Article Text

Abstract
Objectives Anterior neck soft tissue thickness, usually measured by ultrasound, is increasingly being investigated to predict difficult laryngoscopy, but the results have not been validated. Considering the conflicting measurement data, different measuring body positions and lack of a standard ultrasound procedure, we used MRI to verify the efficacy of these popular ultrasonographic parameters.
Design Prospective cohort study.
Setting A tertiary hospital in Beijing, China.
Methods We enrolled 315 adult patients who underwent cervical spinal surgery in Peking University Third Hospital from April to October 2016. We analysed MRI data to predict difficult laryngoscopy. Cormack–Lehane scales were assessed during intubation, and patients with a class III or IV view were assigned to the difficult laryngoscopy group.
Results Univariate analysis showed that male sex (p<0.01), older age (p=0.03) and body weight (p=0.02) were associated with difficult laryngoscopy. MRI data consisted of five common ultrasonographic variables used to predict difficult laryngoscopy, but none was a valuable predictor: skin to hyoid (p=0.18), skin to midpoint of epiglottis (p=0.72), skin to thyroid cartilage at the level of the vocal cords (p=0.10), skin to vocal cords (p=0.44) or skin to anterior to the trachea at the level of suprasternal notch (p=0.92). Adjusted by sex, age and body weight, none of the five MRI indicators had predictive value (p>0.05).
Conclusion The five most commonly studied ultrasonographic indicators of anterior soft tissue thickness appeared unreliable to predict difficult laryngoscopy in patients with cervical spondylosis. Further study is needed to validate the most valuable indicator to predict difficult laryngoscopy.
Trial registration number ChiCTRROC-16008598; Pre-results.
- difficult laryngoscopy
- cervical spondylosis
- ultrasound
- magnetic resonance imaging
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This might be the first MRI study to evaluate anterior neck soft tissue thickness for predicting difficult laryngoscopy.
The protocol of ultrasound predictors for anterior neck soft tissue have not been standardised.
Ultrasound predictors of anterior neck soft tissue thickness are usually performed in neck maximum extension which may be dangerous for patients with cervical spondylosis.
In our study, ultrasound and MRI were not performed at the same time.
The limitation of MRI in airway assessment is that it could not be used for dynamic detection, and all measurements were taken with patients in the neutral position instead of the intubation position.
Introduction
The rate of difficult laryngoscopy and intubation ranges widely from 0.5% to 24% of patients undergoing general anaesthesia among difficult studies.1–4 Patients with cervical spondylosis have a higher incidence of difficult laryngoscopy compared with patients without cervical spondylosis,5 6 and in patients with cervical spondylosis, anaesthesiologists may encounter a large percentage of unexpected difficult airways, which are associated with increased morbidity and mortality.
Airway examination is an essential component of the preoperative assessment. Preoperative assessment of a patient’s airway enables the anaesthesiologist to predict the ease of visualising the glottis and performing intubation. Predictors have variable sensitivities and specificities for identifying a difficult airway.7 Common bedside physical airway assessment tests include interincisor gap, thyromental distance and Mallampati test.8 However, these measurements have high interobserver variability, and predictive accuracy is too low to identify patients with the most difficult laryngoscopy.9–12 To increase the accuracy of preoperative evaluation, recent studies have measured anterior neck soft tissue thickness using ultrasound. Ultrasonographic measurements are rapid and convenient to perform, but ultrasonographic findings in studies of preoperative difficult airway assessment are inconsistent. This may be attributed to the operator’s skill in ultrasonographic scanning, target image recognition and measurement, patient positioning during ultrasonographic scanning and patients’ ethnic differences and operation type. Ultrasonographic predictors of anterior neck soft tissue thickness are usually performed in neck maximum extension which may be dangerous for patients with cervical spondylosis. It should be emphasised that no ultrasound study was performed in such patients with cervical spine pathology. Whether these measurements are appropriate as difficult laryngoscopy predictors requires further evaluation. To verify the accuracy of ultrasonographic measurements proposed by other studies in patients with cervical spondylosis, we used MRI to quantify anterior neck soft tissue thickness, which is more accurate than ultrasonography for evaluating soft tissues.
Materials and methods
Study participants
Patients aged 20–70 years, mentally competent, American Society of Anesthesiologists’ physical status I or II and who were scheduled for elective cervical spinal surgery under general anaesthesia from April to October 2016 were recruited in this prospective cohort study. Written informed consent was obtained from all patients. We excluded patients who were pregnant, experienced cervical spinal instability or who had an oropharyngeal mass.
Equipment and researchers
Neck MRI (MR750; GE Medical Systems, Milwaukee, Wisconsin, USA) examination was performed with the patient in the neutral position, and MRI indicators were measured on the lateral sagittal neck MRI film (figure 1) by an experienced radiologist blinded to group allocation and not involved in intubation and anaesthesia management. MRI data were evaluated using the radiography information system (Centricity RIS-IC CE V3.0; GE Healthcare, Little Chalfont, UK) of Peking University Third Hospital.

Indicators on lateral sagittal neck MRI image. DSE, distance from skin to epiglottis; DSH, distance from skin to hyoid bone; DSS, distance from the skin to anterior to the trachea at the level of suprasternal notch; DST, distance from skin to thyroid cartilage at the level of the vocal cords; DSV, distance from skin to vocal cords.
Measurements
MRI data included the shortest distance from: the skin to the hyoid bone (DSH), skin to the midpoint of the epiglottis (DSE), skin to the thyroid cartilage at the level of the vocal cords (DST), skin to the vocal cords (DSV) and skin to anterior to the trachea at the level of the suprasternal notch (DSS). All MRI indicators were measured by an experienced radiologist in batches containing all patients. The radiologist was blind to group allocation and did not participate in the anaesthesia management, so bias was avoided.
Laryngoscopy
All patients received no premedication. Anaesthesia was induced intravenously with sufentanil (0.3 µg/kg), propofol (2 mg/kg) and rocuronium (0.6 mg/kg). Laryngoscopy difficulty was assessed with the Cormack–Lehane scale determined during Macintosh laryngoscopy, in all patients in the sniff position, by the same senior anaesthesiologist for all patients.13 Patients with a class III or IV view were assigned to the difficult laryngoscopy group, and those with a class I or II view were assigned to the easy laryngoscopy group. Tracheal intubation was then performed with a Macintosh laryngoscope or alternative device. In patients with a difficult airway, intubation was performed according to the Difficult Airway Society 2015 guidelines.14
Patient and public involvement
No patients were involved in the MRI data measures nor were they involved in developing plans for design or implementation of the study. No patients were asked to advise on interpretation or writing up of results. Study reports will be disseminated to investigators and patients through this open-access publication.
Statistical analysis
Estimating a 24% incidence of difficult laryngoscopy,4 the calculated sample size was 278 patients using PASS V.11.0 (NCSS LLC, Kaysville, Utah, USA) to obtain a power of 0.9 and a significance level of 0.05. In consideration of potential dropouts, 315 patients were recruited for the study. SPSS software V.21.0 (IBM) was used for all statistical analyses. Categorical variables were analysed by the χ2 test, and continuous variables were expressed as mean±SD with an independent samples t-test. Binary multivariate logistic regression analyses were performed to identify multivariate predictors for difficult laryngoscopy. We calculated 95% CIs, and p<0.05 was considered statistically significant.
Results
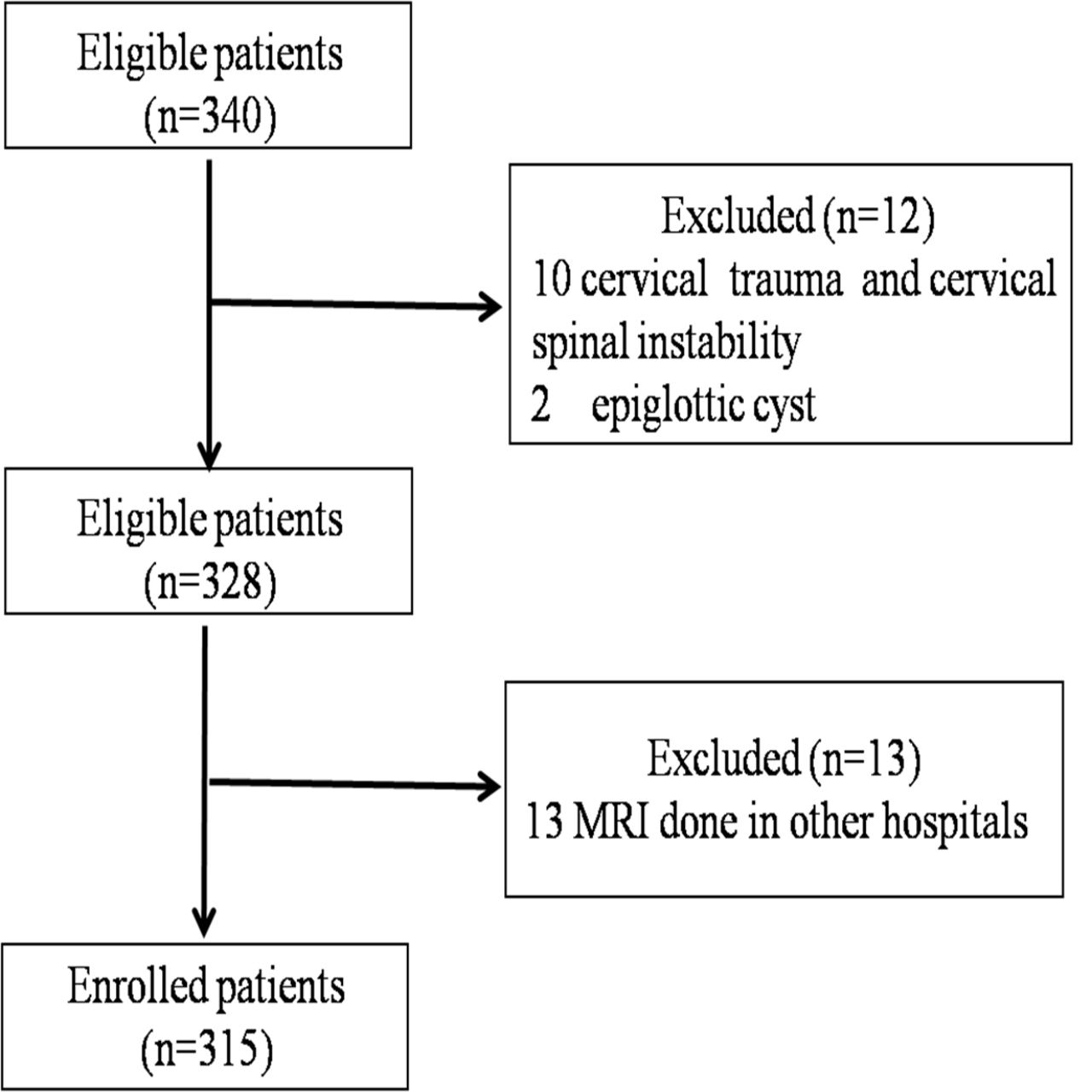
A total of 328 were initially enrolled in the study and 315 were included in the final analysis. The allocation process was presented in figure 2. Patients comprising 200 men (63.5%) and 115 women (36.5%) were included in the study. Univariate analysis demonstrated three risk factors associated with difficult laryngoscopy: male sex (p<0.01), older age (p=0.03) and body weight (p=0.02). Five MRI indicators were not significantly different between the easy and difficult laryngoscopy groups, respectively: DSH (1.73±0.54 cm vs 1.61±0.52 cm; p=0.18), DSE (3.76±0.53 cm vs 3.79±0.53 cm; p=0.72), DST (0.66±0.24 cm vs 0.59±0.23 cm; p=0.10), DSV (1.49±0.41 cm vs 1.43±0.42 cm; p=0.44) and DSS (4.53±0.72 cm vs 4.52±0.75 cm; p=0.92). The indicators are listed in table 1.
Patients’ demographic data and MRI indicators
{kind=link}
{kind=link}
Allocation process.
Adjusted by sex, age and weight, binary multivariate logistic regression analyses for the MRI indicators identified no factor that was independently associated with difficult laryngoscopy: DSH (p=0.51), DSE (p=0.12), DST (p=0.26), DSV (p=0.09) and DSS (p=0.59). ORs (95% CIs) for DSH, DSE, DST, DSV and DSS were 0.79 (0.38 to 1.62), 0.56 (0.27 to 1.16), 0.38 (0.07 to 2.04), 0.44 (0.17 to 1.13) and 1.16 (68 to 1.96), respectively. Results appear in table 2.
The five MRI predictors for difficult laryngoscopy identified by binary multivariate logistic regression (Enter) model
Discussion
To our knowledge, ours is the first study of anterior neck soft tissue thickness verified by MRI. Our results showed that the five most popular ultrasonographic indicators had no significant difference for predicting easy and difficult laryngoscopy.
Our data demonstrated that male sex, higher body weight and older age were associated with difficult laryngoscopy. A significantly greater proportion of difficult tracheal intubations has been reported in men and obese patients.15 16 An association between difficult laryngoscopy and older age has also been reported.17 Osteoarthritic changes associated with decreased thyromental distance, cervical spinal movement, interincisor distance and grade of dentition may be responsible for age-related increases in difficult laryngoscopy.4
Adding ultrasonography to airway evaluation allows for rapid visualisation of structures. With appropriate depth and probe-frequency selection, ultrasound can image any structure lying superficial to the oral, pharyngeal or tracheal air columns.18 This includes the mouth, tongue, oropharynx, hypopharynx, hyoid bone, epiglottis, larynx, vocal cords, cricothyroid membrane, cricoid cartilages and trachea.19 Ultrasonography, as a portable, non-invasive, rapid and effective examination is increasingly used for airway assessment before surgery; however, results are inconsistent.
Adhikari et al 20 reported that DSH could be used to distinguish difficult and easy laryngoscopies, and found that DSH values were higher in the difficult laryngoscopy group compared with the easy laryngoscopy group (1.69 cm, 95% CI 1.19 to 2.19 vs 1.37 cm, 95% CI 1.27 to 1.46, respectively) in a study of 51 American patients in the neutral position without a pillow. However, in a study by Reddy et al,21 DSH was not a significant predictor of difficult laryngoscopy (p=0.86), and our results were consistent with Reddy et al’s. In our study including 315 patients with cervical spondylosis in the neutral position, we found that DSH did not differ significantly between easy and difficult laryngoscopy groups (1.73±0.54 cm vs 1.61±0.52 cm, respectively; p=0.18).
Pinto et al 22 studied 74 Portuguese patients in the neutral position and found that DSE can be used effectively to predict difficult laryngoscopy; DSE was greater in the difficult laryngoscopy group compared with the easy laryngoscopy group (2.83±0.44 cm vs 2.33±0.39 cm, respectively; p<0.01). Soltani et al 23 studied 53 Iranian patients in the supine position with active maximal head tilt and chin lift and found that the correlation between the depth of the pre-epiglottic space and Cormack–Lehane grade III was weak, with a regression coefficient of 0.13 (95% CI 0.70 to 1.71; p=0. 40). In our study, DSE did not differ significantly between easy and difficult laryngoscopy groups (3.76±0.53 cm vs 3.79±0.53 cm, respectively; p=0.72).
Komatsu et al 24 studied 64 obese American patients in the neutral position without a pillow and found that DST in the difficult laryngoscopy group was shorter than that in the easy laryngoscopy group (2.0±0.3 cm vs 2.2±0.4 cm, respectively; p<0.05), but multivariate regression indicated that DST was not an independent predictor of difficult laryngoscopy (p=0.13). Therefore, the authors concluded that DST was not a good predictor and that it failed to predict difficult laryngoscopy in obese patients. In our study, we found that DST did not differ significantly between easy and difficult laryngoscopy groups (0.66±0.24 cm vs 0.59±0.23 cm, respectively; p=0.10).
Ezri et al 15 studied 50 obese Israeli patients and found that DSV and DSS in the difficult laryngoscopy group were both greater than values in the easy laryngoscopy group (2.8±0.3 cm vs 1.8±0.2 cm, respectively; p<0.01 and 3.3±0.4 cm vs 2.7±0.7 cm, respectively; p=0.01). Reddy et al 21 also found that DSV in the difficult laryngoscopy group was greater than that in the easy laryngoscopy group (0.35±0.18 cm vs 0.25±0.11 cm, respectively; p=0.01) and that DSV >0.23 cm was a potential predictor of difficult intubation with 85.7% sensitivity, 57% specificity and 61% accuracy. However, Adhikari et al 20 found no significant differences for DSV and DSS between easy and difficult laryngoscopy groups. We also found that DSV and DSS did not differ significantly between easy and difficult laryngoscopy groups (1.49±0.41 cm vs 1.43±0.42 cm, respectively; p=0.44 and 4.53±0.72 cm vs 4.52±0.75 cm, respectively; p=0.92).
Ultrasonography is convenient and useful for bedside examination, and five indicators of anterior neck soft tissue thickness at different levels measured using ultrasonography have been discussed previously. The results of the five ultrasonographic predictors are inconsistent. Considering that MRI has higher resolution than ultrasound, to obtain better soft tissue images with lower radiation hazard, we chose MRI to measure the related soft tissues. We found that none of the five indices could predict difficult laryngoscopy in patients with cervical spondylosis regardless of whether sex, age and body weight were adjusted with a binary multivariate logistic regression. The reasons for different results between our study and previous studies are as follows: (1) the five MRI indicators focused only on the local anatomy and could not reflect cervical activity and changes in head position (from neutral to extended). Therefore, these may not be meaningful indicators; however, no defined gold standard indicators exist. (2) These indices have been measured previously using ultrasonography, but measurements were not taken using standardised procedures, which have not been determined. Ultrasonographic measurements obtained by the primary investigator might have been associated with bias, and the measurement results were related to the operator’s experience. The lack of a standardised reference and methods for obtaining these ultrasonographic measurements in previous studies also indicates the potential for operator error. Patients’ necks were also positioned differently across studies, which could result in measurement error. (3) Patients’ ethnicity and operation type might also affect results. Our study participants were Asian, and previous studies included American, Portuguese or Iranian patients; studies have documented differences in neck fat tissue distribution between different ethnic groups.20 (4) Our patients had cervical spondylosis, and the presence of this condition was not mentioned for patients in previous studies. (5) Considering superficial measurements reflecting anatomical variation in an extremely anterior airway and the small sample size in previous studies, results might be skewed.
Limitations of the study
Our study has limitations. First, measurements in some previous studies were taken in the head-extended position to facilitate ultrasonographic examination. In our study, during MRI examination, all measurements were taken with patients in the neutral position, and no measurements were taken in the intubation position. Although we positioned all patients in the same position, there is a difference between the MRI examination position and the intubation position, and a deficiency of MRI is that it is not a dynamic measurement method. Second, this study did not have the same design as previous ultrasound studies. We did not perform ultrasonography and MRI simultaneously in the same patients; we used MRI to verify whether the ultrasonographic parameters of anterior neck soft tissue thickness suitable for patients with cervical spondylosis. In this patient cohort, ultrasonography derived measurements reflecting cervical mobility (such as hyo-mental distance ratio) might be more valuable compared with anterior neck soft tissue thickness. Third, although MRI costs more than ultrasound and time required, MRI is a routine preoperative examination in patients undergoing surgery for cervical spondylosis; therefore, we verified the five most popular ultrasonographic indicators in these specific patients to best use data to predict a difficult airway without additional expense. However, our results might not be suitable for other patients, and further research is needed.
Conclusion
Our study suggests that the ultrasonographic indices (DSH, DSE, DST, DSV and DSS) used to evaluate anterior neck soft tissue thickness at different levels, measured by MRI, could not predict difficult laryngoscopy in patients with cervical spondylosis. In future studies of ultrasonographic assessment, patients’ ethnicity, position, operators’ qualifications and standardised operation procedures all must be considered. Based on high-quality and large sample size studies, the most accurate ultrasonographic indicator for difficult laryngoscopy may be determined.
Acknowledgments
We sincerely thank all the staff members of the Anesthesiology and Radiology Department of Peking University Third Hospital for their help in this research.
References
Footnotes
YH and JF contributed equally.
Contributors YH and MX designed and coordinated the study, collected and interpreted data and drafted the manuscript. XG participated in the study design. JF participated in measuring radiological indicators. HZ analysed the data and performed statistical analysis. All authors discussed the results, and read and approved the final manuscript.
Funding The present study was supported by the Capital Clinical Characteristic Applied Research Project (Z181100001718109) and Hospital Medical Research Foundation of Peking University Third Hospital (No. Y75485-05).
Disclaimer The funders were not involved in the study design, data analysis or manuscript preparation.
Competing interests None declared.
Ethics approval The study was approved by Peking University Third Hospital Medical Science Research Ethics Committee (IRB00006761-2015021).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement A full anonymised dataset is available from the corresponding author on request.
Patient consent for publication Not required.