Article Text

Abstract
Objectives Oral direct-acting antivirals (DAAs) for hepatitis C virus (HCV) have dramatically changed the treatment paradigm. Our aim was to project temporal trends in HCV diagnosis, treatment and disease burden in France, Germany, Italy, Spain and the UK.
Design A mathematical simulation model of natural history of HCV infection.
Participants HCV-infected patients defined based on country-specific age, fibrosis and genotype distributions.
Interventions HCV screening practice and availability of different waves of DAA treatment in each country.
Outcome measures Temporal trends in the number of patients who achieve sustained virological response (SVR), fail treatment (by drug regimen) and develop advanced sequelae from 2014 to 2030 in each country.
Results We projected that 1 324 000 individuals would receive treatment from 2014 to 2030 in the five European countries and 12 000–37 000 of them would fail to achieve SVR. By 2021, the number of individuals cured of HCV would supersede the number of actively infected individuals in France, Germany, Spain and the UK. Under status quo, the diagnosis rate would reach between 65% and 75% and treatment coverage between 65% and 74% by 2030 in these countries. The number of patients who fail treatment would decrease over time, with the majority of those who fail treatment having been exposed to non-structural protein 5A inhibitors.
Conclusions In the era of DAAs, the number of people with HCV who achieved a cure will exceed the number of viraemic patients, but many patients will remain undiagnosed, untreated, fail multiple treatments and develop advanced sequelae. Scaling-up screening and treatment capacity, and timely and effective retreatment are needed to avail the full benefits of DAAs and to meet HCV elimination targets set by WHO.
- hepatitis C elimination
- disease trend
- direct-acting antivirals
- treatment failure
- simulation model
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This modelling-based study projected trends in hepatitis C virus (HCV) prevalence, diagnosis rate and treatment coverage in five Europe countries, and shed light on the policy implications for HCV management in each country.
The model used country-specific inputs from multiple sources including published studies, commercial claims data and simulated clinical practice of HCV in each country.
The model was calibrated to the best available data sources, and uncertainty in model outcomes was systematically examined by Monte Carlo probabilistic sensitivity analyses.
Limitations include lack of data on future HCV treatment coverage and diagnosis rate and HCV incidence rate, for which we used conservative assumptions in this study.
Introduction
Chronic hepatitis C virus (HCV) infection presents a major public health burden in Europe, affecting more than 3.2 million people in the European Union.1 HCV is the leading cause of liver cirrhosis and hepatocellular carcinoma, and the most common indication of liver transplantation. In addition, HCV infection is associated with considerable health and economic burden, resulting in productivity loss, activity impairment, reduced quality of life and increased healthcare costs in Europe.2
The recent availability of oral direct-acting antiviral (DAA) therapies for HCV has significantly changed the landscape of HCV treatment. The currently recommended first-line antiviral therapies in Europe include all-oral DAA regimens containing a non-structural protein 5A (NS5A) inhibitor or non-NS5A inhibitor.3 These DAAs are highly efficacious and safe, with sustained virological response (SVR) rates of more than 90%. Because of these advancements, oral DAAs offer an opportunity to eliminate HCV infection—the World Health Assembly pledged to eliminate HCV as a public health threat by 2030 (90% reduction in HCV incidence; 65% reduction in HCV mortality). To reach this elimination goal by 2030, 90% of HCV-infected people need to be diagnosed and 80% of eligible people need to be treated.4
Therefore, it is important to understand the current trends in HCV disease epidemiology and treatment patterns to inform appropriate steps needed to remove barriers to HCV elimination. For instance, a vast majority of patients remain unaware of their HCV infection in Europe and may never reap the benefits offered by the DAAs. Second, even though DAAs are highly cost-effective/cost saving,5 6 limited budget allocated to HCV treatment still remains a major barrier in HCV care and several countries in Europe have restrictions on the number of patients who can receive treatment.7 8 Third, a small percentage of patients will still fail to achieve SVR in the era of DAAs and may not get timely retreatment. Addressing the above barriers will reduce HCV-related deaths, the incidence of decompensation and hepatocellular carcinoma, and need for liver transplantation.
The objective of our study was to project recent trends in HCV disease epidemiology, the number of people who are eligible for treatment and the number of patients who fail currently approved oral DAA therapies in France, Germany, Italy, Spain and the UK.
Methods
Model overview
We adapted our previously developed and validated Hepatitis C Disease Burden Simulation (HEP-SIM) model to simulate the HCV landscape in five European countries: France, Germany, Italy, Spain and the UK. HEP-SIM is an individual-level state-transition model that simulates the natural history of HCV under different situations. The HEP-SIM model was parameterised using country-specific disease and population characteristics. It also captured the clinical management of HCV by incorporating HCV disease progression, diagnosis rate, treatment access and the availability of different waves of antivirals therapies. Model outcomes included temporal trends in HCV prevalence and awareness, the number of patients who achieved a cure, the number of treatment failures, the number of treatment-experienced patients needing retreatment and liver-related deaths from 2014 to 2030. Below, we describe the major model components of HEP-SIM; further model details can be found elsewhere.9–11
Patient and public involvement
Our study simulated the life course of hypothetical patients using a mathematical model. Patients and public were not involved in the study.
Baseline cohort
We first generated the baseline patient cohort in HEP-SIM to represent the HCV population in each country (online supplementary S1, tables S1–S4). For these cohorts, we defined distribution of HCV genotypes, age and gender,12–18 and calibrated the initial prevalence and the distribution of chronic HCV stages based on the estimates from Polaris observatory data up to year 201319 (online supplementary figure S1). The annual incidence of HCV in each country was extracted from Polaris observatory data (online supplementary table S5).
Supplemental material
Natural history of chronic HCV infection
The model simulated the natural history of HCV, which was defined using several health states that represented acute and chronic phases of HCV (online supplementary figure S2). All newly infected patients started in the acute phase, and could either have spontaneous resolution or develop chronic HCV infection. Chronic HCV was defined using METAVIR fibrosis scores (no fibrosis (F0), portal fibrosis without septa (F1), portal fibrosis with few septa (F2), numerous septa without fibrosis (F3) or cirrhosis (F4), and additional states defined as decompensated cirrhosis, hepatocellular carcinoma, liver transplantation, liver-related death and death from other causes.
The transition rates between fibrosis stages were estimated from a published meta-analysis20 (table 1). The disease progression rates from cirrhosis to decompensated cirrhosis were estimated from published observational studies.21 22 Patients developing decompensated cirrhosis or hepatocellular carcinoma had higher mortality rates22 23 and could receive a liver transplant (online supplementary S1, table S6). Patients who achieved SVR at F4 stage fibrosis were at risk of progression to decompensated cirrhosis or HCC.24 In addition, patients could transition to the death state from any of the above states because of background mortality, which was estimated from country-specific life tables from the Global Health Observatory data repository of WHO25 (online supplementary table S7). We cross-validated the natural history results of our model by comparing model-predicted 10-year cumulative incidence of advanced sequelae in cirrhotic patients with that reported by an observational study26 (online supplementary table S8).
State transition probabilities used in HEP-SIM model
HCV awareness and diagnosis rate
Patients unaware of their infection could become aware through routine HCV testing practice, which varied among countries. We set the awareness rate for the baseline cohort to match the awareness rate estimates at year 2001 in each country using the Polaris Observatory data.27 For new HCV infections, we assumed 7.2% patients were aware of their infection at the time of transmission.28 Undiagnosed patients in the model could become aware of their infection over time via diagnosis. This rate in each country was estimated from a published study29 and expert opinion (online supplementary table S9).
HCV treatment waves
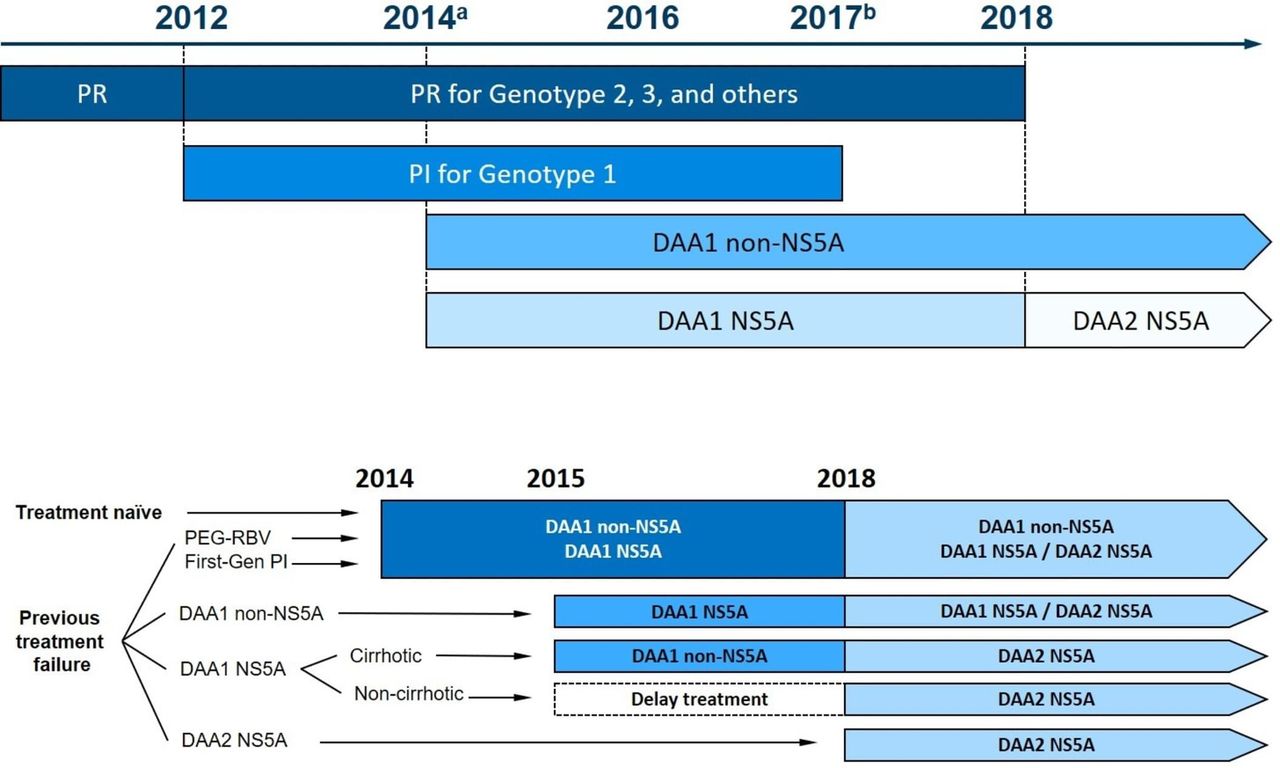
We simulated the changing landscape of HCV treatment in different waves (figure 1). The model started with peginterferon-ribavirin (PEG-RBV) treatment (referred to as PR wave), followed by the launch of first-generation protease inhibitors, that is, boceprevir and telaprevir (referred to as PI wave), for genotype 1 only in 2012. From 2014 onwards, we simulated the availability of oral DAAs including both non-NS5A inhibitors sofosbuvir and simeprevir (referred to as DAA1 non-NS5A wave) and NS5A inhibitors (referred to as DAA1 NS5A wave), which were followed by the next generation of NS5A inhibitors (referred to as DAA2 NS5A wave) from 2018 onwards (figure 1). The timeline of the changing treatment practice varied by country and was based on the approval date of each drug in that country. We also estimated the market share for each treatment type using commercial claims data from QuintilesIMS (online supplementary table S10). The SVR rates of each type of treatment were estimated from real-world data and were based on HCV genotype, fibrosis stage, and prior treatment history (online supplementary table S11).
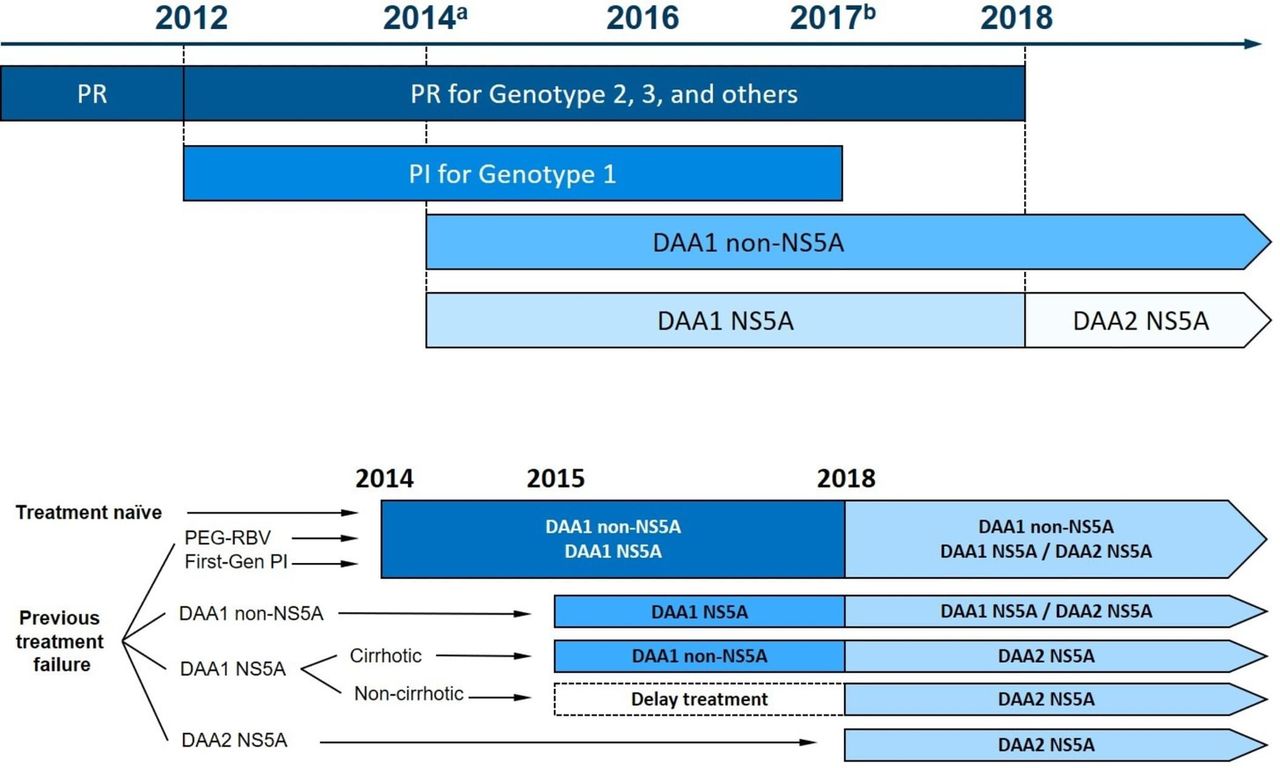
DAA treatment landscape from 2014 onwards (A) and drug regimen type for a patient by treatment history (naïve or type of prior experience) and the year retreatment is offered (B). First generation PI (BOC/TEL+PEG+RBV) used for HCV genotype 1 only. Note that the timing of treatment waves is positioned such that the HCV patients will complete treatment in the given year (not necessarily initiate treatment in that year) DAA1 non-NS5A includes the following drug combinations: SOF +PEG+/-RBV, SOF +/-RBV, SOF +SMV+/-RBV and SMV+PEG+/-RBV. DAA1 NS5A includes the following drug combinations: LDV/SOF+/-RBV, SOF+DCV, DCV+PEG+/-RBV, OBV/PTV/r+DSV+/-RBV, OBV/PTV/r+/-RBV, EBR/GZR and SOF/VEL. DAA2 NS5A includes the next wave of drug combinations such as SOF/VEL/VOX and glecaprevir/pibrentasvir for selected subgroups. Though these drugs became available in mid-2017, the SVR status of patients receiving them would become available from 2018 onwards; therefore, we noted 2018 as the year for this wave of DAAs. BOC, boceprevir; DAA, direct-acting antiviral; DCV, daclatasvir; DSV, dasabuvir; EBR, elbasvir; GZR, grazoprevir; HCV, hepatitis C virus; LDV, ledipasvir; NS5A, non-structural protein 5A; OBV, ombitasvir; PEG, peginterferon; PTV, paritaprevir; r, ritonavir; RBV, ribavirin; SMV, simeprevir; SOF, sofosbuvir; SVR, sustained virological response; TEL, telaprevir; VEL, velpatasvir; VOX, voxilaprevir.
Treatment uptake and prioritisation
Patients were eligible for treatment only if they were aware of their HCV infection. The type of treatment was determined by patient’s HCV genotype, presence of cirrhosis, prior treatment history and the treatment wave in a given year. To estimate the number of patients receiving treatment in each year, we used Polaris Observatory data (up to year 2014) and drug sales (after year 2015) as surrogates for the treatment uptake (online supplementary table S12). We assumed that the current drug sales data represented the maximum annual treatment uptake from 2018 onwards. The actual number of patients receiving treatment was dependent on treatment eligibility criteria, patients’ awareness status and treatment history, and these numbers could be lower than the maximum treatment uptake rate in each country.
Consistent with observed clinical practice, patients with F3 and F4 stages received priority for treatment when the number of treatment candidates was higher than the annual treatment capacity. Patients who have failed previous treatment could receive retreatment with some constraints. In particular, considering that PEG-RBV regimen has low SVR rates and is associated with substantial side effects, we assumed that patients would not have more than two treatment attempts with PEG-RBV regimen; for the first-generation PIs, we assumed patients would receive at most one such treatment because it was available only during a short period of time (2012–2013); for DAAs, we assumed patients would receive at most three DAA-based treatments, because they have high SVR rates (>90%) with minimal side effects, there are no major clinical concerns that prevent patients from receiving retreatment after previous treatment failures, and most patients would be highly likely to achieve SVR within three treatment attempts. Prior to 2018, among those who have failed an NS5A DAA, only cirrhotic patients were eligible for immediate retreatment with a non-NS5A DAA therapy.3 F0–F3 patients who failed treatment with an NS5A inhibitor would wait for retreatment until the next wave of DAA therapies (DAA2 NS5A wave). From 2018 onwards, patients who have previously failed any DAA regimens could be retreated with DAA2 NS5A inhibitors.3 Though these drugs became available in mid-2017, the SVR status of patients receiving them would become available from 2018 onwards; therefore, we noted 2018 as the year for the DAA2 NS5A wave.
Model outcomes
For each country, we projected temporal trends in the prevalence of HCV infection, and tracked the diagnosis rate and treatment rate over time. We defined the diagnosis rate as the percentage of diagnosed viraemic cases and cured cases among the total population (ie, all viraemic and cured cases), and the treatment coverage rate as the percentage of cured cases among the total HCV population. We also projected the number of patients who achieved SVR, the number of treatment failures and advanced outcomes in patients who failed treatment from 2014 to 2030. We presented these outcomes by drug regimen (PEG-RBV, NS5A or non-NS5A failure), and presence or absence of cirrhosis. To test the robustness of the projected outcomes, we performed probabilistic sensitivity analyses and presented the 95% uncertainty intervals of model outcomes (see details in online supplement S2, table S13).
Results
Number of HCV patients: viraemic or cured
We projected the number of HCV patients alive who will either remain viraemic or achieve SVR from 2014 to 2030 in each country (figure 2). The estimated number of patients with SVR would increase from 70 000 in 2014 to 173 000 (147% increase) by 2030 in France, from 81 000 to 193 000 (138% increase) in Germany, from 67 000 to 366 000 (446% increase) in Italy, from 53 000 to 190 000 (258% increase) in Spain, and from 37 000 to 139 000 (276% increase) in the UK. During the same period, the number of viraemic patients is projected to decrease from 243 000 to 91 000 (63% decrease) in France, from 264 000 to 107 000 (59%) in Germany, from 869 000 to 169 000 (77%) in Italy, from 390 000 to 128 000 (67%) in Spain and from 180 000 to 89 000 (51%) in the UK. A 95% uncertainty intervals of key model outcomes from probabilistic sensitivity analysis are provided in online supplementary S3, table S14.

Number of HCV patients alive who either are viraemic (blue) or achieved SVR (red) between 2014 and 2030. Bands show 95% uncertainty intervals generated by probabilistic sensitivity analysis. HCV, hepatitis C virus; SVR, sustained virological response.
We also projected that, for the first time, the total number of hepatitis C individuals alive who have achieved SVR (ie, cured) could exceed the number of viraemic patients. This significant milestone would occur in France by the end of year 2021, Germany by 2019, Italy by 2026, Spain by 2019 and the UK by of 2020.
HCV diagnosis trends
The HCV diagnosis rates varied across countries. In 2014, 122 000 HCV individuals had been diagnosed (diagnosis rate of 59%) in France, 120 000 individuals (55%) in Germany, 531 000 (62%) in Italy, 167 000 (46%) in Spain and 70 000 (48%) in the UK (figure 3). While most patients diagnosed of their infection would receive treatment by 2020, a significant number of patients would still remain undiagnosed of their chronic infection. Under the current practice, HCV diagnosis rates are expected to increase to 71% in France, 70% in Germany, 75% in Italy, 68% in Spain and 65% in the UK by 2030. In other words, 446 000 individuals across these five countries would remain undiagnosed of their HCV status by the end of 2030—among those, 72 000 would be in France, 84 000 in Germany, 125 000 in Italy, 91 000 in Spain and 74 000 in the UK.

Number of patients alive viraemic patients aware and unaware of their infection between 2014 and 2030.
Treatment rate
We projected that 1.32 million patients would receive treatment between 2014 and 2030 in the five listed European countries. In Germany, DAAs became the primary regimen for HCV treatment in 2014, whereas for the other countries, the major shift in treatment to DAAs happened in 2015 (figure 4). Between 2014 and 2030, among all patients receiving treatment, 171 000 (90%) received treatment with NS5A DAAs in France, 177 000 (84%) in Germany, 484 000 (90%) in Italy, 218 000 (90%) in Spain and 123 000 (89%) in the UK. In France, 22% of patients receiving treatment were cirrhotic, and the corresponding estimates were 20% in Germany, 27% in Italy, 23% in Spain and 13% in the UK. Under the current screening and treatment practices, the number of patients receiving treatment would remain steady in France and Italy until at least 2020; whereas, the number of patients receiving treatment would drop substantially in Spain by 2020.

Number of patients treated with DAAs each year from 2014 to 2030 by: (A) NS5A versus non-NS5A inhibitors, (B) presence or absence of cirrhosis. DAAs, direct-acting antivirals; NS5A, non-structural protein 5A.
We also projected the treatment coverage rate for each country. In 2020, the treatment coverage rate would be 50% in France, 62% in Germany, 29% in Italy, 56% in Spain and 54% in the UK. By 2030, the treatment rate is projected to increase to 71% in France, 70% in Germany, 74% in Italy, 68% in Spain and 65% in UK.
Number of treatment failures
Of all patients receiving treatment between 2014 and 2030, 104 000 (8%) are projected to fail treatment in the five listed European countries. In particular, 18 000 (9%) are projected to fail treatment in France, 17 000 (8%) in Germany, 37 000 (7%) in Italy, 21 000 (9%) in Spain and 12 000 (9%) in the UK. Among those, 8600 (49% of all treatment failures) would fail treatment with NS5A DAAs in France, 9700 (58%) in Germany, 23 000 (63%) in Italy, 12 000 (59%) in Spain and 6200 (52%) in the UK. Figure 5 shows the number of patients who fail treatment each year by the type of treatment category. The model projected that the number of treatment failures is expected to decrease, which is driven by the increased use of highly effective NS5A DAAs as well as the decline in the number of people receiving treatment. From 2018 onwards, almost all treatment failures will be from NS5A inhibitors. Of note, the number of treatment failures increased in Italy from 2014 to 2015 and in UK from 2015 to 2016 because of an increase in the treatment capacity. Among those who failed treatment between 2014 and 2030, 45% were cirrhotic in France, 39% in Germany, 46% in Italy, 43% in Spain and 31% in the UK (online supplementary figure S3).

Number of patients who failed treatment each year from 2014 to 2030 by NS5A versus non-NS5A inhibitors. NS5A, non-structural protein 5A.
Figure 6 shows the projected number of HCV patients alive after failing to achieve SVR after treatment with at least one HCV regimen (including non-DAAs). The number of such treatment-experienced patients dropped from 41 000 in 2014 to 2200 by 2030 in France, 31 000 to 1900 in Germany, 41 000 to 3400 in Italy, 37 000 to 1800 in Spain and 17 000 to 800 in the UK. The decrease in the number of treatment-experienced patients was primarily because of the availability of highly effective DAAs from 2015 onwards. By 2020, the type of treatment-experienced patients would differ substantially across countries. For instance, in France and Italy, the majority of treatment-experienced HCV patients would be those who have not failed on an NS5A inhibitor, and therefore would be eligible for retreatment with available NS5A inhibitors. However, in Germany and Spain, the majority of treatment-experienced patients would be those who have progressed to decompensated cirrhosis or hepatocellular carcinoma and thus could be ineligible for retreatment. Online supplementary figure S4 shows the 95% uncertainty intervals of these outcomes obtained from probabilistic sensitivity analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of patients alive between 2014 and 2030 who failed to achieve SVR after one or more treatments. SVR, sustained virological response, NS5A, non-structural protein 5A.
Between 2014 and 2030, 88 000 people who failed to achieve SVR with at least one prior treatment attempt (with pre-DAA or DAA) would develop decompensated cirrhosis: 11 000 (150 failed on at least one DAA) of those cases would occur in France, 12 000 (270 failed on DAA) in Germany, 31 000 (980 failed on DAA) in Italy, 25 000 (230 failed on DAA) in Spain and 8500 (70 failed on DAA) in the UK. During the same period, 80 000 people who failed to achieve SVR with at least one prior treatment attempt would develop HCC: 11 000 (110 failed on at least one DAA) of those cases would occur in France, 13 000 (190 failed on DAA) in Germany, 27 000 (730 failed on DAA) in Italy, 22 000 (180 failed on DAA) in Spain and 6900 (60 failed on DAA) in the UK.
Discussion
The advent of highly effective treatment for HCV with DAAs offers a unique opportunity to eliminate hepatitis C as a public health threat. In this modelling-based study, we simulated the clinical landscape of HCV treatment in five European countries: France, Germany, Italy, Spain and the UK. Our study provides several new insights that have not been previously reported. First, we projected that beginning in 2019, a growing number of people will be living with HCV cure. In fact, for the first time in the history of HCV, the number of individuals alive with cure will supersede the number actively infected individuals—Germany, Spain and the UK could achieve this milestone by 2020. As the cured population increases, disease management efforts focused on regular surveillance of persons with pretreatment advanced fibrosis or cirrhosis is important, as they remain at risk of developing hepatocellular carcinoma.
Second, there is a need for more aggressive HCV screening policies in Europe. The large population of patients will remain undiagnosed under current policies and they would be at risk of ongoing fibrosis development, a process that could be halted or reversed if they were able to reap the benefits of new DAAs. By 2020, most diagnosed patients would have received treatment and the number of people needing treatment will drop substantially, despite the fact that the burden of HCV remains high. Under current screening policies, the diagnosis rate in 2030 will be between 65% and 75% in the five European countries, which is substantially lower than the 90% target defined by WHO. Several countries continue to follow screening policies set prior to the era of DAAs. Recent evidence suggests that universal HCV screening with DAA treatment could be the most effective strategy to diagnose HCV30 31; therefore, such policy-level changes are immediately needed to reduce HCV burden in the era of DAAs.
Third, there is a need to increase the annual capacity for HCV treatment. The number of patients needing treatment exceeds the current treatment capacity in all five countries. When DAAs became available, these countries had several restrictions on who could receive treatment—Germany was most liberal from the beginning, but other countries initially treated only F4 patients, and then gradually included F3, then F2 and finally F0–F1. However, with prices of DAAs dropping in the last few years, more patients could be treated under existing budget constraints.32 HCV treatment has been shown to be not merely cost-effective but cost saving.5 6 Making low-price authorised generic DAAs available could further help in reducing barriers to scaling-up treatment uptake and to achieve greater cost savings.33 34 Therefore, increasing the budget allocation for HCV treatment provides an excellent public health as well as economic argument. This should occur in combination with removal of restrictions on the number of patients who can receive treatment.7 8 35 Under status quo, the treatment coverage in 2030 would reach between 65% and 74%, which (similar to the diagnosis rage) is substantially lower than the 90% coverage target defined by WHO.
Fourth, although the number of patients who fail on DAAs is relatively small compared with the undiagnosed HCV population, these patients could become a significant portion of the viraemic population in the future. Successful retreatment of these patients, who are already linked to care, could reduce the subsequent risk of decompensated cirrhosis, hepatocellular carcinoma and liver-related death. We projected, in the era of DAAs, a total of 1 324 000 people would receive treatment between 2014 and 2030 and 104 000 (8%) would fail to achieve SVR.
Finally, we observed outcome disparities between countries, which would necessitate policies tailored to the regional situation. For instance, the number of patients receiving treatment would remain steady in France and Italy until at least 2020; whereas, the number of patients receiving treatment would drop substantially in Germany, Spain and the UK by 2020, unless diagnosis rate is increased. Therefore, in France and Italy, low treatment rate is the bottleneck; whereas in Germany, Spain and the UK, low diagnosis rate is the bottleneck. Of note, Italy has a treatment uptake and diagnosis rate, however, the viraemic/non-viraemic projection for this country is less favourable compared with other countries. We also noted that in France and Italy, the majority of treatment-experienced HCV patients would be those who have not failed on an NS5A inhibitor, and therefore would be eligible for retreatment with available NS5A inhibitors. Therefore, timely retreatment of these patients could prevent adverse outcomes. However, in Germany and Spain, the majority of treatment-experienced patients would be those who have progressed to decompensated cirrhosis or hepatocellular carcinoma and potentially ineligible for retreatment. In these countries, routine surveillance for HCC could reduce HCV-associated mortality.
Our study has some limitations. First, we did not consider the possibility of fibrosis regression after SVR, which is unlikely to affect the results of our study but could have implications for post-SVR surveillance for hepatocellular carcinoma. Second, we did not consider the potential benefits of HCV treatment on reduction in extrahepatic mortality because of limited data. Third, we made assumptions about future treatment capacity, which could change over time. Fourth, we did not explicitly include resistance-associated substitutions in our model and assumed that patients who failed on second-generation NS5A DAAs could get treatment with the same class. Therefore, we could have underestimated the number of patients who fail on NS5A regimens. Fifth, we did not include HIV-HCV coinfection in our model, which is beyond the scope of the current work. Finally, we made assumptions that future HCV incidence rates remain relative stable in the countries analysed in our study. However, we evaluated a scenario where HCV incidence could rise. This scenario further necessitates the need for increased efforts targeted at timely detection and treatment of HCV.
In conclusion, we found that in the era of DAAs, the number of people with HCV who achieved a cure will exceed the number of viraemic patients. However, despite the availability of highly effective curative therapy for HCV, there still exists a large population of patients that remains undiagnosed and untreated. Some patients will remain viraemic even after multiple treatments and at risk of developing advanced liver disease sequelae. In order to avail full benefits of DAAs and to meet HCV elimination targets set by WHO, systematic changes at the policy level aimed at increasing the diagnosis of HCV, increasing treatment capacity and timely retreatment of patients who have failed on DAAs are needed in each country.
References
Footnotes
Contributors QC contributed to the study design, participated in data collection, developed the analytical model, performed statistical analysis, wrote the analytical plan, interpreted data and drafted and revised the paper. TA participated in the study design, interpreted data and participated in revision of paper. EB and FK contributed to the study design, participated in data collection, interpreted the data, drafted and revised the paper. XW participated in data collection, developed the analytical model, performed statistical analysis and drafted the paper. MR, YZ, SF and JP interpreted data and drafted and revised the paper. JC supervised the study, contributed to the study design, participated in data collection, interpreted the data and drafted and revised the paper.
Funding This research was supported by a research grant from Gilead Sciences.
Disclaimer The content is solely the responsibility of the authors and does not represent the views of the funders.
Competing interests JC received research grants and consulting fee from Gilead Science and Merck. TA received consulting fee from Gilead Sciences. SF has servered a speaker for Gilead Sciences, MSD, Abbvie, Bristol–Myers Squibb, Novartis, Bayer and Janssen. All other authors have nothing to report.
Ethics approval All data used in this modelling study were either publicly available or available in summary form and therefore this study did not require approval from an institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available. All data supporting the conclusions of the paper are included within the article or in the online supplementary material.
Patient consent for publication Not required.