Article Text

Abstract
Purpose The Uppsala–Stockholm Assisted Reproductive Techniques (UppStART) study is a prospectively recruited sample of couples undergoing assisted reproduction in Stockholm and Uppsala county in Sweden. The study was initiated to (1) investigate possible changes in the epigenetic profile of infants inferred through the ART procedures and their consequence and (2) to assess the impact of lifestyle and health exposures on treatment outcome.
Participants Recruitment took place between September 2011 and December 2013, and in vitro fertilisation (IVF) cycles initiated and pregnancies conceived during this time were followed until December 2014. The cohort includes 971 participants (n= 514 women; n= 457 men), and 129 pregnancies were achieved from the first IVF cycle included in the study.
Findings to date Self-reported demographic, health and lifestyle data were collected from a baseline questionnaire, and to assess changes to lifestyle, a follow-up questionnaire was issued at the time of oocyte retrieval, and at subsequent IVF cycles. Questionnaire data were linked to data extracted from medical records. Biological samples were collected at baseline: blood for extraction of serum, plasma and DNA, morning and evening saliva samples for cortisol measurement and at delivery including samples of maternal blood, placenta and amniotic fluid, and cord blood for epigenetic analysis.
Future plans Through the unique identification number assigned to each Swedish citizen at birth or immigration, UppStART study participants will be linked to the Swedish population-based national and quality registers to provide data from prenatal, obstetrical, neonatal and infant care, and subsequent updates will provide data on childhood health and educational outcomes. Collaboration and use of UppStART data is encouraged, and more information about access can be found at www.ki.se/meb/uppstart
- assisted reproductive techniques
- in vitro fertilisation
- infertility
- lifestyle
- epigenetics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The Uppsala–Stockholm Assisted Reproductive Techniques (UppStART) dataset comprises a wide range of sociodemographic and lifestyle data, clinical data from medical records, biological samples (including blood, DNA, saliva, cord blood, placenta) and epigenetic data.
Questionnaires were completed at baseline, oocyte retrieval and during subsequent in vitro fertilisation (IVF) cycles so as to be able to assess health and lifestyle changes during and between cycles.
The process of linking the participants to the Swedish national health registers has been initiated and will allow for long-term follow-up of the couples and infants.
Possible recall bias and volunteer bias are limitations, however, UppStART participants have characteristics typical of couples undergoing IVF treatment in Sweden.
Introduction
Assisted reproductive techniques (ART) include the use of hormones to downregulate pituitary function and to stimulate multiple oocyte production, in vitro manipulation of the oocyte and sperm for in vitro fertilisation (IVF) and intracytoplasmic sperm injection (ICSI) procedures, and culturing of pre-implantation embryos in culture media and incubators before the embryo is transferred to the womb. Hence, ART manipulates many steps involved in natural conception and may therefore potentially alter biological processes in the fetus, which may result in short-term and long-term health consequences on the offspring. It has been well established that ART offsprings have a higher risk of being born with a low birth weight or preterm.1 2 The reasons behind these associations are unknown, and some hypothesise that alterations in the epigenetic profile of the offspring are a contributing factor.3–6
Further, recent studies have indicated that a number of assisted reproduction procedures, including controlled ovarian stimulation, micromanipulation of gametes in addition to embryo culture, can cause epigenetic disruption.7–9
It is estimated that approximately 12%–28% of couples trying to conceive are diagnosed with infertility.10 Further, nowadays, couples and especially women prioritise educational and career goals and securing economic stability, thereby delaying childbearing.11 The use of ART is increasing in Sweden, as well as elsewhere in Europe, with up to 5% of all conceptions being a result of some form of ART in the Nordic countries.12 However, the pregnancy success rate per ART cycle is only 28%, and the take-home baby rate is barely 25%, which is not always known to the general public.13 Little is known of how lifestyle factors can affect the outcomes of ART attempts (ie, number of matured oocytes, number of embryos, pregnancy rate and miscarriage rate).
Therefore, the Uppsala–Stockholm Assisted Reproductive Techniques (UppStART) study was initiated to (1) investigate if epigenetic alterations exist in infants conceived via ART compared with those conceived spontaneously and (2) investigate if lifestyle factors (eg, caffeine consumption, cortisol levels, folate, C-reactive protein, natural products and supplements and prescribed medication use) are associated with time to pregnancy, pregnancy rates, subclinical and clinically recognised miscarriages, ART procedure-specific outcomes (eg, number and quality of oocytes and embryos, sperm characteristics), and obstetric and prenatal outcomes in ART cycles and pregnancies.
Cohort description
Study population and setting
The UppStART study is a prospective cohort study of couples undergoing infertility treatment (specifically IVF or ICSI) in the greater Stockholm and Uppsala municipalities, which provide healthcare for approximately 3 million people. Participants were recruited from three of the four fertility and reproductive health clinics in Stockholm and one clinic in Uppsala, which also serves a large volume of patients from Stockholm. In Sweden, fertility treatments are provided within the tax-funded healthcare system. Treatments are individualised based on the identified causes of infertility.
At the time of planning their first IVF/ICSI treatment, couples were approached by the clinic’s nurse or midwife and asked to participate in the study. To facilitate the process of informed consent, the couples were provided with both verbal and written information approved by the regional ethical board about the purpose of the study, methods, the voluntary nature of participation and the possible risks which included possible discomfort during blood sampling. Additionally, participants were informed that they could withdraw from the study at any time with no impact on their medical care. The requirement for inclusion in the study was an understanding of the Swedish language and exclusion was the use of donor gametes. At the time of recruitment, Swedish law did not allow single women to receive ART treatment; hence, no single women were recruited into the UppStART study. Among the couples, approximately 20% of male partners chose not to participate (n=105).
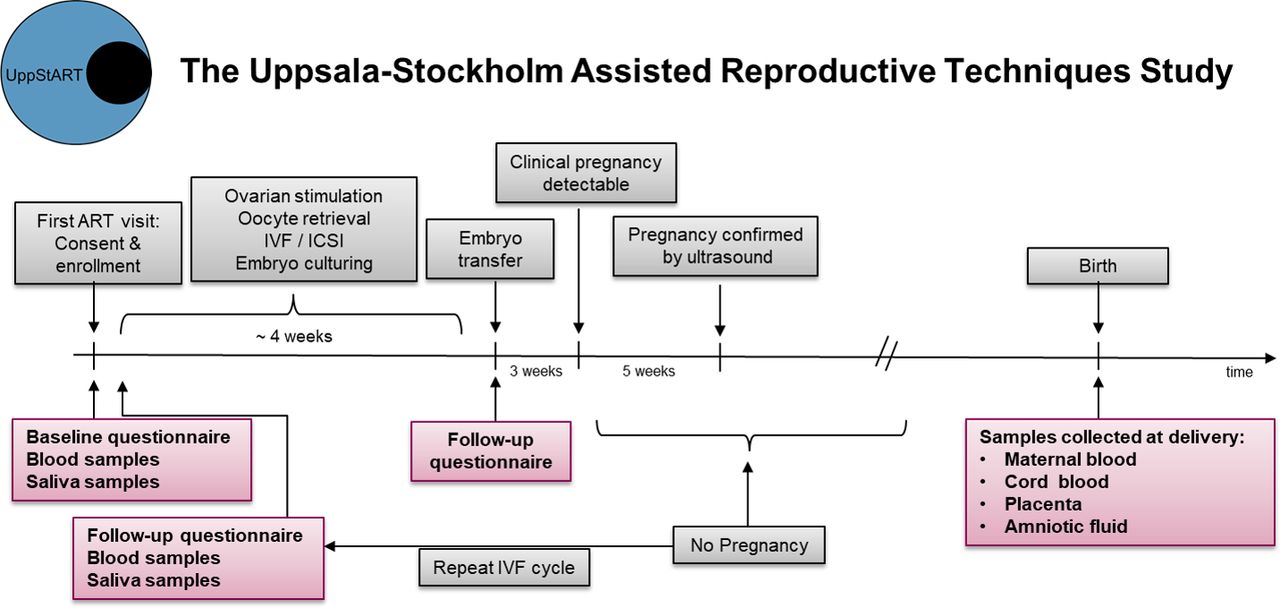
The signed consent forms were sent from the clinics to the UppStART research nurse at the host institution, the Karolinska Institute, who monitored recruitment and questionnaire responses, and reminded participants via email 2 weeks after signing the consent form to answer the baseline questionnaire if they had not done so. A second reminder by email was sent 2 weeks after the first, and if participants still had not completed the online questionnaire, the research nurse attempted to contact them by phone. No other attempts were made after the telephone call and participants were marked as non-responders. Once the ART treatment cycle began and the participants reached the stage of oocyte retrieval, they were asked to respond to a second online follow-up questionnaire (figure 1).

Timeline of participant recruitment and data collection in the Uppsala–Stockholm Assisted Reproductive Techniques study. ART, assistedreproductive techniques; ICSI, intracytoplasmic sperm injection; IVF, in vitro fertilisation.
Recruitment took place from September 2011 to December 2013. IVF treatment(s) of the participants were followed until December 2014 or drop-out/consent withdrawn (n=4), whichever came first. When the couples returned to the clinic for repeated ART attempts, clinic staff collected a blood sample, provided saliva collection tubes and instructed the participants to respond to the online follow-up questionnaire.
Figure 2 reports the number of consented participants and the number of participants who responded to baseline and follow-up questionnaires and provided samples. The cohort includes 971 participants (n=514 women; n=457 men). Eighty percent of the cycles progressed to an embryo transfer, of which 57.6% of the embryos were created via standard IVF, and 42.4% via ICSI. From the first IVF cycle included in the study, 129 pregnancies were achieved. Only pregnancies and children conceived via IVF procedures are included in this cohort.

{kind=link}
{kind=link}
Uppsala–Stockholm Assisted Reproductive Techniques study: number of participants and samples collected. IVF, in vitro fertilisation.
Table 1 shows baseline characteristics of participants and differences between responders and non-responders.
Baseline characteristics of participants in the Uppsala–Stockholm Assisted Reproductive Techniques study
Data collection and measures
Overview
Table 2 and figure 1 provide an overview of data and sample collection in the UppStART study. After informed consent was given, the clinic staff withdrew blood samples and provided the participant with a kit for at-home saliva collection. The participants were asked to answer a web-based baseline questionnaire within a few days of their clinic visit and prior to their IVF/ICSI treatment start, which included an extensive list of questions on sociodemographic, anthropometric and lifestyle factors.
Data and sample collection in the Uppsala–Stockholm Assisted Reproductive Techniques study
Questionnaires data
The baseline questionnaire asked an extensive list of questions about sociodemographic, health, and lifestyle factors in the previous 3 months or the previous year (summarised in table 3). It has been reported that couples undergoing ART change to a healthier lifestyle or try a range of ‘natural’ remedies in order to improve the outcome of their fertility treatment.14 15 Therefore, the follow-up questionnaire at oocyte retrieval and at subsequent ART procedures was a shortened version of the baseline questionnaire, designed to capture changes in lifestyle since the start of fertility treatment or since the previous cycle.
Variables included in the baseline and follow-up questionnaires in the Uppsala–Stockholm Assisted Reproductive Techniques study
Medical records
The medical records of each participant were collected from the four participating clinics and included data on all IVF/ICSI cycles initiated between the date of study entry and end of 2014. Clinical data included the medical and reproductive history of the participant, IVF/ICSI cycle protocol, indicators of oocyte and embryo quality and IVF cycle outcome including pregnancy. Box 1 summarises the available clinical data.
Summary of available clinical data for UppStART study participants
Treatment data
Ovarian stimulation procedure clinical data
Type of treatment: IVF/ICSI
Type of culture media
Number of oocytes and embryos obtained
Indicators of oocyte quality
Indicators of embryo quality
Sperm quality variables
Treatment outcome data
Urine pregnancy test results (week 2/3 after embryo transfer)
Ultrasound-confirmed pregnancy (week 7 after embryo transfer)
Miscarriage
Live birth (to be supplemented by linkage to the Swedish Medical Birth Register)
ICSI, intracytoplasmic sperm injection; IVF, in vitro fertilisation; UppStART, Uppsala–Stockholm Assisted Reproductive Techniques.
Biological samples: baseline
Blood samples
At the time of recruitment into the study, the clinic staff withdrew blood samples, which were then sent to the Karolinska Institutet (KI) Biobank. Plasma, serum and whole blood were aliquoted and stored at −80°C. DNA was extracted from whole blood and stored at −80°C.
Saliva samples
Participants were provided with two pre-labelled Salivette (Sarstedt, Leicester, UK) kits, a pre-paid envelope for the return of samples to the KI Biobank and saliva collection instructions: samples were to be collected at home at 7:00 am (on awakening, before breakfast and teeth brushing) and at 9:00 pm the same day, with no eating, drinking, gum chewing, snus use or smoking within 30 min prior to collection. Saliva samples were returned to the KI Biobank by the participant via post and the samples were stored at the KI Biobank at −80°C until analysis.
Saliva cortisol levels (nmol/L) were measured by radioimmunoassay (RIA) (Orion Diagnostic, Espoo, Finland) by the Study Center of Laboratory Medicine at the Karolinska University Laboratory. The detection limit of the RIA was <1.0 nmol/L, and the intra-assay and inter-assay coefficients of variance for this assay were 12% and 8% for the low control, and 7% and 5% for the high control, respectively.
Biological samples: at delivery
Staff at seven delivery units in Stockholm and Uppsala were recruited to assist in collecting samples from UppStART study participants during delivery. Delivery clinics were provided with a sample collection kit including tubes for collection of maternal blood (EDTA, PAX gene), cord blood (EDTA, PAX gene), amniotic fluid and placenta samples. Step-by-step instructions with pictures, to ensure consistent sampling technique, were provided to the midwives attending the delivery for sampling of one small piece of placenta (approx. 2×2 cm) from the centre of each quadrant, both on the maternal and fetal side, for a total of eight samples. Samples were stored in −20°C freezers at the delivery units until they were collected by UppStART study staff and deposited into the KI Biobank.
Linkage to national registers
Through the unique identification number assigned to each Swedish citizen at birth or immigration,16 it is possible to link our study participants to the Swedish population-based national and quality registers. While no further direct participation by the UppStART study participants is currently planned, all participants consented to their study data being linked to the national population registers for long-term follow-up of themselves and of the children they conceived while being part of the study. The process to link this cohort to the registers has been initiated and will include the Medical Birth Register, Perinatal Quality Register (for neonatal intensive care), Register of Malformations, Prescription Drug Register, Inpatient and Outpatient Registers, Cause of Death Register and the Multigeneration Register.17–19 This initial linkage will provide data from prenatal, obstetrical, neonatal and infant care, and subsequent updates will provide data on childhood health and educational outcomes.
Patient and public involvement
Throughout the study’s inception, design and execution, the Principal Investigator of the UppStART study (ANI) was herself a patient, undergoing IVF treatments. Therefore, the patient perspective was taken into account from start to end. The study was designed by ANI, in collaboration with the clinicians from the participating clinics. ANI also made regular visits to the participating clinics to discuss with clinicians about the patient reactions to the study, how they could optimise recruitment while ensuring that the delicate circumstances of the couples struggling to become pregnant were respected. Further, the questionnaires answered by the participants included a section on how they felt about answering the survey, including a free text option for them to express any concerns related to their participation in the study. These responses were monitored by ANI and the study staff as they were submitted.
Findings to date
Stress
While it is well established that women undergoing fertility treatment experience high levels of stress and higher prevalence of symptoms of depression and anxiety, it remains uncertain if and how psychological stress clinically affects the outcome of IVF treatments.20–22 The first study completed using UppStART study data investigated the association between self-reported perceived stress, infertility-related stress and cortisol levels on IVF cycle outcomes including clinical pregnancy and indicators of oocyte and embryo quality. Overall, we found that stress measured prior to IVF cycle start was not associated with IVF cycle outcome, oocyte maturity or embryo quality. The findings from this study and many other studies reporting no association between stress and IVF outcomes are potentially reassuring to women undergoing fertility treatment and the clinicians who may have concerns about the influence of stress levels on the success of their IVF treatment.23
Cumulative impact of lifestyle factors on IVF treatment outcomes
The UppStART study has been used as a validation cohort in a study examining the cumulative impact of lifestyle factors on IVF treatment outcomes. An individual as well as a cumulative effect of smoking and BMI on the number of aspirated and mature oocytes in fresh IVF treatment cycles has been found, especially among women with low ovarian reserve.24
Epigenetics
In collaboration with researchers at Leiden University, the methylation profile of the cord blood of UppStART study offspring has been measured and compared with the methylation profile in the cord blood of spontaneously conceived offspring from the Swedish Born Into Life study. Details on the Born into Life study are described at length in Smew et al.25 The UppStART study and the Born into Life study were run in parallel from the same department, with the protocols for sample collection coordinated. Genome-wide DNA methylation data were generated using the Illumina Infinium Human Methylation 450K BeadChip (450 k array). A total of 500 ng of genomic DNA isolated from cord blood was bisulfite treated using the EZ-96 DNA methylation kit (Zymo Research, Orange, California, USA). The first aim was to identify potential differences in epigenetic marks between IVF and spontaneously conceived offsprings. Further, comparisons between methylation profiles from infants conceived via different ARTs will be conducted, such as between IVF and ICSI, fresh and frozen embryos and Day 2 and blastocyst embryo transfer. The study results are currently being written up for submission for publication.
Further, while not considered in this study, the plethora of exposure information gathered from the questionnaires also provides unique possibilities to explore gene–environment interactions in the epigenetic analyses and the impact of specific environmental exposures on epigenetic marks.
Strengths and limitations
The major strength of the UppStART study is the plethora of information from multiple sources, including an extensive questionnaire on a large number of lifestyle factors and behaviours, data from medical records, national registers, as well as biological specimens. Further, studies often only include women undergoing ART, however, the UppStART study has collected data on the male partners as well. Additionally, the study has captured repeated ART cycles within the couple and monitored the change in lifestyle factors between cycles to determine if these changes are linked to ART outcomes of interest.
However, there are also some limitations and potential sources of bias. Recruitment of participants was slower than expected, especially at the beginning of the study for a number of reasons: one of the four IVF clinics in Stockholm declined to participate and one clinic halted recruitment for 8 months due to staff restructuring. To encourage the involvement of clinic staff, study personnel visited with clinic staff every 6 months and distributed a newsletter reporting recruitment statistics for each clinic. Additionally, during the last year of recruitment, ethical approval was granted to give participating couples movie tickets on enrollment, thereby providing a small compensation for their participation. While the goal of the study was to capture every treatment of the couples, the clinics often missed collecting blood samples and reminding the participants to complete the questionnaires at subsequent cycles. Lastly, due to the urgent and demanding nature of the labour and delivery units, the collection of samples at delivery of some infants was missed. Midwives expressed that often there was not enough time to collect the number of samples requested while also fulfilling their clinical duties.
With any study including self-reported health and lifestyle information, such as this one, recall bias is an issue. The majority of the questions in the UppStART baseline questionnaire targeted specific lifestyle factors during the previous 3 months to a year. However, women and men experiencing infertility and planning to undergo infertility treatment often make changes in their lifestyle based on what they believe will maximise the chances of conception,14 which will likely make the participants more aware of their lifestyle choices and consequently be able to respond to the questionnaire more accurately.
Further, volunteer bias may be another source of bias in the cohort. The UppStART study was presented to participants as a general study of lifestyle factors in IVF couples. Therefore, individuals with an interest in their lifestyle choices may choose to participate, and those with unfavourable lifestyle habits may have declined. However, the characteristics of the UppStART study are typical of the Swedish population undergoing IVF,26 and a large degree of homogeneity exists in the demographic and lifestyle, including low rates of factors known to affect fertility and IVF outcome (eg, high BMI and smoking). As with the known variables, we speculate that the study sample is also likely to be relatively homogeneous with respect to unmeasured variables which will reduce the influence of confounders on studies performed with data from this cohort.
Collaboration
We encourage the use of UppStART study data as a resource for epidemiological research. The data are available upon request, and more information can be found on the UppStART study webpage (www.ki.se/meb/UppStART). To access the data, a proposal should be submitted to the principal investigators by an applicant with a PhD or an equivalent degree. Proposals will be evaluated and granted according to principles of ethical and scientific soundness. Applicants based outside of Sweden are required to involve collaborator(s) based at a Swedish research institution. Applications can only be granted and data provided after approval by the Stockholm Ethical Review Board. Information and instructions for applicants are available on the website (https://ki.se/meb/uppstart) and from Carolyn Cesta at carolyn.cesta@ki.se.
Acknowledgments
The authors would like to thank the participants of the UppStART study and the clinic staff at the participating clinics: Carl von Linné Clinic, Uppsala; Department of Reproductive Medicine, Karolinska University Hospital; Livio Fertilitetscentrum Gärdet (previously Fertilitetscentrum Stockholm) and Livio Fertilitetscentrum Kungsholmen (previously IVF-kliniken Stockholm, S:t Görans Sjukhus), Stockholm. We thank Bozenna Iliadou, Mariam Lashkariani and Mikael Bröms for assistance with the database management.
References
Footnotes
Contributors ANI, JP, SC, KAR-W, JIO, JH, HW, MW, and ASÖ were responsible for the study design, protocol development and data collection. CEC was responsible for the data analysis and writing the initial draft of the manuscript. Subsequent drafts were reviewed by all authors listed. All authors had input on reporting of the findings. All authors provided approval for the submitted version of this manuscript.
Funding The UppStART study was funded by the EU-FP7 Health program (IDEAL, agreement 259679), the Swedish Research Council (K2011-69X-21871-01-6 and SIMSAM 340-2013-5867) and the Strategic Research Program in Epidemiology Young Scholar Awards, Karolinska Institutet.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The UppStART study has been approved by the regional ethics review board at Karolinska Institutet (Dnr 2011/230-31/1, 2011/1427-32, 2012/131-32, 2012/792-32, 2013/1700-32, 2014/1956-32, 2015/1604-32).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.