Article Text

Abstract
Objectives To map the existing literature and describe interventions aimed at building the capacity of patients to participate in care during hospitalisation by: (1) describing and categorising the aspects of care targeted by these interventions and (2) identifying the behaviour change techniques (BCTs) used in these interventions. A patient representative participated in all aspects of this project.
Design Scoping review.
Data sources MEDLINE, Embase and CINAHL (Inception −2017).
Study selection Studies reporting primary research studies on building the capacity of hospitalised adult patients to participate in care which described or included one or more structured or systematic interventions and described the outcomes for at least the key stakeholder group were included.
Data extraction Title and abstract screening and full text screening were conducted by pairs of trained reviewers. One reviewer extracted data, which were verified by a second reviewer. Interventions were classified according to seven aspects of care relevant to hospital settings. BCTs identified in the articles were assigned through consensus of three reviewers.
Results Database searches yielded a total 9899 articles, resulting in 87 articles that met the inclusion criteria. Interventions directed at building patient capacity to participate in care while hospitalised were categorised as those related to improving: patient safety (20.9%); care coordination (5.7%); effective treatment (5.7%) and/or patient-centred care using: bedside nursing handovers (5.7%); communication (29.1%); care planning (14%) or the care environment (19.8%). The majority of studies reported one or more positive outcomes from the defined intervention. Adding new elements (objects) to the environment and restructuring the social and/or physical environment were the most frequently identified BCTs.
Conclusions The majority of studies to build capacity for participation in care report one or more positive outcomes, although a more comprehensive analysis is warranted.
- patient participation
- patient-centred care
- behavior change techniques
- hospitals
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Identification of behaviour change techniques used in included studies highlights the importance of behaviour change as foundational in interventions designed to build hospitalised patient capacity to participate in care.
Because building capacity of hospitalised patients to participate in care can take many forms, the aims, interventions and study designs included in this review were heterogeneous and largely descriptive.
Exclusion of grey literature, articles published in languages other than English and articles published after August 2017 are limitations of the study.
Formal measurement of agreement levels between coders was not performed during the coding training sessions.
Patient focus groups were not included in the scoping review process. Additional patient representatives on this project may have contributed to broader patient perspective.
Introduction
Improving the safety, quality and patient-centredness of care delivered in hospitals is well-recognised as a global priority,1 2 with increasing recognition of the potential of patient engagement to contribute to the improvement agenda.3 4 Patient engagement is defined by the WHO as ‘the process of building the capacity of patients, families, carers and healthcare providers, in order to enhance safety, quality and patient-centredness of healthcare delivery’.5
Effective engagement of patients in care provided during hospitalisation has been associated with better self-management,6 7 fewer adverse events8 and diagnostic tests,9 decreased use of health services10 and shorter lengths of stay.11 Patients and families who are engaged in care have opportunities to provide information essential to appropriate care planning,12 to recognise errors in care delivery13 and to adhere to treatment plans.14 Additional benefits of effective patient and family engagement include: enhancing system responsiveness to evolving user needs;15 promoting decision-making transparency and improving quality16 17 and reducing cost and waste.15
The quality challenges common to healthcare systems include the need to improve patient safety, patient-centred care, coordination of care, effective prevention and treatment, healthy living and care affordability.18 Within hospital settings, high acuity and rapid patient turnover represent barriers to effective patient participation in care to an extent not found in other healthcare settings. Wide variability in the implementation of practices designed to promote patient and family engagement was identified in a survey of US hospitals.17 These practices were classified into the following categories: (1) organisational (eg, formal policy for disclosing medical error); (2) bedside (eg, participation in shift change report) and (3) access to information and shared decision-making (eg, online access to personal health information).
Better understanding of the characteristics of interventions aimed at building the capacity of hospitalised patients to participate in care is important for building the evidence base in this area and strengthening the theoretical underpinnings of future interventions at the design phase. Successful implementation of these types of interventions may be facilitated by the incorporation of systematic methods such as behaviour change techniques (BCTs) for characterising interventions and linking these to an analysis of the targeted behaviour.19 20 BCTs are defined as ‘observable, replicable and irreducible component(s)[s] of an intervention designed to alter or redirect causal processes that regulate behaviour’.19 The BCT Taxonomy can offer a reliable and systematic framework for the identification of the ‘active, effective’ components within specific interventions,19 provided sufficient detail is provided about the intervention.21
Given the dynamic state of evidence describing interventions to promote patient participation, a scoping review was the most appropriate method to produce a narrative integration of relevant evidence addressing our broadly defined question.21 Although efforts to intentionally build capacity to participate in care have become a priority in many hospitals, much remains to be learnt about how to best accomplish this goal. In order to advance the evidence base in this area, this scoping review aimed to map the existing literature and describe interventions aimed at building the capacity of patients to participate in care during hospitalisation. Our specific research questions were to: (1) describe and categorise the aspects of care targeted by these interventions and (2) identify the BCTs used in the interventions to build patient participation in care.
Methods
Design
As one form of knowledge synthesis, scoping reviews provide narrative integration of relevant evidence by mapping key concepts, types of evidence and gaps in research to address a broad question investigating a particular field.22 To date, there have been no syntheses of the interventions designed to build capacity of hospitalised patients to participate in care. The original protocol for this review was published in 2018.23
This systematic scoping review has allowed us to determine the extent, range and nature of research activity related to initiatives designed to build the capacity of hospitalised patients to participate in care. Guided by the methodology proposed by Arksey and O’Malley22 and its subsequent revisions,24 25 this review included the following steps: (1) identifying the research question; (2) identifying relevant studies; (2) describing study selection criteria; (3) charting the data and (3) collating, summarising and reporting the results. In keeping with other scoping reviews in which the research team is large and multidisciplinary,26 we did not undertake the optional step of consultation. To further outline the methodology, a completed PRISMA-SCr Checklist27 for scoping reviews has been attached. Because scoping reviews seek to understand topics of significant complexity in a broad area, rather than synthesise only the best available evidence, a quality appraisal of included studies was not performed.22
Patient and public involvement
A patient who was also a retired university professor (MS) with an education background was a member of the research team. He was recruited to provide a patient’s perspective.28 The lack of patient focus groups is recognised as a limitation of the study; however, the patient representative contributed actively to all phases of the scoping review from inception. He shared his experiences within the system and contributed to interpretation of the findings. We did not include patient focus groups in the consultation process for this scoping review.
Identifying the research question
In collaboration with knowledge users from the provincial Health Quality Council and health region in Saskatchewan, Canada, as well as decision makers from the Saskatchewan Ministry of Health, the team identified the following question as the focus for this scoping review: What are the characteristics of interventions designed to build the capacity of hospitalised patients in addressing key healthcare priorities reported in the literature?
Identifying relevant studies
Following an initial scan of potentially relevant databases (including the Cochrane Database of Systematic Reviews), MEDLINE, Embase and CINAHL were selected for use in this review as having the best coverage of literature related to hospitals. A comprehensive electronic literature search was conducted by an experienced medical librarian (EW) in MEDLINE (through OVID), Embase (through OVID) and CINAHL Plus (through EBSCOhost) from inception to 15 December 2016 and updated on 31 August 2017. Our search strategy included the following key terms and synonyms: acute care; hospitals; caregivers; family and patient participation, empowerment, engagement or involvement. Please see online supplementary file 1 for the comprehensive search strategy in MEDLINE. The reference lists of studies were examined to identify additional relevant articles.
Supplemental material
Literature search results were uploaded into Covidence Systematic Review Software29 after removing duplicate references. This software provides a decision dashboard and annotation tool as well as the capacity to create forms for screening and extracting data. Additional duplicates missed by the reference software were removed as identified. Studies were selected in two phases: (1) title and abstract screening and (2) full text screening/review.
Study selection
Inclusion and exclusion criteria were developed based on a preliminary literature review and the advice of knowledge users and decision-makers. In order to be included in this scoping review, the studies must have: (1) taken place within a hospital setting (including inpatient rehabilitation); (2) described or included a structured or systematic approach to building capacity of patients to participate in care, including organisational practices, bedside practices or access to information practices; (3) included adult patients only and (4) described the outcomes of the interventions from any one of the following stakeholder perspectives: patients and families; healthcare providers; health systems or administrators/funders. All study designs were included, provided that the studies adhered to the inclusion/exclusion criteria. We included only studies published in English for this scoping review, as this was the primary language spoken by team members.
Papers addressing interventions to build capacity in the following populations were excluded: children and adolescents; community or home settings; oncology patients (because this group often experiences rapid transitions between community, outpatient and inpatient settings) and emergency department settings. We also excluded papers focused on patient participation in research, databases, quality improvement (eg, patient advisory councils) or healthcare service redesign or patient needs, knowledge or activation assessments.
Team training sessions for reviewers consisted of group screening of 20 titles. The inclusion and exclusion criteria were pilot-tested during the training session resulting in minor revisions to enhance the clarity of descriptors and improve inter-rater reliability. Following this training, titles and abstracts were screened by two reviewers, one of whom was the PI (DG).26 Discrepancies were resolved through consensus between the reviewers.
A second team training session for full text screening and review was held. Eight of the nine team members participated in full text screening and review, with EP serving as an arbitrator. Two researchers independently reviewed each of articles selected for full-text screening to ensure inclusion criteria had been met. Discrepancies were discussed between the researchers to achieve consensus and in one case, the dispute was resolved by the arbitrator.
Charting the data
A standard data extraction form created using Microsoft Word (online supplementary file 2) was pilot-tested in the team training session prior to data extraction. Use of this software, rather than the preset categories in Covidence, allowed us flexibility in data extraction categories and entries. Pairs of team members were randomly assigned to extract data from 20 articles. Key characteristics extracted by the two reviewers for each article included: (1) study identification (author, year of publication, setting, country); (2) focus of the intervention; (3) description of the intervention; (4) study design and participants and (5) study findings. All extracted data from each pair of team members were reviewed and confirmed by DG.
Supplemental material
In order to categorise the focus of each article, reviewers initially coded each article according to the terms used by the authors (eg, multidisciplinary goal setting). Two team members (DG and CH) then assigned each article to one of seven categories adapted from the AHRQ National Quality Strategy Priorities18 that reflected dominant themes of this corpus of literature: patient safety; care coordination; effective treatment; bedside nursing handovers; communication; care planning and the care environment.
Coding of BCT categories and techniques occurred following the data extraction. Each article was re-read by DG, MM and LN. BCT codes were assigned independently using the operational definitions provided by the BCT taxonomy v119 and the supplementary BCT coding framework reported by Presseau et al.21 There was no limit on the number of BCTs that could be identified. Discrepancies in BCT assignment were discussed and consensus achieved.
Collating, summarising and reporting the results
A narrative approach was used to collate, summarise and report the data. Summary statistics were used to describe the number of studies by setting, country, year of publication, methods, focus and BCTs identified.
Results
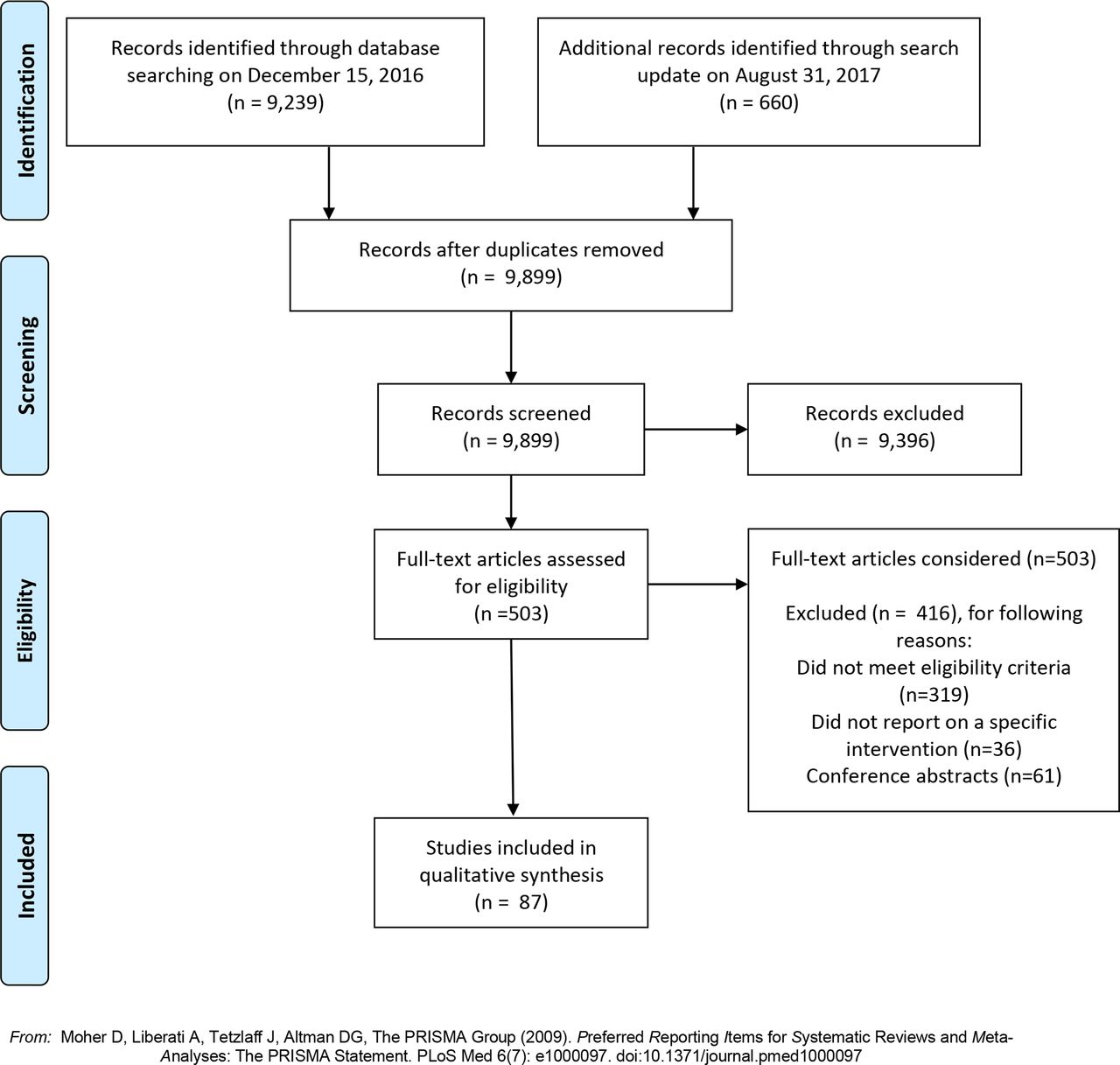
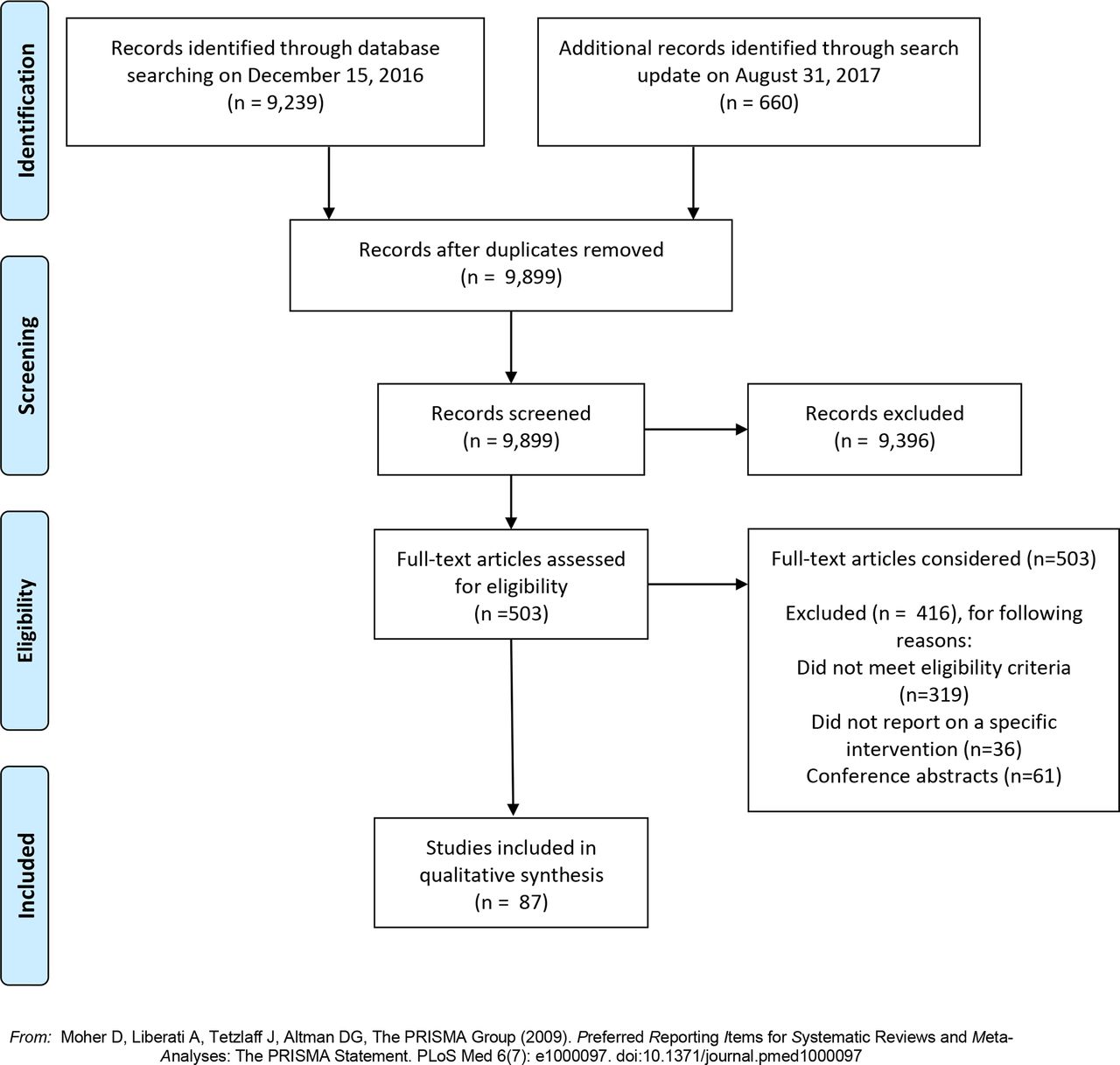
A total of 9899 articles (9239 on 15 December 2016 and 660 in the search update on 31 August 2017) were identified after duplicates were removed through the search process (figure 1). Following title and abstract screening, 503 remaining articles met our inclusion criteria and underwent full-text screening. During the full-text assessment, 416 were excluded because they did not meet one or more of the eligibility criteria (n=319), did not report on a specific intervention (n=36) or were conference abstracts (n=61). See figure 1 for the PRISMA flow diagram.
{kind=link}
PRISMA screening flowchart.
Characteristics of included studies
Online supplementary file 3 presents the summary of included studies (n=87).30–117 Over half of these studies originated in either the USA (n=32, 36.8%) or the UK (n=17, 19.5%). Fifteen (17.2%) came from Scandinavian countries and eight from Australia (9.2%). Only five (5.7%) articles were published prior to 2000.
Supplemental material
Study designs
The studies included were methodologically diverse. Of the 87 included articles, three (3.4%) were randomised controlled trials examining outcomes of interventions designed to build patient capacity to participate in care coordination,40 communication66 and effective treatment.109 Three (3.4%) cluster randomised controlled trials were aimed at improving patient capacity to participate in safety initiatives,82 recognise deteriorating condition106 and the care environment.115
The remaining studies included quasiexperimental designs, case-controlled studies (including the use of administrative data), interrupted time series, ethnographies, case studies, chart reviews and pretest and post-test designs. Qualitative and mixed methods approaches (n=29, 33.3%) and cross-sectional or preinterventions and postinterventions surveys (n=21, 24.1%) were used in over half of the included studies.
Patient populations
While a significant proportion of capacity-building interventions (eg, safety, rapid response teams) were implemented across entire acute care hospitals, other studies were directed towards specific patient populations, such as critically ill (n=7, 8.0%),35 52 56 71 73 85 97 geriatric (n=6, 6.9%),53 78 86 92 103 113 rehabilitation (n=9, 10.3%),48 69 70 89 97 104 108 116 117 surgical (n=6, 6.9%)64 72 109 112 113 or psychiatric (n=8, 9.2%)34 58 68 87 95 100 101 110 patients.
Outcomes
Positive outcomes were reported in two of the three randomised controlled trials40 68 and two of the three cluster randomised controlled trials.106 115 Failure to achieve key study objectives were reported in a number of the remaining studies.33 50 77 82 85 87 96 100 112 The remaining studies reported one or more positive outcomes associated with the intervention to build hospitalised patient capacity to engage in care.
Aspects of care addressed by capacity-building interventions
Interventions designed to build patients’ capacity to participate were found to address seven key aspects of care in hospitals. These aspects of care included: patient safety (n=18; 20.7%); bedside nursing handovers (n=5; 5.7%); communication (n=25; 28.7%); care planning (n=12; 13.8%); modifications to the care environment to promote engagement (n=17; 19.5%); care coordination (n=5; 5.7%) and effective treatment (5; 5.7%).
The interventions focused on patient safety addressed a range of safety issues including: medications;30 39 60 77 114 falls;30 53 69 hand-washing;30 46 47 54 84 90 surgical site identification;30medical error80 or patient reporting and action.32 77 82 88 93 98 Eleven (12.6%) studies incorporated a form of information technology to build the capacity of patients to participate in care.
One-third of the included studies (n=25; 28.7%) reported interventions designed to enhance communication between patients and providers to promote participation in care. Examples included interventions designed to encourage interactions between patients, families and providers,35 44 52 71 to provide a means by which patients or families could communicate their wishes or concerns74 75 81 85 or to share clinical information with patients.33 61 66 72 97
Multicomponent programmes aimed at enhancing the environment in which patient-and family-care was delivered accounted for 17 (19.5%) studies. These interventions often involved new models of care specifically aimed at promoting patient-centredness using multiple interventions, such as the adoption of new standards of care.79
Behaviour change techniques identified to build patient capacity to participate in care
Table 1 describes the types of BCTs used to build capacity for each of the seven key aspects of care.
BCTs identified to build patient capacity to participate in care (n=87)
Overall, the use of antecedents was the most frequently identified category of BCT (n=76, 87.3%). This category includes: restructuring the physical environment; restructuring the social environment; avoidance/reducing exposure to cues for the behaviour; distraction; adding objects to the environment and body changes (eg, strength training).19 Antecedents can be used to ‘set the stage’ for desired responses. Because of the frequency of identification of the category of antecedents, this category of BCT was further coded into the specific techniques employed. Adding objects to the environment was identified as an antecedent in a total of 48 (55.2%) studies. Examples of adding objects to promote patient participation in care included the use of instructional videos, for example, Refs. 62, 99 and introduction of technologies such as tablets to share information.31 Fifteen (17.2%) of these studies simultaneously added objects in conjunction with restructuring the social environment. This is illustrated by Dykes et al’s55 multifaceted intervention involving a patient-centred care and engagement programme and web-based technology, including a safety checklist and a messaging platform used by patients and care partners to view health information, participate in their care plan and communicate with care providers.
Studies that changed the social environment (n=41, 47.1%) to facilitate patient participation in care were classified as having employed the BCT of restructuring the social environment (BCT). Following the BCT coding rules of Presseau et al,21 we included in this category studies which described interventions in which someone new (patients, family member or provider) took on care, someone was added to take on new care responsibilities or someone was added to the team or care was shifted outside the team. An example of changes made to the social environment was the adoption of a new model of care providing flexible family visiting, supporting carer involvement and improving partnerships between carers and the healthcare team.59
Five studies (5.7%) were identified as making simultaneous changes to both the social and physical environments. An instance of changing both the social and physical environment was reported by Rise et al,100 who established a new patient education centre as one component of an intervention, along with appointing staff who could be contacted by families. No studies were identified as restructuring only the physical environment.
Shaping knowledge was identified as a BCT in 33 studies (37.9%). This BCT is illustrated in the study by Langer et al 80 in which clinicians were brought together with patients and families in a collaborative learning experience focused on developing patient-centred medical error disclosure communication skills. A second example of shaping knowledge was the use of the PINK (Participate; Be informed; Notice and be alert; Know what you can do) video46 with the specific goal of educating patients in the prevention of medical errors.
Feedback and monitoring were identified in 20 studies (23.0%). An example is Coleman et al’s40 Care Transition programme, in which patients monitored and responded to changes in their health conditions as a component of the intervention. Goals and planning were coded in 19 studies (21.8%). An example of goals and planning involved goal setting meetings between the patient, family and multidisciplinary team.43 Other categories of BCTs identified in the studies included: social support (n=7; 8.0%); repetition and substitution (n=5; 5.7%); regulation (n=4; 4.6%); natural consequences (n=3; 3.4%) and comparison of behaviour (n=2; 2.3%). The BCTs of association, identity and scheduled consequences were identified in one study each. Categories of BCT not identified in any of the included studies were reward and threat, self-belief and covert learning.
In the majority of studies (n=69; 79.3%), the use of multiple categories of BCT as part of the capacity-building intervention could be identified. In studies where only a single BCT was identified, restructuring the social environment52 73 76 86 91 96 99 101 108 110 occurred most frequently (n=10), although adding objects to the environment,33 39 53 56 60 63 and goals and planning48 51 were also employed as BCTs.
Discussion and conclusion
This scoping review has identified seven aspects of care in which efforts to build capacity of hospitalised patients to participate in care were reported: patient safety; care coordination; effective treatment; bedside nursing handovers; communication between patients and providers; inpatient care planning; and the overall care environment. Both large-scale (hospital-wide) and population-specific and unit-specific interventions were reported. Descriptions of these interventions in the included studies provided sufficient detail to allow for classification of the key BCTs used within each intervention. The use of antecedents (eg, adding objects to the environment or restructuring the social and/or physical environment) was the most frequently identified BCT category across all included studies. In 60% of the studies, multiple BCTs could be identified.
In keeping with the nature of a scoping review, the articles included in this scoping review were heterogeneous in terms of the aspect of care addressed, aims and methodological rigour. The strength of evidence was generally weak to very weak, thus limiting the interpretation and application for wider clinical practice. This heterogeneity limited our ability to draw conclusions about the effectiveness of the interventions. Quality appraisal was not undertaken and, as previously identified, articles were limited to English language only and did not include grey literature. Specific details of interventions were not always provided in the publications and it is possible that some BCTs used could not be accurately identified by the three reviewers who classified and achieved consensus on the BCTs identified. While our search strategy was limited to MEDLINE, Embase and CINAHL, it would be helpful to consider the inclusion of additional databases in future reviews. Although we searched the Cochrane database and did not find relevant systematic reviews, new reviews may be available in the future. As research addressing patient participation in care becomes increasingly more sophisticated, future reviews may focus on specific aspects of care such as safety for defined groups of patients.
Reviews are increasingly seeking to identify the BCTs used in a range of interventions118–120 in order to better understand the content of interventions and the underlying reasons for the outcomes associated with interventions. Adding objects to the environment was identified as the most frequently used BCT intervention in this scoping review, in keeping with the findings of Presseau et al.21 Depending on the nature of the publication and the intervention, more detailed descriptions of interventions were available for some studies compared with others. Attempts to build capacity for patients to participate in care are, at their core, social in nature and particular care should be taken to describe how the social environment facilitates performance of the desired behaviour or creates barriers to behaviours excluding patients or families from participation.
Interventions aimed at building the capacity of hospitalised patients to participate more fully in care require the use of complex interventions, especially as patient behaviour cannot change independently of provider behaviour and healthcare system attributes. Genuine engagement of patients in care will require a realignment of long-standing power imbalances between patients, providers and the healthcare system, resulting in significant changes in behaviour at many levels.121 The participation of a patient representative on this team examining the issue of patient participation proved to be extremely helpful. This individual participated in all aspects of this review, from defining the research question, screening and selection of included studies and data extraction. He provided key insights into the interpretation of the results from the perspective of an end user of the healthcare system. This individual reported that participation in this process gave him a sense of empowerment that he was influencing the knowledge base of patient care. He also noted that the process provided him with knowledge to better critique the delivery of health services. The recent GRIPP2 reporting checklist on improving the reporting of patient and public involvement in research26 provides important guidance on this issue. We would recommend that future studies include patient focus groups as a means of expanding patient input.
The rapidly evolving interest in developing interventions promoting the participation of hospitalised patients in care was demonstrated by the additional 660 articles that were published over the 8 month period between the time of the initial search and the search update. Given the growing corpus of research, this review provides an important synthesis of what has been reported to build the capacity of hospitalised patients to participate in care. This review aimed also to classify the ‘active ingredients’ underpinning the interventions by using the BCT Taxonomy.19 The findings generated through this synthesis will provide an evidentiary basis for the development of, and future research related to, tailored approaches to building patient capacity to participate in care.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
Footnotes
Contributors DG, EH, MS and TR conceptualised the study. EW conducted the literature search. DG coordinated the project and is the guarantor. MM, LN, MS, EH, TR, CH, EDP and DG screened the studies and contributed to the interpretation of findings. DG, MM and LN extracted the data. DG drafted and all authors critically reviewed and approved the revised manuscript.
Funding This work was supported by a Targeted Collaborated Innovation Grant #3894 from the Saskatchewan Health Research Foundation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All publications cited in this journal are publicly available.
Patient consent for publication Not required.