Article Text

Abstract
Objective Cardiovascular disease (CVD) is one of the leading non-AIDS-defining causes of death among HIV-positive (HIV+) individuals. However, the evidence surrounding specific components of CVD risk remains inconclusive. We conducted a systematic review and meta-analysis to synthesise the available evidence and establish the risk of myocardial infarction (MI) among HIV+ compared with uninfected individuals. We also examined MI risk within subgroups of HIV+ individuals according to exposure to combination antiretroviral therapy (ART), ART class/regimen, CD4 cell count and plasma viral load (pVL) levels.
Design Systematic review and meta-analysis.
Data sources We searched MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews until 18 July 2018. Furthermore, we scanned recent HIV conference abstracts (CROI, IAS/AIDS) and bibliographies of relevant articles.
Eligibility criteria Original studies published after December 1999 and reporting comparative data relating to the rate of MI among HIV+ individuals were included.
Data extraction and synthesis Two reviewers working in duplicate, independently extracted data. Data were pooled using random-effects meta-analysis and reported as relative risk (RR) with 95% CI.
Results Thirty-two of the 8130 identified records were included in the review. The pooled RR suggests that HIV+ individuals have a greater risk of MI compared with uninfected individuals (RR: 1.73; 95% CI 1.44 to 2.08). Depending on risk stratification, there was moderate variation according to ART uptake (RR, ART-treated=1.80; 95% CI 1.17 to 2.77; ART-untreated HIV+ individuals: 1.25; 95% CI 0.93 to 1.67, both relative to uninfected individuals). We found low CD4 count, high pVL and certain ART characteristics including cumulative ART exposure, any/cumulative use of protease inhibitors as a class, and exposure to specific ART drugs (eg, abacavir) to be importantly associated with a greater MI risk.
Conclusions Our results indicate that HIV infection, low CD4, high pVL, cumulative ART use in general including certain exposure to specific ART class/regimen are associated with increased risk of MI. The association with cumulative ART may be an index of the duration of HIV infection with its attendant inflammation, and not entirely the effect of cumulative exposure to ART per se.
PROSPERO registration number CRD42014012977.
- Myocardial infarction
- Cardiovascular disease
- HIV
- Combination antiretroviral therapy (ART)
- Relative risk
- Systematic review
- Meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Myocardial infarction
- Cardiovascular disease
- HIV
- Combination antiretroviral therapy (ART)
- Relative risk
- Systematic review
- Meta-analysis
Strengths and limitations of this study
We used explicit eligibility criteria and a comprehensive search strategy for this systematic review and meta-analysis.
Adjudication of studies for eligibility and the data extraction were performed by two independent reviewers working in duplicate.
This systematic review and meta-analysis analysed several additional drug exposure comparisons and clinical measures (eg, CD4 cell count, plasma viral load) that had not been previously examined in relation to myocardial infarction risk among HIV-positive individuals.
Some of the meta-analyses were based on a small number of studies which is a limitation.
Variability in the quality of the included studies may have influenced the results and thus the conclusions drawn.
Introduction
Cardiovascular disease (CVD) is one of the leading non-AIDS causes of death and disability among people living with HIV in the combination antiretroviral therapy (ART) era.1 2 Although HIV-positive (HIV+) individuals are believed to be at higher risk of CVD compared with uninfected individuals,3 4 the results and conclusions from the studies that have examined the nature of the risk of CVD, in particular myocardial infarction (MI) among HIV+ individuals have been conflicting. While some cohort studies have suggested a positive association between ART including specific drug (eg, abacavir) or drug class (eg, protease inhibitors (PIs)) use and MI, or CVD risk,5–9 others have not.10–12 Furthermore, there has been a lack of agreement between observational studies,8 11 13 and randomised controlled trials (RCTs).14 15 Clearly, the evidence regarding the nature of, and extent of the risk of MI and other CVD events among HIV+ individuals is far from uniform.
Five meta-analyses have been conducted in an attempt to synthesise the data on CVD risk among HIV+ individuals.16–20 These have either been limited in scope by assessing only the association between ART use and risk of CVD16; included trials that lacked MI event adjudication17; included trials where CVD events were not among the pre-specified outcomes of interest18; provided incomplete results on MI risk19; or amalgamated all CVD events (eg, MI, stroke) as a single outcome.20 In addition, this latter meta-analysis was fraught with a number of methodological ambiguities.21
Given these limitations, coupled with the publication of several new and updated study reports on the topic, we sought to undertake an updated systematic review and meta-analysis of studies assessing the risk of CVD among persons living with HIV. Considering the scope, diversity and differences in the definition,22–25 aetiology and clinical picture of different CVD events,26 coupled with the strong body of literature related to HIV and MI and the ongoing debate around potential MI risk associated with use of specific ART medications such as abacavir, we have elected to focus primarily on MI as the outcome of interest for this meta-analysis, as it is the most widely researched CVD outcome among HIV+ individuals. The objective of our study was to estimate the risk of MI among HIV+ individuals relative to uninfected individuals. Additionally, we examined MI risk within subgroups of HIV+ individuals according to exposure to ART, ART class, specific ART regimen, CD4 cell count and plasma viral load (pVL) levels.
Methods
Search strategy and selection criteria
The systematic review and meta-analysis was performed in accordance with the PRISMA statement.27 A protocol describing the inclusion criteria and analysis methods for this systematic review was specified in advance, registered and published at the international prospective register of systematic reviews (PROSPERO).28
The search strategy (see online supplementary appendix table 1) was developed in consultation with a medical librarian at Simon Fraser University, BC, Canada. The search terms were based on a combination of indexed and free-text terms reflecting clinical outcomes of interest to the review, and included the following keywords: ‘HIV, human immunodeficiency virus, acquired immunodeficiency syndrome, HIV/AIDS, stroke, myocardial infarction, cardiac death, cerebrovascular disease, ischemic heart disease, cardiovascular disease and CVD’. These terms were used in combination to execute the searches, which were up to 18 July 2018. Using the Ovid platform, we searched the following electronic databases: MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials and the Cochrane Database of Systematic Reviews. In addition, we screened the abstracts of the International AIDS Society conferences (AIDS 2012, 2014, 2016; IAS 2013) and the Conference on Retroviruses and Opportunistic Infections (CROI 2014, 2015 and 2016). We also searched the reference lists of relevant articles and previous systematic reviews for additional eligible publications. Finally, we set up automatic PubMed literature alerts to identify any new relevant article published while the manuscript was under development.
Supplemental material
We included original research published in English where at least one of the participant groups were individuals living with HIV, and presenting comparative data on the incidence of MI. We included studies in which results were stratified according to HIV status; CD4 cell count; pVL levels; ART use; or exposure to particular ART class or regimen. Studies involving non-human populations; children; as well as those reporting only unadjusted estimates, intermediate, surrogate or CVD biomarker outcomes were excluded (for additional information, see Study selection section in the online supplementary appendix, p1). To reflect the current context of HIV treatment and disease management, we selected studies published from the year 2000 onwards. Although both observational studies and RCTs were eligible for inclusion, we did not include RCTs that were not designed to assess CVD events as a prespecified outcome to avoid bias.
Working independently and in duplicate, two reviewers (OE and GB) scanned the titles and abstracts of the retrieved records for eligibility. The full-text articles of potentially eligible studies were obtained and reviewed in greater details. Disagreements in study selection were resolved through discussion, and where necessary, a third investigator (RSH) was invited to facilitate consensus.
Data extraction and quality assessment
The same two reviewers (OE and GB) conducted data extraction independently using a predesigned data abstraction sheet. We extracted data on study descriptors, sample characteristics, outcome assessment, risk estimate for relevant comparisons and study quality features. Where necessary, we sought clarification directly from study authors through email contact. In cases where data from the same study described the same event risk in multiple publications, we extracted data from the most comprehensive report while supplementing missing study-level information from the others. In keeping with characterisations in the included studies, exposure to ART was categorised as any (or prior/some compared with none), recent (or within the preceding 6 months compared with not recent) and cumulative ART exposure per year of exposure.
The quality of the included studies was assessed according to risk of bias criteria based on the type of study design. As only observational studies were eventually included in the meta-analysis since eligible RCTs were not identified, we made this assessment by evaluating study design features of the eligible observational studies. Following guidelines in the Newcastle-Ottawa Scale for assessing the quality of observational studies in meta-analyses29 and with slight modification of the scoring system to simplify reporting, the risk of bias assessment was performed based on the adequacy of three key domains of the study design features namely: the group/participant selection; comparability of groups; and the exposure and outcome assessments in the individual studies. For each of these key features, we assigned a ‘+’ (plus) sign when this was clearly and adequately described in the study, and a ‘–’ (minus) sign when it was not clearly described or was missing. A detailed description of the results of the quality assessment is available in the online supplementary appendix.
Patient and public involvement
No patients were involved in this study. We used data from published materials only.
Data analysis
We calculated the kappa statistic as a measure of the inter-reviewer agreement for the selection of articles meeting the inclusion/exclusion criteria. For interpretation, we defined a priori the interval for the kappa result using Landis and Koch criteria.30 For effect measure, we assumed the incidence rate ratio (IRR), OR and HR with corresponding sampling variance to be numerical approximate measures of the relative risk (RR) for a given association of interest with the underlying assumption of a generally low event risk (<20%),31–36 and thus combined them as previously described.19 37–40 We tested this assumption in sensitivity analyses by performing separate meta-analyses where studies presenting results reported using a similar effect measure type were pooled. Given the expected variability among eligible studies, we pooled studies using the DerSimonian-Laird random-effects model.41 To minimise bias in our pooled estimates, adjusted risk estimates were not combined with unadjusted estimates. The final set of studies that adjusted for confounders did not consistently adjust for the same set of confounders but were deemed to have sufficient internal validity to permit pooling. For the analysis that quantified the overall RR of MI associated with HIV infection, we performed a sensitivity analysis where we examined the appropriateness of the comparison group by repeating the meta-analysis and including two additional studies that involved a general population comparison group,42 43 as opposed to an HIV-uninfected comparison group. Given the limitations of the I 2 statistics with observational studies and Cochran Q test when the number of studies is small,44 45 we assessed heterogeneity by visual inspection of the forest plots for overlap in the confidence intervals of the individual studies, although the I 2 as a measure of the degree of heterogeneity across studies is reported in the forest plots for completeness. We were unable to perform meta-regression analyses to assess the potential effect of study-level covariates on the pooled estimate due to insufficient studies (<10),46 in each of the meta-analyses. Although we assessed publication bias by visually inspecting and testing for funnel plot asymmetry,47 its interpretation was limited by a lack of sufficient number of studies per meta-analysis.48 49 A p value <0.05 was considered statistically significant. The meta-analysis was conducted using the metafor package of the R statistical programme V.3.3.1.50
Results
Of 8130 records identified through the database search, the final screening process yielded 64 potentially eligible publications on CVD outcomes, 32 of which had relevant data on MI and were included in this meta-analysis (figure 1). Overall, there was near perfect agreement between reviewers on the inclusion of studies (kappa statistic=0.94; 95% CI 0.89 to 0.99). The included studies, most of which were conducted in the USA and Europe, were published between 2000 and 2017 and involved ~383,471 HIV+ and > 798, 424 HIV- individuals (online supplementary appendix table 2: characteristics of the included studies; note: the number of individuals in cohorts with multiple publications was accessed only from one of the publications). The mean duration of follow-up varied across studies from ~1 to 20 years. All 32 publications were non-randomised studies and included two nested case–control studies,11 51 one cohort/nested case–control study,52 and 29 cohort studies; 15 of which were prospective studies, by design.3 7 8 13 42 53–62 Twenty-nine studies were published as full-text journal articles, while three were available as conference abstracts.
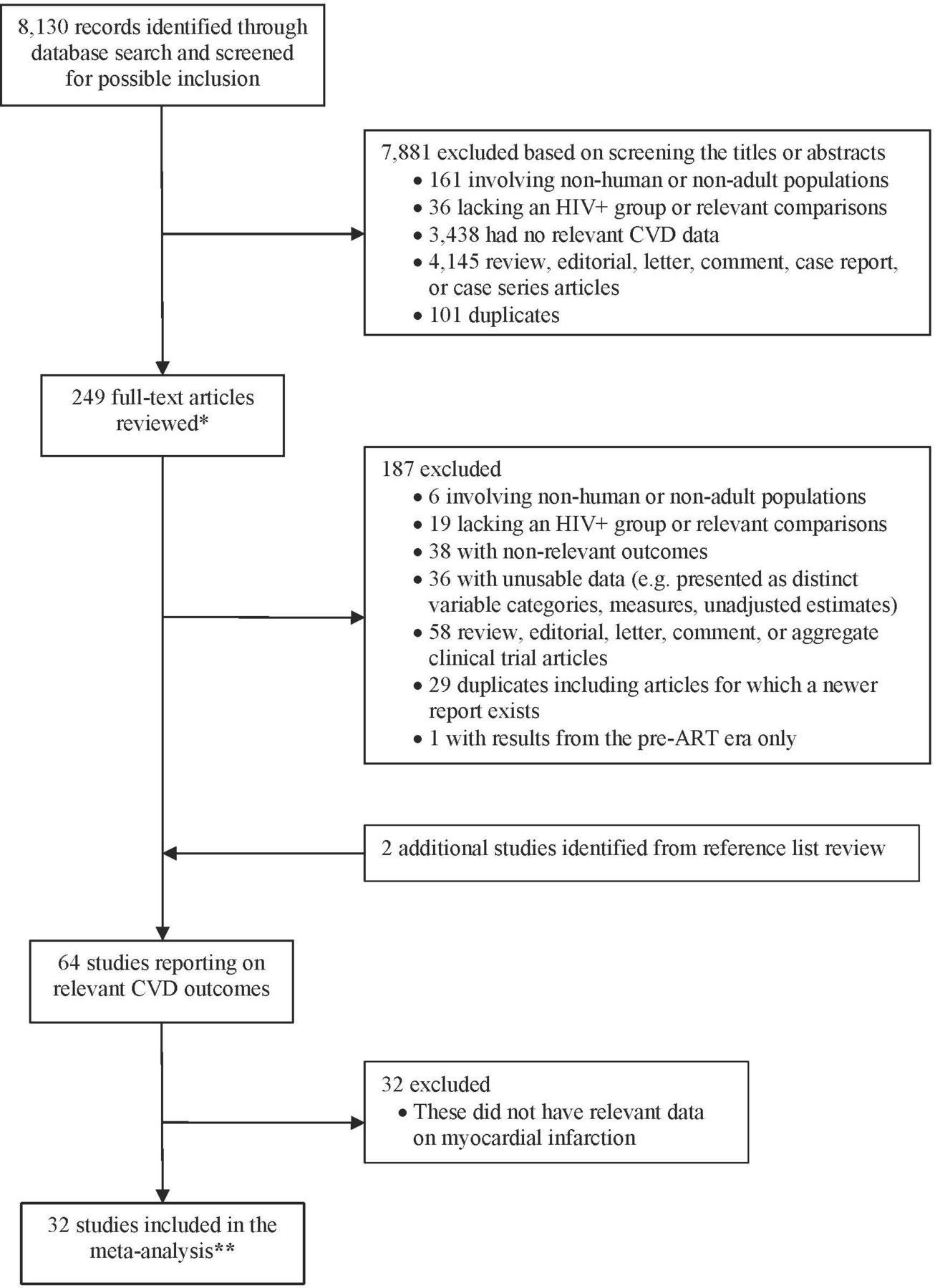
Flow diagram of study selection. *, includes several conference abstract records captured through the database search; **, includes two studies involving a ‘general population’ comparison group. ART, combination antiretroviral therapy. CVD, cardiovascular disease.
In general, the reporting and quality of the methodological aspects of the included studies were variable. Three studies did not provide sufficient information necessary to assess the study quality, as they were reported and available as conference abstract/poster.55 57 63 The eligibility criteria were clearly defined in the majority of studies (94%), description of study participants/ groups was sufficient (100%); however, the exposure or outcome was not adequately ascertained in 15 studies (47%)8 12 24 52 54 56 60 63–70; 1 (7%) of which was published as an abstract63 (see online supplementary appendix table 3: risk of bias in the included studies).
Meta-analysis of the risk of MI
Below, we summarise the results of the meta-analyses of MI risk according to the various risk stratifications assessed. To avoid duplication of reporting, only statistically important RR are stated in text; although both statistically significant and insignificant results are presented in the figures (forest plots).
Risk of MI associated with HIV infection
The pooled RR from the five studies that met eligibility for this assessment of MI risk according to HIV serostatus suggests that HIV+ individuals are more likely to have an MI event compared with uninfected individuals (RR: 1.73; 95% CI 1.44 to 2.08).3 52 56 69 71 In sensitivity analysis (online supplementary appendix figure S1) where we repeated the meta-analysis and included two additional studies that involved a general population comparison group,42 43 the overall pooled RR was 1.60; 95% CI 1.38 to 1.85. Figure 2 shows the forest plots for the association between HIV infection and MI risk. Two studies assessed the risk of MI by HIV serostatus according to whether ART treatment was received.60 72 Compared with uninfected individuals, the pooled RR of MI was significantly higher among HIV+ individuals on ART (RR: 1.80; 95% CI 1.17 to 2.77), but not the ART-untreated HIV+ individuals (RR: 1.25; 95% CI 0.93 to 1.67).

Forest plot of the meta-analysis of the risk of MI associated with HIV infection. ART, antiretroviral therapy.
Risk of MI associated with CD4 cell count and pVL levels
The pooled RR based on combining data from three studies suggests that low CD4 cell count (<200 cells/mm3) is associated with higher MI risk compared with CD4 ≥200 (RR: 1.60; 95% CI 1.25 to 2.04).3 57 68 Conversely, a high pVL (≥100 000 copies/mL) was found to be associated with increased MI risk compared with pVL <100 000 (RR: 1.45; 95% CI 1.11 to 1.90), based on the pooled results from two studies (figure 3).54 68

Forest plot of the meta-analysis of the risk of MI associated with CD4 cell count and plasma viral load levels.
Risk of MI associated with recent ART exposure
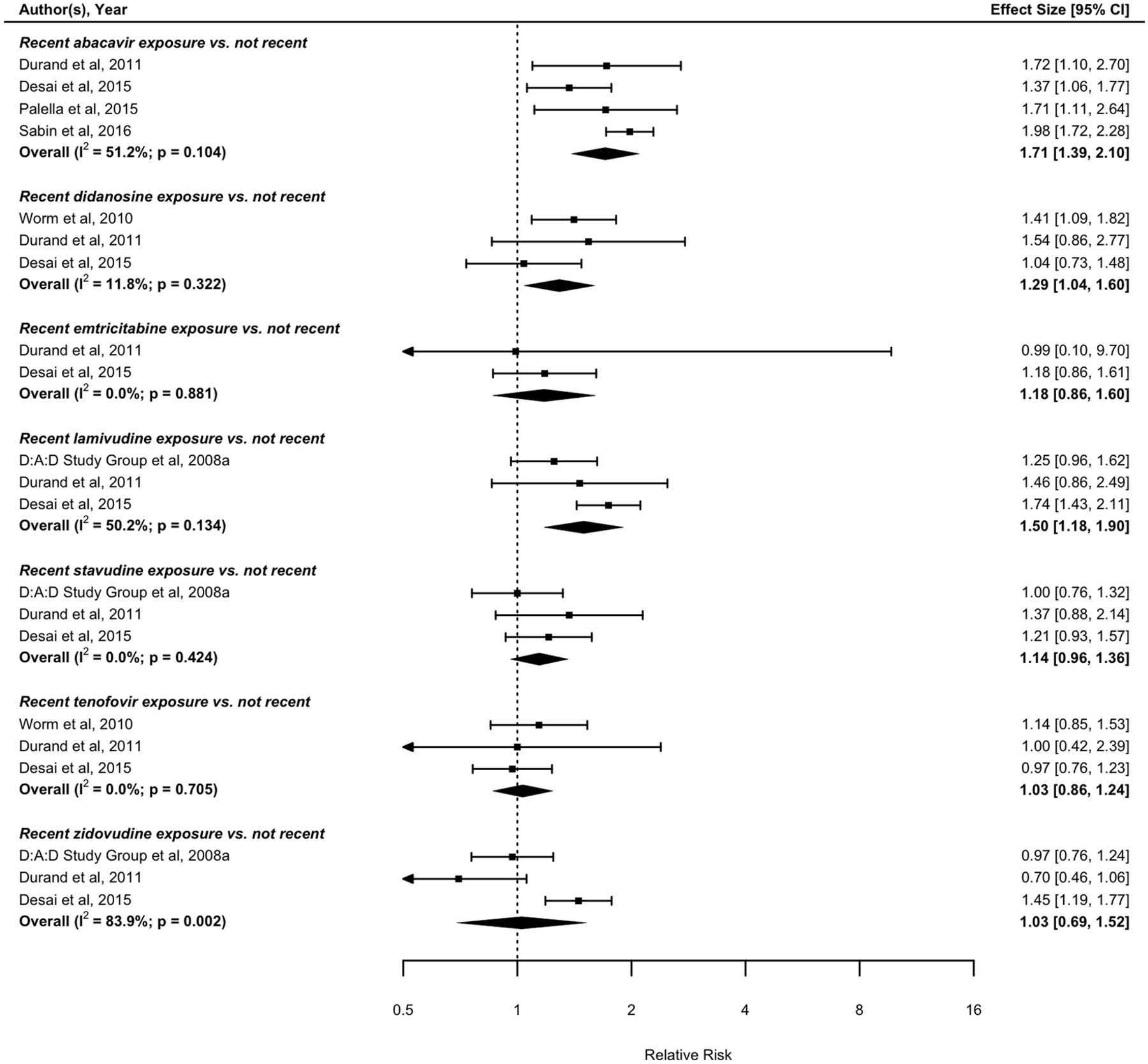
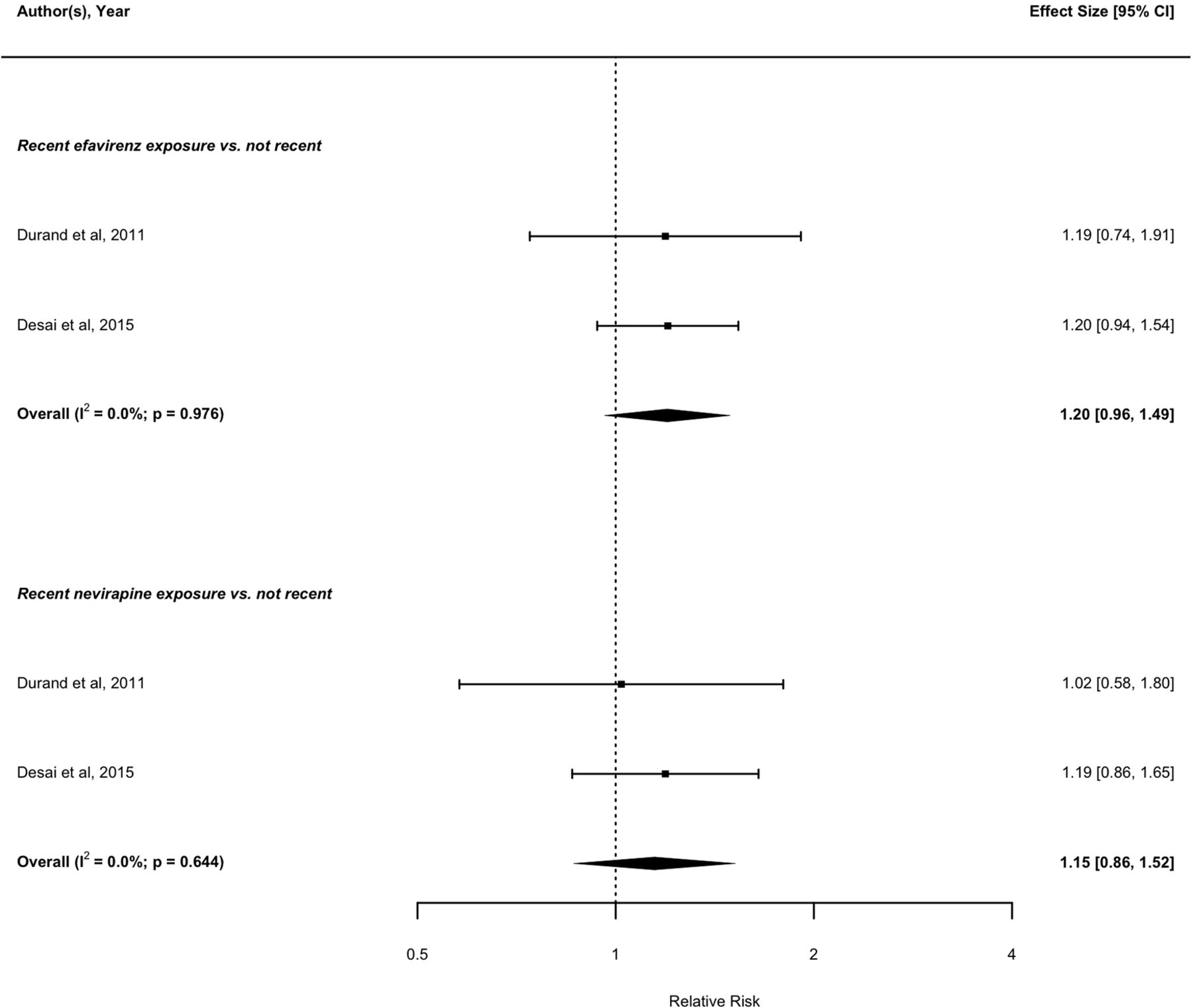
With regards to recent treatment exposure (i.e., within the preceding 6 months), four eligible studies with data on nucleoside reverse transcriptase inhibitor (NRTI) exposure assessed the risk of MI associated with recent compared with not recent abacavir exposure.52 53 55 67 The pooled result from these four studies suggests that recent abacavir exposure is associated with increased risk of MI compared with not recent exposure (RR: 1.71; 95% CI 1.39 to 2.10). Similarly, recent didanosine (RR: 1.29; 95% CI 1.04 to 1.60),52 58 67 and lamivudine (RR: 1.50; 95% CI 1.18 to 1.90),13 52 67 exposure is associated with increased risk of MI compared with not recent exposures. In contrast, there was no detectable association between recent tenofovir,52 58 67 zidovudine,13 52 67 stavudine,13 52 67 emtricitabine52 67 and MI risk compared with not recent exposure (figure 4). Based on pooling data from two studies with data on non-nucleoside reverse transcriptase inhibitor (NNRTI) exposure,52 67 no association was found between recent efavirenz or nevirapine exposure and MI risk compared with not recent exposure (figure 5). Based on pooled results from the studies assessing the MI risk of individual PIs, recent indinavir was associated with increased MI risk compared with not recent exposure (RR: 1.46; 95% CI 1.08 to 1.95).52 67 Recent exposure to other PI regimens including atazanavir,52 67 lopinavir,52 67 ritonavir,52 67 nelfinavir52 67 and saquinavir,52 67 were not found to be significantly associated with MI risk compared with not recent exposure (figure 6).

Forest plot of the meta-analysis of the risk of MI associated with recent exposure to drugs of the NRTI class. NRTI,nucleoside reverse transcriptase inhibitors.

Forest plot of the meta-analysis of the risk of MI associated with recent exposure to drugs of the NNRTI class. NNRTI,non-nucleoside reverse transcriptase inhibitor.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of the meta-analysis of the risk of MI associated with recent exposure to drugs of the protease inhibitor class.
Risk of MI associated with any ART exposure
In terms of any treatment exposure, our meta-analysis did not find an association between exposure to ART and risk of MI compared with no exposure (online supplementary appendix figure A1).62 72 Based on the pooled results from six studies with data on NRTI exposure,8 11 13 52 63 68 individuals receiving abacavir were more likely to have an MI compared with those who did not (RR: 1.58; 95% CI 1.25 to 2.00). We found a similar association between didanosine exposure and MI risk (RR: 1.48; 95% CI 1.16 to 1.90).13 52 68 No detectable association was found between exposure to tenofovir,52 68 zidovudine,13 52 stavudine,13 52 68 emtricitabine52 68 and MI risk, based on our pooled results (online supplementary appendix figure A2). The meta-analysis of studies with data on NNRTI exposure did not find any evidence of an association between either efavirenz52 65 or nevirapine exposure,52 68 and MI risk compared with no exposure (online supplementary appendix figure A3). The pooled RR from four studies demonstrates that PI exposure is associated with an increase in the risk of MI events compared with no exposure to PI (RR: 1.49; 95% CI 1.16 to 1.91).3 6 61 63 When the analysis was limited to two studies comparing recent PI exposure to no exposure,3 63 similar results were found (RR: 1.40; 95% CI 1.16 to 1.69 (data not shown)). For the individual PIs, there was no association between either atazanavir,52 64 66 68 saquinavir,52 68 or nelfinavir exposure,52 68 and MI risk, compared with no exposure (online supplementary appendix figure A4).
Risk of MI associated with cumulative ART exposure
With regards to cumulative treatment exposure, three eligible studies provided relevant data regarding the risk of MI and cumulative ART exposure.12 68 70 We found that cumulative exposure to ART was associated with an increase in the risk of MI per year of exposure (RR: 1.12; 95% CI 1.06 to 1.18) (online supplementary appendix figure A5). For exposure to NRTI regimens, we estimated an increase in MI risk per year of exposure to abacavir (RR: 1.08; 95% CI 1.01 to 1.15) based on pooling data from two eligible studies.12 58 Similar to abacavir, cumulative zidovudine exposure was associated with an increase in MI risk per year of exposure (RR: 1.05; 95% CI 1.01 to 1.10).11 13 We found no association between cumulative exposure to either didanosine,11 13 tenofovir,11 58 lamivudine11 13 or stavudine,11 13 and MI risk per year of exposure (online supplementary appendix figure A6). The overall RR suggests that cumulative NNRTI exposure as a class (RR: 1.02; 95% CI 0.97 to 1.08),59 70 72 or as individual drugs (nevirapine and efavirenz),11 58 is not significantly associated with increased risk of MI events per year of exposure (online supplementary appendix figure A7). Three eligible studies reported data assessing the risk of MI associated with cumulative exposure to PIs as a class.59 70 72 There was an increase in risk of MI per year of exposure to PIs (RR: 1.14; 95% CI 1.03 to 1.26). For individual drugs, cumulative exposure to lopinavir with ritonavir (RR: 1.19; 95% CI 1.03 to 1.39),11 58 but not nelfinavir,11 58 was found to be associated with increase in the risk of MI events per year of exposure (online supplementary appendix figure A8).
Sensitivity analyses
The strength and direction of the overall RR from the various meta-analyses remained robust in sensitivity analyses where estimates reported using similar effect measures were pooled. For example, HIV+ individuals continued to have higher risk of MI events compared with uninfected individuals when pooled using either IRRs (overall effect: 1.68; 95% CI 1.17 to 2.40) or HRs (overall effect: 1.75; 95% CI 1.24 to 2.48) effect measures, compared with a RR of 1.73; 95% CI 1.44 to 2.08, obtained from pooling results reported using multiple relative effect measures (online supplementary appendix figure S2).
Discussion
This updated systematic review and meta-analysis assessing the risk of MI among people living with HIV reflects contemporary ART era and found the following: (1) HIV+ individuals have a greater risk of MI compared with uninfected individuals; and among HIV+ individuals, (2) low CD4 cell count (<200 cells/mm3) and high pVL (>100 000 copies/mL) are associated with increases in MI risk compared with higher CD4 or lower pVL, respectively; (3) cumulative ART exposure is associated with a greater risk of MI per year of exposure; (4) among NRTIs, any type of exposure to abacavir; cumulative exposure to zidovudine; and recent exposure to either didanosine or lamivudine are significantly associated with higher risk of MI; (5) compared with no exposure, any or cumulative exposure to PIs as a class; cumulative exposure to lopinavir with ritonavir; and recent indinavir exposure were associated with higher risk of MI; (6) NNRTIs assessed either as a class or individually were not associated with increased MI risk.
Previous meta-analyses comparing CVD risk among HIV+ and uninfected individuals reported estimates for the association between HIV-seropositivity and MI (RR: 1.79; 95% CI 1.54 to 2.08)19 or CVD (RR: 1.61; 95% CI 1.43 to 1.81)20; risk that are similar to our findings for MI (RR: 1.73; 95% CI 1.44 to 2.08). As has been previously hypothesised,3 23 73–75 the probable mechanistic pathway through which HIV infection can induce MI may include a cascade of events involving chronic inflammation, immunodeficiency/CD4 cell depletion, endothelial dysfunction, increased thrombosis and accelerated atherosclerosis that typically accompany both controlled and uncontrolled HIV disease. Relative to uninfected individuals and similar to what we found (RR: 1.80; 95% CI 1.17 to 2.77), one of the previous meta-analysis also reported a higher risk of CVD among ART-treated individuals (RR: 2.00; 95% CI 1.70 to 2.37).20 We suspect that the higher MI risk among ART-treated HIV+ individuals may not necessarily be attributable to ART alone but rather to the combined effect from a host of factors including HIV itself, ART, and other comorbid risk factors which have been individually shown to contribute to MI risk.3 5 76 77 Furthermore, the risk associated with cumulative ART exposure may be an index of the duration of HIV infection with its attendant inflammation, and not entirely the effect of cumulative exposure to ART per se.
Specific to abacavir and MI risk, our findings were similar to reports from a previous meta-analysis of observational studies of MI,16 but different from those of the meta-analysis of RCTs,17 18 or reports from aggregate clinical trial studies,14 15 that suggested no risk associated with abacavir exposure. Although observational studies and RCT results regarding MI and CVD risk due to abacavir exposure among people living with HIV are largely at odds, the Simplification with Tenofovir-Emtricitabine or Abacavir-Lamivudine trial is the first RCT to support observational studies finding of increased risk of CVD with exposure to abacavir.78 Based on the available evidence to date, the controversy regarding the potential association between abacavir use and risk of MI will likely continue to plague the field of HIV therapeutics until such a time when definitive evidence describing the underlying mechanism can be produced.79 80 A sufficiently powered RCT with long follow-up and including real-world populations reflective of those typically seen clinically may be needed to fully resolve this clinical controversy.
Unlike our results where a class-level effect was evident for PIs, pooled aggregate clinical trial data after 1 year of treatment with four different PI-based regimens did not find evidence of an increased risk associated with PI compared with NRTI regimen (RR: 1.69; 95% CI 0.54 to 7.48).81 When we pooled data of individual PIs separately, we did not observe the same ‘class-level’ results. In our analysis, different PI regimens carried different risks. For example, while recent indinavir and cumulative lopinavir-ritonavir exposure were associated with increased MI risk, nelfinavir or atazanavir did not appear to contribute to MI risk irrespective of the type of exposure data that were pooled.
In terms of the scope and design, our study differs from previous meta-analyses on this topic in several ways. First, we used an expanded search strategy that included more data sources and search of conference archives compared with prior meta-analyses.16–20 Second, as the association of HIV and ART may affect the risk of MI and other CVD events differently, we did not assess the risk of CVD in general, as was done in previous meta-analysis.20 Third, we have used more recent risk estimates from studies with longer follow-up such as the Data Collection on Adverse Events of Anti-HIV Drugs (D:A:D) study. Fourth, we have included studies published between 2000 and 2017 with reported data from the post-ART era. The historical nature of some of the studies included in previous meta-analysis may have limited their relevance in contemporary times. Finally, this systematic review analysed several additional drug exposure comparisons and clinical measures (eg, CD4 cell count, pVL) in relation to MI risk that had not been previously examined.
There are several important considerations that should be taken into account in the interpretation of the results of this study. Accurate characterisation of the risk of MI and CVD outcomes in general may be confounded by a number of factors that may have affected our conclusions. The first concern has to do with the differences in the risk factors, drug exposure, HIV-related variables, or population considered in the included studies. Indeed, no two studies of HIV+ individuals from different underlying populations can have participants with the same exact demographic, clinical and drug exposure profile—all of which play a role in overall health outcomes. Given that studies typically included in a global meta-analysis such as ours do not come from the same underlying source population, we acknowledge that there may be some differences in the population distribution in the included studies (eg, in the distribution by age, sex, disease stage, medication profile/history) that we were unable to account for. A second concern relates to the variability in the quality and design features of the included studies, which may have influenced the results of the meta-analyses and thus the conclusions drawn. Although the majority of included studies were cohort-based (90%), almost one half (47%) were retrospective in nature and did not adequately report how the exposure or outcome was ascertained including whether an adjudication protocol was applied in the ascertainment of MIs. It has been shown that the application of an adjudication protocol in the study of MI and other CVD events is important to ensuring accurate identification of events as relying only on administrative diagnostic codes could result in misclassification.82 While some studies retrospectively assessed MI and relied on International Classification of Diseases codes alone—something that is quite common in large epidemiological studies of MI,76 others followed participants over time and prospectively assessed and validated the MI events. It is unclear how differences in MI definition across studies may have affected our results although in two studies from the same underlying population (Veterans Ageing Cohort Study) that used similar but not the same definitions for MI,3 83 the RR differed slightly: 1.48 (95% CI 1.27 to 1.72)3 versus 1.76 (95% CI 1.49 to 2.07).83 Regarding studies that quantified the risk of MI associated with HIV infection, the available evidence based on the included studies all point in the same direction suggesting an increase in MI risk. However, we noted some variability in the design and quality of the studies, something that may have contributed in part to the observed heterogeneity. For example, three studies did not provide sufficient information on the exposure or outcome ascertainment in the studies.52 56 69 Furthermore, the appropriateness of the HIV-uninfected group used for comparison purposes is critical in the assessment of MI risk associated with HIV infection; an issue that has been extensively reviewed elsewhere.84 While some studies made this comparison using an HIV-uninfected group, other studies used the general population group for comparison. In sensitivity analysis, the overall RR of MI associated with HIV infection was reduced when we included in the meta-analysis two additional studies involving a ‘general population’ comparison group,42 43 therefore highlighting the importance of using an appropriate control group.
Another potential concern relates to differences in the extent to which key confounding factors were adjusted for in the individual analysis contributing to the meta-analysis. For example, some studies lacked data on smoking—an important risk factor for CVD in general, and therefore did not account for it in the analyses.52 60 65 In this regard, we noted that the included studies did not consistently control for the exact same set of confounders which may have undermined their internal validity and explained some of the differences in the effect measures from the individual studies. There is also the potential for residual, unmeasured confounding given the observational nature of the included studies. Therefore, heterogeneity arising from differences in study design or other quality features may have influenced the results and thus the overall conclusions drawn. Although we observed heterogeneity across results of studies included in some of the meta-analyses, this is a common limitation in meta-analysis especially those involving observational studies.44 Our a priori choice of employing the random-effects modelling strategy was driven in part by this expected variability among studies.85 Furthermore, our study combined results presented using several different relative effect measures with the assumption that these represent approximately the same numerical value.31–36 In sensitivity analyses, we did not find any evidence of bias in our pooled estimates, as these did not differ importantly from the pooled estimates we obtained when we combined studies reporting results using the same effect measure. Moreover, we reached comparable conclusions with previous meta-analyses that combined,19 or did not combine HR estimates with OR, and RR.16
Also, some of the meta-analyses in our study such as those examining the risk of MI in relation to CD4, pVL or use of specific ARV regimens were based on a small number of studies (only 2–3 studies), which is a serious limitation. It is important to also consider this point in the interpretation of these specific findings. We acknowledge that the results from such meta-analyses could have been strengthened with the inclusion of additional eligible studies. Nevertheless, in the absence of sufficient number of studies examining these relationships, our results could be viewed as the best available evidence summarising the risk of MI associated with CD4, pVL or use of specific ARV regimens among people living with HIV.
Given the foregoing discussion in relation to the design and quality aspects of the included studies as well as issues of sufficiency of available studies examining several potential associations with MI risk, additional rigorously conducted studies with extensive confounding factor stratification/adjustment are needed to further confirm our findings. Furthermore, considering that the majority of the studies on this topic are carried out in North America and Europe, our study highlights the need for more research to be conducted in resource limited settings where most people living with HIV reside.
Conclusions
In summary, this updated systematic review and meta-analysis suggests that HIV infection, ART use in general including exposure to specific ART class (eg, PIs) and regimen (eg, abacavir) are associated with increased risk of MI. These findings should be interpreted in light of the key considerations that we have highlighted in this review. We found the totality of the evidence for an association between HIV infection and MI to be compelling. With respect to ART and MI risk, HIV treatment strategies should certainly consider cardiovascular risk factors including exposure to particular ART drugs as part of patient-tailored care. However, given what we currently know about ART’s effectiveness, the benefits of ART for the treatment of HIV infection in terms of viral suppression and immune reconstitution should be balanced against its potential unfavourable impact on MI. Specific to abacavir and MI risk where there is conflicting evidence between observational studies and RCTs, additional rigorously conducted studies in real-world populations are needed to definitively substantiate our findings and strengthen the existing evidence on this topic. Given the multiple potential contributory and mechanistic pathways to developing MI among HIV+ individuals and the complexity/feasibility of designing a large enough study to completely tease apart the potential contributions of each of the factors believed to increase the risk of MI, managing known modifiable risk factors for CVD outcomes (eg, smoking) through behavioural/lifestyle interventions, would be an excellent first step in reducing the incidence and risk of MI among people living with HIV.
Acknowledgments
We thank Simon Fraser University library staff for the assistance provided during the search strategy development.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
Footnotes
Contributors OE, MWH, SAL, JSGM and RSH conceived and designed the study. OE, GB and RSH acquired the data. OE performed the statistical analysis with input from CHG, CF-V and EJM. OE, GB, CHG, MWH, SAL, MB, SG, CF-V, AA, EJM, JSGM and RSH contributed to the interpretation of the data. OE drafted the manuscript. OE, GB, CHG, MWH, SAL, MB, SG, CF-V, AA, EJM, JSGM and RSH reviewed the manuscript critically for important intellectual content and approved the final version submitted for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data and materials used in this research are available in Medline/PubMed. References have been provided.