Article Text

Abstract
Background Pregnancy is an opportunity for health providers to support women to stop smoking.
Objectives Identify the pooled prevalence for health providers in providing components of smoking cessation care to women who smoke during pregnancy.
Design A systematic review synthesising original articles that reported on (1) prevalence of health providers’ performing the 5As (‘Ask’, ‘Advise’, ‘Assess’, ‘Assist’, ‘Arrange’), prescribing nicotine replacement therapy (NRT) and (2) factors associated with smoking cessation care.
Data sources MEDLINE, EMBASE, CINAHL and PsycINFO databases searched using ‘smoking’, ‘pregnancy’ and ‘health provider practices’.
Eligibility criteria for selecting studies Studies included any design except interventions (self-report, audit, observed consultations and women’s reports), in English, with no date restriction, up to June 2017.
Participants Health providers of any profession.
Data extraction, appraisal and analysis Data were extracted, then appraised with the Hawker tool. Meta-analyses pooled percentages for performing each of the 5As and prescribing NRT, using, for example, ‘often/always’ and ‘always/all’. Meta-regressions were performed of 5As for ‘often/always’.
Results Of 3933 papers, 54 were included (n=29 225 participants): 33 for meta-analysis. Health providers included general practitioners, obstetricians, midwives and others from 10 countries. Pooled percentages of studies reporting practices ‘often/always’ were: ‘Ask’ (n=9) 91.6% (95% CI 88.2% to 95%); ‘Advise’ (n=7) 90% (95% CI 72.5% to 99.3%), ‘Assess’ (n=3) 79.2% (95% CI 76.5% to 81.8%), ‘Assist (cessation support)’ (n=5) 59.1% (95% CI 56% to 62.2%), ‘Arrange (referral)’ (n=6) 33.3% (95% CI 20.4% to 46.2%) and ‘prescribing NRT’ (n=6) 25.4% (95% CI 12.8% to 38%). Heterogeneity (I2) was 95.9%–99.1%. Meta-regressions for ‘Arrange’ were significant for year (p=0.013) and country (p=0.037).
Conclusions Health providers ‘Ask’, ‘Advise’ and ‘Assess’ most pregnant women about smoking. ‘Assist’, ‘Arrange’ and ‘prescribing NRT’ are reported at lower rates: strategies to improve these should be considered.
PROSPERO registration number CRD42015029989.
- smoking
- healthcare providers
- smoking cessation
- maternal health
- pregnancy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Comprehensive meta-analysis and meta-regression of health providers implementation of the ‘Ask’, ‘Advise’, ‘Assess’, ‘Assist’, ‘Arrange’ combining like measures for smoking cessation care.
Fifty-four studies from seven high-income and three low-to-middle-income countries include disciplines of medicine, nursing and allied health.
High heterogeneity in the meta-analyses was unexplained by the meta-regressions, except for ‘Arrange referral-often/always’ which was related to year and country.
Quality ratings of some papers were poor—findings from these studies may be less reliable.
Review aids in determining which components of smoking cessation care are less reliably implemented in pregnancy.
Introduction
Smoking during pregnancy carries high risks for mother and child, including obstetric complications for the mother,1 and for the baby, premature birth, growth restriction, low birth weight, stillbirth and congenital defects.1 2 Longer term effects on the child include respiratory illnesses, learning and behavioural problems, and increased risks of chronic diseases,1 2 and of taking up smoking in adolescence.3
Smoking during pregnancy remains a prevalent behaviour in many countries, with estimated smoking prevalence rates ranging from 0.2% to 38.4%.4 Pregnancy is a time when women are more likely to be motivated to stop smoking.5 However, disadvantaged women, including women from minority and indigenous populations where there is a high prevalence of community smoking, also smoke at higher rates and are less likely to try to stop smoking, or succeed than more advantaged women among whom smoking prevalence is lower.6 7 Also, less likely to stop smoking are women who are: of low socioeconomic status,6 multiparous,6 adolescents,8 partnered by smokers,6 and those experiencing: alcohol or substance use,8 depression,9 life stressors10 11 or intimate partner violence.12 Women frequently reduce tobacco consumption when discovering they are pregnant,11 13 indicating a consciousness about the risks, but may be less likely to abstain than non-pregnant women.14 Pregnant women report a lack of support for smoking cessation, and that health providers (HPs) consider cutting down to be acceptable.15 16
HPs in primary care have a critical role to offer advice and support women to stop smoking during pregnancy.17 Ideally smoking cessation care (SCC) includes counselling and pharmacotherapy—most successful when combined.17 18 In pregnancy, the effective use of pharmacotherapy is less certain, and clinical guidelines vary across and within different countries.17 In pregnancy, only nicotine replacement therapy (NRT) is recommended, but not consistently advised for use in pregnancy in all countries,17 19 for example, NRT is not advised in the USA for use in pregnancy,20 but it is more routinely prescribed in the UK.21 Clinical guidelines in the UK, Australia, New Zealand (NZ) and Canada recommend that a woman should initially endeavour to quit without medication, but if she cannot, NRT can be prescribed.17 22–25
The 5As (‘Ask (about smoking)’, ‘Advise (to quit)’, ‘Assess (motivation and/or dependence)’, ‘Assist (with cessation)’ and ‘Arrange (follow-up or referral)’) has been adopted in many countries as a strategy for HPs to deliver all the important components of SCC.26 Several studies have examined the performance of the 5As in pregnancy. Two reviews summarised the literature . Okoli et al’s integrative review reported on HP performance of components of the 5As. While authors reported more than 50% of HPs ask and advise about smoking, and less than 50% Assess,Assist or Arrange (referral or follow-up), it is unclear how these estimates were calculated. This is an important limitation considering the variable ways studies collect data and report them.27 Baxter et al’s qualitative systematic review, on the factors that influenced uptake of interventions by pregnant women, included studies on HP and women’s reports of their receipt of SCC, and noted variation between HPs for recording smoking status and advice.28 As neither review included a meta-analysis, it is timely and important from the point of view of rigour to have a definitive evaluation of HP practices, and furthermore to accurately inform recommendations to guide strategies to improve SCC. An urgent need for research to increase the uptake of smoking cessation interventions, and improve quit rates in pregnant women who smoke has been identified by Siddiqi and Mdege.29
The objective of this systematic review was to summarise published empirical research of eligible studies from a range of HPs who consult with pregnant women who smoke, and synthesise findings with meta-analyses where feasible. The primary aim was to determine the prevalence of the components of SCC that were being practised, including the 5As, prescribing NRT and related behavioural change techniques (BCTs—observable and replicable components designed to change behaviour),30 thus determine which aspects of SCC need improvement. A second aim was to examine which factors were associated with delivery of the 5As, and NRT prescribing, that is, HP types, country, year and pregnant women in high-risk populations. We also examined data about knowledge and attitudes of the HPs to inform their practices.
Methods
Data were identified by searches of MEDLINE, EMBASE, CINAHL and PsycINFO, and reference lists from relevant articles. Where possible, search terms were matched to MeSH or database specific subject headings, and used as keywords. Search terms included (see online supplementary table 1): pregnancy (eg, perinatal care, mother), smoking (eg, nicotine dependence, smoking cessation), health professional (eg, general practitioner (GP), midwife) and attitudes or practices (eg, capacity, belief). Searches were performed in September 2015; additional studies included until June 2017.
Supplemental material
Inclusion criteria: peer-reviewed full papers on SCC to pregnant smokers by any HP in any setting, restricted to English language, with no date restrictions. Quantitative studies and/or quantitative data from mixed-methods studies with any study design were included, comprising self-reported provision of SCC by HPs, reported receipt of SCC by pregnant women, or other indicators, for example, chart audit or audio recordings of consultations. For this review, SCC was based on the 5As: asking about smoking, advising about quitting, assessing motivation to stop smoking or nicotine dependence, assisting to quit and arranging follow-up or referral.26 In addition, we included papers reporting HP knowledge, attitudes and other practices, for example, advising about relapse and smoke-free homes, discussing psychosocial contexts of smoking, involving family members or partners, prescribing NRT and other BCTs (eg, setting a quit date, making a quit plan, providing resources and self-help materials, aiding social support, encouraging smoke-free environments and monitoring carbon monoxide readings).31 32 Exclusion criteria: intervention studies and studies in non-peer-reviewed literature; studies on preconceptual and postnatal care. Additionally, 10 papers that did not have a main focus on the review topic and/or reported minimal data about the topic such as one line or one data item in a full paper were excluded (list available from authors on request). We used the MOOSE checklist when writing our report.33
Two researchers (LT—behavioural scientist, YBZ—physician) independently screened titles, abstracts, and then full papers and applied the inclusion criteria to determine eligibility. Discrepancies were resolved by consensus, with a third researcher (GSG) acting as adjudicator, when agreement was not reached. Studies that met all criteria were retained for full review. One researcher completed data extraction (LS) with a second (YBZ) extracting 20% of articles, then results compared. A summary table (see online supplementary table 2) was developed from this data (GRG and GSG). The characteristics of each study were examined including aims, setting, country, sample characteristics, study focus (HP or women), HP type, study design and method, measures, extracted results for each of the 5As, prescription of NRT, and whether the study addressed the provision of BCTs, and if so a description of the BCTs (eg, setting a quit date, increasing self-efficacy, monitoring carbon monoxide reading, validating abstinence).
As the studies overall were of all types of design, a quality assessment of the quantitative and mixed studies was carried out using Hawker et al’s tool for reviewing disparate data systematically.34 This was chosen in the absence on any consensus on the best tool, as we were including quantitative and mixed-method studies in the review. LS rated all studies using the tool (20% double rated by YBZ). Studies were included irrespective of quality.
Quantitative data were presented as percentages and counts were possible, and meta-analyses made for estimates of each of the 5As of SCC provision and prescribing NRT. A narrative analysis summarises other studies or outcomes, including BCTs where reported. For each outcome measure, we looked at the specific measurements across studies to determine whether it was clinically appropriate to group them together, that is, Ask, Advise, Assess (motivation to quit, nicotine dependence), assist (cessation support, quit date, quit plan, prescribe NRT), Arrange (follow up, referral). To achieve this, we considered both the data collection method (cross-sectional survey; audit of patients’ medical records; audio recording of consultation; women’s report through survey or interview) and the measure itself that was used (eg, Likert scale or a dichotomous yes/no response and so forth). General principles applied were as followed (explained in more detail in online supplementary text 1):
‘Often/always’ included survey measures reflecting asking ‘often’ and ‘always’, ‘usually and always’; and/or ‘most of the time’ and ‘all of the time’). The combined answers in Likert scales were dichotomised for analysis.
‘Always/all’ included in this analysis was the proportion of HPs answering ‘always’ or ‘all of the time’, if a Likert scale was used, or the proportion answering ‘yes’ if a dichotomous question was used: either asking ‘do you ask all of your patients?’ or ‘do you ask your patients always?’ Answers reporting on ‘Asking’ more than 75% of their patients were considered as ‘yes’ for these analyses.
‘Yes’ where a survey asked the HP a dichotomous question, for example, ‘do you advise? Yes/no’ were grouped separately as ‘advise—yes’.
Papers describing women’s reports were analysed separately from those describing HP reports.
All statistical analyses were programmed using Stata V.13.1 (StataCorp LP). Meta-analyses were performed to examine the performance of each of the 5As, including prescribing NRT, as above. Stata program Metaprop was used to pool dichotomised responses for each of the 5As. If more than five studies were pooled, random-effects modelling (DerSimonian and Laird’s method) was used to account for differences in underlying estimates due to study population and design; heterogeneity (I2) was measured for each reporting type. If the number of studies was low (≤5), fixed-effects modelling was used as the between-studies variance (τ2), and therefore, the mean of the underlying random distribution cannot be estimated with precision; heterogeneity is not presented.35 Where required, in order to include studies where the per cent reporting the outcome was 100%, the Freeman-Tukey Double Arcsine Transformation method was used to stabilise the variances prior to pooling. Pooled estimates for study outcomes were split by response, and also by HP type. Significance was set as α=0.05 a priori.
For the ‘often/always’ responses to Ask, Advise, Assist, Arrange, including prescribing NRT, meta-regression (Stata program Metareg) was used to examine whether some of the heterogeneity seen in the proportions reported for each study could be explained by HP type (eg, midwife, GPs, obstetricians (OBS) or mixed groups of HPs), high-risk population versus not (eg, women in low socioeconomic groups, indigenous women or with mental health diagnoses), country (USA, Europe, Australia/NZ or other) or year of publication (1990–2017). P value, changes in heterogeneity (I2 residual), changes in between study variance (τ2) and proportion of between-study variance explained by predictor (adjusted R2) were reported. For year, the linearity of proportion over time was examined, and if a non-linear trend was seen then the meta-regression was not performed. Meta-regressions for the other meta-analyses were not performed.
An analysis of agreement of quality-rating coders was performed. Weighted kappa (ordinal multirater—quadratic weighted Kappa) was used to compare the rating of 9 quality study criteria for 15 studies; each criterion was scored on a 5-point scale (very poor, poor, fair, good and very good). Mean (SD) ratings were calculated for each criterion for each rater. Kappa and weighted kappa estimates were interpreted using cut-off criteria specified by Altman.36 Strength of agreement was <0.20 poor; 0.21–0.40 fair; 0.41–0.60 moderate; 0.61–0.80 good; 0.81–1.00 very good.
Patient and public involvement
As a systematic review, we did not directly involve any patients or public in the study. However, the review was informed by patient and HP needs. Participants from previous studies reported to us that they were not receiving comprehensive SCC during pregnancy from their HPs,16 nor were HPs in a previous study reporting they delivered comprehensive SCC.37 This review was responsive to global knowledge about the receipt and delivery of SCC in pregnancy being a gap in the literature.
Results
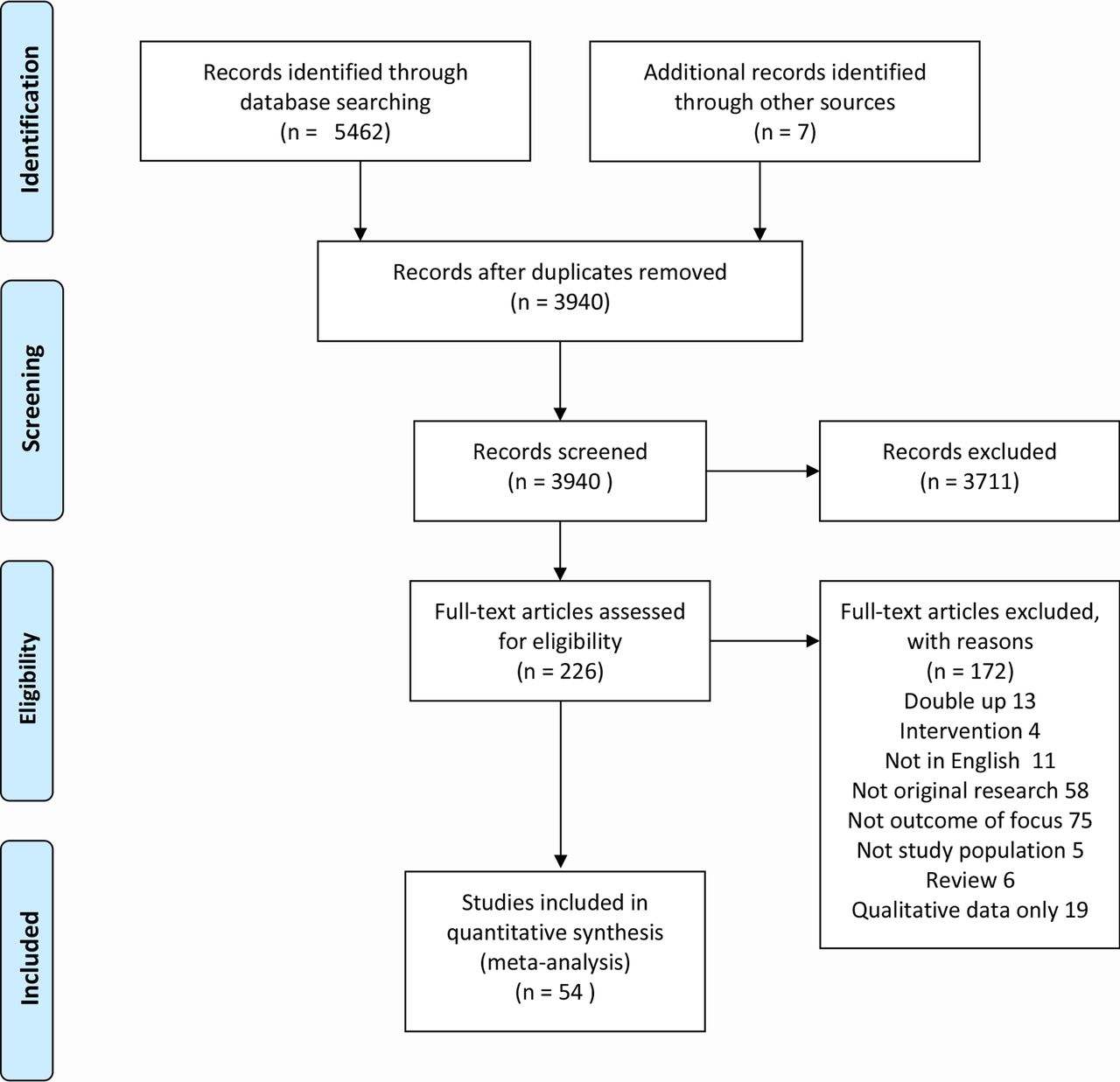
Of the 3933 studies found, 54 papers met the inclusion criteria for quantitative review. See Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart for included studies (figure 1).

PRISMA flow chart of included studies.98
A total of 54 studies were included in this analysis.37–90 Study details, including author, country, study focus (HP, women or both), population and risk category (high/low), study aims, inclusion of 5As and summary of results, are presented in online supplementary table 2. Of these studies, approximately 90% were quantitative (n=49),37–43 45 48–64 66–75 77–90 and approximately 10% (n=5) used mixed methods, containing both quantitative and qualitative aspects.44 46 47 65 76 The included studies used the following study methods: survey (n=48),37–45 48–62 64–67 69–81 84–90 audio recordings (n=2),46 47 audit (n=2),82 83 audit with interview (n=1)63 and observational (n=1).68
Study location included seven high-income countries (USA,38 45 49 54 57–59 61 65 71 78 79 86 UK,44 48 52 60 74 Australia,37 51 75 76 87 90 Germany,81 84 Switzerland,66 NZ,55 56 80 France,46 and three low-to-middle-income countries (Jordan, Argentina and Uruguay).28 32 59
Included studies focused on either HPs (n=39, 72%),37–39 41 43 44 47–55 57–61 65 66 68–73 75 78–81 83 84 87–90 pregnant women (n=12, 22%)40 42 45 56 62 63 67 74 76 82 85 86 or both HPs and pregnant women (n=3, 6%).46 64 77 Studies encompassing HPs included obstetricians and gynaecologists (OBS) (n=9, 21%),39 49 53 54 57 65 71 73 79 midwives (n=7, 17%),38 41 51 52 64 72 84 GPs (n=3, 7%),60 61 68 multiple professions (eg, OBS, GPs, nurses, healthcare assistants; n=21, 50%),37 43 44 46–48 50 55 58 59 66 69 70 75 77 79–81 87 89 90 or did not report the profession (n=1, 2%).83
Out of the 54 papers, information on 5As, ie, Ask, Advise, Assess, Assist and Arrange (follow-up/referral) was reported by approximately 68%, 70%, 28%, 63% and 54% of studies, respectively. Few studies addressed all of the 5As combined (n=12, 22%). These reported that HPs rarely addressed all of the 5As, for example, only 19.6% of respondents in Zeev et al’s study of GPs and OBS performed all of the 5As ‘often/always’.37
Only four studies (7%) addressed the provision of other BCTs in pregnancy. In one study, 31% of OBS advised women to set a quit date39; in a second study 29% of midwives suggesting quitting with an acquaintance52; 97% of women in a third sample reported they had not had their exhaled carbon monoxide tested,56 and a fourth study reported which of the clinics used open-ended questions and problem solving.89 Additionally, some studies (n=12, 22%) obtained information on or addressed a woman’s psychosocial context for smoking, for example, family or partner’s smoking status or involvement in quitting, a woman’s social support or her living environment, for example, a smoke-free home or vehicle (n=3, 6%). Information regarding the use of resources was addressed in 20 studies (37%), that is, providing pamphlets or recommending an online programme. Advice about relapse was rarely addressed in the included literature (n=3, 6%); for example, in one of the studies midwives reported they discussed with women how to avoid relapse.52
Twenty-nine of the 54 papers addressed NRT in some capacity. These included knowledge and training, attitudes to NRT and prescribing of NRT. Papers addressing knowledge, attitudes and training in general (n=14, 26%) also reported on HP knowledge about whether NRT can be used in pregnancy, and HP confidence about their smoking cessation knowledge, awareness of smoking cessation guidelines, knowledge about the consequences of smoking for expectant mothers and risks to their baby. The majority of HPs believed maternal smoking to be harmful to the fetus and/or the woman, with reports ranging from 90% to 100%. General knowledge about smoking in pregnancy varied (eg, in Bonollo et al 43 only 44%–52% of US HPs of various types, had correct knowledge). In Mejia et al’s study, 75% of Argentinan physicians believed that it was safe to smoke up to six cigarettes when pregnant.69
In addition, the above group of studies included aspects of smoking cessation training (ie, whether training had been offered, engaged in and if more training was needed). In general, HPs reported that they had received limited training on SCC in pregnancy, and identified that they required more training.
Papers including information on NRT prescribing (n=14, 26%) reported on the frequency of considering to prescribe NRT, the frequency of recommendation of NRT, frequency of prescribing NRT, percentage of NRT scripts filled by women, percentage following Food and Drug Administration (FDA) NRT prescription recommendations and the different NRT types prescribed (eg, patches, gum or inhalators). Overall findings suggested that HPs more often than not chose to not prescribe NRT to pregnant women who smoke, this was also supported by the meta-analysis below.
Attitudes and knowledge were associated with HP practices. In one Australian study, higher levels of knowledge about NRT were associated with greater likelihood of assessing women’s smoking status.75 In another US study, OBS who perceived NRT as safe to use in pregnancy were 20 times more likely to prescribe NRT.78 An Australian study determined that HP optimism, and confidence in counselling and/or prescribing NRT, and having sufficient time and resources were associated with a higher performance of all the 5As.37
Thirty-three studies were suitable for meta-analysis.38 39 42 44 45 48 49 51 52 54–58 60 61 65 66 69 71 74–76 78 80 81 84 87 90 91 Seventeen meta-analyses were performed and associated forest plots constructed (see online supplementary figures 1–17). Figure 2 provides a visual comparison for pooled percentages of selected categories of ‘often/always’.

{kind=link}
{kind=link}
Comparison of pooled percentages of selected categories of ‘often/always’. NRT, nicotine replacement therapy.
Overall the performance of ‘Ask—often/always’ (n=9) was 91.6% (95% CI 88.2% to 95%). Percentages for ‘Ask—‘always/all’ (n=11) was similar at 91.5% (95% CI 85% to 96.3%). Percentages for ‘Ask—yes’ (n=4, all by women’s report) was slightly higher at 93.6% (95% CI 92.6% to 94.6%).
The performance of ‘Advise—often/always’ (n=7) was 90% overall (95% CI 72.5% to 99.3%). Percentages for ‘Advise—always/all’ (n=6) was 86.4% overall (95% CI 79.6% to 93.3%). Percentages for ‘Advise—yes’ (HP report) (n=4) was much lower at 58.1% overall (95% CI 55.9% to 60.4%). Percentages for ‘Advise—women’s report yes’ (n=4) was similar at 53.6% overall (95% CI 52.6% to 54.6%). Percentages for ‘Assess motivation to quit – often/always’ (n=3) was 79.2% overall (95% CI 76.5% to 81.8%).
Overall 34 manuscripts included a question about assisting. Some were generally asked about assisting the patient to quit, others specified a method of assisting such as counselling, setting a quit date, making a quit plan and prescribing NRT. Those in the meta-analysis were as follows: ‘Assist cessation support—often/always’ (n=5) was 59.1% (95% CI 56% to 62.2%); ‘Assist counselling—yes’ (n=5) was higher at 80.7% (95% CI 79% to 82.5%); ‘Assist quit plan—often/always’ (n=2) was 57.6% (95% CI 54.1% to 61.1%); ‘Assist quit date—often/always’ (n=3) was low at 29% (95% CI 25.3% to 32.7%); ‘Assist—women’s report yes’ (n=4) was the lowest at 26.8% (95% CI 25.3% to 28.3%). The performance of ‘Arrange referral—often/always’ (n=6) was 33.3% overall (95% CI 20.4% to 46.2%). There were no analysable data on women’s report for ‘Arrange’.
‘Prescribing NRT—yes’ was 25.4% (n=6) overall (95% CI 12.8% to 38%). ‘Prescribing NRT—often/always’ (n=4), however, was very low at 12.8% overall (95% CI 10.7% to 15%). The performance of ‘Prescribing NRT—always’ (n=4) was the lowest at 6.2% overall (95% CI 4.9% to 7.4%). There were no analysable data on women’s report of having been prescribed NRT. All of the studies in the meta-analysis for ‘Prescribing NRT—yes’ were from the USA (see online supplementary figure 17).
High heterogeneity (I2=95.9%–99.1%) was seen for: ‘Ask—often/always’; ‘Ask—always’; ‘Advise—often/always’; ‘NRT prescription’; ‘Arrange referral—often/always’; thus indicating considerable diversity in study outcomes, methodology or populations. A fixed-effects model was used for the following outcomes due to low number of studies, and heterogeneity was not measured: ‘Ask—women’s report yes’; ‘Advise—yes’; ‘Assess motivation to quit—often/always’; all the ‘Assist’ categories; ‘NRT Prescription—always’, ‘NRT Prescription—often/always’.
Table 1 displays the results of the meta-regression of the ‘often/always’ categories of ‘Ask’, ‘Advise’, ‘Arrange’ and ‘Prescribing NRT’ from the meta-analysis. ‘Assist’ only had five studies, so the meta-regression was not performed. For nearly all of the measures, none of the predictors examined significantly explained the heterogeneity of the proportions for the studies. For ‘Arrange referral—often/always’, country was found to explain some of the differences in proportion of HPs providing this type of SCC; with Australian and NZ studies having significantly higher proportions of HPs reporting ‘Arrange referral—often/always’ than US studies (on average). Year was also found to explain some of the differences in proportion with later years having higher proportions of HP reporting this ‘Arrange referral—often or always’ (on average).
Meta-regression analysis of HP practices performed ‘often/always’
Table 2 shows the quality rating with the Hawker et al tool,34 for included studies. Over 70% of the studies had some aspects at least that were rated as good, and 20 out of 53 (37.7%) studies that were rated had at least 5 ‘good’ categories out of the 9 available options. Common flaws were lack of clarity about aims, sampling processes not detailed, ethics processes not described, and no suggestions made for further research.
Quality assessment of 54 included studies
Table 3 shows the quality ratings of the studies, and level of agreement from using the Hawker tool,34 for the 15 papers that were rated independently by two raters. Coder agreement varied from poor for two criteria, fair for four of the criteria and moderate for three criteria.
Findings from agreement of quality rating analysis of coders using the Hawker tool
Discussion
This systematic review of 54 studies from 10 countries on a range of HPs who consult with pregnant women who smoke. Thirty-three studies were suitable for meta-analyses for at least one outcome measure. Studies displayed considerable variation in the way they assessed HP provision of each of the 5As. Commonly surveys employed Likert scales that were recategorised as ‘often or always’ or questions forcing a ‘yes/no’ option. We pragmatically transformed outcome measures so they could be combined for meta-analysis, over the 5As and their subcategories, resulting in small numbers of studies in each forest plot, which means that interpretations should be cautious. We acknowledge that there was no ideal way to combine these measures. Conceptually, using a scale to quantify responses is quite different from a ‘yes’ option: the latter may be an option chosen by respondent whether they perform the practice at an frequency from occasionally to always (ie, not at all quantified)—therefore we did not combine ‘often/always’ with ‘yes/no’ study measures.
The primary aim to determine the prevalence of the components of SCC that were being practised by a range of HPs. The review demonstrated several aspects of SCC that could be improved for pregnant women, including those seen in primary care settings. The highest rates were for Ask and Advise and Assess. Assist and Arrange were consistently lower. Our secondary aim to examine whether SCC differed between different HP types, for pregnant women in high-risk populations, by country, and by year was achieved by meta-regressions of studies reporting practices ‘often/always’. Only ‘Arrange referral’ had a significant result, indicating that year and country could explain some of the heterogeneity, and perhaps indicating an increased awareness of referral options in later years, or in Australia and NZ. The 21 studies not included in the meta-analysis revealed few comparable quantitative studies on HP knowledge, attitudes and the lesser reported practices of BCTs, and the implementation of all components of the 5As together. On the whole HP knowledge base might be insufficient about NRT. Poor understanding about the safety or efficacy of NRT in pregnancy compared with continued smoking may lead to underprescribing of NRT as a stop smoking aid, however, this is likely to be context sensitive as not all countries recommend the use of NRT and clinical guidelines vary across time and even within the same country.17 However, all of the studies in the meta-analysis of NRT were from the USA, and considerable variation for prescribing NRT is seen within that one country. Access to HP training for SCC was reported as being limited, and HPs indicated they required more training.
The strength of this study is that, as far as we are aware, it is the broadest and most rigorous systematic review of HP performance of the 5As in pregnancy, including seven high-income and three low-to-middle-income countries and the only review, to our knowledge, to perform a meta-analysis and meta-regression. We took care to combine outcome measures with like measures, for each of the 5As, wherever possible. Multiple meta-analyses were performed, for each combined measure. The high heterogeneity suggests a cautious interpretation of the results. The review was limited by not being able to determine the cause for the high heterogeneity in the meta-analyses by our meta-regression, except for ‘Arrange referral-often/always’ which was related to year and country. We recognise that differing clinical guidelines may have impacted the provision of NRT in pregnancy in some countries. In particular, NRT is not recommended for pregnancy in the USA. Additionally, while most countries do use the 5As, there are variations, such as ABC (Ask, Brief Advice, Cessation) in NZ and Ask, Advise, Action in the UK. These have in common the first 2As, and then a variation to shorten the mnemonic or practice. This variation may be a limitation to this study. The review was also limited by publications only being included up to June 2017.
Where the number of studies was low (≤5), fixed-effects modelling was used because the between-studies variance (τ2), and therefore, the mean of the underlying random distribution cannot be estimated with precision; heterogeneity is also not presented in these cases. We suggest that these results are interpreted with caution, and consideration be given to the degree of overlap in the study specific CIs. The quality rating revealed aspects of some papers were poor; findings from these studies may be less reliable. However, unresolved discrepancies between the raters indicate a circumspect interpretation.
Two other reviews examined the provision by HP of SCC for pregnant women. Okoli et al’s non-systematic review included 28 studies from 6 high-income countries (USA, Australia, UK, Germany, Canada and the Netherlands).27 The review reported that few HPs working with pregnant women use all the components of the 5As. Although more than 50% of HPs in the review asked women about their smoking status and advised pregnant smokers to quit, fewer than 50% assessed motivation, assisted smoking cessation, or arranged follow-up or referrals. Our review highlighted the diversity of the ways different studies surveyed HPs about their use of the 5As, but it is unclear from the Okoli review how these estimates were made. Instead a range was reported for each of the 5As, (eg, ‘Ask’ 73%–100%; ‘Assess’ readiness or willingness to make a quit attempt 42%–81%) without the reader being able to determine which studies used Likert scales, if measures were recategorised, or a dichotomous yes/no employed. Baxter et al’s systematic review included 23 papers from 6 high-income countries, 1 middle-income country (UK, France, Sweden, USA, Australia, NZ, South Africa) and one multination study, in a qualitative synthesis.28 Similarly, although Baxter’s review reports percentages of HP or women giving or receiving different aspects of the 5As, they do not describe how these questions were asked.28
The low rates of reported implementation of components of the 5As may be related to barriers at several levels. Okoli et al’s review suggests several important provider-specific, patient-specific and system or organisational barriers hindering the provision of SCC by HP.27 Provider-specific barriers centred around HP self-efficacy or perceived ability to provide SCC to pregnant smokers, namely low knowledge, low confidence for counselling and use of NRT, the perception that as HPs they could not influence the patient’s smoking behaviour, or that SCC was not their role. In the studies in our review, HP practices also related to HP knowledge and attitudes (optimism and confidence). Patient-level barriers included HP perceptions that pregnant smokers were not interested in quitting, had stressful lives, and HPs not wanting to jeopardise their relationship with the pregnant patient by raising smoking as an issue. System-level barriers included lack of time, resources, training and protocols, similarly described in our review. Baxter et al’s review also reports barriers to providing SCC: discussing smoking cessation depended on whether HPs were able to broach the subject, staff confidence and perception of effectiveness, manner of communication, whether follow-up occurred, time and resource constraints, and service protocols.28
One of the included Australian studies explained some of the factors that may impinge on the quality of SCC for pregnant women. Zeev et al analysed the factors associated with performance of the 5As, and provision of NRT in Australian medical practitioners.37 In a national study of 378 GPs and OBS, ‘internal influences’ (including HP confidence for counselling and prescribing NRT, optimism, sufficient time and resources) were associated with a higher likelihood of performing the 5As, whereas ‘external influences’ (ie, workplace routines, doctor–patient relationship, comfort raising the issue, perceived priority) were associated with performing the shorter version of Ask, Advise, Refer (AAR).37 92 93 Furthermore, being an OBS compared with being a GP, low confidence, and uncertainty about safety of NRT, were associated with lower odds of prescribing NRT.91
Our objective to determine which aspects of SCC for pregnant women could need improvement, revealed on the whole that ‘Assist’ and Arrange’ were less performed. Assisting pregnant smokers to quit is a vital priority. Unless there are high-quality specialised services to refer pregnant smokers to, it is insufficient for HPs to raise the issue, advice and assess, without going further to actually assist a quit attempt, and as a duty of care arrange follow-up or referral. Psychosocial support coupled with NRT (if needed, available and approved) may give pregnant women the best chance of quitting.17 94 Various implementation strategies could be considered to improve SCC delivery to pregnant women, which may include HP education and training, promotion of clinical practice guidelines, audit and feedback, reminders, opinion leaders, incentives or supervision.95 Training was reported as an educational need by the HPs in the studies, and worthy of consideration. Training should most urgently focus on the elements of the 5As that are seldom performed, taking into account country-specific needs and guidelines. Training should provide actual skills to HPs in how to assist smokers to quit, and give opportunities to practise and receive feedback on their performance. Evidence-based updates on the use of NRT in pregnancy may be warranted especially if professional college guidelines are not up to date, with a caution about jurisdictions that may deter prescribing or access.17
Providing access to resources, such as educational and training materials for HPs, evidence-based and culturally appropriate patient information sources and affordable NRT, will demand changes to policy in some settings and countries. Time is a perennial problem for HPs, however, changes in practice protocols, and a whole-of-service approach, could support pregnant women to receive the time investment warranted by such an important issue for their own and their baby’s health. Additionally, policy changes to provide accessible and culturally appropriate referral options are critical. Further research is warranted to understand which interventions can successfully improve HP performance of the 5As, and whether other models, such as the AAR,95 the ABC96 or Ask, Brief Advice, Cessation, Discuss97 approach may better facilitate HP implementation of SCC, and correspondingly improve quit rates in pregnant women. Standardised methods to assess the provision of SCC and the 5As in research or programme evaluations would aid future comparisons.
Conclusions
In a systematic review of HPs’ provision of SCC for pregnant women in 10 countries, meta-analyses were performed after combining like measures across studies where feasible. Pooled percentages revealed that HPs reliably ‘Ask’, ‘Advise’ and ‘Assess’ pregnant women about tobacco smoking. ‘Assist’, including assist by ‘prescribing NRT’, and ‘Arrange referral’ were much lower, and may be improved by appropriate interventions such as training, incentives or prompts. Meta-regressions were significant only for ‘Arrange referral’ for year and country. Further research may be required to understand other factors driving the heterogeneity between different studies. Standardised methods to assess the provision of SCC and the 5As are warranted.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
Footnotes
Contributors GSG was responsible for the design of the review, publishing the protocol in PROSPERO, oversaw all aspects of the study and wrote the manuscript. LT conducted the searches with YBZ. LS did the data extraction, and with YBZ the quality analysis. KP conducted the meta-analyses and meta-regressions. GRG assisted GSG in writing the methods and results sections, and preparing tables. BB advised on study design and critically reviewed the manuscript. YBZ advised on manuscript drafts as senior author. All authors reviewed and approved the final manuscript.
Funding This study was funded by a grant from Hunter Cancer Research Alliance, Australia.
Disclaimer The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Competing interests GSG reports grants from National Health and Medical Research Council, grants from Cancer Institute New South Wales, grants from Hunter Cancer Research Alliance, during the conduct of the study; grants from National Health and Medical Research Council, grants from Hunter New England Central Coast Primary Health Network, grants from Cancer Australia and Cure Cancer Australia, grants from Ministry of Health NSW, grants from John Hunter Hospital Charitable Trust, outside the submitted work. YBZ reports grants and others from Hunter Cancer Research Alliance, during the conduct of the study; personal fees from Novartis NCH, personal fees from Pfizer Israel LTD, outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplementary information.