychomotor speed), but not on emotional state and quality of life. Hildreth et al 40 found that TRT improved body composition, but it had no effect on functional performance. Testosterone replacement can improve lipid and insulin metabolism, resulting in changes of body composition, such as decreasing fat depots and growth of muscle fibres can also be observed.39 Permpongkosol et al 41 in their work from 2016 found that 8 year treatment of long-acting testosterone undecanoate did not improve all obesity parameters.
It is still not clear how testosterone effects cognitive function in adult men, but testosterone may exert its action through androgen receptors in the brain and has been shown effect on serotonin, dopamine, acetylcholine and calcium signalling.42 Barrett-Connor et al 43 found correlation between higher bioavailable testosterone and better scores on 2 of 12 cognitive function tests. Higher total or bioavailable testosterone levels tended to be associated with better performance on tests with verbal memory and mental control. Testosterone enhanced cerebral perfusion in hypogonadal men and that perfusion takes place specifically in Brodmann areas 8 and 24, regions of the brain that are concerned with: strategic planning, higher motor action, cognitive behaviours, emotional behaviour, generalised emotional reaction, wakefulness and memory.44 Hypogonadal men have lower scores in tests of memory, visuospatial function, with a faster decline in visual memory.27 McIntyre et al 45 found, that middle-aged males with depressions did have a reduction in bioavailable testosterone.
Risks associated with testosterone replacement therapy
Testosterone treatment is contraindicated in subjects with breast cancer or benign prostate hyperplasia, lower urinary tract symptoms and if risks of treatment is perceived to be high by many physicians.3 The risk of prostate cancer with TRT is still unclear. Only intramuscular treatment found slight increase in prostate-specific antigen (PSA) levels.46 Loeb et al 47 found that TRT remained significantly associated with more favourable-risk prostate cancer and lower risk of aggressive prostate cancer. But other studies and meta-analysis found TRT as a safe urological approach to treat hypogonadism.48–50 Other risks of TRT in men include fluid retention, mood fluctuations, gynaecomastia, worsening of sleep apnoea, polycythaemia, elevation of PSA.3 5 50 Bhasin et al 51 found higher incidence of adverse effects (included haematocrit greater than 54%, leg oedema with shortness of breath, urinary retention and prostate cancer) in treating older men with the very high doses of total testosterone (T) compared with young males. Rhoden and Morgentaler52 have reviewed the adverse effects and recommend the long-term monitoring of the above-mentioned parameters. Potential adverse events not related to hormones include pain at injection site and local skin irritation.
The effects of strength training
Much research has been conducted on the effect of strength protocols on muscle mass and muscle strength which incorporate large muscle groups at intensities around 70% to 80% of 1RM (one repetition maximum), volumes from two to three sets of 10 to 12 repetition and rest periods of short to medium duration (60 to 90 s).53 54 Beneficial effects of exercise, especially resistance training have been clearly shown with regards to the quality of life, fatigue, muscle strength, muscular endurance and functions and body composition in elderly men with prostate cancer receiving androgen-deprivation therapy, thus being in a chronically low testosterone condition.55 56 Clearly, resting levels of testosterone and other androgens but not their acute elevations due to exercise have also impact on muscle hypertrophy as suggested by a recent review article.57 As for exercise interventions with ADAM patients, the scientific evidence is very limited but promising. Schwarz and Willix23 found positive outcomes on coronary risk factors such as glucose intolerance and hyperlipidaemia when TRT was combined with endurance exercise. To our knowledge, only Hildreth et al 40 have used resistance training and found benefits of both resistance exercise with TRT as well as without TRT in hypogonadal males. After intervention, there were no significant differences between combination of resistance exercises with TRT or with placebo in improvements in muscle function or strength in the two exercise groups. However, adding TRT resulted in greater improvements in decrease of fat mass and increase of fat-free mass. In the TRT but no exercise condition, patients did not improve muscle function but decreased fat mass, increased fat-free mass and upper body strength. Importantly, TRT plus progressive resistance training produced greater improvements in body composition than either intervention alone.
Glintborg et al 58 studied effects of TRT and/or strength training (ST) on cardiovascular risk in hypogonadal males for 6 months. This double-blinded, placebo-controlled study found that only ST +placebo significantly decreased soluble cluster of differentiation 36 (sCD36) levels. Only placebo group did not decrease fat mass during this period. Compared with TRT, 6 months of strength training reduced sCD36 levels suggesting decreased cardiovascular risk, possibly due to a reduction in central fat mass.
In a pilot randomised controlled trial by Cho and colleagues59 when hypogonadal males were treated with combination of exercise and TRT, significantly better results in serum testosterone levels and symptoms of hypogonadism compared with TRT alone after 12 weeks of intervention were found. The levels of testosterone were significantly higher in the combination group (p=0.01) In addition, these improvements were well-maintained in the combination group with continuous exercise even after cessation of TRT. After 20 weeks of intervention the group which used TRT and strength training kept the testosterone levels significantly higher (p=0.01) compared with the group with TRT only. Consequently, it seems that exercise can augment the durability of response to TRT and it may be the solution to shorten the treatment duration with a lower risk from testosterone therapy.59 There are some very promising results showing a great potential of exercise in hypogonadal patients. However, the above-mentioned studies did not focus on possible physiological and metabolic mechanisms responsible for the positive effects of resistance training at circulating, cellular and molecular level. Up to date, there are no studies investigating the effects of strength training on the regulation of muscle mass and neuromuscular function at a cellular level in hypogonadal male patients.
Aims
The overall aim of the trial is to examine the effect of a 12-week strength training programme with and without TRT on body composition, physical function, selected biochemical markers of metabolic health, histological and molecular parameters and the quality of life of patients with ADAM.
Study design
The study is a clinical trial with three arms comparing the effect of strength training with testosterone replacement therapy (ST +TRT), strength training alone (ST) on hypogonadal males and on a control group of healthy eugonadal males (HM), also engaged in strength training for 12 weeks (figure 2).

{kind=link}
{kind=link}
Timeline of the ADAM study.
Trial status
At the time of the first submission of the protocol, the trial was in the phase of participant recruitment. The recruitment began in February 2017 and the last part of data collection is expected to end in August 2019.
Participants
Subjects will be included from urological units at Department of Urology, University Hospital-Petrzalka, Bratislava, Slovakia; Department of Urology, Faculty of Medicine, Comenius University, Bratislava, Slovakia and 5th Department of Internal Medicine, Faculty of Medicine, Comenius University, Bratislava, Slovakia. The study will involve in total 66 male participants divided into three groups (n=66): group 1, males with hypogonadism who are undergoing TRT (n=22); group 2, newly diagnosed males with hypogonadism without testosterone replacement therapy (NON-TRT) (n=22); group 3, healthy eugonadal men (HM) (n=22). The participants from all groups engaged in strength training. The volunteers are screened for testosterone levels before the start of the participation by the specialist.
The most important inclusion criteria for participation in the study from the patient population are age 40 to 60 years old, subjects with hypogonadism on TRT or newly diagnosed patients of hypogonadism. The hypogonadal patients fulfilling the criteria for study participation will be verified for low testosterone before entering the study. The same verification will take place at the end of the study. The most important exclusion criteria include regular strength training, conditions that are medical contraindications and prostate cancer or abnormal serum PSA levels without adverse histological examination. All inclusion and exclusion criteria are listed in online supplementary additional file 1. In addition to written information, eligible subjects will be verbally informed about the study by their responsible urologist and the study officials before participation. TRT provided to patients is intramuscular injection of testosterone undecanoate (TU) at a dose of 1000 mg repeated every 12 weeks. Testosterone undecanoate (Nebido) is the only injectable form of testosterone used at the institutes of collaborating physicians of the study. According to our knowledge, this form of T at dose of 1000 mg is the most stable of all available preparations for 3 months’ period, which is considered a standard treatment in Slovakia. Shorter-acting forms may cause more pronounced fluctuations in 24 hours circulating levels of testosterone. The participants will be asked to not change their habitual dietary intake and physical activity patterns. Participants will be asked to continue in physical activities as before, but any kind of regular physical activity, especially strength training or any other kind of weight training during the intervention will be also prohibited. The exclusion criteria reject any participant, who performed any kind of regular strength training 1 year prior to study.
Supplemental material
Strength training intervention
The strength training protocol will be a modified strength exercise programme from Segal et al 60 which was used in similar group of patients. The participants will perform 24 training sessions of strength training protocol with the frequency of two training sessions per week for 12 weeks. There will be at least 48 hours rest period between two subsequent training sessions (Monday and Thursday). The intervention will take place at the Faculty of Physical Education and Sport, Comenius University in Bratislava, Slovakia. All training sessions will be supervised and guided by professionals with university degree in sports training to ensure safety, correct technique and progression in training load, with a maximum of three participants per one trainer. The participants will be familiarised with the equipment and exercise technique 1 week before the start of the intervention. The technique corrections will be possible during the whole intervention if needed. Ten repetition maximum (RM) and 12RM diagnostic test for all exercises will be conducted during the first week of training intervention. Each training session will include a 5 min dynamic warm-up, consist of 10 exercises for approximately 30 s of each, and exercises will be focused on main muscle groups (table 2).
Dynamic warm-up
The strength protocol exercises will be performed with free weights and on machines. The training programme consist of six exercises for upper and lower body at an intensity of 60% to 80% (8 to 12RM: the load that induces technique failure in eight or twelve repetitions) of one-repetition maximum and takes approximately 60 min. The inability to perform full repetition will be assessed by a supervisor or by participants’ feedback. The participants will be instructed to perform a concentric action for 2 s and immediately after an eccentric action also for 2 s. There will be 90 s rest period after each set. The same duration rest period will be between all of the exercises. The rest periods will be controlled by timer (The miniMAX, Gymboss, USA). The load will be added, if participant can complete prescribed number of repetition in each set of the exercise. More detailed strength training protocol can be seen in table 3. During the first 3 weeks of the intervention, there will be one set in the beginning with light weight to focus on safety and technique. After that three more sets with weight close to 60% to 80% of 1RM will follow. After first 3 weeks, the number of sets will be increased to four.
Strength training protocol
The exercises performed during every session will be: leg press, split squat, bench press. The exercises alternating through the week are knee extension with leg curl, seated row with seated pull down and incline dumbbell bench press (training equipment provided by KOHI Leopoldov, Slovakia, and Technogym, Italy). Since unilateral exercises (eg, one leg squats) develop similar magnitude of muscle activity with producing less load on the spine, thus they are safer,61 the split squats are chosen instead of regular squats. Prescribed exercises in the strength training protocol for every training sessions can be found in table 4. Each session will be supervised by at least two professionals, who received strength training programme and record every repetition and set made in each session in an individual training plan. At the start of each session, the trainers will ask participants if they experienced any adverse events since the last session and record reported events. All adverse events during the training session will be written down into paper spread sheet and processed afterwards. Each training session will be monitored with an attendance list, with minimum 85% attendance during the study. Each session will be marked as successfully completed when at least 80% from the total volume and intensity of the training protocol planned for the particular training session is performed. If a participant will be unable to perform any of the exercises or sets, this will be recorded into a prepared training plan and the situation will be managed during the first week during familiarisation with the training protocol. The appropriate alternative exercise will be considered depending on the restriction or participant’s limitation.
Training sessions, type of exercises and type of resistance
Clinical outcomes
Clinical outcomes will be collected 1 week before the intervention (pre-intervention assessments) and 1 week after the intervention (post-training assessments). All outcomes, specific variables and assessments in each testing are listed in online supplementary additional file 2. All participants will be tested at the same time of the day, and asked to avoid caffeinated and alcohol beverages before the assessments.
Supplemental material
Familiarisation
To secure validity of the physical tests, all subjects undergo a session of familiarisation 7 days prior to the intervention assessments. All sessions are performed based on the same guidelines, but after the familiarisation session the load of each resistance exercise will be adjusted to match the expected maximum.
Primary outcome measure lean mass
The primary outcome of the study will be the change in LM measured by dual-energy X-ray absorptiometry (Hologic fan-beam bone densitometer Discovery QDR series). The changes in lower and upper body LM are analysed separately because of differences in androgen sensitivity in leg muscles compared with neck, chest and shoulder muscles.62 Due to very similar results but greater participant comfort62 we decided to use The National Health and Nutrition Examination Survey (NHANES) protocol, which required the participant to be positioned in a supine position in the middle of the densitometry table with head straight, space between the arms and torso, palms flat on the table and feet together secured by a strap. The systematic review of Shiel et al 63 showed a strong level of agreement as illustrated by high intraclass correlation coefficients (ICC's) and concordance correlation coefficients (CCC's) between the Nana and NHANES positioning protocols, however systematic bias within limit of agreement plot and a large difference in 95% confidence limits indicates that the protocols should not be interchanged when assessing an individual.
Secondary outcome measures
Body composition
Other body composition parameters (fat mass, total body mass) will be measured at the same time so also the protocol is the same as with the primary outcome. The height will be measured by stadiometer and waist circumference will be measured by stretch‐resistant tape that provides a constant 100 g tension. The body mass index is afterwards calculated and reported.
Muscle strength
Muscle strength of lower extremities will be measured as force production during maximal voluntary contraction (MVC) isometric knee extension and isometric knee flexion knee dynamometer (ARS dynamometry, S2P Ltd, Ljubljana, Slovenia). Each of the test will be performed six times with three practise trials and three recorded trials. For the first practise trial, participants will be instructed to achieve approximately 50% of the maximum, with 20 s rest period. The second and third practise trial will be performed at 80% of the maximum with 20 s rest periods. The last three trials will be performed with maximal voluntary effort and will be recorded. The best out of three will be taken for further analyses. Rest period during recorded trials will be 60 s. During the MVC, the participants will be asked to push/pull as strong as possible and hold for 5 s. Intrasession repeatability for MVC is the 5.7 coefficient of variation (CV) % and 0.98 ICC. Additionally, with awareness of health issues (such as higher blood pressure) and because of a safety reasons, dynamic leg press 1RM (one repetition maximum) will be predicted from multiple repetition maximum testing.64
For assessing the muscle strength of the upper extremities, the isometric MVC handgrip strength will be measured by Camry Digital Hand Dynamometer. The participant will stand upright and hold the dynamometer in the hand next to the body, with the minimal or none flexion in the elbow joint. The base of the handle will be on the first metacarpal, while the handle should rest on the middle of the four ringers. None of the body parts will be allowed to move. The test will be performed with three practise trials. First on 50% and the others on 80% of their perceived maximum with 20 s’ rest period. After that, three maximum trials with rest period of 60 s will be recorded and the best out of three will be taken for further analyses. The participants will be encouraged to give their maximum effort. The participant will squeeze the dynamometer for 5 s. After the test with dominant hand, the test will be performed for non-dominant hand.
Cardiorespiratory fitness
Cardiorespiratory fitness will be measured by the single stage treadmill walking test,65 where the participants will be asked to walk on Pro Treadmill (Woodway, USA). During the walking test, participants will wear same shoes they will use during the whole intervention. The speed during the test can be changed if needed. The procedure will be performed once and heartbeat will be tracked by heart rate monitor attached on the chest. VO2max (the maximum rate of oxygen consumption) will be calculated according the literature.65
A 10 m preferred walk-speed and 10 m maximum walk-speed will be measured by timing gates WITTY GATE (MicroGate, Italy). Participants will walk 10 metres and the time will be measured for the intermediate 6 metres. This allow acceleration and deceleration. The gates will be placed on 2-metre mark and 8-metre mark. The timing starts when participant cross the first mark and stop when the 8-metre mark is crossed. There will be three trials for preferred and three trials for maximum walk-speed. The outcome measure will be velocity in metres per second calculated as mean of the three trials or the best trial from the preferred and maximum walk-speed test, respectively. Participants will be asked to perform at preferred walking speed first followed and then at the fastest walking speed possible.
Psychosocial functioning
The general health status will be measured by The Short Form (36) Health Survey patient-reported survey of patient health (SF-36). In addition, clinically investigating the health-related quality of life symptoms of ageing men are measured by Ageing Males' Symptom (AMS) Scale. The AMS scale had internal consistency (α = 0.89 (95% CI 0.88 to 0.90)); the mean alpha estimates across the AMS subscales ranged from 0.79 to 0.82. The AMS scale also had good test-retest reliability (r = 0.85 (95% CI 0.82 to 0.88)); the test-retest reliability coefficients of the AMS subscales ranged from 0.76 to 0.83.66 AMS is a standardised scale according to psychometric norms. Most of the currently available language versions were translated following international standards for linguistic and cultural translation of quality of life scales.67
Serological outcomes
Fasting morning venous blood will be taken after overnight (10 hours) fasting and 15 min rest from cubital vein from 8:00 am to 10:00 am68 into closed system collection tubes containing beads coated with a clotting activator and polyacryl ester-gel (Sarstedt AG & Co, Germany). The blood will be centrifuged (3000 g, 4°C, 10 min) immediately after sampling to obtain EDTA plasma or they will be centrifuged (3000 g, 4°C, 20 min) after 30 min at room temperature (RT), to obtain serum. The haematological and biochemical parameters analysed immediately will be haemoglobin, haematocrit, leucocytes, thrombocytes, glucose, urea, sodium, potassium, calcium, alanineaminotransferase, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglyceride, testosterone, oestrogen, luteinizing hormone, follicle-stimulating hormone, SHBG, albumin, bilirubin, total protein, c-reactive protein, insulin and PSA. Plasma and serum aliquots (500 ul) will be stored at −20°C (analysis within 6 months) and at −80°C for the long-term storage. Bioactive molecules (myokines, exerkines, released from skeletal muscle and/or other tissues) which could be associated with the adaptive response to exercise in all patients will be quantified.
Muscle cellular outcomes
Muscle biopsies will be obtained from approximately 80% of the subjects included in the study. Subjects not willing to undergo biopsy are still eligible for trial participation. With the subject in a supine position, a 5 mm muscle biopsy cannula (Bergstrom-Stille, Sweden) with manual suction is used to obtain muscle samples (200 mg), under local anaesthesia (lidocaine 2%). Before the intervention, the biopsy will be obtained from the mid-section of the right musculus vastus lateralis, and after the intervention the biopsy will be obtained 3 cm proximal to the pre-intervention biopsy.
Muscle fibre size and regulators of muscle fibre size
Muscle fibre size, measured as muscle fibre cross-sectional area, represents the primary muscle cellular outcome. Secondary muscle cellular outcomes reflecting regulators of muscle fibre size are (a) number of myonuclei per muscle fibre, (b) number of satellite cells per muscle fibre, (c) number of satellite cells and myonuclei positive for androgen receptors and (d) proteins involved in muscle protein degradation (muscle breakdown). The number of satellite cells will be quantified on frozen muscle cross sections with a immunohistochemical protocol as described in Bjørnsen et al.69 (Pax7 +Laminin + DAPI).
Muscle fibre cross-sectional area and regulators of muscle fibre size are analysed by immunohistochemistry on cross sections of muscle biopsies and by western blots and ELISA in muscle homogenate.
Muscle fibre cross-sectional area is measured by cutting transverse serial sections of the muscle biopsy (8 µm thick) with a cryostat microtome (Microm, Germany) at −22°C and mounted on glass slides. Serial sections are immunohistochemically stained for fibre types (type I and type II) (used to measure muscle fibre cross-sectional area), number of satellite cells, number of myonuclei and number of satellite cells and myonuclei positive for androgen receptors. Muscle fibre cross-sectional area is measured for the different fibre types separately.
Statistical analysis
Normality of the data distribution will be assessed by comparing histogram of the sample data to a normal probability curve and outliers will be identified as values distant for more than 3 σ from the average. Normality will be further tested with Kolmogorov-Smirnov test if needed.
Differences between normally distributed variables will be evaluated by the analysis of variance with repeated measures and Bonferroni post-hoc test, differences between pre-training and post-training values of the specific subpopulation will be evaluated with a paired Student’s t-test. Non-normally distributed variables will be log transformed. Variables that could not be log transformed to normal distribution will be tested with non-parametric tests (Mann-Whitney test and Wilcoxon rank test).
Cohen’s d will be used to calculate effect size, represented by ‘d’ and interpreted as <0.2 is a small, 0.2 to 0.8 is a moderate and >0.8 is a large effect size.
For studying the relationships between the various outcomes, the Pearson or Spearman correlation tests will be used.
All statistics were performed using a statistical software Statistical Package for the Social Sciences (SPSS) 21.0 (IBM Inc, Armonk, New York, USA) and p values<0.05 will be considered significant. Data will be presented as means and SD. Missing endpoint data will disqualify patient from the endpoint analysis. Missing single value, of training progression records will be replaced by the last observed value.
Background variables
Information about medical situation as time points for treatment and stage of symptoms are collected from the medical record. Past illnesses and other medical problems are also reported in the questionnaire.
Patients and public involvement
Patients (study participants) will be informed about the individual results of the baseline examination as well as on the primary and secondary outcomes of the study, in a form of individual consultation with a research team member.
Patients or public (patient organisations) were not involved in the development of the research question or study design. However, they will be asked to help with recruitment, and will also be involved in the conduct of the study with the power to shape (individualise) the training intervention according to individual preferences, prior experiences and medical conditions. Moreover, they will be involved in individualising the follow-up intervention protocol, shaping thus the long-term exercise programme to increase its sustainability.
Sample size
The pre-existing data from our previous 12 week exercise intervention study related to fat (5.6% decrease p=0.002) & lean body mass (1.8% increase, p=0.047, dual-energy X-ray absorptiometry) and that of maximal voluntary contraction force measured on linear leg-press (31% increase, p<0.0001, 1RM). Lean body mass was used to determine sample size for the population of the designed intervention study. The Type I error probability was set at 0.05 and the power to 0.90 and 0.95. Results indicate that 22 patients per group will be sufficient to detect exercise intervention related change of 1,06±1,56 kg (average ±SD) of lean body mass at the power of 0.90, accounting for the 10% patients drop-out.
Ethics and dissemination
All the participants will be fully informed on the study protocol risks and benefits and will provide the written informed consent prior to entering the study. Participation in the trial is fully voluntary. Inability to comply with the study protocol will not affect the healthcare. Data will be stored and handled anonymously using the coding system complying with the General Data Protection Regulation 2016/679. All unexpected, serious adverse events will be reported to the study sponsor as well as to the relevant health insurance company within 7 days. The findings of this trial will be published in peer-review journals, scientific conferences with main audience of healthcare professionals, healthcare providers, but also patients and their families.
References
Footnotes
Contributors MK, JC, TR, MS participated in the study design and drafted the manuscript, GB participated in the development of the intervention protocol, TR, BU and JU designed protocol for biological sample collection and processing, and will participate in biological material sampling & analyses. MP, ZK, JP, BK and PB provide access to patients. MS, JC, JU and MK performed data analysis. All authors contributed to and approved the present manuscript.
Funding The study is funded by the Scientific Grant Agency of the Ministry of Education, Science, Research and Sport of the Slovak Republic and of the Slovak Academy of Sciences (VEGA) no. 1/0714/16.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This trial was approved by Ethics Committee of the University Hospital in Bratislava, Slovakia (ref. trial number: 127/2017).
Provenance and peer review Not commissioned; externally peer reviewed.