Article Text

Abstract
Objectives With the high and rising total cost of medical school, medical student debt is an increasing concern for medical students and graduates, with significant potential to impact the well-being of physicians and their patients. We hypothesised that medical student debt levels would be negatively correlated with mental health and academic performance, and would influence career direction (ie, medical specialty choice).
Design We performed a systematic literature review to identify articles that assessed associations between medical student mental health, academic performance, specialty choice and debt. The databases PubMed, Medline, Embase, Scopus and PsycINFO were searched on 12 April 2017, for combinations of the medical subject headings Medical Student and Debt as search terms. Updates were incorporated on 24 April 2019.
Results 678 articles were identified, of which 52 met the inclusion criteria after being reviewed in full text. The majority of studies were conducted in the USA with some from Canada, New Zealand, Scotland and Australia. The most heavily researched aspect was the association between medical student debt and specialty choice, with the majority of studies finding that medical student debt was associated with pursuit of higher paying specialties. In addition, reported levels of financial stress were high among medical students, and correlated with debt. Finally, debt was also shown to be associated with poorer academic performance.
Conclusions Medical student debt levels are negatively associated with mental well-being and academic outcomes, and high debt is likely to drive students towards choosing higher paying specialties. Additional prospective studies may be warranted, to better understand how educational debt loads are affecting the well-being, career preparation and career choices of physicians-in-training, which may in turn impact the quality of care provided to their current and future patients.
- medical student
- debt
- stress
- mental health
- academic performance
- specialty choice
- physician
- well-being
- vocation
- loans
- financial
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- medical student
- debt
- stress
- mental health
- academic performance
- specialty choice
- physician
- well-being
- vocation
- loans
- financial
Strengths and limitations of this study
A unique systematic review that evaluates and integrates the strength of the evidence for the effects of medical education debt on medical students’ and future physicians’ mental health, academic performance and area of specialisation.
Fifty-two articles were included in the initial systematic review, with seven added on 24 April 2019.
This review does not assess evidence from primary literature that was not available in English.
Articles from only six countries met criteria for the systematic review.
Introduction
As medical students’ debt burdens rise along with the cost of education, the potential for this debt to significantly impact their well-being, career preparation and career choices, and thus the quality of care that they can provide to their current and future patients, also grows. This debt has long been a concern for current and prospective medical students, as well as graduates. Education-related costs incurred by medical students may include, at minimum, housing and living expenses, health insurance and tuition fees, and most medical students incur significant debt to cover these costs, usually in the form of government or private loans. In the USA, median indebtedness at graduation was US$192 000 in 2017 compared with US$50 000 in 1992,1 2 which is an approximately 220% increase even after accounting for the rate of inflation. Increases in these costs have outpaced the relative compensation of primary care physicians and specialists, as well as grants and scholarships.3 The effects of this debt are significant and myriad; it can negatively impact mental health and academic performance, and influence specialty choice.4 5 This issue is of great importance with the recent focus on mental health concerns in medical students and physicians.6 7
Background
Medical student debt is commonly accrued as a result of borrowing to cover the costs of medical school tuition fees, housing and living expenses. For many, this debt may be additive with pre-existing educational debt, the levels of which are already considered to constitute a ‘student debt crisis’ in many parts of the world, particularly the USA. Australia has Commonwealth supported places, that is, subsidised university education, available to all Australian citizen university students through the Higher Education Contribution Scheme—Higher Education Loan Programme, which does not incur interest and is repaid once an income threshold is reached (US$51 957 for the 2018–2019 financial year).8 New Zealand has a similar loan system to Australia, with Government Student Loan schemes available to all students. America offers three main types of loans: (1) federal loans, available to all students studying at least half-time, the accumulating interest on which may be subsidised (ie, paid) or unsubsidised (not paid) by the government during the student’s time in school, (2) Stafford or Perkins loans that accrue interest but do not require repayment until 6 months after graduation and (3) private (unsubsidised) loans from third parties like banks or state loans, sometimes offered directly from the student’s college or state.9 Canada offers grants and student loans to those with financial need studying at least part-time, which vary by province and with stated lifetime limits up to 400 weeks (or 520 weeks for those with a permanent disability).10 Typically, these loans do not incur interest until the lifetime limit is reached, and repayments are not commenced until 6 months after the student leaves or completes his/her studies.10
There is contrasting evidence regarding the extent to which debt influences choice of medical specialty.11 Results have varied between studies, with high and low debt being associated with desire for both high paying specialties and practice in primary care. The income gap between primary care and subspecialist physicians has risen to nearly threefold in some countries.12 This wage gap may contribute to the role debt plays in specialty choice. It is important to elucidate the extent to which debt affects these choices, particularly in regard to high levels of physician burnout associated with unsatisfying career choices, and insufficient numbers of primary care doctors in many countries.
Despite these concerning statistics, few studies have explored how medical students’ debt affects their mental health and academic performance. It is important to investigate the links between debt and these outcomes in order to inform interventions aimed at alleviating student stressors, and to guide specialty planning. This review was conducted to appraise the available evidence regarding the extent to which medical student debt impacts mental health, academic performance and specialty choice.
Methods
Search strategy
We searched the databases PubMed, Medline, Embase, Scopus and PsycINFO on 12 April 2017 for combinations of the medical subject headings Medical Student and Debt as search terms. A full string of search terms for PubMed is provided in the online supplementary figure S1. A language filter was then applied to exclude articles not published in English. The databases were searched from inception: PubMed 1996, Medline 1946, Embase 1974, Scopus 2004, and PsycINFO 1967. Updates were incorporated on 24 April 2019.
Supplemental material
Eligibility criteria
After the application of this filter, articles were included if they fulfilled the following criteria: (1) a primary clinical research paper; (2) specifically assessed medical students (ie, not mixed with other student groups); (3) reported on the effect of debt on (a) medical student mental health, (b) academic performance or (c) specialty choice and finally (4) available in full text.
Selection of studies
The titles and abstracts of the included publications were examined by one author (MSP), and consensus achieved in cases of uncertainty through discussion with a second author (SB), to determine if they met inclusion criteria. Those publications that were likely to meet the eligibility criteria were reviewed in full text before being included or excluded by one author (MSP). To further reduce any possible selection bias, the suggested included studies were then reviewed again by a second author (ATA) with respect to eligibility. Those for which likely eligibility could not be determined from the title and abstract were also retrieved in full text and analysed for inclusion or exclusion. Interlibrary requests were sent for any full texts that could not be accessed through the online databases. Reference lists of the included articles were searched for other studies that might be eligible.
Data extraction and quality assessment
Extraction of the following data and quality assessment for each of the included articles was completed using a standardised form in Microsoft Excel (Microsoft, Redmond, Washington, USA): study characteristics (description of study protocol, how results were assessed); characteristics of the study population (sample size, stage of medical training, undergraduate or postgraduate degree, country of study); information to evaluate risk of bias (anonymity of surveys, selection bias, presence of control group, selective reporting bias, quality assessment as seen below) and finally outcomes relevant to one of the three areas of interest (mental health, academic performance or specialty choice).
Quality of evidence
The quality of evidence of the included articles was assessed using the Oxford 2011 level of evidence, ‘quality rating scheme for studies and other evidence’, a commonly accepted tool for rating evidence. It rates trials from 1 to 5 as follows: systematic review with meta-analysis, prospective comparative cohort trial, retrospective cohort study, cross-section study and case reports.13 14 The articles’ level of evidence assessment and significant data points are summarised in tables 1-3.
Articles investigating the effect on Mental Health
Articles investigating the effect on academic performance
Articles investigating the effect on specialty choice
Role of funding source
The University of Adelaide provided institutional funds for retrieval of interlibrary requests.
Patient and public involvement
Patients and the public were not involved in this systematic review.
Results
On the initial database searches, 678 potential articles were identified. Six hundred and sixty-seven of these were in English, and after reviewing these titles and abstracts, two hundred and twenty were reviewed in full text. Fifty-two articles met the inclusion criteria and were included in this review (figure 1). A further seven articles were added in the 24th of April 2019 review.

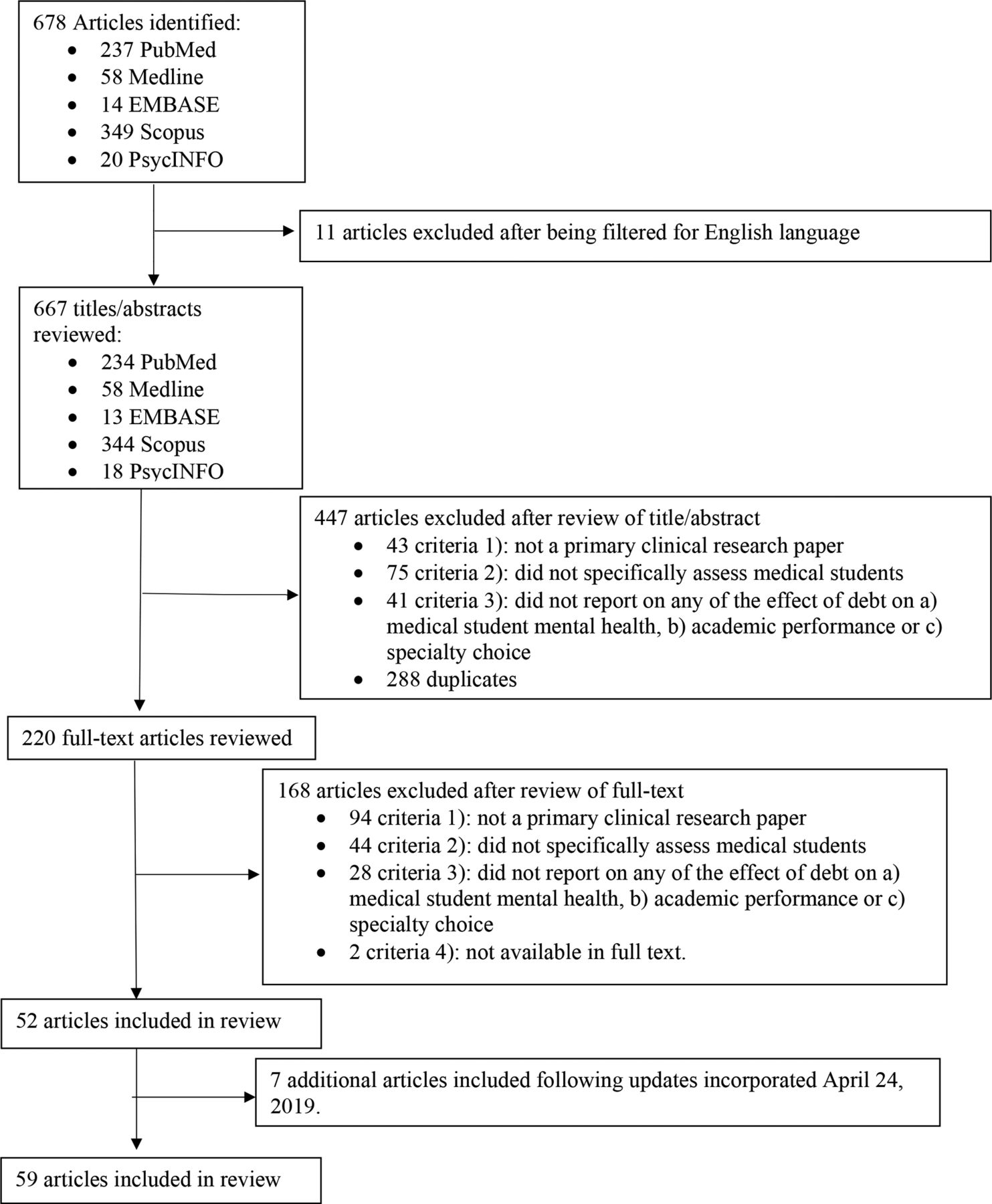{kind=link}
Flow chart detailing results of the search strategy and application of the eligibility criteria for a review of articles investigating the effects of medical student debt on mental health, academic performance or specialty choice.
The majority of the identified (included) studies examined the influence of debt on specialty choice. Only 14 articles assessed the influence of debt on (a) medical student mental health.5 15–27 Four studies assessed debt in relation to (b) academic performance.15 23 28 29 Fifty articles assessed the relationship between debt and (C) specialty choice.4 5 11 12 17 18 21 22 25 26 30–69 Several articles fell under one or more of these categories. All but one27 of the additional articles from the 2019 review examined the effect on (c) specialty choice.64–69
Effect on mental health
The 14 studies identified that assessed the impact of debt on different aspects of medical student mental health included results from several countries: the USA,5 16 18 22 56 Canada,17 19 20 25 27 New Zealand,15 26 Scotland23 and Australia24 (table 1). These studies mainly focused on the effect of debt on stress levels, rather than on symptoms of anxiety or depression. Reported levels of financial stress were typically high and correlated with debt levels at a statistically significant level (p<0.05) (table 1).
The publications with data collected from medical students in the USA found clear correlation between higher levels of debt and stress levels. In a study of 3032 postgraduate medical students, Rohlfing et al22 found that each US$50 000 increase in medical student loan debt was associated with increased self-reported stress. This stress was mainly financial, that is, related to concerns over repaying or managing debt. Another study found increasing debt levels to be positively correlated with worry and negatively correlated with comfort when rated on a Likert scale.18
Canadian studies demonstrated that junior students were more likely to report significant stress associated with finances. For example, one study found first-year medical students were more likely to report that their financial situation was very or extremely stressful (20.5%) compared with fourth-year students (17.5%).25 Those earlier in their education were found to have higher anticipated debt levels, which accounted for an additional 11.5% variance in reported stress levels when added to current debt, over that predicted by current debt alone.20 It was also found that rural students had higher levels of financial stress compared with non-rural students.17 These results were consistent with those seen in a large study by Merani et al19 that examined the financial stress levels of 7795 medical students from across Canada, lower stress levels were experienced by students in Quebec (where medical school tuition had remained stable), compared with those outside Quebec (where medical student tuition had risen dramatically).19 A more recent 2018 study found that one of the predictors for burnout and psychological distress was feeling psychologically/emotionally unsupported at their university, which increased through the years of medical training.27
In contrast, a study of 170 New Zealand undergraduate students found that concern about debt was higher in more senior (sixth-year) students, and predictably, in those who had higher levels of debt.15 In this study, those who reported that they never worried about debt (14%) had average debts of $2500 (New Zealand Dollars (NZD)), whereas those reporting that they always worried about debt (7%) had on average $NZD86 750 in debt. These results were supported by another New Zealand-based study, which showed a positive correlation between worry and indebtedness, with 32% of all students reporting worrying about debt ‘often’ or ‘always’.26 Studies from Scotland and Australia reported similar findings.23 24
Another study used a prompted-essay type format to examine how medical students in the USA emotionally perceived debt in the context of career planning.56 Common themes highlighted by the authors suggested that the responding students felt their debt burdens reflected a lack of societal investment in medical education; that their sacrifices related to that debt were underappreciated by most outside of their profession and that these debt burdens and consequent sacrifices appeared to leave them feeling entitled to certain income and lifestyle expectations going forward. Also concerning, Jackson et al16 measured alcohol dependence in medical students using the Alcohol Use Disorders Identification Test screening tool, and found alcohol abuse/dependence was significantly more common in those with >US$100 000 in educational debt (p<0.01).16 Nonetheless, the majority of students considered their debt in a positive manner: 45% sought ways to avoid accumulating more, 22% managed debt proactively and only 2% deliberately avoided thinking about debt’s consequences and ways to manage it.56
Effect on academic performance
The correlation between academic performance and debt was only investigated in four articles,4 23 28 29 shown in table 2. Debt was negatively correlated with academic performance in three of these reports,4 23 28 while one study showed no correlation between debt and attrition rates (table 2).29
One group found suboptimal academic outcomes in those with debts over US$10 000, and a progressive decrease in the percentage of students graduating with optimal outcomes as debt rose; 90.1% of students with no debt achieved a passing score on their first attempt at a high stakes examination, while only 76.4% of those with debt >US$50 000 passed on their first attempt.28 Ross et al23 found that although there was no significant relationship between total debt and class rank, the students who reported that financial worries affected their performance had lower class ranks and higher debt.23 Those who had a previous degree were also more likely to state that money affects their academic performance.23 Similarly, Gill et al15analysed students’ opinions of the effect of debt on their participation in the degree, and 21% of respondents stated that debt ‘sometimes’ impacted their ability to fully participate in their course of study.15 However, 46% stated debt never impacted them, and 31% said it rarely impacted them.15 Other studies have suggested that higher debt levels,70 or matriculation in MD-PhD programmes that are not ‘fully funded’ (ie, not supported by federal Medical Scientist Training Program (MSTP) funding),29 may increase likelihood of attrition from MD-PhD programmes.
Effect on specialty choice
The association between debt and specialty choice was assessed in a large number of studies,4 5 11 12 17 18 21 22 25 26 30–69 each of which are listed individually in table 3. There were more longitudinal studies in this area than there were studies that assessed the impact of debt on mental health or academic performance. The studies typically divided specialty choices into high paying specialties versus low paying areas (most commonly family practice/primary care). Higher paying specialties typically included surgery, dermatology, neurology, ophthalmology, radiology and other surgical and medical subspecialties. The results were varied. Overall, the majority (21) of the articles found that the presence of debt was associated with the choice of higher paying specialties.5 11 12 22 30–33 37 39 41 44–46 51 55 57 59 64–67 Nine articles found that the presence of debt was associated with lower paying specialty choices.17 22 32 38 40 42 44 56 63 A further 10 articles said there was no or minimal effect,34 35 43 47 48 52–54 62 and 13 articles found there was an association but did not further explore the nature of this relationship.4 17 18 25 26 36 49 50 56 60 68 69 The majority of these studies were conducted in the USA (table 3).
Studies conducted in the USA examining the effect of debt on specialty choice
Twenty articles from the USA5 11 12 22 30–33 37 39 41 44–46 51 55 57 59 64–67 found that the presence of significant debt was associated with higher paying specialty choice. Eight articles17 22 32 38 40 42 44 56 63 found debt was associated with a greater degree with lower paying specialties like primary care/family practice and academic medicine, compared with other medical and surgical specialties. Nine US publications found that debt did not significantly influence specialty choice.34 35 43 47 48 52–54 62 Four studies18 49 56 60 found that debt levels had an effect on specialty choice, but did not clarify in which direction.
One of the most authoritative studies in this area was a longitudinal study of 4916 US medical students, conducted by Grayson et al37 from 1992 to 2012. This study found that first-year and fourth-year medical students wanting to pursue high paying non-primary care careers anticipated a greater debt burden, placed higher importance on income and anticipated greater incomes, compared with their same-year peers seeking a career in primary care. Moreover, 31% of those reporting intending to pursue primary care at year 1 had decided to switch to a higher paying specialty by year 4, with debt and income appearing to be driving factors.37 Another longitudinal study by Jeffe et al41 found that from 1997 to 2006, the proportion of medical students with at least US$150 000 total debt at graduation rose from 6.7% to 35.9%, in conjunction with a decline in the number of physicians pursuing generalised primary care. Similarly, Schwartz et al12 found greater debt in 2007 compared with 1990, and students in 2007 were more likely to report that debt repayments pushed them away from primary care careers. More recently, high debt levels (US$150 000–US$249 999) of family medicine residents were associated with decreased odds of working in a government organisation, and very high debt levels (>US$250 000) associated with decreased odds of academic practice or geriatric fellowships.64
Although less frequently examined, loan types were also found to play a role in specialty choice. For example, Bazzoli32 examined both subsidised loans with lower interest rates that only accrue after graduation/residency, and health education assistance loans (HEAL) which had comparatively higher interest rates with accrual beginning from the date of taking the loan (ie, unsubsidised). Higher relative debt accrued from subsidised loan programmes seemed to predict primary care as a specialty choice, whereas higher (unsubsidised) HEAL debt was associated with higher paying specialties.32 These findings were consistent with more recent studies of osteopathic medical students.65 66 Conversely, Nguyen and Bounds67 found that only 24% chose primary care despite having no student debt.
Studies conducted outside the USA examining the effect of debt on specialty choice
There were five Canadian studies17 25 36 51 61 that looked at the effect of debt on specialty choice. Three articles found there was an affect but did not specify the influence,17 25 36 one found higher debt was associated with a preference for family medicine,61 and the remaining publication found debt to be associated with higher paying specialties.51 Two reports found that current debt load affected urban students’ preference for specialty choice, but had no statistically significant influence for rural students.17 36 Vanasse et al61 found that higher expected debt on completion of medical school was a strong predictor of desire to do family medicine. Morra et al51 provided an interesting possible insight into this pattern. This study found that a large number of students agreed with the rationale of doing family medicine to start paying off their debt faster, as the residency is shorter.51
Several studies were identified that studied the influence of debt on specialty choice in New Zealand.4 26 50 68 In these studies, debt was found to influence specialty choice, but generally it was not specified whether the directionality was towards higher paying specialties or primary care. McHardy et al50 found that 11% of students reported debt would have a significant influence on their career choice. Likewise, Gill et al4 found 16% of students stated level of debt as an important and strong influence on their career choice. They also noted that in sixth-year students there was a slight trend for those with higher debt to exclude general practice from their top three preferences but not to a statistically significant level. A more recent study from New Zealand found complex relationships that varied with one’s medical profession, and preference for rural versus urban practice.68
One 2018 Singaporean study investigated the associations between economic factors and residency choices. It found 40.5% of the 1241 students studied were to graduate with debt, and these students were more likely to rank an economic factor as significantly influencing their postgraduate training.69
Discussion
The majority of studies meeting the eligibility criteria and examined in this review support the notion that educational debt burden has a profound and often negative impact on medical students. Many studies reported debt as having adverse effects on student stress levels, and in some cases being associated with troubling patterns of alcohol use.16 Other reports strongly suggested that debt may also adversely affect academic performance.
Although few studies explored other aspects of students’ mental health, one example that did assess other aspects of their mental health was an Australian study by Rogers et al.24 This study identified personality traits that accounted for variances in levels of psychological stress: students with higher levels of extraversion, conscientiousness, professional expectations and lifestyle expectations, and lower levels of neuroticism, reported better well-being. In addition, future work could aim to prospectively investigate the interactions between resilience, debt and psychological distress in medical students. Results from such studies could underpin future targeted interventional strategies to maximise medical student mental health.
The influence of debt on specialty choice has been investigated much more extensively, although the majority of these studies have been conducted in the USA. These studies have produced conflicting results, and the generalisability of these findings to other countries with different socioeconomic structures may be limited. Another significant finding evident in multiple studies was differences between urban and rural students. Students from urban backgrounds were more likely to report debt as influencing their specialty choice and increasing the likelihood of them choosing higher paying specialties. Conversely, those from rural backgrounds were less likely to report an effect despite commonly having greater debt levels and/or coming from lower socioeconomic backgrounds.17 36 Together these findings illustrate the need to more clearly assess (and control for) whether one’s socioeconomic background/financial liquidity in itself is a determinant of preferred practice area, with incurred debt being simply a consequence thereof, for example, do individuals of greater or lesser financial means gravitate towards higher or lower paying practice areas, and for what reasons—or are one’s socioeconomic background and educational debt burden separate and independent predictors of specialty choice? Future studies in this area would help answer these key questions.
The vast majority of studies identified were cross-sectional in nature. Of the 52 articles included, there were only 6 prospective studies,29 37 41 42 49 59 which primarily focused on the effects of debt on influencing specialty choice. The lack of longitudinal studies is important to consider, given the dynamic nature of debt and its capacity to compound. The majority of studies employed self-report questionnaires. Likert scale-type responses were commonly used. Few studies were identified that used alternative methodologies such as interviews or focus groups, although at least one study used a prompted-essay response design.56
Furthermore, no qualifying studies could be located that examined the effects of interventions targeting debt on medical student mental health, academic performance or specialty choice. Given debt’s influence on these parameters has has been identified by the observational studies in this review, it may be reasonable to hypothesise that such interventions could influence these outcomes. Some possible debt-targeting interventions worth exploring for their effects on these outcomes, perhaps even in a prospective study, are loan forgiveness programmes. Along a similar theme, one report compared the impact of unsubsidised versus subsidised loans (a form of debt forgiveness) on specialty choice, and found those with greater unsubsidised loan burdens were more likely to pursue higher paying specialties.32 Further research yielded additional information on loan forgiveness. The US Public Service Loan Forgiveness programme, established in 2007, advertises complete (remaining) loan forgiveness for public-sector/non-profit employees after they have made 120 qualifying monthly payments. One study found more future primary care physicians intended to use this programme compared with programmes expressly designed to promote primary care.71 A survey on physician recruiting incentives reported that for 31% of respondents, whether or not a potential employer (eg, a hospital) offered educational loan forgiveness as a job incentive would have a great effect on selecting an offer.72 Findings from a very recent study of osteopathic medical graduates ‘consistently showed that graduates with a loan forgiveness/repayment programme were more likely to choose primary care over graduates without such a programme’.65 Another similar recent study reported that osteopathic ‘graduates with the most debt intended to practice in underserved areas at a higher percentage than those with the least amount of debt, and they also planned on using loan-repayment programmes at a higher rate’.66 More studies are needed in these areas, to determine whether loan forgiveness or similar programmes can obviate some the negative impacts that debt burden has on medical student mental health, academic performance and specialty choice.
Interestingly, while many studies supported the notion that significant medical school debt may drive some graduates away from primary care or other lower paying practice areas, particularly in the absence of loan repayment programmes, the converse may not necessarily be true, that is, at least one recent study suggests that the absence of medical student debt alone does not appear to drive more graduates into primary care.67
The majority of articles assessed whole-year level cohorts and were anonymous, which helped to minimise any selective reporting bias. However, many studies had small sample sizes, the smallest being 27,33 while some sample sizes were not specified.41 This raises the issue of possible non-response bias, which could have influenced results in studies with smaller sample sizes. There was also concern of differing stress levels depending on the time of the year the survey was administered. Ross et al23 acknowledged this, with their survey being released just before the examination period, which may have contributed to general stress levels as well as low response rate.
Because our initial full search and meta-analysis was performed in April 2017, which is a potential limitation of this study for publication in 2019, we incorporated key search updates on 24 April 2019. This more recent search revealed similar findings to those already concluded, in particular the majority of articles being related to specialty choice. Examples of the most recent studies64–69 are included throughout the ‘Results’ and ‘Discussion’ sections.
We also recognise the exclusion of non-English language publications as a potential limitation of this review. Additionally, there is the possibility of selective outcome reporting or publication bias that may have influenced the conclusions formed.
Additional prospective studies investigating the effects of debt on all three areas examined in this review are likely to be beneficial, especially regarding the influence of debt on medical student mental health. Furthermore, the international generalisability of studies conducted in other countries may be limited, due to a range of often significant cultural, socioeconomic, sociopolitical and structural differences regarding the costs and financial responsibilities for medical education. Many countries around the world, for example, have far greater opportunities for tuition-free medical education than others, thus making medical education debt a non-issue for some students. Accordingly, studies examining these issues may be warranted in countries in which it has not yet been examined. Future interventional studies may be useful, for example, in regard to addressing shortages of primary care physicians.
Conclusions
Medical student debt is negatively associated with mental well-being, academic outcomes and may drive physicians to practice in higher paying specialty areas rather than primary care. Further prospective studies are warranted, and student debt may be a suitable target for interventional studies aiming to improve or influence these outcomes in future.
References
Footnotes
Contributors Conception of the work: JL, M-LW, SB, MSP. Design of the work: MSP, SB, ATA, SWP. Acquisition, analysis or interpretation of data: MSP, SB, ATA, SWP, MW, M-LW, JL. Drafted the manuscript: MSP, SB, ATA. Revised the manuscript for intellectual content: SWP, MW, M-LW, JL.
Funding This work was supported by institutional funds from the University of Adelaide, and from the State University of New York (SUNY) Upstate Medical University. This paper is subject to the SUNY Open Access Policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data relevant to the study are included in the article or uploaded as supplementary information.
Patient consent for publication Not required.