Article Text

Abstract
Objectives To understand help-seeking by male victims of domestic violence and abuse (DVA) and their experiences of support services by systematically identifying qualitative and mixed-method studies and thematically synthesising their findings.
Design Systematic review and qualitative evidence synthesis. Searches were conducted in 12 databases and the grey literature with no language or date restrictions. Quality appraisal of the studies was carried out using the Critical Appraisal Skills Programme tool. Reviewers extracted first and second order constructs related to help-seeking, identified themes and combined them by interpretative thematic synthesis.
Setting DVA experienced by male victims and defined as any incident or pattern of incidents of controlling coercive or threatening behaviour, violence or abuse among people aged 18 or over who are or have been intimate partners or family members, regardless of gender or sexuality.
Participants Male victims of DVA.
Interventions Any intervention which provides practical and/or psychological support to male victims of DVA including but not limited to DVA-specific services, primary healthcare and sexual health clinics.
Primary and secondary outcome measures Qualitative data describing help-seeking experiences and interactions with support services of male victims of domestic violence
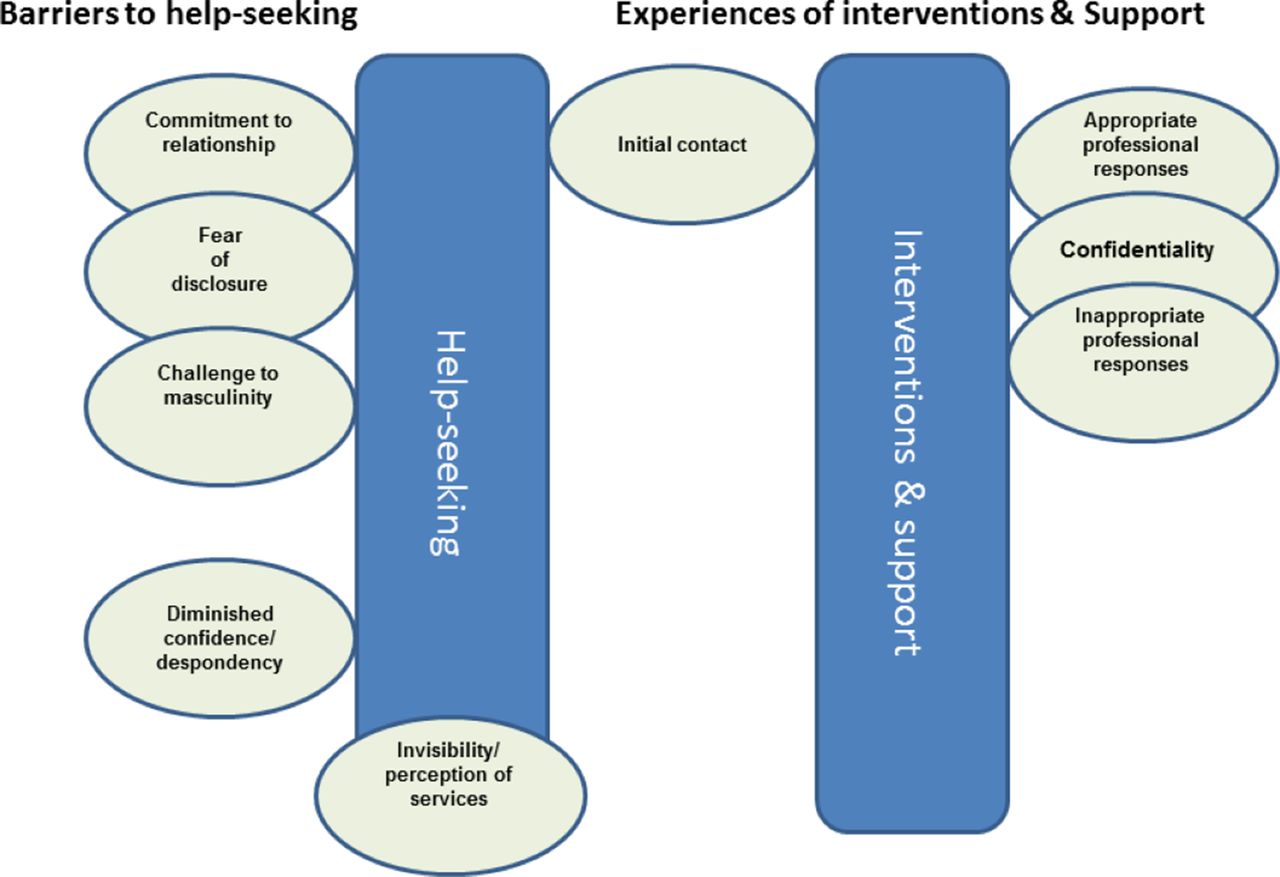
Results We included twelve studies which were published between 2006 and 2017. We grouped nine themes described over two phases (a) barriers to help-seeking: fear of disclosure, challenge to masculinity, commitment to relationship, diminished confidence/despondency and invisibility/perception of services; and (b) experiences of interventions and support: initial contact, confidentiality, appropriate professional approaches and inappropriate professional approaches.
Conclusion The recent publication of the primary studies suggests a new interest in the needs of male DVA victims. We have confirmed previously identified barriers to help-seeking by male victims of DVA and provide new insight into barriers and facilitators to service provision.
PROSPERO registration number CRD42016039999.
- systematic review
- qualitative evidence synthesis
- thematic synthesis
- male/men
- domestic violence and abuse
- help-seeking
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- systematic review
- qualitative evidence synthesis
- thematic synthesis
- male/men
- domestic violence and abuse
- help-seeking
Strengths and limitations of this study
This review employed established, rigorous methodology for systematic reviewing and qualitative synthesis.
All the included studies were recently published (2006–2017) and therefore likely to be relevant to the current situation of male victims of domestic violence and abuse.
The data extraction and assessment of full articles by two researchers’ generated themes, concordant between the review team in a transparent and reproducible manner.
The profile of men in the included qualitative studies was limited in that the participants were willing to talk about their experiences (self-selecting), they were predominantly white and within a relatively narrow age range of 40–60 years.
In the majority of studies, the currency of the abusive relationship(s) was not well recorded.
Introduction
Domestic violence and abuse (DVA) is a highly prevalent violation of human rights that damages health and well-being. For the purpose of this review we have used the UK intergovernmental definition of DVA: any incident or pattern of incidents of controlling coercive or threatening behaviour, violence or abuse between people aged 18 or over who are or have been intimate partners or family members, regardless of gender or sexuality.1
Although women experience more DVA than men and substantially more severe abuse, men in heterosexual relationships and men who have sex with men (MSM) can also suffer abuse from a partner, ex-partner or adult family member.2 3 Yet the needs of male victims of DVA have been comparatively neglected.4
Studies of male victims of DVA initially focused on survey data which described the type and severity of DVA experienced as well as providing numerical data on services accessed.5 As the problem of male victims of DVA has been acknowledged more widely in the literature, limited evaluation studies have been published, mainly in the grey literature describing support services for men.6 In recent years, there have been more qualitative studies conducted on the help-seeking experiences of male victims of DVA encompassing both heterosexual men and MSM and to lesser extent men of other sexualities.7
Our systematic review aims to address the gap in the review literature focusing on the qualitative research which explores the barriers to formal help-seeking and the experiences of all male victims of DVA with help-seeking services. This not only brings together data not previously collated and synthesised but also provides an evidence-based summary for future service development.
Methods
Overall strategy
The aim of the systematic review was to understand the help-seeking experiences of male victims of DVA. Our objectives were to systematically identify qualitative and mixed-method studies that reported qualitative data of men’s experiences of help-seeking, particularly with regard to services, and to thematically synthesise their findings.
Eligibility criteria of studies
Types of study
Qualitative studies and mixed-method studies were included. Mixed-method studies were only eligible if they reported qualitative findings separately. Eligible study designs included interviews, focus groups, ethnographies and observational studies.
Population
Studies were included which described male victims of DVA (≥18 years). The justification for limiting to ≥18 years is that between 16 and 18 years, although within the UK definition of DVA, there is a legal overlap with child maltreatment.1
Searches
A search strategy was devised in Medline using the eligibility criteria and modified appropriately for: EMBASE, CINAHL, CENTRAL, PsycINFO, LILACS, BNI, HMIC, ERIC, SSCI, Conference Proceedings Citation Index-Social Science & Humanities, IBSS and Social Services Abstract from their inception dates (online supplementary file 2). Searches were conducted on 14 March 2016 and updated on 9 June 2017. We searched the National Institute of Health Research (NIHR) Register, E-Thesis Online Service (for PhD theses) and www.who.int/trialsearch/ with keywords in March 2016 and June 2017. We contacted the authors of all eligible studies for further publications which may not be available in the public domain and performed forward (via Google Scholar) and backward (reference lists) reference searches of eligible papers to find any additional studies. In addition, the grey literature was searched in terms of examining relevant websites that may have described additional studies (eg, http://respect.uk.net/). There were no language or date restrictions.
Supplemental material
Reference management and data extraction
References were downloaded into Endnote and duplicates removed. Following the first round of searches in 2016, the screening included an extra step in which the first author performed an initial screen of the title/abstract removing any obvious female victim citations. The removal of these female victim citations was verified by the last author and the fifth author checking 10% of these choices: finding 100% concordance. This extra step was performed due to the lack of sensitivity of search terms for male victims of DVA which significantly increased the number of citations. The citations were then screened by two reviewers via title/abstract and then full paper by the first and second authors using our Population, Intervention, Control, Outcomes (PICO) criteria. Any disagreements were resolved by a third member of the team. In the update searches in 2017, the citations were screened by title/abstract by the first author and the full paper choice was verified by the fifth author.
Data extraction
Study demographics were reported into predefined tables by the first author. Qualitative data were extracted independently by two reviewers using customised forms, and any discrepancies were resolved by discussion with all the authors.
Quality assessment
Papers were critically appraised independently by two authors using the Critical Appraisal Skills Programme (CASP) tool.8 The appraisal decisions were discussed by all authors to ensure agreement. We used the appraisal to determine the applicability of the qualitative data to our aims, commenting on study design, recruitment techniques and whether the relationship of researcher to participants was reported.
Data synthesis
The findings were organised into first order constructs (verbatim views/experiences of research participants) and second order constructs (authors’ interpretations).9 A framework was devised with columns for these and a row for each article. We conducted data synthesis taking an interpretive thematic approach.10 All the authors met to identify and agree consensus on descriptive themes across papers, incorporating all the first and second order constructs. The themes were summarised, and patterns identified by the first author in order to develop overarching descriptive themes which remained very close to the constructs in the primary studies. These overarching themes were discussed and modified by all co-authors in face-to-face meetings and by email.
Patient and public involvement
There was no patient and public involvement.
Results
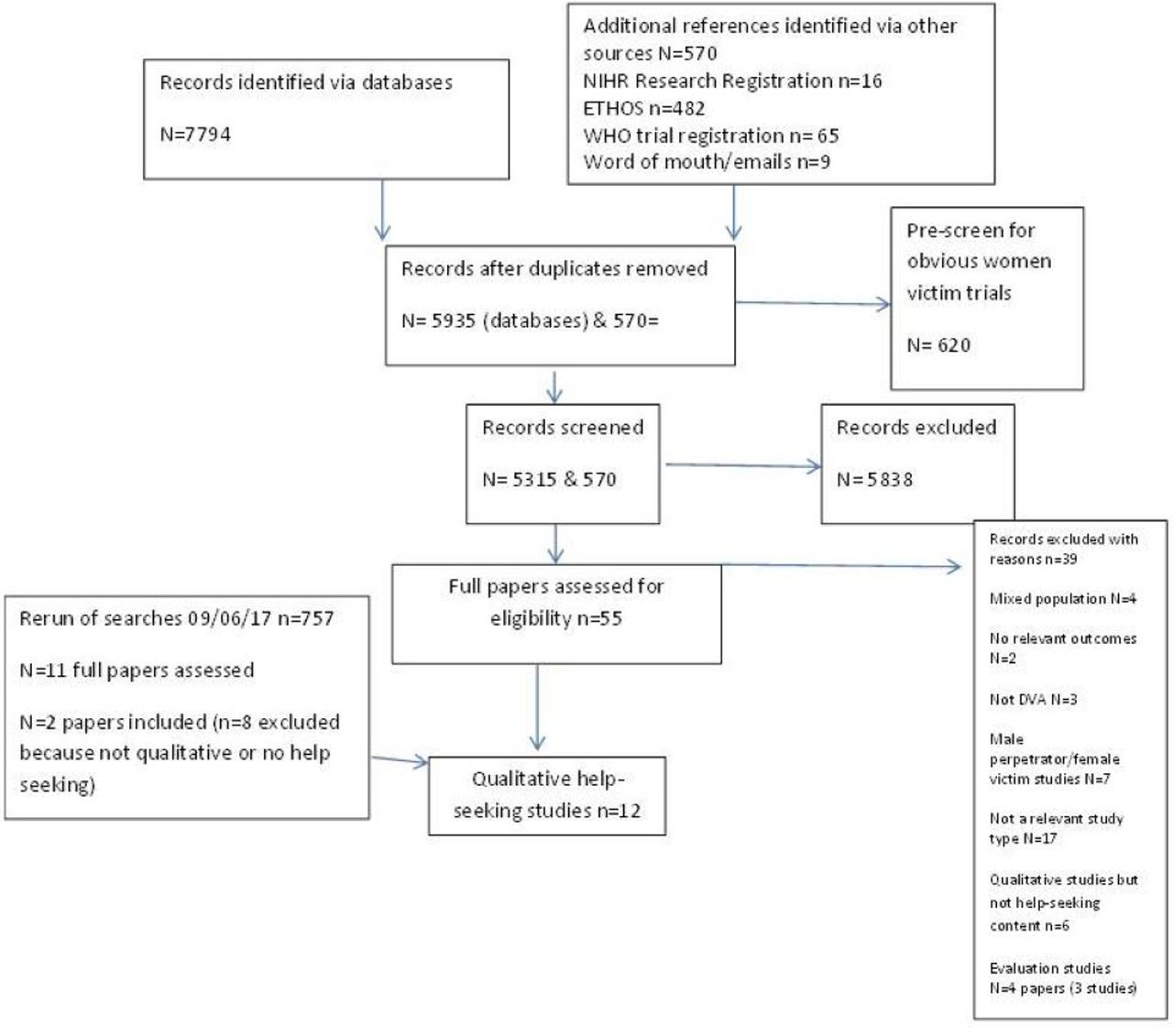
The searches identified 12 relevant qualitative studies (figure 1).11–22 Characteristics of studies (table 1).

Preferred reporting items for systematic reviews and meta-analyses flow chart. DVA, domestic violence and abuse.
Study characteristics
Six studies were conducted in the UK, four in the USA and one each in Sweden and Portugal and were published between 2006 and 2017. Five studies used mixed methods (survey and qualitative data).11 12 14 18 21 The remaining studies were all qualitative, employing interview methods.13 15–17 19 20 22 Six studies focused specifically on help-seeking14 16–18 20 21 and in the remaining six studies it was a significant part of the research.11–13 15 19 22
Quality of studies
Assessed with CASP criteria, the studies were generally well conducted. However two studies were predominantly quantitative in design,14 19 three studies had potentially inadequate recruitment strategies,14 19 21 only three studies considered the relationship between the researcher and participant11 13 15 and while eight of the studies described obtaining ethical approval for their research, in four studies there was no mention of ethical approval which could either mean they did not consider seeking approval but more likely they have not reported it (online supplementary file 3).13 16 17 21 Overall, ethical approval details were brief and ethical considerations were not elaborated on within all of the included studies. We know from the wider literature in the field that ethical considerations relating to the safety of potential participants and researchers is important.23 Therefore it is disappointing that these studies did not clarify how safety, confidentiality (and its limits) and signposting to services where appropriate, was administered during the research.
Supplemental material
Characteristics of study population
Seven studies recruited men via DVA or social and community services,12–16 19 21 one study recruited from the criminal justice system,17 two recruited from sexual health/HIV clinics11 22 and two from primary healthcare (table 1).18 20
Three studies recruited MSM (gay, bisexual and transgender men),11 13 22 five studies recruited heterosexual men,14–18 and four studies recruited men of diverse sexuality or did not specify sexuality.12 18 20 21
The majority of studies recruited men with a mean age between 40 and 60 years; four studies did not give any details although some specified an age range for recruitment.12 13 19 20 Ethnicity was recorded in six studies11 13–15 21 22 with most studies recruiting a majority of white men although Frierson focused on African-American men.13
The currency of the abusive relationship(s) was not well recorded, with the exception of three studies.14 15 19 Equally most studies included participants who self-reported having experienced DVA with little detail of duration, frequency or type of abuse experienced, although in one study the male victims were taking criminal proceedings against their former partner suggesting prolonged serious abuse.17
We described the themes over two phases (1) barriers to help-seeking and (2) experiences of interventions and support (figure 2) (table 2).
{kind=link}
{kind=link}
Thematic analysis.
Studies providing data for the themes and subthemes
Phase 1: barriers to help-seeking
We derived five themes on the barriers to initial disclosure and help-seeking by male victims of DVA. Three themes were closely related: fear of disclosure, challenge to masculinity and commitment to relationship in addition to the themes of diminished confidence/despondency and the invisibility/perception of services (figure 2).
Theme 1: fear of disclosure
This important theme emerged from ten of the twelve included studies of which two were focused exclusively on MSM (table 2).
There was a strong theme across the studies of difficult emotions experienced by male victims: internal fears, ambivalence related to shame and denial.13 15 20 21 This was expressed by both MSM and heterosexual men in the studies. In the study by Frierson13 in which gay African-American men were interviewed the author comments that ‘As the abuse continued, participants described being embarrassed to discuss the various aspects of their abuse outside of their personal networks. For some men they describe feeling as if they are less of a man if they report the abuse.’
One of the participants describes the internal struggle
Is this really going on? Am I in an alternate dimension? It was just that confusing… (Arelle) (Frierson, 2014).
This is also discussed by Tsui et al, ‘Men who have been assaulted by their intimate partners, either in same sex partner or heterosexual relationships, do not want to disclose their problems, in part because they wish to avoid additional problems. Although some may relate abuse to their own weaknesses, others blame their injuries on their own mistakes such as a careless fall or other accidents.’21 Self-perception and societal perception of masculinity is also an important factor in these fears. This is described in more detail in the theme of ‘challenge to masculinity’.
The external pressures surrounding the fear of disclosing DVA are significant and a multifaceted barrier for men discussing their situation with others. This related to perceptions about not being believed by informal or formal potential support.14 15 17 20 Seeking and receiving support from family and friends was generally perceived as beneficial. In Machado et al, 16 in which the authors interviewed male heterosexual victims of DVA, they reported how informal help-seeking leads on to formal help-seeking, but they also say ‘However, the overwhelming majority of participants rated formal sources as unhelpful, especially the services of the judicial system. Conversely, men reported that they had received valuable support from friends, family and colleagues at work.’
The other day, my neighbor saw me, and I was really down; she made me an appointment and took me to the doctor. (F., 43 years) (Machado, 2017)
A heterosexual participant when interviewed alluded to a fear of not being believed and the impact this can have on wider systems responses.17 This fear of not being believed by professionals was coupled with the fear of being falsely accused of being the perpetrator.
The professional [from social services] always treated me as if I was an offender. (M., 36 years) (Machado, 2017)
Men also feared the practical implications of disclosure, such as having nowhere to go, as well as the financial and professional impact. One of the most recurrent fears was losing custody of their children.14 15 20 This fear around the breakup of the family with children is related to the theme of victims’ commitment to their relationship.
In the Tsui et al study, in which men completed open-ended questions, men expressed the fear of putting themselves at future risk of harm from their partner by disclosing. The authors concluded that while ‘fear of [the] perpetrator’, and ‘threat of retaliation’, was not as frequently expressed as in abused women’s experience, fear was still regarded a factor blocking help-seeking among men.21
Theme 2: challenge to masculinity
Seven studies, one of which focused on gay African-American men describes the stigma of being a male victim of DVA on both a personal and on a societal level. Masculinity was linked closely in the papers under review with the fear of disclosure and internal pressures. A participant in the Hogan 2016 study said:
They won’t believe me you know, I mean I’m taller than my wife, you know I’m a big built fella you know, if I call up and say this is not, you know they just wouldn’t believe that (Simon). (Hogan, 2016)
This latter quote suggests that some people who may be physically bigger or perceived to be physically stronger than their partner, can feel that no-one would believe their disclosure of abuse. The assumption that abuse is mainly physical likely deters male victims to disclose experience of abuse. Similar experiences were expressed in the Frierson study of gay African-American men in which the authors state that ‘For some men they describe feeling as if they are less of a man if they report the abuse’.13
Theme 3: commitment to relationship
Two of the included studies of heterosexual men discussed commitment to their relationship and concern for the perpetrator of the abuse as both barriers to help-seeking.14 20 The desire voiced by study participants was for everything to be okay and ‘normal’. Men expressed wanting the abuse to stop, but not their relationship in which they were still emotionally invested. In some cases, concern for their female partner’s well-being took priority over their own.
‘For better or for worse,’ and, well, this was worse. I didn’t care that she was too psychologically disturbed to love me back, I didn’t care. I loved her. And I hoped I could get help for her condition before it was too late. (no id.given) (Hines, 2014)
Commitment to the relationship was closely linked to the fear of losing contact with children as described above in relation to fear of disclosure.14 15 20
Theme 4: diminished confidence/despondency
Three studies, one of which focused on MSM, explored diminished confidence.17 21 22 Both McCarrick et al and Valentine et al studies high-lighted the effect of diminished confidence influencing help-seeking behaviours and the potential role of post-traumatic stress disorder.17 22
It’s been 3 years now since I, I eventually got out the house but, them 3 years I might as well have gone to jail, because I’ve lived in a house and I very rarely go out now. (Lee) (McCarrick, 2016)
In the Valentine et al study, interviews with MSM showed that help-seeking was linked to self-realisation and self-preservation, for example, needing to protect one’s mental health.
I got depressed from it. I was starting to get depressed. And I had started seeing a therapist because some of the verbal [abuse], it was making me feel like—why am I, why would someone choose to stay with someone [like that]?’ (African-American/black, aged 44 years) (Valentine, 2013)
Complacency was related to the longevity of abuse in the Tsui et al study, leading older men to report in open-ended survey questions that they were less likely to seek help as abuse had been going on so long that it seemed futile or not worth doing anything about it.21
Theme 5: invisibility/perception of services
Three studies, two were focused on MSM, explored invisibility of male victims within services.11 13 17 These studies found that men were either not aware that services are available for them or that they did not perceive them as appropriate.13
It would have been certainly an out of body experience because it was certainly something, I couldn’t have imagined for myself. Again, especially as a man. A gay man. So, I- probably would have felt a little awkward about it all. I felt like they wouldn’t understand me because I was gay. (Terry) (Frierson, 2014)
The studies highlighted the importance of the ‘shop front’ of services. The need for a DVA gender-aware culture in services was discussed in both practical and policy terms.11 Some of the papers stated that separate services are needed if male perception of service availability is to be improved. The portrayal of DVA services as a space for women survivors was a barrier to help-seeking in the McCarrick et al study:
‘The headquarters of the DV unit has a massive billboard outside its building, ‘he’s a big hit with the ladies’ and it’s a man standing over a woman, hitting the woman.’ (Lee) (McCarrick, 2016)
To summarise barriers to help-seeking, fear of disclosure was an important theme, covering both the internal pressures of shame and denial and the external pressures of fear of not being believed, fear of being labelled the perpetrator and the practical (negative) consequences of disclosure. It overlaps with ideas of help-seeking being perceived as a challenge to masculinity and commitment to the relationship. There were less data from studies on MSM but experiences appeared to be comparable to heterosexual victims. Challenge to masculinity was also an important theme for MSM populations and describes the societal pressure of ‘being a man’ regardless of sexuality, although it should be noted only one study focused on gay men.
The two remaining themes in this section are more individual; the fourth theme sums up the hopeless of men in abusive relationship due to degraded confidence and responsibility and the fifth theme describes the perceived availability, and potentially the reality of available services for male victims of DVA both in terms of gender and sexuality.
Phase 2: experiences of interventions and support
Four themes emerged relating to experiences of interventions and support: initial contact, confidentiality, appropriate professional approaches and inappropriate professional approaches. Confidentiality is closely linked to ideas of the appropriateness of professional approaches (figure 2) (table 2).
Theme 6: initial contact—tipping the balance
Four studies explored the importance of the perceived levels of crisis; none of which focused on MSM12 17 18 20 These studies describe that a crisis often needed to happen before a man seeks help. Simmons et al described that ‘a sense of urgency to seek help and feeling ready to talk about one’s victimisation were strong factors that tipped the balance towards a high likelihood of disclosing victimisation, whereas a low perceived need for help tipped the balance towards a low likelihood of disclosure.’20 Family and friends were generally seen as a positive source of support whether that was associated with an initial acknowledgement or support further down the line.12 17 18 20
Had I not spent most of the day that I was arrested with a close friend who was able to identify my wife’s behaviour and advise me, I would have been in a psychologically weak situation when arrested. (Henry) (McCarrick, 2016)
Theme 7: confidentiality
Five studies emphasised the importance of confidentiality for men seeking help, two of the five studies focused on MSM.11 15 17 18 20 This need was expressed generally and in practical ways, such as valuing the provision of an appropriate private space for disclosure within a healthcare setting. Overall men’s primary motive was to keep their situation private. A heterosexual respondent in the Simmons et al study expressed doubt in the confidentiality of the health system within a small town.20 In the Frierson et al study in which gay African-American men were interviewed one participant said
‘I don’t think I would ever seek domestic violence help…’ It’s probably the way that I was raised. Like it’s a black thing. Whatever happens in your house stays in your house. People from the outside don’t need to know. Chuck, (Frierson, 2014)
There was relatively little information on the types of services that men preferred but in the Hogan 2016 study, a heterosexual man described the importance of the anonymity of the telephone.15
Talking to you is alright because we’re on the phone; I don’t know what you’re doing at the other side of the phone, but, if you was like, phew I don’t know, if you was looking at me, I don’t think I’d be looking at you when I’m talking to you (Stuart). (Hogan, 2016)
Religious mentors were described as important resources because they were considered non-judgemental and could be trusted although a participant in the Morgan 2014 study expressed doubts.18
It pains me to say it but I wouldn’t always trust the church’s approach to confidentiality (ID.1220030, aged 59). (Morgan, 2014)
Theme 8: appropriate professional approaches
Five studies explored the professional approach, one of studies focused on MSM.11 15 16 18 20 A preference for receiving help from a female professional was a consistent theme across studies and settings.11 15 18 20 Conversely there was little or no discussion around male professional support.
Studies in the healthcare settings suggested that continuity of contact (care) was favoured by men.11 18 20 Simmons et al proposed that in the caring encounter confidence could be built in just one session for some, whereas others required a longer term relationship for disclosure.20 According to Morgan et al a pre-existing relationship with the general practitioner facilitates disclosures by men.18 This was echoed by a MSM participant in the Bacchus et al study.11
When I come here I just want to get the job done and go. I probably may not have met that person before; I don’t want to start spluttering out all the things that have been going on. I now have a very good relationship with my HIV consultant and if he were to ask me that question, I would probably be much more open about discussing it with him. (Gabe, 33 years) (Bacchus, 2016)
The primary healthcare setting was regarded as a suitable and safe place to talk about violence by some, suggesting an overlap with the theme of confidentiality. Discussions with primary healthcare professionals around common physical and mental health symptoms associated with DVA seemed to facilitate disclosure. In the Simmons 2016 study the author described how a supportive, empathetic attitude from a professional opens ‘the door’ for disclosure.20 A heterosexual participant in the Morgan et al study speculated:
I think it’d probably be a good thing because I bet there’s a load of it going on all the time. Maybe people don’t even consider it abuse until they really question it like that. […]. [ID.1150023 aged 25] (Morgan, 2014)
Other views were at odds with this, with the suggestion by a man that non-medical professionals were more suitable to trigger and respond to potential disclosures.
…Definitely health advisor cos they are much more likely to have an empathic approach. And the doctors would be like ‘I don’t know which pill to give you for that. (Shaun, 52 years) (Bacchus, 2016)
While there was little content in the studies suggesting which interventions were preferred by men, Hogan 2016 suggested that counselling was acceptable to most men who had been victims of female-perpetrated violence.15 In the Machado et al study, two heterosexual men talked about the usefulness of being signposted to a psychologist from DVA services.
…I consulted a psychologist and it was good (…) It changed the way that I think and understand what was happening to me. (B., 35 years) (Machado, 2017)
Theme 9: inappropriate professional approaches
Six studies explored inappropriate professional approaches; one of which focused on gay men.12 13 15–17 19 Some negative comments were made regarding interactions with professional support. In the Hogan study, the authors described some men experiences as a ‘wall of silence’ from health professionals and ‘a lack of sensitivity and compassion’.15
Some participants described a lack of understanding from professionals towards lesbian, gay, bisexual, and transgender (LGBT) help-seekers, with a general feeling that services were ‘heterosexual-orientated’ with ‘gender stereotyped treatment’. One participant in the Frierson 2014 study talked about how a therapist had normalised abuse with in a gay relationship.
Something radiates off of a person’s body when they are uncomfortable around gay people. And that’s the feeling I get when I am the only gay person in a room. Even if people don’t know and I tell them that hey I date guys, they kind of just like eww. It could be me. (Chuck) (Frierson, 2014)
The men’s accounts of interaction with the police were polarised, with both positive and negative encounters.12 13 15 16 18 19
Hogan commented ‘a few (LGBT men) who did report to the police got a mixed response. Some had a sympathetic response but no follow through in terms of applying the law to the abusive partner. A small number had very unhelpful responses from the police though these said this had happened a long time ago.
When I did speak to the police they were like basically you’re two men, work it out. That it’s an abusive relationship but you know basically like why are y’all doing this? (Quin) (Frierson, 2014)
In the Morgan et al study, one man described how although the initial response from the police was supportive, there was no follow-up or signposting to further services.
Yes the police did arrive, they did take me seriously, they did follow-up etcetera etcetera but there was no, you know there was no, offer of on-going [support] to have a talk to the support line. They said what I had to do was call my lawyer up. (Participant 5) (Morgan, 2016)
Summarising the experiences of interventions and support; the theme of initial contact describes how many men get to a tipping point, generally a crisis or low point which leads to disclosure. It is unfortunate that none of the contributing studies include the views of MSM. Confidentiality is an important theme, describing the various forms it can take and relates to participants experiences of interaction with professionals.
A consistent element of appropriate professional response is that men appear to prefer to disclose and discuss DVA with a female professional. Primary healthcare professionals appear to be acceptable to male victims of DVA, but the study of gay African-American men suggests other professionals may be preferred. Participant’s descriptions of the criminal justice system are mixed but suggest that at best the police support is short term.
Discussion
In this systematic review, we have articulated nine themes in an exploration of barriers to formal help-seeking and the experiences of male victims of DVA with support services. From the review we have generated recommendations for policy and practice (box 1).
Recommendations for policy and practice
Service provision for male victims needs to be more publicly advertised.
Images and wording of publicity need to represent different types of masculinity and sexuality.
Service provision needs to be more inclusive and better tailored to more effectively address the needs of different sociodemographic groups.
Ensuring confidentiality and building trust in service provision is essential for male victims of domestic violence and abuse (DVA).
Continuity of contact (care) is an essential feature of services for male victims.
Services should aim to give all people seeking support for DVA a choice of professional personnel in terms of gender or sexuality.
Barriers to help-seeking are complex, but fear of disclosure is central, overlapping with the challenge to both men’s personal sense of and societal interpretations of masculinity and the importance of the relationship with the abuser. These factors contribute to diminished confidence and persistent despondency for some male victims of DVA. Masculinities as a field of study emerging from feminist scholarship and activism, has been used analytically to understand embodied practices and structural reinforcement of gender-based violence within patriarchal systems of power, articulating multiple positions men themselves occupy, including disadvantaged identities on the basis of ethnicity, class and sexual identity.24 25 While the perspective of masculinities has been used to understand the genesis and reinforcement of DVA experienced by women, the findings of our review suggest there has been little investigation of the relationship of masculinity to male DVA victim vulnerability, invisibility and help seeking. Josolyne’s interviews with heterosexual men who had experienced abuse from a partner highlighted the obstacles of a masculine identity to acknowledging abuse or a victim status.26 The DVA service providers in Wright’s interview studied repeatedly drew attention to masculinity in their explanation of the reluctance of men to seek support.27
Perceptions that men were invisible as victims within services points to a lack of an appropriate ‘shop front ‘of support, even those available to male victims. Two of our recommendations for practice are that service provision for male victims needs to be more publicly advertised and that images and wording of publicity needs to represent different types of masculinity and sexuality. Participants in the studies suggest that they reach a tipping point that leads to initial disclosure and help-seeking. Their subsequent help-seeking experiences highlight the importance of confidentiality and trust in its many forms. Their voices suggest that men anticipate and have experienced both appropriate and inappropriate responses from support services from which some preferences emerge.
Our review revealed that the experience of many male victims of DVA are comparable to the experiences of all victims of DVA; for example, fear of disclosure, shame and diminished confidence. Similar to women, although male victims wanted the violence to stop, they did not necessarily want to end the relationship.28 Men expressed concern about losing contact with their children; this is also a major theme within the female DVA literature.29 30
Male victims raised the importance of the continuity of relationship with professionals to whom they disclose and the quality and scope of interaction with those professionals. This is consistent with qualitative research with female victims.31 Our review also highlighted experiences that were specific to men. For example, fear of being accused of perpetration of DVA and challenges to masculinity.
While we know both men and women are reluctant to disclose DVA from fear of not being believed, there is an added barrier for men voiced in these studies that they may be falsely accused of being the perpetrator.17
Men raised wider concerns about masculinity. The perception that victims may have about negative reactions from family; friends and professionals may be reinforced by these behaviours.32 33 In our recommendations for practice we state that service provision needs to be more inclusive and better tailored to more effectively address the needs of all genders and socio-demographic groups. Furthermore, confidentiality and building trust in service provision is essential for male victims of DVA with continuity of contact (care) an essential feature of services for all victims. Our review highlights crisis points as an important trigger to help-seeking.17 18 20 Research suggests that even if a victim does not report/disclose abuse at the time of a crisis, a positive interaction with a professional can influence their decisions at a later date.34 This is similar for female victims and has resulted in the development of the policy and practice of ‘go-orders’ which are ‘intended to extend this window of opportunity to intervene with the victim and offer support’.35 This review highlights that men feel there is a lack of appropriate services for them.
Men raised concerns about the level of confidentiality in relation to professional services. Concerns about the inappropriate handling of confidential information have been also reported by women victims.36 Men voiced their preference for disclosing or talking about DVA to a female professional. This was not a consistent finding in a systematic review of women’s expectations of healthcare professionals.31 In that review of qualitative studies, some victims of DVA said that the gender of the professional was not important, as long as they listened and were supportive, whereas other participants in the reviewed studies preferred a female professional. Our final recommendation for practice is that services should aim to give all people seeking support for DVA a choice of professional personnel in terms of gender or sexuality
We have described how MSM participants generally found professional services were not configured for their needs and could respond inappropriately.
Strengths and limitations
The search for studies was systematic and exhaustive without language limitations and including the grey literature. We used prespecified inclusion and exclusion criteria and independent reviewers for inclusion and data extraction review was conducted. The critical appraisal and thematic synthesis followed established methodology.8–10 This is the first evidence synthesis of qualitative studies on the experience of help-seeking by male victims of DVA and our thematic findings on the interaction with professional services adds to the evidence base.
The limitations of this review are that not all dimensions of the topic are covered by these qualitative studies, for example, ethnicity and cultural barriers to help-seeking by men. Throughout this systematic review we have used the term men who have sex with men (MSM) as we recognise that some men may not identify as gay or as in a same-sex relationship even when they do have sex with men. However, in the Frierson study which clearly defines its participants as gay men we have kept this description. We acknowledge however that MSM is a contentious term and that further refinement of terms is needed.37 It is also important to point out that these qualitative studies have captured the voices of those who were willing to come and speak to someone, whereas more anonymous methods might have yielded some different findings. While we do not have empirical evidence this could have an impact on disclosure figures.
Conclusion
This paper reports a systematic review and qualitative thematic synthesis of help-seeking and interactions with services by male victims of DVA. The thematic analysis confirms previously identified barriers to men seeking help and provides new insight into barriers and facilitators to successful professional advocacy and service provision with recommendations for practice. It would seem that services need to be inclusive, to cater to diverse client groups, to involve ongoing support and to be widely advertised. In addition, specialised training is required to address the specific needs of men and to foster greater levels of trust.
Supplemental material
References
Footnotes
Contributors ALH was involved in protocol development and led on both the systematic review and synthesis of data. She co-wrote the final paper with all the other authors. LP was involved in protocol development, screened references with ALH in the systematic review stage, was involved in the discussion of the data and qualitative synthesis and contributed to the final content of the paper. EW was involved in protocol development, discussion of the data, qualitative synthesis and contributed significantly to the final content of the paper. AM was involved in protocol development, the discussion of the data and advised on and was involved in the qualitative synthesis. She commented on the final content of the paper. ES was involved in protocol development, checked the initial screening of references in the first round and in the rerun of the search strategy, was involved in the discussion of the data and the qualitative synthesis, and contributed to the final content of the paper. GF was involved in protocol development, checked the initial screening of references in the first round, was involved in discussion of the data in the qualitative synthesis and contributed to the final content of the paper.
Funding This paper presents research funded by the National Institute for Health Research (NIHR) as part of their Programme Development Grant for Applied Research (PGfAR) scheme (RP-PG-0614-20012).
Disclaimer The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Full data extraction and synthesis data are available from the authors.
Patient consent for publication Not required.