Article Text

Abstract
Objectives To examine the longitudinal relationship between cardiovascular fitness in young adult men and future risk of migraine and to estimate eventual differential effects among categories of body mass index (BMI) and blood pressure.
Design National, prospective, population-based cohort study.
Setting Sweden 1968–2014.
Participants 18-year-old Swedish men (n=1 819 828) who underwent mandatory military conscription examinations during the years 1968–2005.
Primary and secondary outcomes The primary outcome was the first dispensation of prescribed migraine-specific medication, identified using the Swedish Prescribed Drug Register. The secondary outcome was documented migraine diagnosis from the Swedish National Hospital Register.
Results During follow-up, 22 533 men filled a prescription for migraine-specific medication. After confounding adjustment, compared with high cardiovascular fitness, low and medium fitness increased the risk of migraine-specific medication (risk ratio (RR)low: 1.29, 95% CI 1.24 to 1.35; population attributable fraction: 3.6%, 95% CI 1.7% to 5.3% and RRmedium: 1.15, 95% CI 1.12 to 1.19; population attributable fraction: 8.0%, 95% CI 4.0% to 11.7%). To assess potential effect measure modification, stratified analyses of these association by levels of BMI and blood pressure showed that lower fitness levels increased risk of migraine across all groups except among underweight men or men with high diastolic blood pressure.
Conclusions Young men with a lower cardiovascular fitness had a higher long-term risk of developing pharmacological prescription-requiring migraine. This study contributes with information regarding risk factors for migraine in men, an understudied population in migraine research.
- cardiovascular fitness
- cohort
- men
- migraine
- prospective
- risk factor
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is a large, longitudinal study of a nearly total population sample of young Swedish men undergoing mandatory military conscription examinations between 1969 and 2005 (n=1 819 828), employing objective measurements of cardiovascular fitness at baseline.
The study has a long follow-up time (range: 2–46 years) and relies on high-quality national register data to identify men, an understudied population in migraine research, who later develop prescription-requiring migraine.
The incidence of migraine in our study is likely conservative since men with undiagnosed migraine or those only using over-the-counter or preventative migraine medication are not captured in the available data.
Although analyses were adjusted for several important potential confounding variables, some residual confounding may remain in the estimates (such as smoking and alcohol consumption).
Introduction
Migraine is an intermittent neurological disorder with strong influences on the vascular system.1 Cardiovascular fitness, a state indicating overall capacity of the cardiovascular and respiratory systems and the ability to carry out prolonged strenuous exercise, has been shown to have beneficial effects on vascular health as well as associated with a reduced incidence of several neurological and cardiovascular disorders.2–4 However, data on the relationship between cardiovascular fitness and the development of migraine are lacking. Higher levels of physical activity, a behaviour in which body movement produced by muscle action increases the energy expenditure and enhances or maintains cardiovascular fitness,2 have been prospectively associated with a reduced risk of migraine.5 Physical activity is strongly correlated but is not interchangeable with cardiovascular fitness, as the latter also depends on other components such as genetic makeup.2
Although uninformative regarding direction of causality, cross-sectional studies have shown an inverse association of peak oxygen uptake with migraine,6 whereas findings from cross-sectional studies of migraine and physical activity have been heterogeneous.7–10 Among individuals with migraine, regular physical activity appears to have alleviating effects on migraine symptoms such as frequency and intensity.11 However, acute physical exercise may also be a trigger of migraine episodes,12 and individuals with migraine or severe headaches might therefore be more reluctant to exercise. There is also a high comorbidity between migraine and cardiovascular conditions.13 While factors affecting cardiovascular health, such as weight and blood pressure, have also been shown to influence migraine prevalence,14 15 the contribution of cardiovascular fitness to long-term migraine risk may be differential across strata of body mass index (BMI) and blood pressure, though this has yet to be formally assessed.
Migraine is two to three times more prevalent in women, and findings on factors influencing migraine in men are scarce.16
The primary aim of this study was to estimate the effect of baseline cardiovascular fitness level on the long-term risk of prescription-requiring migraine in a large, prospective population-based cohort of young Swedish men with objective measures of cardiovascular fitness at baseline and a long follow-up time. The secondary aim was to evaluate whether the relationship between cardiovascular fitness and future risk of migraine is modified by baseline levels of BMI or blood pressure.
Methods
We performed a population-based prospective study of young Swedish men enlisting for military service. Exposure variables were obtained at conscription (baseline) from records in the Swedish Military Service Conscription Register. Data from this register were linked to the Swedish Prescribed Drug Register, the National Hospital Registers, the Longitudinal Integration Database for Health Insurance and Labour Market Studies and the Swedish Cause of Death Register. Linkage of individual data was made possible by the unique personal identification number assigned to each registered person in Sweden. After linkage, all data were anonymised and coded by Statistics Sweden to maintain the confidentiality for the included men.
During follow-up, use of migraine-specific medication identified through the Swedish Prescribed Drug Register served as a proxy for migraine. Further, in a secondary analysis, hospital diagnoses of migraine, identified in the National Hospital Register, were recorded as outcomes.
Study population
The source population of the study comprised all men (n=1 819 828) who enlisted for military service during 1968–2005, were 16–25 years old and had a documented test centre location. Enlistment was mandatory during this period for all Swedish men. Only individuals with severe chronic medical or mental conditions, serious disabilities or incarceration were granted exemption (in all, 2%–3% of the male population per year). The vast majority were 18 years old at time of conscription (mean age 18.2, SD=0.7). To reduce the risk of possible reverse causation, men with a prescribed migraine-specific medication or migraine diagnosis prior to or during the 2 years after conscription (identified through the National Hospital Register and Conscription Register) were excluded from all analyses, as were men who died or emigrated within 2 years of conscription, as well as individuals with missing data on cardiovascular fitness (figure 1). For analyses using the Prescribed Drug Register, men who died or emigrated prior to the start of the register (2005) were excluded (figure 1).

Flowchart of the study populations showing included and excluded subjects and number of outcomes.
Ascertainment of exposure: cardiovascular fitness
All men underwent a 2-day examination at one of six Swedish conscription centres (Southern, Western, Eastern, Central/Bergslagen, Northern lower and Northern upper). Cardiovascular fitness was evaluated at all centres for all included years. Cardiovascular fitness was objectively measured by a physician using a standardised maximal cycle ergometric test. Following 5 min of warm-up, the work rate was increased continuously by 25 W/min until exhaustion. The final work rate (Wmax) was recorded, divided by body weight and then converted into a stanine score, which served as a measure of cardiovascular fitness. We have previously observed that the frequency distribution of cardiovascular fitness in the dataset is right skewed and not normally distributed. Therefore, as in other studies,17 cardiovascular fitness categories were trichotomised as low (score 1–4), medium (score 5–7) and high (score 8–9). Although the protocol for the ergometer test has changed over the years, average cardiovascular fitness scores have remained stable over time (<1% change). The conscription cardiovascular fitness test has also been shown to have good reliability and validity.18
Covariates
Weight, height and systolic and diastolic blood pressures were measured by a physician following a written standard protocol. Systolic and diastolic blood pressures were measured on the first conscription day after 5–10 min rest in the supine position. One measurement was generally performed, although when systolic blood pressure was over 145 mm Hg or diastolic blood pressure was outside the range of 50–85 mm Hg, a second measurement was made on the following day and included in the register instead. Weight (kg) and height (m) were measured and BMI was calculated as (kg/m2). BMI values <10 and >60 km/m2 were treated as implausible values and excluded. BMI was categorised as low (<18.5 kg/m2), normal (18.5–24.9 kg/m2) and high (>25.0 kg/m2). Systolic and diastolic blood pressures were divided into three groups; systolic blood pressure: ≥140, 120–139 and ≤119 mm Hg and diastolic blood pressure: ≥80, 66–79 and ≤65 mm Hg. Information on conscription test centre, conscription year, age at conscription and parental education level were also taken into account as potential sources of confounding. We anticipated differences in conscription procedures and diagnosis frequencies depending on enlistment year. Socioeconomic status has also been shown to affect level of cardiovascular fitness in the current dataset and has been associated with migraine risk.19 Therefore, we controlled our analyses for parental education as a proxy for socioeconomic status. Information on parental education (80% coverage), as well as emigration, were collected from the Longitudinal Integration Database for Health Insurance and Labour Market Studies (Swedish acronym LISA; http://www.scb.se/Pages/List____257743.aspx) at Statistics Sweden. The LISA database includes data from all Swedish residents aged 16 years and older and is annually updated. Parental education information (maternal and paternal education treated separately) was graded in three levels: prehigh school education (up to 9 years), high school education and university/postgraduate education.
Outcome variables
The outcome of migraine between age 20 and 60 was obtained using first recorded dispensing of prescribed migraine-specific medication, identified using the Swedish Prescribed Drug Register. This national register started in 2005 and includes detailed information on all prescription drugs (from primary care and hospital-based care) dispensed by all pharmacies in Sweden.20 The Prescribed Drug Register is updated monthly, and the prescriptions are grouped according to the Anatomical Therapeutic Chemical classification (WHO). The following migraine-specific medications were included: sumatriptan (N02CC01), naratriptan (N02CC02), zolmitriptan (N02CC03), rizatriptan (N02CC04), almotriptan (N02CC05), eletriptan (N02CC06), frovatriptan (N02CC07), dihydroergotamine (N02CA01) and ergotamine (N02CA02). As these medications are also indicated for cluster headache, men with this diagnosis (International Classification of Diseases (ICD)-10: G44.0; ICD-9: 346C; ICD-8: 346.01) in the National Hospital Register were excluded from the analyses.
Secondary analyses were additionally performed using ICD codes for migraine diagnosis from the Swedish National Hospital Register as an outcome (ICD-10: G43; ICD-9: 346A,B,X,W; ICD-8: 346.09). This register contains both inpatient and outpatient diagnoses recorded in a hospital setting including referrals to neurologists/migraine specialists and emergency visits. In Sweden, it is mandatory for all private and publicly funded hospitals to register one principal diagnosis at discharge and up to 30 contributory diagnoses. Register coverage for all inpatient care increased gradually during 1968–1986, and diagnoses from hospital outpatient care were documented starting in 2001. The Swedish National Hospital Register is a national, population-based register with high coverage; it is validated with positive predictive values of (85%–95%) for most ICD diagnoses.21
Statistical analyses
To address the primary aim that is, how cardiovascular fitness at baseline affects risk of migraine during follow-up, we calculated risk ratios (RRs) and 95% CIs using Poisson regressions, with exposure time as an offset to correct for differences in exposure time, and robust SEs. Using these models, we also calculated the maximum likelihood estimations for the adjusted population attributable fractions (PAF) with corresponding 95% CIs.22 23 We here interpret PAFs as the estimated percentage of all cases of the outcome during follow-up that could have been prevented if the men of specified cardiovascular fitness group had instead belonged to the group with high cardiovascular fitness. We chose to perform RR analyses due to the aggregation of both new and older records in the Prescribed Drug Register at register initiation. For this reason, it was not possible to establish the exact time of first prescription, rendering Cox proportional hazards models unsuitable.
All analyses were adjusted for age at conscription, conscription region, conscription decade and parental education (model 1). Given that BMI might affect both cardiovascular fitness and migraine, we also performed an additional model (model 2) additionally adjusting for BMI,24 though there is uncertainty about the directionality of this relationship. To address our secondary aim that is, whether the relationship of cardiovascular fitness and migraine was modified by levels of BMI or blood pressure, we stratified the risk estimates from model 1 by categories of baseline BMI, as well as systolic and diastolic blood pressure, as previously defined. Missing data on parental education levels were treated as additional, separate category. High cardiovascular fitness was used as the reference category.
We also performed secondary analyses to evaluate the relationship between cardiovascular fitness and risk of hospital-based migraine diagnosis, which likely includes the most severe migraine cases. Since time of diagnosis information was available in this register, Cox proportional hazards models were used to estimate HRs and 95% CIs. The follow-up period began at conscription (baseline), and person-time was included until time of (1) first record of migraine in the National Hospital Register, (2) death, (3) emigration or (4) at the end of follow-up, that is, on 31 December 2014, whichever happened first. Observed follow-up ranged from a minimum of 2 years to a maximum 46 years. All death dates were obtained from the Swedish Cause of Death Register, which has kept record of virtually all deaths in Sweden since 1961. We performed separate analyses for outpatient migraine diagnoses only, as well as outpatient and inpatient diagnoses, together. By removing the inpatient diagnoses, individuals with the highest degree of psychiatric and somatic comorbidities, medication overuse and highest pain scores were excluded25 rendering the patient group more homogeneous. We also performed a separate set of analyses including only primary diagnoses of migraine.
All analyses were conducted using SAS V.9.4 (SAS Institute).
Patient and public involvement
There was no patient involvement in this register-based study.
Results
Baseline characteristics for the full study population and stratified by levels of cardiovascular fitness in the study population are shown in table 1. Men with lower cardiovascular fitness levels were more likely to have lower parental education, higher BMI and higher systolic blood pressure than men with higher fitness. After we applied the exclusion criteria, analyses of dispensed migraine-specific medication were conducted using data from a total of 1 143 831 participants. Secondary analyses of migraine diagnoses documented in the National Hospital Register were conducted with 1 213 104 included participants (figure 1).
Baseline characteristics of the study population, stratified by cardiovascular fitness level in a cohort of 1 142 831 male conscripts included in the analyses of migraine-specific medication prescription before age 60
Cardiovascular fitness and future dispensing of migraine-specific medication
Prescriptions for migraine-specific medication were filled by 22 533 of the included men (2.0%). Compared with those with a high cardiovascular fitness level at conscription, both low and medium levels of fitness were associated with an increased risk for use of migraine-specific medication during follow-up (adjusted RR 1.29, 95% CI 1.24 to 1.35 and 1.15, 95% CI 1.12 to 1.19; table 2). The PAF of medium cardiovascular fitness for migraine-specific medication (8.0%) was higher than that of low fitness (3.6%). Including BMI as an additional potential source of confounding in the multivariable models did not change the RRs or PAFs substantially. The proportion of men with missing values for cardiovascular fitness was 31.6% for men with migraine-specific medication and 32.4% for men without.
Risk ratios and population attributable fractions for prescribed migraine-specific medication before the age of 60 in relation to cardiovascular fitness levels in young adult men
Risks stratified by categories of BMI and blood pressure
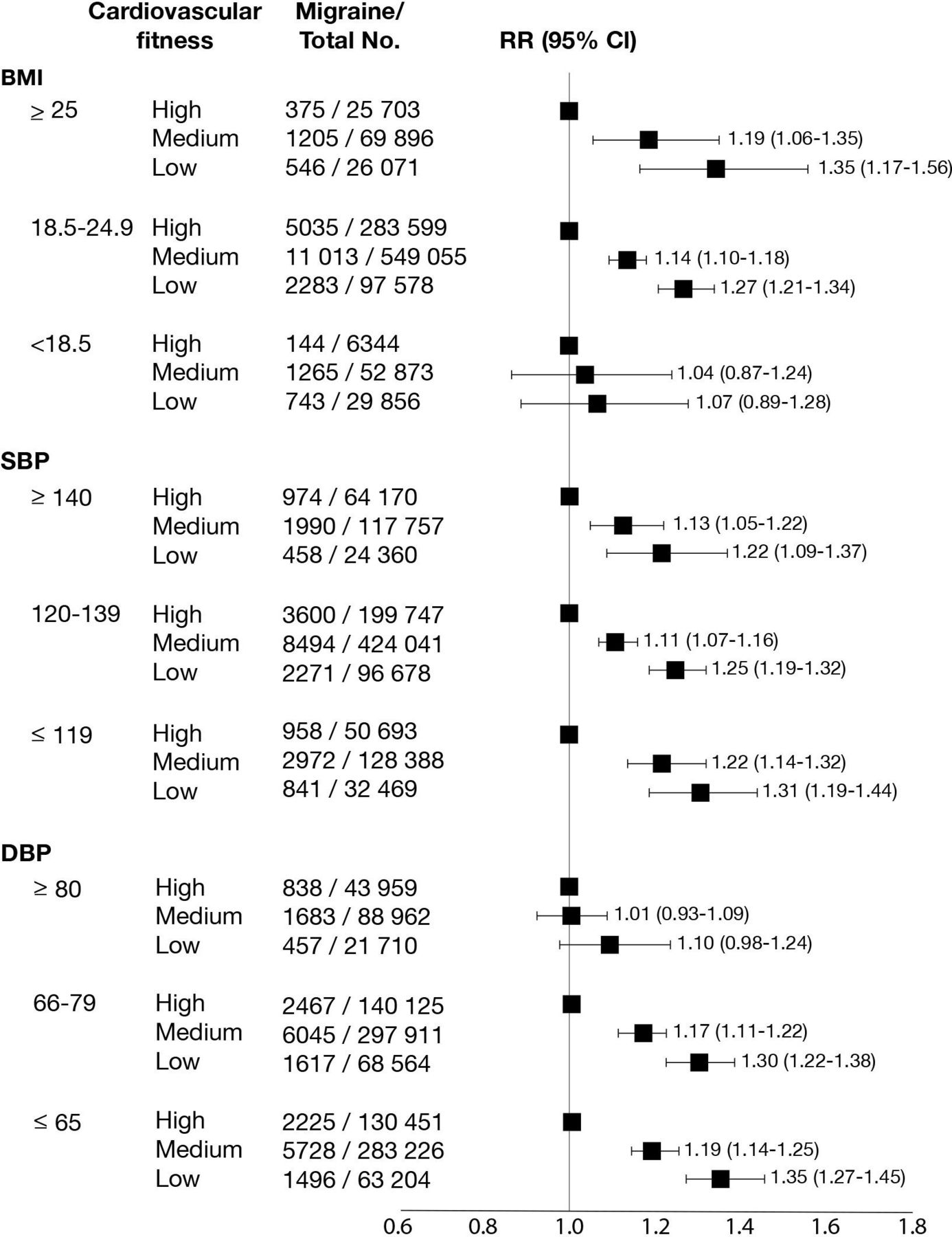
The association of cardiovascular fitness with future migraine-specific medication was analysed in separate strata of BMI and blood pressure groups to assess potential effect measure modification (figure 2). Low and medium fitness were associated with an increased risk for migraine medication prescription among men with high and normal BMI, but no increased risk for the outcome was observed among underweight men. On stratification for systolic blood pressure levels, low and medium fitness had similar associations with future migraine medication across all three categories. Fitness was not associated with future migraine-specific medication prescription in men with high diastolic blood pressure (≥80 mm Hg) but was associated with increased risk of prescription in men with lower diastolic blood pressures (in 66–79 mm Hg as well as ≤65 mm Hg groups).
{kind=link}
{kind=link}
RRs of prescribed migraine-specific medication in relation to cardiovascular fitness levels stratified by categories of BMI, SBP and DBP at baseline. RR adjusted for age, conscription calendar year and region parental education. BMI, body mass index; DBP, diastolic blood pressure; no., number of events; RR, risk ratio; SBP, systolic blood pressure.
Cardiovascular fitness and future migraine diagnosis
Migraine diagnoses were recorded in the National Hospital Register for 10 043 men (0.8% of the entire study population). Most (82%) were primary diagnoses. Approximately one-third of the men with a migraine diagnosis in the National Hospital Register were also observed to have a migraine medication prescription in the Prescribed Drug Register. Lower cardiovascular fitness was found to increase the risk of a first-time migraine outpatient diagnosis (table 3). Adding migraine codes for inpatient migraine to the outpatient codes did not result in a substantial change in our findings. Associations were similar when analysing only primary migraine diagnoses. For primary outpatient diagnoses, the HR for low and medium cardiovascular fitness were 1.15, 95% CI 1.05 to 1.26 and 1.07, 95% CI 1.01 to 1.14, respectively. For combined primary outpatient and inpatient diagnoses, the HR for low fitness was 0.98, 95% CI 0.91 to 1.09 and HR for medium fitness was 1.03, 95% CI 0.98 to 1.09.
HRs of migraine diagnoses, recorded in the National Hospital register, in relation to cardiovascular fitness levels in young adult men followed for up to 46 years
Discussion
In this large, prospective cohort of young adult men, cardiovascular fitness was inversely associated with future prescription-requiring migraine. Though quite similar, the risks were somewhat larger for filled migraine-specific drug prescriptions than for outpatient migraine diagnosis. The increased relative risk of migraine among those with a low level of cardiovascular fitness was higher than for those with a medium level fitness. However, more new migraine cases detected in this study were attributable to medium cardiovascular fitness, which was more common in the study population, rather than to low cardiovascular fitness.
Comparisons with other studies
This longitudinal, population-based study provides new insights into the effects of cardiovascular fitness on migraine risk. While not directly comparable with cardiovascular fitness, two prospective studies have previously evaluated the relationships between physical activity and migraine with inconsistent results.5 8 We emphasise the importance of distinguishing cardiovascular fitness from physical activity. Cardiovascular fitness is more strongly related to health outcomes than physical activity, and activity not resulting in an increase in fitness level may not provide protective effects against adverse health outcomes.26 For this reason, studies of cardiovascular fitness in addition to physical activity are of great importance. A cross-sectional study found an inverse relationship of peak oxygen uptake and migraine in adults younger than 50,6 but given its cross-sectional study design, no conclusions can be made regarding the direction of the observed effect.
Effect measure modification by BMI and blood pressure
The association of cardiovascular fitness and migraine was only observed in men with normal and high BMI but not in those with low BMI. Prospective studies of BMI and later risk of migraine appear to be lacking, but a meta-analysis of cross-sectional studies concluded that the risk of migraine appears to be moderately increased in both obese and underweight individuals.14 Our results suggest that among men with a low BMI at age 18, there was no additional beneficial effect of having a higher cardiovascular fitness with respect to prescription-requiring migraine risk later in life. It should, however, be noted that the number of men in this category was limited. It is also possible that there might be a common underlying factor influencing both BMI and migraine.
While an association between lower cardiovascular fitness and later migraine was observed across all categories of systolic blood pressure, this was not the case for the group with a diastolic blood pressure of ≥80 mm Hg. This observation may partly be explained by the previously reported relationship between higher blood pressures and hypoalgesia.27 It could also reflect an unknown, underlying cause of migraine in young men with extreme blood pressures. Additional studies are needed to further elucidate the modifying effects of BMI and blood pressure on the inter-relationship between cardiovascular fitness and migraine.
Possible mechanisms
The increased risk of migraine among men with lower cardiovascular fitness at age 18 observed in this study may be explained by a combination of several factors. There might be an unknown, common predisposing factor for both lower cardiovascular fitness levels and migraine given the known, clear association of migraine with unfavourable cardiovascular risk factor profiles.28 An association between migraine and cardiovascular risk comorbidities could be explained by a common pathology underlying both conditions, and migraine might be a local manifestation of a systemic, rather than neurological, phenomenon.28 Our research findings expand on previous studies linking migraine to cardiovascular risk factor profiles, highlighting the long-term association between cardiovascular fitness and migraine.
Several areas of the brain are still developing during late adolescence, and it is also possible that cardiovascular fitness during this period has long-term effects on brain health that might reduce susceptibility to migraine. Low cardiovascular fitness has been shown to increase the risk of several other neurological and psychiatric disorders such as stroke,3 epilepsy4 and depression.29 It could be that a common mechanism affecting neuroprotection, neurogenesis, synaptic plasticity, neuroinflammation and neurotrophic factors such as brain-derived neurotrophic factor (BDNF) may be involved.30 Hence, higher cardiovascular fitness might result in a greater ‘brain reserve’ that may act as a compensatory buffer of brain plasticity and neural resources and better enable the brain to cope with neuropathology, resulting in long-lasting beneficial effects on brain health.31 Indeed, there is increasing evidence suggesting that behavioural interventions such as physical activity during critical stages of development can have such long-lasting and robust effects on the brain.31
Cardiovascular fitness may influence specific aspects of migraine burden contributing to severity. Several studies report lower migraine burden with more physical activity,32 and a recent randomised study of exercise in migraine patients showed decreased migraine pain, intensity and frequency after the training intervention.33 Neuroadaptive changes with pain are well-known,34 and decreased levels of BDNF have been reported in patients with migraine.35 Higher fitness levels during adolescence could contribute to long-lasting structural and/or biochemical changes to the brain, generating a higher threshold for migraine pain.
Strengths and limitations of this study
Strengths of this study include the population-based design, its large size and the objective measurements of cardiovascular fitness at baseline. Other strengths are available information on a large number of important covariates, the long available follow-up time and the linkage of national register data to identify conscripts who later developed migraine. Furthermore, our study focuses on men, an understudied population in migraine research.
Several limitations should, however, be considered when interpreting our results. We show that 2% of the men filled a first-time prescription of migraine-specific medication during follow-up. However, the mean prevalence of current migraine among adult men in Europe has been estimated to be 8% in a review combining studies with variable timeframes.36 Although our figures show first-time prescriptions, these should not be interpreted as equivalent to prevalence. Since our outcome measurements only capture men who seek healthcare and we are unable to identify men using over-the-counter migraine medication only, no medication at all, or preventative medications, incidence of migraine in the current study is likely underestimated. The included men classified as having the outcome likely have more severe migraine episodes, which cannot be managed by the patient himself.
Although we excluded men who died or emigrated before the Prescribed Drug Register started in 2005, we may have missed men who enlisted during the earlier years and had migraine that later resolved (or men who did not seek treatment for migraine later). Boys with an early migraine diagnosis that resolved prior to conscription might have been misclassified as having migraine at baseline and would hence be wrongfully excluded from the analyses. Although we have attempted to reduce the risk of possible reverse causation by excluding men with migraine prior to or during the 2 years after conscription, there is still a possibility that adolescent men had migraine but were not diagnosed and had not received prescribed migraine medication. Such men have been included in the current study, and this could influence cardiovascular fitness if they were less active due to their migraine.
The hospital register does not include codes from primary care; therefore, men suffering from migraine without hospital-based care could only be otherwise identified through the Prescribed Drug Register. In Sweden, migraine or cluster headache are the only indications for triptans and ergotamide (Farmaceutiska Specialiteter i Sverige (FASS); https://www.fass.se/). We have excluded men with prescribed migraine-specific medication at baseline as well as men diagnosed with cluster headache. However, there is still a small possibility that these medications could be prescribed for other indications, and these participants could be misclassified as having the outcome of interest in our analyses using the Prescribed Drug Register data. The migraine diagnosis based on ICD codes has not been formally validated in the Swedish Hospital Register. However, we have no reason to believe that the generally high positive predictive values observed for other ICD codes in this register would not also apply to migraine.
Although we have controlled for confounding by adjusting for information on several covariates, residual and unmeasurable confounding may still be present. In particular, we had no information on smoking and alcohol consumption.
Our research goal was to estimate the effect of baseline cardiovascular fitness on long-term risk of migraine. Therefore, we do not include data on cardiovascular fitness or other health-related risk factors at later stages in life. We have no information regarding changes in this variable over time. An additional limitation is that, due to the identification method of migraine used, we were not able to stratify subjects according to migraine frequency or severity, episode duration or aura status. Hence, we could not assess how cardiovascular fitness influences the risk of different subtypes of migraine. We emphasise that our findings should not be interpreted as explanatory regarding the causal chain leading to the onset of migraine.
We acknowledge the relatively large number of missing values for cardiovascular fitness exposure variable. However, since proportions with missing values were very similar among men with and without migraine-specific medication, we think it is unlikely this missingness would be differential. Since the main purpose of the Swedish Conscription Register was for military use, detailed descriptions of causes for missing data are classified, and we thus unfortunately cannot explore these reasons further. Lastly, we emphasise that since women have a different body composition, physiology, and clinical features of migraine,16 our findings should not be directly extrapolated to women.
Conclusion
Lower cardiovascular fitness in adult young men was found to be associated with increased risk of future prescription-requiring migraine. Our study calls for future targeted research to assess whether interventions to improve cardiovascular fitness result in a reduced risk of developing migraine among men with low cardiovascular fitness levels. In addition, studies that explore possible mediators of the effect of cardiovascular fitness on the later development of migraine may provide important insights into the biological understanding of migraine, ultimately informing the development of further preventive strategies.
References
Footnotes
Contributors JN, SG, ML, NDÅ, MÅ, MW and GHK conceptualised the study. JN, SG, NDÅ, MÅ, MW and GHK contributed to data acquisition. JN, SG, JLR and TK designed the analyses, and JN and SG performed the analyses. All coauthors contributed to interpretation of as well as drafting and critically revising the manuscript for important intellectual content. JN, SG and GHK are the guarantors.
Funding This work was supported by the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement (ALFGBG-726541, ALFGBG-715841), the Swedish Brain Research Foundation (Hjärnfonden), the Swedish Research Council (521-2014-3224) and the Stiftelsen Peter Erikssons minnesfond för hjärnforskning. JR’s research position is funded by a grant from the Else-Kröner-Fresenius Stiftung (GSO/EKFS-17, granted to TK).
Competing interests TK reports having contributed to an advisory board of CoLucid and a research project funded by Amgen, for which the Charité – Universitätsmedizin Berlin received an unrestricted compensation. He further reports having received honoraria from Lilly, Newsenselab, and Total for providing methodological advice, from Novartis and from Daiichi Sankyo for providing a lecture on neuroepidemiology and research methods, and from the BMJ for editorial services. The other authors have no conflicts of interest.
Patient consent for publication Not required.
Ethics approval The Ethics Committee of the University of Gothenburg and Confidentiality Clearance at Statistics Sweden approved this study (Dnr 462-14).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. All data relevant to the study are included in the article or uploaded as supplementary information.