Article Text

Abstract
Objective Case-fatality rates (CFRs) for myocardial infarction (MI) and ischaemic stroke (IS) have decreased over time due to better prevention, medication and hospital care. It is unclear whether these improvements have been equally distributed according to socioeconomic position (SEP) and sex. The aim of this study is to analyse differences in short-term and long-term CFR for MI and IS by SEP and sex between the periods 1990–1994 to 2005–2009 for the entire Swedish population.
Design Population-based cohort study based on Swedish national registers.
Methods We used logistic regression and flexible parametric models to estimate short-term CFR (death before reaching the hospital or on the disease event day) and long-term CFR (1 year case-fatality conditional on surviving short-term) across five distinct SEP groups, as well as CFR differences (CFRDs) between SEP groups for both MI and IS from 1990–1994 to 2005–2009.
Results Overall short-term CFR for both MI and IS decreased between study periods. For MI, differences in short-term and long-term CFR between the least and most favourable SEP group were generally stable, except in long-term CFR among women; intermediate SEP groups mostly managed to catch up with the most favourable SEP group. For IS, short-term CFRD generally decreased compared with the most favourable group; but long-term CFRD were mostly stable, except for an increase for older subjects.
Conclusion Despite a general decline in CFR for MI and IS across all SEP groups and both sexes as well as some reductions in CFRD, we found persistent and even increasing CFRD among the least advantaged SEP groups, older patients and women. We speculate that targeted prevention rather than treatment strategies have the potential to reduce these inequalities.
- epidemiology
- social medicine
- cardiac epidemiology
- myocardial infarction
- stroke
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
In this study, we use the entire Swedish population and a follow-up period of 20 years to analyse the association between socioeconomic position (SEP) and case-fatality rates (CFRs) in myocardial infarction (MI) and ischaemic stroke (IS).
We modelled short-term and long-term CFRs separately, which allowed us to deal adequately and statistically correctly with the fact that almost 1/3 of all deaths occurred within the first day after the event.
With our statistical methods, we estimated both CFRs and CFR differences.
Information on risk factors and hospital care treatment before and after the event was not available, which prevented us from investigating medication mechanism for the association between SEP and CFRs for MI and IS.
Socioeconomic status was based on Swedish population census information, which was more current at the beginning of the study period than at the end; however, sensitivity analyses indicate that this has little or no effect on our findings.
Introduction
Although global mortality rates for cardiovascular disease (CVD) have decreased by 22% over the last two decades, CVD is still the major cause of mortality and disability worldwide.1 This decline in CVD mortality can partly be attributed to decreasing CVD incidence, suggesting effective primary prevention and improvements in modifiable risk factors such as smoking, but is also due to reduction in CVD case-fatality, reflecting improved primary and secondary care.2 3
Healthcare in Sweden is largely tax-funded with a low out-of-pocket payment, a system that allows for equal access to healthcare irrespective of financial considerations. Still, there is consistent evidence that CVD case-fatality differs by socioeconomic position (SEP),4–7 with 50% worse prognosis for the lowest compared with the highest SEP group.8 Whether reductions in CVD case-fatality have been equitable between SEP groups, as well as between sexes, is an important public health question that can direct policy and healthcare towards more vulnerable groups; the importance of trend studies for assessing socioeconomic inequalities in CVD outcome has been emphasised previously.4
However, comparatively few studies have addressed how differences in CVD case-fatality between SEP groups change over time: Davies et al report persistent socioeconomic differences in short-term case-fatality for myocardial infarction (MI) in Scotland between 1988 and 20049; Igland et al found persistent educational inequalities during the period 2001–2009 for MI case-fatality in Norway.10
Individuals with an acute CVD event who reach a hospital have access to a range of effective treatments that have contributed to observed improvements in CVD case-fatality.11 12 A significant proportion of fatalities, however, occurs directly after an CVD event, almost 30% of patients with MI in Sweden died within 1 day after this event13 and the corresponding figure for stroke was 15%.13 Still, most studies of case-fatality in CVD exclude deaths outside hospitals8 9 often because of lack of data. This is an important limitation, as SEP may affect the chances of immediate and long-term survival in different ways.
The aim of this study was to analyse changes in short-term and long-term case-fatality rates (CFRs) in MI and ischaemic stroke (IS) between the periods 1990–1994 and 2005–2009 by age, sex and SEP for the entire Swedish population.
Materials and methods
Study population
We used Swedish registers with high quality and coverage (online supplementary methods) and a follow-up period of 20 years. The Swedish National Patient Register (NPR) and the Swedish Cause of Death Register (CDR) were used to identify all cases of first primary MI and IS in two study periods, 1990–1994 and 2005–2009. All subjects who died from or were treated for MI or IS between ages 45 and 84 years at time of event were identified according to the International Classification of Diseases (ICD-9 and ICD-10, online supplementary table S1).
Supplemental material
Sex and birth date of study subjects were retrieved from the Total Population Register. We followed study subjects from the date of MI/IS until death, emigration (based on the Swedish Migration Register) or end of follow-up 1 year after the disease event.
Exposure
We identified SEP from the mandatory Swedish Population and Housing Census in 1990; for subjects with missing information on SEP, we retrieved information from the 1980 census. SEP was derived from the Socioeconomic Index14 (online supplementary methods), with five different categories, high non-manual (HN-M), low non-manual (LN-M), self-employed (SE) including farmers, high manual (HM) and low manual (LM). HN-M is supposed to be the most advantaged group and LM the least advantaged with LN-M, SE and HM as intermediate groups.
Outcome
Main outcomes are short-term mortality (defined as death within 1 day after an acute MI/IS event, including death outside the hospital) and long-term mortality (as 1-year survival, conditional on surviving the first day). For sensitivity analyses, we also considered 7-day, 28-day and 90-day survival, conditional on surviving the first day. As virtually all short-term fatalities (MI: 99.7%, IS: 99.2%) and great majority of long-term fatalities (MI: 89%, IS: 84%) are recorded as having CVD as primary or contributing cause of death, we study all-cause mortality as outcome.
Statistical methods
For both MI and IS, we modelled short-term and long-term case-fatality separately. All subjects were included in a logistic regression model for the binary outcome of dying before reaching the hospital or on the date of the disease event. Subjects who survived the first day of the disease event were included in a time-to-event analysis using flexible parametric models15 16 for 1-year survival.
For both models, we included SEP as the main exposure of interest and adjusted for sex and age as a natural spline with three df. In total, we fit eight models for all possible combinations of outcomes (MI vs IS), short-term and long-term case-fatality and period (1990–1994 vs 2005–2009). In each case, we started with a fully saturated model with a three-way interaction between age, sex and SEP and simplified by removing model terms that did not achieve statistical significance at a nominal level of α=0.05, until no further simplification was possible. These final models were used to estimate the CFRs per 1000 subjects as either event probability (logistic regression, for short-term CFR) or 1-year survival probability (time-to-event analysis, for long-term CFR) as a function of age, sex and SEP. In both cases, estimates were calculated on the linear predictor scale, for all combinations of sex and SEP at three prespecified ages (55, 65, 75) covering the age range under investigation; these contrasts were then transformed to the probability scale using the inverse link functions (logistic regression: inverse logit, flexible parametric survival regression: inverse log-log). Case-fatality rate differences (CFRDs) per 1000 subjects were estimated as differences in CFRs between SEP groups, with the most advantaged HN-M group as reference. For both CFRs and CFRDs, approximate standard errors were calculated via the multivariate delta-method17 and used to establish approximate 95% CI.
For the time-to-event analysis, we selected time since disease event as time scale and modelled the corresponding baseline hazard as a natural spline function with five df. The proportional hazard assumption for the effect of SEP on MI and IS was tested via an interaction term between SEP and time scale; as no statistically significant evidence for non-proportional effects at α=0.05 was found in any of the models, these interaction terms were not retained.
Data preparation was carried out using SAS 9.4 software (SAS Institute, Cary, North Carolina, USA). STATA (Release 14. College Station, Texas, USA, Stata) was used for the statistical analysis.
Patient and public involvement
No patient was involved in this study.
Results
Myocardial infarction
For MI, 55 456 subjects aged 45–84 years old were identified in 1990–1994 and 72 883 in 2005–2009 (table 1, online supplementary table S2). In both study periods, LM group had the highest CFR, and the HN-M had the lowest CFR across all three prespecified ages, among men and women (table 2).
Study cohort for case-fatality in myocardial infarction and ischaemic stroke by sex, age, socioeconomic position, short-term and long-term case-fatality in two periods 1990–1994 and 2005–2009
Short-term and long-term case-fatality rates and 95% confidence limits per 1000 subjects for myocardial infarction by socioeconomic position among men and women at prespecified ages 55, 65 and 75 years old in 1990–1994 and 2005–2009
Based on testing nested models, we retained only the main effects of the SEP, sex and age splines for study period 1990–1994, while for study period 2005–2009, we retained all two-way interactions (table 3).
AIC and LRT p values for evaluating candidate models for case-fatality in myocardial infarction and ischaemic stroke
Short-term case-fatality rates
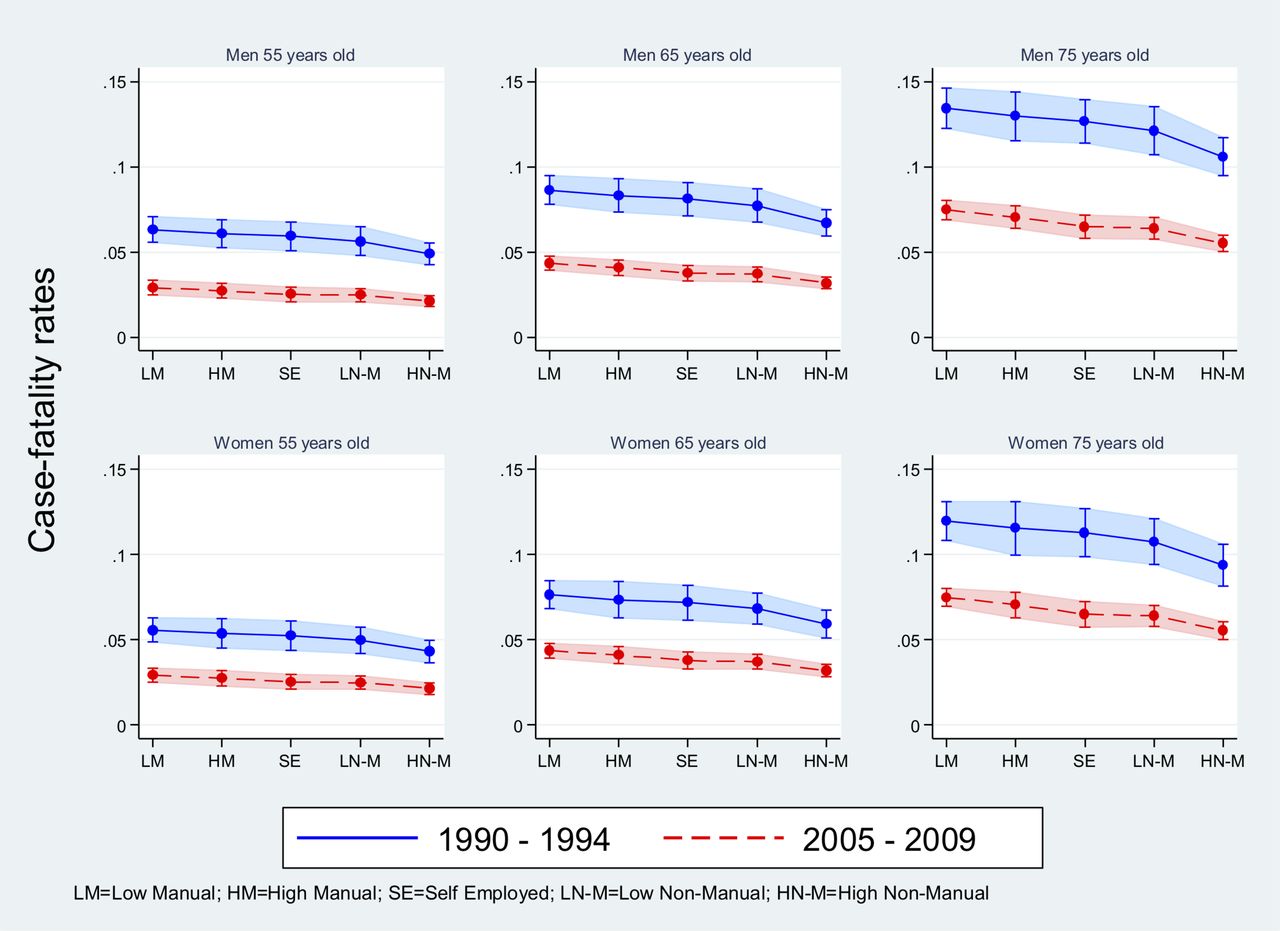
For MI, 96% of all short-term mortality was identified through CDR. Overall, short-term CFR for MI increased with age, with higher CFR in men compared with women. Over time, the short-term CFR for MI decreased for all SEP groups at all three prespecified ages among men and women (table 2, figure 1).

Short-term case-fatality rates in myocardial infarction by socioeconomic position for men and women at prespecified ages 55, 65 and 75 years old in 1990–1994 and 2005–2009.
CFRDs between LM and HN-M remained stable over the study period with a range of 39–66 extra deaths in 1990–1994 compared with 25–68 in 2005–2009 (per 1000 MI) among men and women (online supplementary table S3, online supplementary figure S1).
In comparison, 55 years old men and women in the intermediate groups (HM, SE, LN-M) had substantial smaller short-term CFRD in 2005–2009 than 1990–1994; moreover, they managed to improve their survival and had non-significant CFRDs compared with HN-M. Men and women 65 and 75 years old in intermediate SEP groups did not improve their survival over the study period.
Long-term case-fatality rates
Long-term CFR for MI for those who survived first day increased generally overall with age and was slightly higher for men compared with women (table 2, online supplementary figure S2a).
For men, CFRD between LM and HN-M remained stable over the study period, with a range of 9–35 extra deaths per 1000 MI in 1990–1994 compared with 11–35 in 2005–2009 (online supplementary table S3 and figure S2b). For women however, CFRD between LM and HN-M seemed to increase, with a range of 7–29 extra deaths in 1990–1994 compared with 15–39 extra death in 2005–2009. For intermediate groups, CFRD seemed to decrease to similar levels as for HN-M, while there was an increasing tendency for women in LN-M.
Ischaemic stroke
For IS, 24 046 subjects aged 45–84 years old were identified in 1990–1994 and 53 213 in 2005–2009 (table 1, online supplementary table S4). In both study periods, the LM group had the highest CFR and the HN-M had the lowest CFR across all three prespecified ages, both among men and women (table 4).
Short-term and long-term case-fatality rates and 95% confidence limits per 1000 subjects for ischaemic stroke by socioeconomic position among men and women at prespecified ages 55, 65 and 75 years old in 1990–1994 and 2005–2009
Based on comparison of nested models, we retained only the main effects of the SEP, sex and age splines for both study periods (table 3).
Short-term case-fatality rates
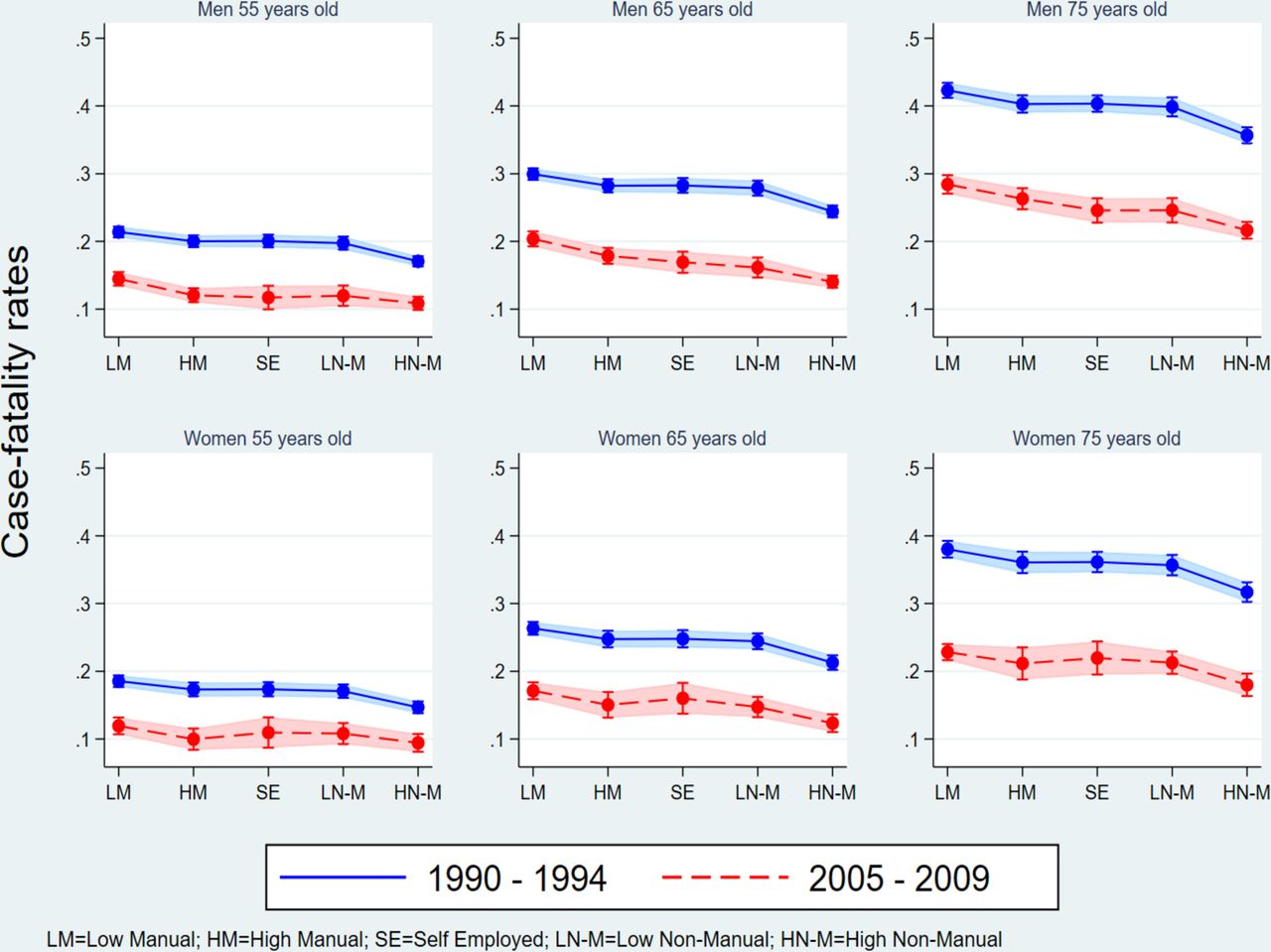
For IS, 68% of all short-term mortality was identified through CDR. Overall, short-term CFR for IS increased with age, with similar CFR among men and women. Over time, short-term CFR for IS decreased for all SEP groups, and at all three prespecified ages among men and women (table 4, figure 2).
{kind=link}
{kind=link}
Short-term case-fatality rates in ischaemic stroke by socioeconomic position among men and women at prespecified ages 55, 65 and 75 years old in 1990–1994 and 2005–2009.
Compared with HN-M, CFRDs for all other SEP groups decreased over time, among both men and women. For the LM group, the CFRD decreased from a range of 13–29 extra deaths per 1000 IS in 1990–1994 compared with 8–19 extra deaths in 2005–2009; for intermediate groups, the range decreased from 7–24 to 4–15 extra deaths per 1000 IS (online supplementary table S5 and figure S3).
Long-term case-fatality rates
Long-term CFR for IS ranged from 30 to 151 extra deaths in 1990–1994 compared with 25 to 116 in 2005–2009 (table 4, online supplementary figure S4a).
For men and women 55 and 65 years old, CFRD between the two study periods were stable (online supplementary table S5 and figure S4b). However, 75 years old men and women increased their CFRD from a range of 6–24 to 14–52 extra deaths per 1000 IS.
Discussion
In this population-based cohort study, we found that short-term CFRs for MI and IS have decreased from 1990–1994 to 2005–2009 for all SEP groups among both men and women. Short-term CFRs in the most disadvantaged LM group in 2005–2009 were lower than in the most advantaged HN-M group in 1990–1994. CFRDs for MI between the most and least disadvantaged LM and HN-M groups have mostly remained stable over time, but increased for long-term CFR among women. For IS, short-term CFRD have generally decreased over time, while long-term CFRD among the oldest subjects (75 years) has increased.
General improvements in both short-term and long-term case-fatality for MI and IS have been reported in Sweden18–21 and other European countries22 23 as well as other high-income countries.24 Evidence for SEP inequality in both short-term and long-term CFR have been reported both in Sweden and globally.4 6 The degree with which these inequalities have changed given the temporal improvements is however less well understood, since comparatively few studies have reported inequalities in CVD case-fatality over time. Davies et al 9 found persistent socioeconomic inequalities in short-term MI case-fatality among men and women in Scotland between 1988 and 2004; inequalities for case-fatality during day 1–27 were comparatively smaller, but equally persistent. Igland et al 10 reported educational inequalities in both 28 days and 29–365 days MI mortality that were strong and persistent during 2001–2009, even after adjustment for comorbidities and revascularisation. Yang et al 8 found SEP inequalities in incidence and case-fatality after MI in Sweden between 1987 and 2008; the authors also report persistent SEP inequalities in MI incidence, similar to what we have reported previously,25 but did not address trends in case-fatality. While previous results are in general agreement with our findings on MI, they are based on less complete information on short-term case-fatality (deaths outside the hospital were excluded),10 less precise SEP measurements (derived from geographical area),9 and less stringent distinction between short-term and long-term case-fatality (excluding all deaths within 28 days)8 compared with our study.
Globally, almost 80% of mortality from ischaemic heart disease and 70% of mortality from stroke is attributed to physiological and behavioural risk factors including high blood pressure, high serum cholesterol, smoking, high body mass index, alcohol use, low intake of fruits and vegetables and physical inactivity.26 Sweden, as most other high-income countries, has benefited from decreasing trends in blood pressure, cholesterol levels, smoking and alcohol use, although these positive trends have partially been offset by rising obesity and glucose levels.27
Historically, there is clear evidence for SEP inequalities for these risk factors in Sweden during our earlier study period 1990–1994.28 Recent studies, however, indicate that some of these differences have at least partially abated: SEP inequalities in both blood pressure levels as well as awareness and control of high blood pressure have decreased since then.29–31 Educational inequalities with regard to cholesterol levels were stable in men, but decreased among women, and access to treatment with lipid-lowering drugs did not differ between sex or educational levels.32 In the same period, educational inequalities in smoking and alcohol use have decreased in men, but increased in women.33 On the other hand, while a recent review suggested that the association between socioeconomic inequalities and obesity has remained stable at least until the beginning of our later study period 2005–2009,34 socioeconomic inequalities in leisure time physical inactivity have generally increased during this period.35
Short-term case-fatality
For both MI and IS, most cases of short-term case-fatality in our material are identified through CDR, limiting the potential role of improved clinical treatments in reducing short-term CFR. Determining factors for short-term survival are more generally disease severity and access to emergency acute care: the observed general decreases in short-term CFR may be attributed to a reduced severity of MI and IS due to overall positive trends in physiological and lifestyle factors as outlined above, as well as better management of pre-CVD risk factors (eg, use of angiotensin-converting enzyme inhibitors, aspirin and statins) or greater awareness of early symptoms and improvements in acute care treatment.6 7 11 24 36 37
Myocardial infarction
Assuming that the changes in short-term CFRD for MI at least partly reflect corresponding changes in risk factors, a possible explanation for the observed changes would be that the intermediate SEP groups at younger ages have embraced similar physiological and behavioural risk profiles for MI as the least disadvantaged HN-M group during the most recent study period 2005–2009, whereas the more disadvantaged LM group did not, at least not fully or in a manner where negative trends (like for physical leisure time activity) compensated for potential benefits due to positive trends (like, eg, for smoking and alcohol use).
Ischaemic stroke
Since high blood pressure is well-established as the main risk factor for all stroke subtypes,38 the decrease in short-term CFRD for IS seen in our study could be attributed to improved and more equitable control of high blood pressure among different SEP groups reducing incidence and severity of the IS events. Indeed, a Swedish study29 observed improved overall awareness and control of high blood pressure as well as diminishing differences in awareness and control between educational levels from 1990 to 2010.
Long-term case-fatality
Long-term case-fatality is affected by both the severity of the disease and quality of hospital care, including all previously mentioned physiological and behavioural risk factors for CVD that also affect short-term case-fatality as well as revascularisation and secondary care. A recent study presenting inequalities in secondary prevention after CVD in 21 countries reported Sweden as one of the countries providing most equitable access to the relevant drugs (antiplatelet, cholesterol and blood-pressure-lowering).39 It has, however, been indicated that treatment intensity at coronary care units after first MI is lower for men with low compared with high educational level.40 Other studies have also found evidence that statin medication is given preferentially to patients with a higher SEP after stroke41 or MI.42 In addition, patients with lower income have been reported as receiving revascularisation procedures to a lesser extent than patients with higher income.43
Myocardial infarction
We found that long-term CFRDs have increased in women, but not in men. While men have previously been reported to be almost twice as likely to undergo revascularisation procedures than women, the same study also found significant socioeconomic inequalities in access to coronary artery bypass grafting in men, but not in women.44 Further studies on long-term CFRD for MI among different SEP groups may be required to shed light on the reasons for increased CFRD among women.
Ischaemic stroke
Oral anticoagulants, which are recommended for secondary prevention against stroke, have been reported to be less often prescribed to older age groups and for individuals with lower educational level.45 Moreover, adherence to statin treatment over 2 years after stroke was lower in older age groups.46 These inequalities in medication for elderly can partly explain the increase CFRD at age 75 seen in our study.
Short-term versus long-term case-fatality
Short-term case-fatality is sometimes used as a proxy for severity of disease,19 which in turn is affected by disease prevention, awareness of early symptoms and the emergency transport system. Long-term case-fatality, on the other hand, is affected by the severity of the disease and also by the clinical treatment following the event. Consequently, we hypothesise that the driving forces behind broadly similar changes in short-term and long-term CFRs (stable for MI and decreasing for IS) are physiological and behavioural risk factors, and not primarily access to care after an event. This, however, does not explain the increasing SEP inequalities in long-term CFR among older men and women after IS and among women after MI, where inequitable care after an event may well be a contributing factor. Given the rapidly ageing population in Sweden and other high-income countries, this is potentially an important challenge for health services.
Strengths
To our knowledge, this is the first study to analyse short-term and long-term CFRD for MI and IS over time for an entire population, systematically including mortality both before and after hospitalisation. Other studies about socioeconomic inequalities in MI or stroke CFR10 47–50 did not distinguish in their analysis between short-term and long-term CFR; consequently, reports of decreasing long-term CFR as in Refs. 7, 47 and 48 could be biased by improvements in short-term CFR. Our approach, which models short-term CFR separately, allows us to deal adequately and statistically correctly with the fact that almost 1/3 of all deaths during the study period occurred within the first day after the event. By combining the results of the two separate models, we can still report the overall 1-year CFR (online supplementary figure S5). Our sensitivity analyses for 7-day, 28-day and 90-day CFR support the separation of short-term and long-term models (data not shown): after taking the excess short-term case-fatality into account, the estimated CFRs for 7 days, 28 days and 90 days do not differ substantially from the long-term CFRs pattern reported here.
Limitations
We only report findings for ages 45–84 years at diagnosis. The lower limit was set to exclude early-onset cases that are likely etiologically different from cases later in life. The upper limit was imposed by incomplete coverage in the population register and declining reliability of the main diagnosis in the CDR. However, these exclusions amounted to only 6% of all events during the study period. We had no information on risk factors, preventing us from investigating any medication mechanism for the association between SEP and CFR for MI or IS. Moreover, we do not have data on hospital care treatment before and after the event, such as revascularisation. The registers also lack of information important determinants of case-fatality, such as vascular comorbidity, medication adherence, access to emergency medical services and rural/urban living setting. The rural/urban divide also affects SEP and is therefore a potential confounder for the association between SEP and case-fatality. The other determinants such as vascular comorbidity are largely on the causal pathway from SEP to case-fatality and have consequently less potential for confounding this association.
As the latest census information available to us was from 1990, misclassification of SEP will affect the 2005–2009 cohort more strongly than the 1990–1994 cohort. To examine the strength of the bias this can introduce, we performed a sensitivity analysis where we back-dated the SEP for subjects diagnosed 1990–1994 to the 1980 census; this did not change our findings (data not shown). The Swedish NPR has nation-wide coverage only after 1987, which may lead to misclassification of outcomes if we included individuals with prior disease as their first primary diagnosis. However, already from 1983 the coverage of NPR was 88% (online supplementary methods) and therefore the misclassification is probably small and should not bias our results dramatically. Short-term case-fatality is largely based on the CDR, and incorrect information in the CDR will lead to misclassification of the short-term outcomes. While Johansson et al have reported 87% agreement for ischaemic heart disease as main underlying cause of death in death certificates (on which the CDR is based) and assessment of case summaries, it is unknown to which degree misclassification is differential between SEP groups; consequently, we cannot rule out some degree of bias in our estimates for the association between SEP and short-term case-fatality. Due to legal limitations, the linkage of our study population against population registers can no longer be updated beyond 2010, therefore we were limited to the current study period.
Healthcare in Sweden is largely tax-funded with a low out-of-pocket payment, a system that ensures equal access to healthcare services for everyone. Costs for health and medical care as a percentage of Sweden’s gross domestic product are stable and on par with most other European countries.51
Sweden has low rates of 30-day mortality following hospital admissions for acute MI and stroke as in many European countries. Moreover, the mortality in CVD is similar to the most of European countries.52 From international contents, our results should be comparable to most European countries that offer a universal healthcare system.
Conclusion
Both short-term and long-term CFR for MI and IS improved between study periods. Notably, both men and women in the LM group had a lower short-term CFR in 2005–2009 compared with HN-M group in 1990–1994. Despite extensive improvements, long-term CFRD remained and increased for MI in women and for IS among elderly men and women. With our novel model approach based on comparisons between short-term and long-term CFRs, we speculate that behavioural and physiological risk factors affecting MI and IS severity are the driving factors behind reduced SEP inequality in CFRs rather than more equitable access to hospital care, although continued research is required.
References
Footnotes
Contributors NM and PS conceived the original research idea. NM extracted the data. NM and AP conducted all data analyses and drafted the manuscript. NM, SH, ST, IK, PS and AP were involved in interpretation of results. NM, SH, ST, IK, PS and AP revised the manuscript and agreed on the final version to be submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval Ethical approval (03-466) was obtained from the Regional Ethical Review Board in Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Patient consent for publication Not required.