Article Text

Abstract
Objective This study aimed to investigate cohort effects in selected opioids use and determine whether cohort differences were associated with changes in risk factors for use over time.
Design This study presents secondary analyses of a longitudinal survey panel of the general population that collected data biannually.
Setting Data from the Canadian Longitudinal National Population Health Survey 1994–2011.
Population This study included 12 542 participants from the following birth cohorts: post-World War I (born 1915–1924), pre-World War II (born 1925–1934), World War II (born 1935–1944), Older Baby Boom (born 1945–1954), Younger Baby Boom (born 1955–1964), Older Generation X (born 1965–1974) and Younger Generation X (born 1975–1984).
Main outcome Responses to a single question asking about the use of codeine, morphine or meperidine in the past month (yes/no) were examined.
Results Over and above age and period effects, there were significant cohort differences in selected opioids use: each succeeding recent cohort had greater use than their predecessors (eg, Gen Xers had greater use than younger baby boomers). Selected opioids use increased significantly from 1994 to 2002, plateauing between 2002 and 2006 and then declining until 2011. After accounting for cohort and period effects, there was a decline in use of these opioids with increasing age. Although pain was significantly associated with greater selected opioids use (OR=3.63, 95% CI 3.39 to 3.94), pain did not explain cohort differences. Cohort and period effects were no longer significant after adjusting for the number of chronic conditions. Cohort differences in selected opioids use mirrored cohort differences in multimorbidity. Use of these opioids was significantly associated with taking antidepressants or tranquillisers (OR=2.52, 95% CI 2.27 to 2.81 and OR=1.60, 95% CI 1.46 to 1.75, respectively).
Conclusions The findings underscore the need to consider multimorbidity including possible psychological disorders and associated medications when prescribing opioids (codeine, morphine, meperidine), particularly for recent birth cohorts. Continued efforts to monitor prescription patterns and develop specific opioid use guidelines for multimorbidity appear warranted.
- opioid use
- age-period-cohort
- multimorbidity
- antidepressants
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Analyses of data from long-term longitudinal panel survey representative of the population spanning 18 years with a wide age range (10–95 years).
Our analyses integrated changes in codeine, morphine or meperidine use with changes in risk factors over time.
The estimates of opioid use are likely underestimates as the survey only asked about the use of specific opioids (morphine, codeine and meperidine). The study survey asked participants about opioid use regardless of source and did not ask about prescription use specifically or enquire as to the reason(s) for usage. We therefore cannot be certain of the source of opioids (eg, prescribed, prescription sharing, obtained illegally) nor can we distinguish between medical and non-medical use or definitively attribute use to specific conditions.
Introduction
Opioid use in North America and its associated harms have gained increased attention in recent years among policy makers, clinicians and the general public. Canadians are the second largest per-capita consumers of prescription opioids after the USA1; as such, better understanding of the factors associated with changes over time in opioid use is important for clinicians, policy and public health organisations, to identify population groups that are potentially at a higher risk of opioid-related harms. However, examining patterns of change over time is complex. There are three, closely related, temporal components underpinning these changes: age, period and cohort effects. Age effects are the effects of growing older independently of year of birth. Period effects are variations across time periods that simultaneously affect all age groups (eg, changes in prescription practices), while birth cohort effects are the results of being born at a specific point in time. Members of a birth cohort (generation) experience the same historical and social events at the same ages, and as result, they are more likely to have distinct and cohort-specific values and attitudes.2 These conditions and circumstances may uniquely shape the patterns and trajectories of opioid use among members of different cohorts.
Examining cohort differences in opioid use requires longitudinal data spanning the age difference between cohorts or the ability to combine data from a series of cross-sectional studies. Few national studies have examined cohort and period effects on opioid use in the general population.3–6 Two studies based on the US national cross-sectional surveys of the population have generally found greater prevalence of opioid use in more recent birth cohorts.3 4 Hu et al 5 examined prescription opioid use in the US population at ages 12–34 years and similarly found that the prevalence of use increased from the 1972–1979 to the 1984–1987 birth cohorts, but in contrast to other studies, use then declined consistently among the more recent cohorts. Furthermore, none of these studies took into account the possible influence of changes in risk factors for opioid use over time in explaining the identified differences between birth cohorts. Although these studies have contributed to our understanding of changes over time in opioid use, it is not completely understood the factors underpinning these differences.
Although age has been found to be strongly related to opioid use, studies show inconsistent results.7–9 While some studies suggest higher opioid use among younger people,9 others show the opposite.7 8 These studies have also shown that women, those with higher education, smokers, obese individuals, those with greater depressive symptoms and greater pain had higher odds of reporting opioid use.7–9 It has also been shown that often opioid users also use antidepressants.10–13 Furthermore, studies have reported increased educational attainment and income, as well as obesity, smoking, physical activity and chronic conditions in more recent cohorts,14–19 and that the co-use of benzodiazepine and opioids in the US population has significantly increased between 1999 and 2014.20 Whether changes in these factors underlie cohort differences in opioid use remains to be explored.
Our study addresses this issue by drawing from 18 years of data from the Canadian longitudinal population health survey (1994/1995 to 2010/2011) to study the patterns of use of selected opioids in the population over time. While using panel data has the advantage that it follows the health experience of same people over time, a drawback is that the question on opioids is restricted to a list of agents chosen at the beginning of the survey in 1994/1995. A reflection of the timeframe of the survey is that it asked about use of opioids that were commonly used in the 1990s: morphine, codeine and meperidine. Whereas this could be seen to limit the relevance of the study, data from Ontario—largest province accounting for 40% of the population of Canada—show that codeine was the most frequently prescribed opioid between 1991 and 2007 and that the prescribing of morphine also increased considerably over the same period.21 In contrast, meperidine use in the population has substantially declined since the 1990s.22–24 Furthermore, another study show that in 1991, codeine and morphine together accounted for almost all opioid-related deaths in Ontario; however, while the proportion of deaths accounted for these two agents have declined over time, the number of deaths associated with these drugs remained fairly constant between 1991 and 2015.25 These findings coupled with research showing that the non-medical use of prescription opioids are a gateway to drugs particularly in younger generations26–28 point that examining the temporal patterns of these three agents is informative and add to the literature in this topic.
We conducted an age–period–cohort analysis to examine whether the use of these opioids differed by birth cohort after accounting for age and period effects. We also examined the contribution of changes in sociodemographic (eg, education, income) and health-related factors (eg, chronic conditions, pain, antidepressants use) to any identified age, period and cohort effects.
Methods
Study setting and population
This paper presents secondary data analyses of the longitudinal component of the National Population Health Survey (NPHS). Conducted by Statistics Canada between 1994 and 2011, the NPHS followed up a representative sample of the Canadian population. The target population included household residents in Canada’s 10 provinces in 1994/1995. More details on the NPHS sampling plan are available from Statistics Canada.29
The NPHS longitudinal sample included 17 276 participants from all ages in 1994/1995 who were interviewed every 2 years. The present study included 12 542 participants who were born between 1915 and 1984 (aged 10–79 years in 1994/1995) and who provided data at baseline and at least two follow-up cycles.
Data sharing
The survey is not publicly available and authorisation from Statistics Canada is required to access the data.
Measures
Opioid use
The NPHS defined use of opioids based on answers (yes/no) to one question: ‘In the past month, did you take codeine, Demerol or morphine?’
Age–period–cohort
We measured age in single year increments and defined period as the survey year. The birth cohorts examined were post-World War I (born 1915–1924), pre-World War II (born 1925–1934), World War II (born 1935–1944), Older Baby Boom (born 1945–1954), Younger Baby Boom (born 1955–1964), Older Generation X (born 1965–1974) and Younger Generation X (born 1975–1984).
Risk factors
Sociodemographic characteristics considered were sex, education (years of schooling grouped as ‘<12 years’, ‘12–15 years’ and ‘16+ years’) and household income quartiles. Although the survey collected data on ethnicity/cultural background, the vast majority (93.2%) of the survey participants identified themselves as white, and therefore, this variable was not included in the analysis. Lifestyle factors included were smoking status (current smoker, past smoker, never smoker); alcohol consumption (regular drinker: at least once a month, occasional drinker: less than once a month, and not currently drinking: former or never); physical activity (active vs inactive); and body mass index (BMI) (obese, overweight, normal/underweight). We also included two variables assessing health status: a variable for pain that prevents activity (no pain/pain does not prevent activity versus pain prevents activity few/sometimes/always) and a variable for number of chronic conditions (0, 1 and 2+conditions (multimorbidity)) was derived based on the reported presence of 16 doctor-diagnosed conditions: allergies (excluding food allergies), arthritis, asthma, back problems, bronchitis, cancer, cataracts, diabetes, emphysema, glaucoma, heart conditions, high blood pressure, migraine, stroke, ulcers and urinary incontinence. Lastly, two variables related to medication use were included: use of antidepressants and tranquillisers. Similar to opioid use, these variables were ascertained through the questions, ‘In the past month, did you take anti-depressants?’ and ‘In the past month, did you take tranquillisers such as Valium?’, respectively.
Statistical analysis
A hierarchical age–period–cohort (HAPC) modelling strategy was used to understand the contribution of age, period and cohort to time changes in use of selected opioids.19 30 In these models, observations are nested within individuals and individuals are nested within time periods. In the HAPC model, age and cohort were estimated as fixed effects, while period was estimated as a random effect. An unadjusted model with only age, period and cohort was estimated first (model 1). Linear and quadratic age terms were tested and the best transformation retained. Risk factors were then added sequentially to the fixed part of the model to examine their contributions to age, period and cohort effects: sociodemographic and lifestyle factors (model 2), chronic conditions and pain preventing activities (model 3) and use of tranquillisers and antidepressants (model 4). Comparing these models allowed us to examine whether changes in these risk factors over time accounted for changes in use of selected opioids. In all models, age was centred at 35 years (the median of the distribution at baseline (1994/1995)).
All models were fit using the GLIMMIX procedure from SAS/STAT version 9.4 software including incomplete cases up to the point at which they dropped out or died, and maximum likelihood estimators were used that adjust for non-response assuming the data are missing at random.31
Supplementary analyses
As it has been suggested that opioid use differs between men and women,32 analyses were stratified by sex. To examine the contribution of each individual chronic condition to cohort differences in the use of selected opioids, each of the 16 conditions were added to the final model one at a time and cohort effect estimates from these models were examined.
Almost two-fifths of eligible participants died or dropped out before the end of the study; therefore, the potential impact of attrition was also examined: models 1–4 were re-estimated by including dummy variables indicating whether the participant died or dropped out of the study. We also re-estimated the models with the sample limited to participants with complete data across the nine survey cycles.
Patient involvement
This study is based on a population survey that did not involve patients.
Results
Sample characteristics
In 1994, there were 12 542 participants contributing to three or more years of data: 1020 in the post-World War I cohort, 1377 in the pre-World War II cohort, 1591 in the World War II cohort, 2201 in the Older Baby Boom cohort, 2773 in the Younger Baby Boom cohort, 2219 in the Older Generation X cohort and 1361 Younger Generation X cohort. By 2010/2011, 27.5% of participants dropped out and 11.8% died. Table 1 contains birth cohort characteristics at baseline. There were substantial differences across cohorts related to education, income and lifestyle factors such as smoking status, BMI, physical activity and alcohol consumption. There were also differences in the number of chronic conditions reported, as well as the use of tranquillisers and antidepressants. Over the study period, codeine, morphine or meperidine use slightly increased from 4.7% at baseline to 5.7% in 2010/2011 with similar increases across all cohorts.
Birth cohort characteristics at baseline (1994/1995). Canadian National Population Health Survey, 1994–2011
Changes in codeine, morphine or meperidine use: age–period–cohort effects
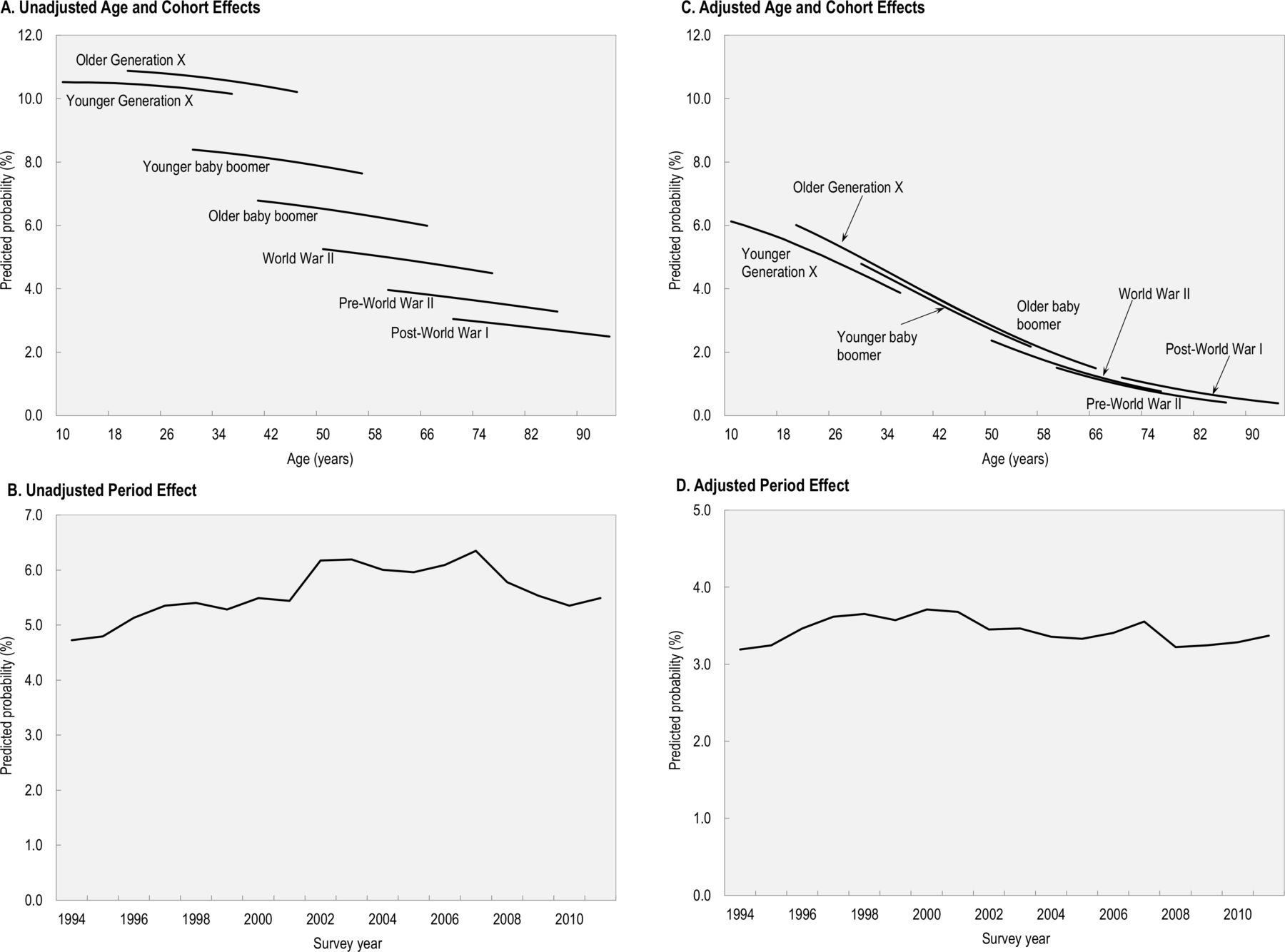
Results from the unadjusted model are shown in table 2 and illustrated in figure 1A,B. There were significant age, period and cohort effects in use of selected opioids (table 2, model 1) such that comparing birth cohorts at the same age, there was a trend of greater use of these opioids from Gen Xers to the post-World War I cohort (figure 1A). In other words, members of more recent cohorts were using these opioids at earlier ages than previous cohorts. Furthermore, there was an overall decline in use with increasing age (figure 1A). In addition to the age and cohort effects, there was a significant period effect: use of selected opioids increased steadily between 1994 and 2002, plateauing between 2002 and 2006 and declining until 2010/2011 (figure 1B).
{kind=link}
Age–period–cohort effects in opioid (codeine, morphine and meperidine) use. Canadian National Population Health Survey, 1994–2011. Values in (A) were obtained from the fixed effects of model 1 in table 2. Predictions are conditional on period effects. Values in (B) were obtained from the solution of the random effects of model 1 in table 2. Predictions are conditional on age and cohort effects. Values in (C) were obtained from the fixed effects of model 5 in table 2 with covariates at their means. Values in (D) were obtained from the solution of the random effects of model 5 in table 2.
Results from logistic hierarchical age–period–cohort models for opioid use. Canadian National Population Health Survey, 1994–2011
This model was extended by including sociodemographic and lifestyle factors (table 2, model 2). The inclusion of these variables did not substantially alter estimates for age, cohort and period effects. We then added pain preventing activity to the model and, although significant, the inclusion of pain did not alter the cohort estimates (data not shown). In contrast, after adding number of chronic conditions to the model (table 2, model 3), cohort differences were no longer significant and the period effect was largely reduced (figure 1C,D, respectively). The inclusion of use of antidepressants and tranquillisers (table 2, model 4) did not affect the estimates for the age, period or cohort effects, although the effect of number of chronic conditions was attenuated.
Risk factors for use of studied opioids
The final model (table 2, model 4) shows that in addition to age, cohort and period, other independent personal risk factors for selected opioid use were being female, having higher educational attainment, being obese or being a current smoker or drinker. Health-related risk factors were having pain that prevents activity, chronic physical health conditions, taking antidepressants and tranquillisers.
Supplementary analyses
Although women reported overall greater use of selected opioids than men, analyses stratified by sex found no significant differences in the age and cohort patterns for men and women. The findings of the analyses examining the contribution of each individual condition to cohort differences in use of selected opioids did not find that cohort differences were explained by, or attributable, to any condition in particular. Finally, the results from the analyses examining the impact of attrition (complete cases and adjusting for dropping out and death) indicated similar period and cohort effects to those obtained from the main analyses. These additional analyses did not alter our conclusions.
Discussion
Using nationally representative data, this study adds to our understanding of the dynamics of morphine, codeine and meperidine use over time by identifying a strong cohort effect of greater use of these opioids in more recent birth cohorts (eg, the prevalence for Gen Xers was higher than that for younger boomers and so on). Independently of birth cohort, there was a general effect of higher use of these opioids in younger age and higher educational level. While pain preventing activity was associated with use, pain did not explain cohort differences. The cohort effect in use of these opioids parallels cohort differences in multimorbidity previously identified for this population.19 However, the cohort differences in use were not associated with any specific chronic condition in particular.
We also found a period effect: use of selected opioids increased steadily in Canada between 1994 and 2002, plateauing between 2002 and 2006 and then declining until 2011. This finding is similar to that found in other studies.21 33–36 It has been suggested that the increase in opioid use in the 1990s is related to pharmaceutical industry opioid marketing practices to physicians during this period.37 Also over this period of time, there has been a shift from prescribing opioids primarily for severe acute or terminal pain to an increase in the use of opioids to manage any chronic painful condition.38–40
The greater morphine, codeine and meperidine use identified among those with multimorbidity is concerning, as studies have shown that the use of opioids to treat ongoing chronic conditions is associated with greater duration of use and higher dosages than for which the opioids were originally prescribed.39 40 These are, in turn, risk factors for opioid use disorder and overdose.41–43 Furthermore, the evidence of the efficacy of opioids for chronic non-cancer pain is limited and studies show that as well as addiction, other consequences of opioid use include increased risks of myocardial infarction, bone mineral density loss and overall mortality.44–47
In addition to having more multimorbidity, those using the three studied opioids were more likely to be taking antidepressants and tranquillisers, which is consistent with a recent US population-based study.20 It may be that reported use of antidepressants and tranquillisers are additional markers of greater multimorbidity, which is consistent with the reduction in the coefficient for multimorbidity when these drugs were added to our final model. Alternatively, this finding could represent an association between use of studied opioids and psychological issues. A number of studies focused on patients with chronic pain have reported that those with depression or other mental health disorders are more likely to be prescribed opioid therapy48–50 as well as to be prescribed a higher dose.51 It has also been reported that individuals with depression are more likely to develop clinically recognised opioid abuse and dependence.52 Likewise, the concomitant use of opioid, antidepressants and tranquillisers poses higher risks of opioid overdose and death due to overdose.10–13 As such, individuals with mental health disorders appear to represent a population for which particular caution in prescribing opioids is warranted.
The overall association of morphine, codeine or meperidine use with younger age and having higher educational attainment is in contradiction to the fact that the major clinical indications for opioids tend to increase with age and be more frequent in those with lower educational level.53 54 It is possible that, at the same level of multimorbidity, the higher use of these opioids at younger ages reflects their higher non-medical use.4 5 55 Another possibility is that differences in the combinations of chronic conditions by age may underlie the age differences in opioid use. Guidelines for prescribing to older people indicate opioid use should be avoided in the presence of certain conditions to prevent adverse events.56 As a result, physicians may be more cautious about prescribing opioids to older adults. Alternatively, younger people may demand or be more willing to take these opioids than their older counterparts. The higher use of these opioids among those with higher educational level contrasts findings from other studies.8 35 57 It is not clear if our findings are related to differences in physician’s practice patterns or individual preferences or a combination of both. Future research is warranted to better understand the factors underlying age and educational differences in opioid use.
Strength and limitations
A major strength of this study is that it was based on one of the few available long-term longitudinal panel datasets representative of the population, with a wide age range (10–95 years), which extended over 18 years in a period of time when there were changes in codeine, morphine and meperidine use. However, the following limitations should be considered in interpreting these findings. A major limitation of the study is that the survey question asked only about three opioid agents: morphine, codeine and meperidine. At the time of the baseline survey in 1994/1995, these three agents were the most common opioids prescribed. However, since the 1990s, clinical guidelines have discouraged the prescription of meperidine, which in turn has resulted, at least partially, in a substantial declined in use of this agent in the population.22–24 This should be taken into consideration when interpreting the study findings. Another limitation is that the study survey asked participants about opioid use regardless of source and did not ask about prescription use specifically or enquire as to the reason(s) for usage. We therefore cannot be certain of the source of opioids (eg, prescribed, prescription sharing, obtained illegally) nor can we distinguish between medical and non-medical use or definitively attribute use to specific conditions. Also, our study is based on self-reported data and the biases and inaccuracies associated with it are unknown. However, in a study of older adults, overall agreement between self-reported data on opioid use and data recorded by the pharmacy was high (93%).58 Another study of patients with chronic pain comparing self-reported data on analgesic use with prescription claims data found that self-reported usage was accurate.59 These limitations notwithstanding, our study findings are informative to the literature of opioid use in the general population.
Conclusions
The dynamics of morphine, codeine or meperidine use over time are complex. Each succeeding recent generation reported greater use, and over and above this cohort effect, there was a general trend for higher use at younger ages and also in those with higher educational level. The birth cohort differences were largely explained by more multimorbidity in recent cohorts. Morphine, codeine or meperidine use was also associated with greater use of antidepressants and tranquillisers. The findings underscore the need for taking multimorbidity, including psychological disorders and associated medications, into account when prescribing opioids particularly for more recent generations. The higher opioid use in recent generations highlights the need for continued efforts to monitor opioid prescription patterns and to develop and update specific and meaningful guidelines for their appropriate use in the management of painful chronic conditions while preventing opioid misuse.
Acknowledgments
We thank all the participants of Statistics Canada’s National Population Health Survey.
References
Footnotes
Contributors MC was the lead author on this paper. Her contributions included study design, statistical analysis and drafting of the manuscript. JDP and YRR contributed to the design of the study, interpretation of results and critically revised the manuscript. EMB provided guidance on the study design, analysis and structure of the manuscript. All authors read and approved the final manuscript and are accountable for all aspects of the study.
Funding This study was partially supported by the Toronto General & Western Hospital Foundation through the University Health Network Arthritis Program. The funding source had no role in study design, analysis or interpretation of data, writing of the manuscript or the decision to submit it for publication.
Disclaimer Access to the data was through the Statistics Canada Research Data Centres (RDC) Program, which was approved by the Social Sciences and Humanities Research Council of Canada. RDCs are operated under the provisions of the Statistics Act in accordance with all the confidentiality rules and are accessible only to researchers with approved projects. The findings and conclusions of this paper are those of the authors and do not necessarily represent the official position of Statistics Canada.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data may be obtained from a third party and are not publicly available.
Patient consent for publication Not required.