Article Text

Abstract
Objective The goal of this study is to assess the correlation between protection of women’s economic and social rights (WESR), health improvement and sustainable development.
Methods A cross-country analysis of 162 countries was employed to assess development, health and human rights of the countries by measuring associated variables. Data sets for the health, human rights and economic and social rights of these countries were from 2004 to 2010. The dependent variables are health and human development and the independent variables are the human rights variables. Regression analysis and principle axis factoring were used for extraction and varimax method for rotation. Country grouping was made using cluster analysis. Potential biases, resulting from measurement differences in human rights values, were eliminated by using z-transformation to standardise variables.
Results Regression results reveal that WESR variable is correlated with the health outcomes. Cluster analysis separated the countries into three clusters, based on the WESR variable. Countries where WESR were ‘highly respected’ (44 countries) are categorised into cluster 1; countries where WESR were ‘moderately respected’ (51 countries) are categorised into cluster 2 and countries where WESR were ‘poorly respected’ (63 countries) are categorised into cluster 3. Countries were then compared in their respective clusters based on health and human development variables. It was found that the countries which ‘highly respected’ WESR had better average health values compared with the second and third clusters. Our findings demonstrate that countries with a strong women’s rights status ultimately had better health outcomes.
Conclusion WESR status has correlation with the health and human development. When women’s rights are highly respected, the nation is more likely to have higher health averages and accelerated development.
- global health
- human rights
- women’s economic and social rights
- health policy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of of this study
The study uses cross-country data from 162 countries to reveal connections between women’s rights and health using quantitative tools.
A major strength of the study is that the regression analysis and exploring country differences by cluster analysis reveal similar results, thus contributing to the robustness of the study.
Another strength is that the study presents evidence on the distinction between International Covenant on Economic, Social and Cultural Rights and The Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW) and that CEDAW ratification does not affect women’s rights.
A major weakness is that the data used are average values of the health and human rights variables for the 2004–2010 period. The period included the most complete available data set for the 162 countries.
Due to some of the missing values in the data set, the researchers used average values which may reduce the variability of the data.
Introduction
Human rights, health and economic development have distinct long histories, which gained attention during the decolonisation in the 1960s and the end of the Cold War in the 1990s.1 Some practical examples of health, human rights and development pertain to HIV/AIDS as well as reproductive and sexual health concerns.2 3 The definition of development as a qualitative change in environmental, social and economic principles has close links with human rights and the value of being human. Both civil and political rights (CPR) and economic and social rights (ESR) are deeply interrelated with the right to development.
The Millennium Development Goals (MDG) were created to eradicate several looming problems that threatened progress internationally for optimal health and development in a 25-year plan. After ending the MDG in 2015, the follow-up Sustainable Development Goals (SDGs) aim to maintain growth and reach those countries with low health and development rates. This is done by targeting human rights-oriented goals. In fact, the need for a SDG arose from the lack of emphasis on human rights in the MDG. For instance, Goal 3 of the SDG, ‘Ensure healthy lives and promote well-being for all at all ages’, Goal 5, ‘Achieve gender equality and empower all women and girls’ and Goal 10, ‘Reduce inequality within and among countries’.4 In doing so, the SDG assumes two components of human rights, the CPR and the ESR. Furthermore, these goals extend to women. Thus, altogether combined, the SDG manages to truly impact the promotion of women’s rights and development.
Civilly, there are many charters and documents that acknowledge women’s rights. These include the ‘Maputo Protocol’, the Arab Charter on Human Rights, the Inter-American Convention on the Granting of Civil Rights to Women, the Inter-American Convention on the Granting of Political Rights to Women and the International Covenant on Civil and Political Rights.5 6 Many of the regions in the world have progressed economically through participation in multiple organisations whose objective often omits women as a crucial factor in their plans.7 8 Thus, women’s ESR (WESR) is often stagnated in many of the countries in these regions. Despite their contributions, WESR and CPR seem to be often overlooked. This has a severe impact on women’s health and development.
Promotion of CPR is not sufficient in paving the way for health and development. Of the 30 countries with greater than 30% female parliament members, regional Africa hosts a third of those nations.9 One would assume a state with a high indicator of women’s CPR (WCPR) would also have a high ranking in development and WESR. Yet, despite this, the region of Africa does not share the developmental progress its indicators foreshadow. Limited accessibility to the three capitals: financial capital, human capital such as skills and experience, and social capital such as networks and communities could deprive women of the opportunities they need in order to impact the sustainable development of the nation.10 While states with history of WCPR can find change in WESR to be more easily facilitated,11 a greater cooperation between states and the UN agencies is necessary for new policies to make health and development a global priority with respect to WESR. In this respect, a turning point was the 1994 International Conference on Population and Development. Correspondingly, United Nations Population Fund (UNFPA) links human rights with sexual and reproductive health and reproductive rights. The UNFPA approach is centred on the view that human rights system is related with reproductive health.12 Given that women make up approximately half of the population, and their higher morbidity rates on average,13 a lack of ESR also prevents optimal health and retards them from partaking in a nation’s gross domestic product, social services and, in turn, injures development.
In redesigning health policies with these implementations, it is important to know the extent to which different human rights issues impact health outcomes and development. For example, it is important to know whether one set of human rights issues, such as ESR, have greater impact on health than another set of human rights issues such as CPR. Furthermore, one must understand the gender disparity on the protection of women with respect to ESR and CPR so their ramifications on health and development can be explored. This may provide states a framework in structuring and placing special emphasis on certain women’s rights policies for enhanced progress of health outcomes and development.
Interestingly, many countries have legal documents enshrining women’s rights. However, despite these legislative tasks, WESR are still left wanting. The Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW), an international bill of rights for women, consists of 30 articles that define what constitutes as discrimination against women alongside setting up regulations against such actions in an attempt to alter the gender disparity with limited success.14 Discrimination against women is noted as any distinction, exclusion or restriction made on the basis of sex that impairs the recognition, enjoyment or exercise by women. The states that ratified CEDAW are required to ensure gender equality into their legislation, repeal all discriminatory provisions and must take steps to eliminate all forms of gender discrimination.13
The strengthening of female rights would be in the best interest of men and society, due to the complex relationships that connect men and women. Ratified by 187 nations, the CEDAW has not influenced awareness on the importance of women’s rights. To this extent, the SDG should take into consideration the benefits reaped from fulfilled women’s rights and learn from the shortcomings of the MDG and CEDAW. It is imperative to understand the relative impact of different human rights issues on health outcomes and development. Concerning the global issues pertaining to reproductive and sexual health, women have been instrumental in making the connections between health and human rights.
This study aims to contribute to the larger field of human right empiricism in global health. The field began with an article in the Lancet a decade ago,15 after which the human rights community criticised the methodology of the study.16 The works eventually gave rise to the Hunt and Bustreao monograph.17 The monograph was only the start of a larger effort to examine the public health impact of human rights and a stream of literature exists on correlation of health and human rights. For a brief review on the current literature, see, for example, Todres18 and Forman, Kenyon and Brolan.19 The aim of this study is to contribute to the larger literature on human rights and health by specifically examining the correlation between protection of WESR and health outcomes in comparison to ESR and CPR. The aim is to investigate the correlation of women’s rights separate from the role of ESR and CPR on achieving improvements in health outcomes.
Methods
Variables
The study employs data from a cross section of 162 countries across different geographies. The development variable is operationalised by the human development index (HDI) developed by the UNDP. It includes and captures three major capabilities: access to long life (longevity), access to knowledge and access to a decent standard of living. The HDI is a measure of average achievements in key issues of human development. When looking at it from a human rights perspective, all the key variables for development must be assessed in order to determine usefulness and accuracy of data. This study employs the HDI released in 2010 by the UNDP by utilising the average value of HDI for the years between 2004 and 2010.
The variables operationalising health are from World Bank, World Development Indicators (WDI) Database (The World Bank, 2014). The WDI database includes cross-country data for a wide range of health variables with subheadings, risk factors, nutrition, disease prevention, mortality, reproductive health and health systems. From the database, the researchers chose variables that represent disease prevention, mortality and health systems. The selected variables are as follows: ‘mortality rate under 5 (per 1000 live births)’; ‘mortality rate neonatal (per 1000 live births)’ (MORT_NEO); ‘immunisation of diphtheria, pertussis and tetanus (DPT) (% of children ages 12–23 months)’ (DPT); ‘immunisation of measles (% of children ages 12–23 months)’; ‘number of hospital beds per 1000 people’ (HOSP); ‘number of physicians per 1000 people’ (PHYS); ‘lifetime risk of maternal death (%)’; ‘improved sanitation facilities (% of population with access)’ and ‘life expectancy at birth’ (LIFE_EXP).
There are two categories of variables that operationalise human rights. The first set of variables operationalises CPR. These are as follows: ‘Physical Integrity Index’ (an additive index constructed from the Torture, Extrajudicial Killing, Political Imprisonment and Disappearance indicators; ranges from 0 [no Government respect] to 8 [full government respect]), ‘Empowerment Rights Index’ (an additive index constructed from the Foreign Movement, Domestic Movement, Freedom of Speech, Freedom of Assembly & Association, Workers’ Rights, Electoral Self Determination and Freedom of Religion indicator; ranges from 0 [no Government respect] to 14 [full Government respect]), ‘Women’s Political Rights’ (WOPOL) (a score from 0 to 3 depending on the level of political rights for women) and ‘Independence of the Judiciary’ (a score from 0 to 2 depending on the level of independence). All the CPR data for the 162 countries were obtained from the Cingranelli-Richards (CIRI) Human Rights Data set. The data set is open access and does not require permission for use since it is publicly available. Ethics approval was therefore not required. The CIRI database was chosen since the variables reflect the CPR variables that are parallel to the International Covenant on Civil and Political Rights.
The second set of variables on human rights operationalises economic, social and cultural rights that follow the terms and requirements of the International Covenant on Economic, Social and Cultural Rights (ICESCR). The definition suggests that countries are obligated to devote the maximum of their available resources to progressively realise the substantive rights enumerated in the ICESCR. We use the data from Social and Economic Rights Fulfillment (SERF) index of 162 countries covering all but high-income Organisation for Economic Co-operation and Development countries (Core SERF index). SERF index operationalises economic, social and cultural rights (ESCR) that follows the terms and requirements of the ICESCR. The core country index consists of the right to food (% of children under 5 years not stunted) (FOOD); right to education (primary school completion rate; combined school enrolment rate) (EDUC); right to health (contraceptive use; child under 5 years survival rate; age 65 years and over survival rate) (HEALTH); right to housing (% of rural population with access to improved water source; % of population with access to improved sanitation) (HOUSE) and right to decent work (% of population with income greater than $2 per day) (WORK). The variables used for the core index and supplemental index are not the same so it is neither possible to compare nor merge the two series (Fukuda-Parr, Lawson-Remer and Randolph, 2011). We use the following core index for the study: ‘women’s economic rights’ (a score from 0 to 3 depending on the level of economic rights for women) and ‘women’s social rights’ (a score from 0 to 3 depending on the level of social rights for women) are obtained from CIRI Human Rights Dataset.
Given the principle of progressive realisation, the researchers used a control variable in the regression model. The aim is to account for the role of economic resources for enabling access to health services and products. We use per capita (pc) current health expenditures (CHE) adjusted by purchasing power parity (PPP) in international dollars (CHE_pc_PPP). The data are from the WHO data set for the years 2004 and 2010. The variable measures the average capital, including domestic general government, private and external source health expenditure, per citizen of a country spent on healthcare goods and services during a year after adjusting by PPP.
For purposes of consistency, we took the overlapping years (2004–2010) for the different data sets described above and used average values for all variables on a sample of 162 countries that represent different geographies across the world. Note that in the analysis it was not possible to use the whole set of countries due to missing values.
Analysis Methods
One way to explore the correlation between human rights issues and health or human development is to use regression analysis. The aim is to account for different human rights issues in an econometric model to explore the distinctive effects of human rights variables on health and human development. Here, the dependent variables are the selected health variables and HDI. The independent variables are human rights variables and the control variable is CHE_pc_PPP. In order to overcome the problem of multicollinearity, also reflecting the unobserved latent factors of these variables, we use factor analysis to reduce the number of human rights variables. We use principal axis factoring for extraction and varimax method for rotation. In regression model, we used factor scores to represent different and independent dimensions of human rights variables.
In order to explore whether there are systematic variations across countries, the researchers grouped the countries according to different levels of women’s rights. The country grouping is made using hierarchical cluster analysis. Cluster analysis is a class of techniques used to classify objects or cases into relatively homogeneous groups called clusters. Objects in each cluster tend to be similar to each other and dissimilar to objects in the other clusters. The aim of the cluster analysis is to classify the countries into dissimilar human rights groups in order to see whether countries that are grouped according to distinct human rights variables also differ in health and human development variables. The analysis aims to reveal systematic differences in health and human development variables within the clusters that are formed using different issues of women’s right variables. In order to eliminate potential biases in cluster analysis due to differences on measurement of the human rights values, we use z-transformation to standardise the variables.
Patient and public involvement
In this study, patients and public were not involved. The data consist of secondary data as described above.
Results
Factor analysis reduces the number of human rights variables into three factors. We use the scores of the factors that represent ESR, CPR and WESR as independent variables in the regression model. As described above, CHE_pc_PPP is the control variable and the dependent variables of the regression model are the health outcomes and HDI.
Regression analysis reveals that all health variables and the HDI index are positively correlated with ESR. The WESR has an additional positive correlation with many of the health outcomes, except for HOSP and PHYS (the health variables that represent variations in health systems across the nations). This can be interpreted as, given that the ESR is sufficient in a country, the citizens would have access to hospital beds and physicians and there is no additional role of WESR.
CPR variable does not show correlation with many of the health outcomes. The only health variables that are significantly affected by CPR are vaccination variables. CPR predicts improved sanitation facilities as well; however, it is not in the expected direction. Moreover, the CHE_pc_PP variable is correlated with all health outcomes except for the vaccination variables. Regression results are presented in table 1.
Regression results (dependent variables: health variables and HDI)
Cluster analysis reveals three country groups with different WESR levels. These clusters are as follows: cluster 1 WESR ‘highly respected’ (44 countries), cluster 2 WESR ‘moderately respected’ (51 countries) and cluster 3 WESR ‘poorly respected’ (63 countries) (table 2). The averages are statistically different from each other. Scheffe’s method for post hoc analysis confirms that WESR variables are able to divide the countries into three meaningful clusters.
Comparison of WESR clusters variables among different clusters
The health variables across the WESR clusters show the expected pattern. The health variables improve for country groups where WESR are highly respected and deteriorate for country groups where WESR are moderately and poorly respected (table 3). Countries in cluster 1 (highly respected) have consistently superior average values than clusters 2 (moderately respected) and 3 (poorly respected). The post hoc analysis shows the difference between the health values of Clusters 2 and 3 are ambiguous for the most variables, except for MORT_NEO and HDI.
Comparison of different health variables among different WESR clusters
The first part of table 4 presents health outcomes for the countries where ESR, WESR and CPR are all highly respected. In this group, only one European country (Bulgaria) has all human rights variables averaging higher than the sample average. The other countries with highly respected human rights belong to the Inter-American human rights system (six countries) or the Asian human rights system (one country), where all but one variable (the variable that measures health systems: access to hospital beds and physicians) are higher than the sample average. This result implies that although access to hospital beds and physicians is insufficient, highly respected human rights may still lead to improved health outcomes.
Health outcomes for the countries where both sets of human rights (ESCR and CPR) are highly respected
The second part of table 4 includes countries where ESR and WESR are highly respected with low CPR. Here, we see two groups of countries both of which include countries from Inter-American, European and Asian health systems. Some countries have all health outcomes higher than the sample average while some partly have health outcomes lower than the sample average. The results imply that even with poorly respected CPR, we generally see improved health outcomes.
The third part of table 4 includes countries where CPR is highly respected. The countries in Inter-American and European health systems have better health outcomes. However, in sub-Saharan African countries where CPR is highly respected, we see inferior health outcomes.
In summary, table 4 shows only one European country where all three dimensions of human rights are high and has health outcomes superior to the sample average. For the rest of the group, where the CPR, ESR and WESR are highly respected, all health outcomes, except for health system variables (hospital beds and physicians), are consistently better than the sample average. The results confirm that even with a lack of resources, if the country has strong human rights structure, the health outcomes are better. It is not possible to make similar interpretations for the countries with only highly respected CPR. The countries with high CPR and superior health outcomes belong to European and Inter-American health systems where access to health services is easier and the quality is much better. The countries with high CPR and poor health outcomes belong to sub-Saharan African health system where nearly all aspects of health measures are inferior to the sample average.
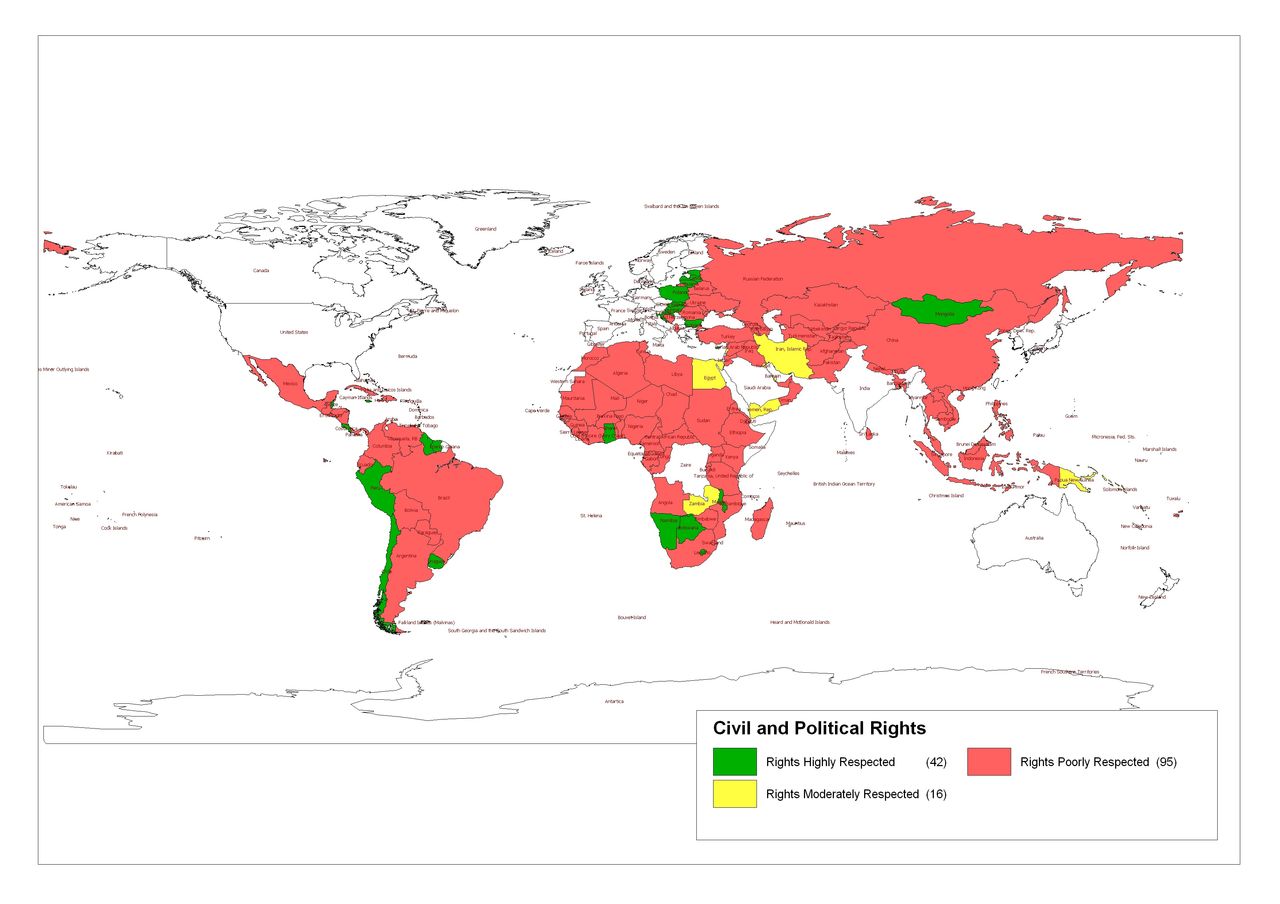
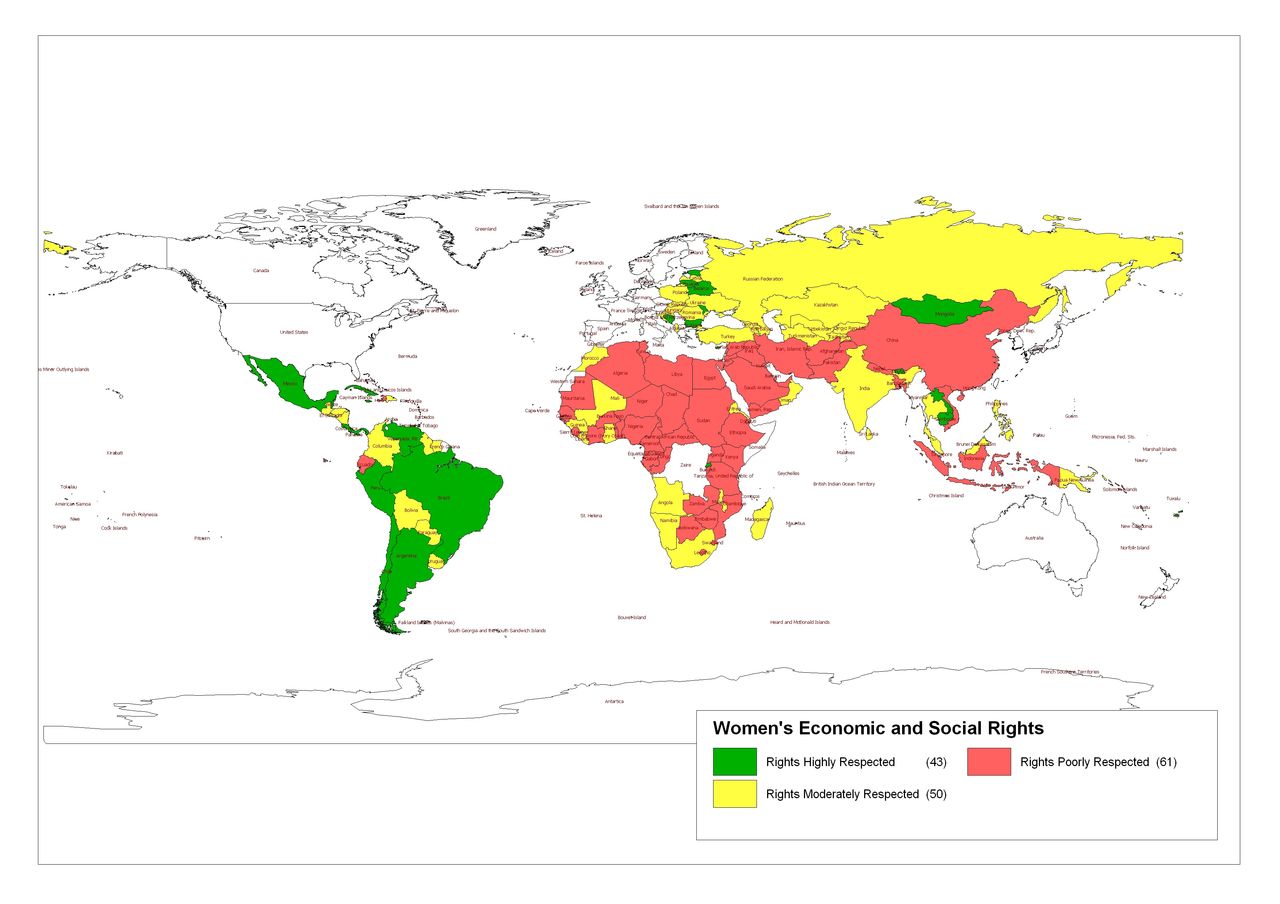
Figures 1, 2 and 3 show countries with varying levels of human rights according to ESR, CPR and WESR. The map demonstrates that the countries do not show a similar pattern with respect to human rights classification. CPR is poor in the majority of countries and high in European and Inter-American countries. ESR is highly respected in the Inter-American region, Asia and North Africa. WESR are highly respected in the Inter-American region as well but not in South Eastern Asian countries that are mostly dominated by conservative societies. Given high levels of WESR, even with low numbers of physicians (human resources for health) and low hospital beds, the health outcomes are superior to sample average.

Economic social and cultural rights. Green, rights highly respected; Red, rights poorly respected; Yellow, rights moderately respected.
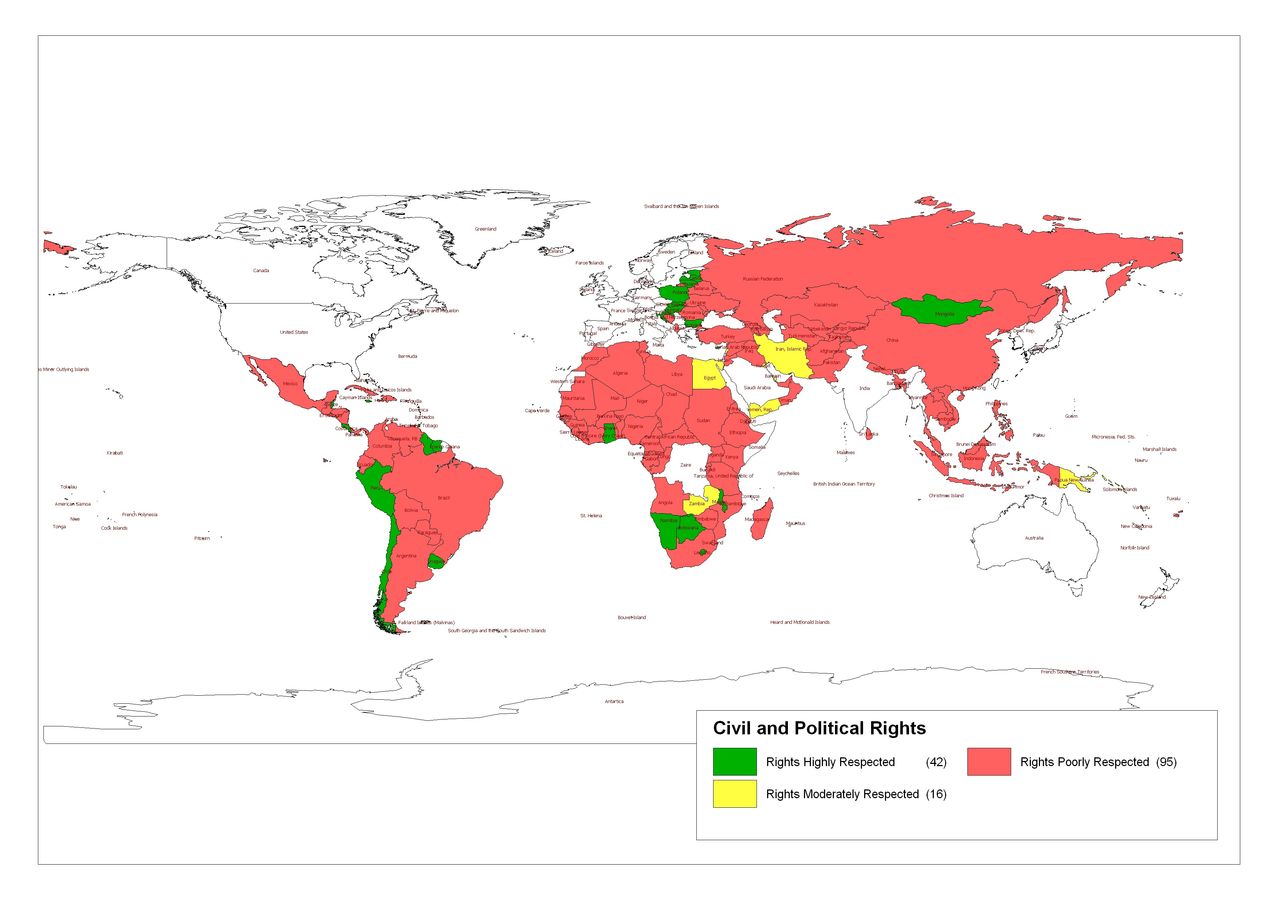
Civil and political rights. Green, rights highly respected; Red, rights poorly respected; Yellow, rights moderately respected.

{kind=link}
{kind=link}
{kind=link}
Women’s economic, social and cultural rights. Green, rights highly respected; Red, rights poorly respected; Yellow, rights moderately respected.
As described in the Methods section, the data set for this study includes HDI variable, health variables, CPR variables, ESCR variables of countries from different data sources. Also, as mentioned in the Methods section, the missing values do not allow us to use the whole set of 162 countries for statistical analysis. Although the data set as a whole includes a total of 162 countries, the missing values for the HDI, health, CPR and ESCR variables represent variety of different countries where at least one of the observation is not available. For example, the cluster analysis for this paper was done using two variables regarding women’s economic rights: WECON and WOSOC where the number of observations of WECON was 160 and the number of observations of WOSOC was 158. Since the cluster analysis omit missing data, the total number of countries used in the cluster analysis is 158.
Discussion
Principle Findings
The results of the regression analysis reveal that while WESR and ESR are correlated with health outcomes, the predictive power of the CPR variable in explaining variations in health outcomes is weak. Moreover, health system variables such as number of hospital beds and number of physicians are better explained by per capita health expenditures but not by women’s rights. All other health outcomes are correlated with the WESR variable. Cluster analysis results are consistent with the results of the regression analysis and show that promotion of women’s right is significant in explaining health outcomes.
Our findings further demonstrate discrepancies across nations with respect to the gender divide, despite having signed, or more importantly, ratified CEDAW. The findings of the cluster analysis show that despite high level of ESR, respect for women’s rights is low for some countries. For example, although Algeria, Egypt, Iraq, Syria, Iran, China and Indonesia have high respect for ESR, the cluster analysis results show that these countries have poorly respected WESR. Similarly, Morocco and Turkey have high ESR but moderate WESR, whereas Yemen and Pakistan have moderate ESR but low WESR. Since the promotion and protection of women’s rights play a fundamental role in progress for states as they unite health, human rights and development, nations that have the ability to promote WESR, as evidenced by their support of ESR, are missing a crucial component in positive health outcomes.
Thus, CEDAW has not shown to be very successful in altering the disparity in the aforementioned states. Although states have acceded the bill and have agreed to the specific mandates, they still show poorly or moderately respected WESR. The majority of nations with highly respected ESR have signed ICESCR and have followed those regulations. However, the countries with highly respected ESR may show poor WESR. The ICESCR defines a broad set of rights that all states must provide to their citizens that pertain to housing, education, cultural rights (eg, language and religion), as well as self-determination.
Findings in relation to other studies
The idea that CEDAW ratification does not necessarily entail implementation of women’s rights is no new finding in the literature. In fact, a larger frame of literature has also seen similar trends. In an attempt to emphasise the dual edge of international bodies, Dutton found that, statistically, even countries with the worst practices would sign international human rights legislature if the ‘treaty mechanisms are too weak for the states to view them as a credible threat to their sovereignty’.20 Similarly, the study found that in treaties with strong enforcement mechanisms, such as the creation of the International Criminal Court with an independent Prosecutor and Court, states are only willing to join if they are willing to comply, as ‘states with poorer records are significantly less likely to commit’.16 This study complies with our findings, as many states have ratified CEDAW, yet have poor implementation of WESR. According to Dutton,16 this may be due to the fact that CEDAW lacks strong enforcement mechanisms.
One of the core works of human rights literature, The Power of Human Rights details the conditions under which theories of human rights may be converted into practice, most commonly known as the spiral model.21 The model stress the need for transnational regimes that can normalise human rights practices in individual states and how these networks may affect violating behaviour through five phases. Phase four of this model claims that international regimes may be able to coerce states through various forms to more liberal policies or government and administrative changes.17 In an attempt to understand the course of human rights behaviours through quantitative research, Beth Simmons claims that such detailed methodological theories may not be effective in changing enforcement tactics. Rather, Simmons claims that understanding the disconnect between theory and practice, through quantitative data, can encourage change through adjusting the problems that are already prevalent.22
The findings within this study, therefore, further contribute to the literature by displaying the lack of enforcement in women’s’ rights, specifically WESR, despite ratifications to transnational treaties such as the CEDAW. This fortifies the idea that, though the spiral model may have been one of the most carefully executed treaties of the time, mainstream research, specifically quantitative research, has shown the shortcomings of current regimes. Thus, our study adds to the current literature that continues to show the unambiguous relationship between treaty ratification and human rights implementation.
The disparity between CPR and ESR among the general population in several countries correlates with women’s rights and may impact development. Per the Gender Gap Report in 2016, economic participation and opportunity for women have been inconsistent since 2006 and have steadily declined since 2013.23 Since 2006, the rate of WCPR has steeply inclined, especially after 2013, which shows a discrepancy between WCPR and WESR. Political empowerment for women has no direct impact on their ESR as indicated by the opposing trends since 2013.19 The disparate statistics between ESR and WESR show that a shortcoming in WESR can result in low-paying jobs for that are stereotypically feminine, or even unemployment for many women.24 For instance, occupations such as teachers, which offer relatively static salaries could restrict women financially.25 Given the lack of access to healthcare, whether it be due to deficiencies in transportation, financial shortfalls or inability to acquire beneficial goods and services, health largely parallels economic status. An indication of how economic curtailment affects women’s health is that individuals with higher incomes, regardless of gender, have a lower mortality and morbidity rate as compared with those with overall lower incomes.26
The gradient between socioeconomic status and health can be detrimental for the public. In order to treat growing numbers of unhealthy women, who cause financial pressure, governments would need to allocate higher amounts of funds into public health and, in turn, elicit heavier taxes.22 These taxes would harm morale and aggravate the gradient between health and economy further. Economic status for both men and women would decrease and health will follow. Health has the highest global gender gap with a nearly 100% disparity while economic disparity is 60%.27 Despite all this, the gender gap for politics has been steadily narrowing closing almost 80% of the gap in some nations.28 WCPR are important in society; however, development cannot be sustained if the trend of WESR is not changed.
There are many global problems that overcast the bright light of development throughout the world. Reproductive health and maternal and infant care are a huge health concern. One of the leading causes of death in women between the ages of 15–19 years worldwide is labour.29 Lack of access due to socioeconomic conditions or discrimination has led many young women into preventable deaths. Similarly, inability to access contraceptives and strict abortion regulations have stagnated developed countries and has limited developing countries from maturing.30 Gender discrimination seems to be prevalent and common even in the most developed countries. No nation has closed over 80% of the gender gap between men and women.24
Within this study, it has been found that even in a state of low resources, a nation with strong instruments to promote and maintain WESR would still arrive at positive health outcomes. However, there are some states that highly respect ESR yet fail to extend these rights to include women.
Implications
The impact of limited women’s rights influences more than just women. As Paul Wolfowitz, former President of the World Bank said, ‘Gender equality is not only a women’s issue, it is a development issue'.31 In this study, specifically, the data were quantified to show a more discrete correlation between WESR and development. This has an impact on current events as these findings can help the SDG and the UN in implementing factors that account for WESR at a greater level. Though correlation does not cede causation, the implications of higher WESR can only help advance development goals. Today, the value of human rights has often been questioned from an economic standpoint; however, our data find that rather than limit progress, human rights, and WESR in particular, can only benefit them.
Limitations
The study is a preliminary work using average values of all variables for the 2004–2010 years. Given the focus within 10 years, older data are not analysed and accounted for, perhaps leading to a different trend. Since the data set consists of average values, there is no way to determine the specificities, causes and rationale behind some of the values. Finally, the data emphasises countries specifically, without considering their status within their respective subregion, nor the dynamics within the country as well. Further studies should investigate longer time periods to determine an overarching trend, along with the need to view countries in equalised settings. That is, countries with similar human rights trends should be compared with one another for greater insight into the development of WESR. Subsequent research should also include an in-depth investigation into the various statistics and undercurrents within each country.
Acknowledgments
In addition, Leila Ahdieh contributed by summarising the UN CEDAW reports and analysis.
Supplementary materials
Press Release
Press Release
- Press Release -
Press Release
- Press Release -
Footnotes
Contributors All persons who meet authorship criteria are listed as authors, and all authors certify that they have had equal contributions to the creation of the manuscript. KA is the corresponding author for this paper and has contributed in revising, editing and drafting the introduction. SA and W-FC performed the data analysis and contributed to the variables and data, and findings section. SH and AM contributed to writing the introduction and discussion sections, as well as editing and revising the manuscript. ES edited and revised the manuscript, and wrote pieces of the discussion. AA performed research and analysis for the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The depiction of boundaries on the map(s) in this article do not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The map(s) are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data can be accessed by emailing Sedef Akgüngör at sedef.akgungor@deu.edu.tr.
Patient consent for publication Not required.