Article Text

Abstract
Objective Blood type A antigen on porcine aortic bioprostheses might initiate an immune reaction leading to an increased frequency of structural valve deterioration in patients with blood type B or O. The aim was to analyse the association between ABO blood type and porcine bioprosthetic aortic valve degeneration.
Design Observational nationwide cohort study.
Setting Swedish population-based study.
Participants Adult patients (n=3417) who underwent surgical aortic valve replacement and received porcine bioprosthetic aortic valves between 1995 and 2012 from the Swedish Web system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies register. The study database was enriched with information from other national registers.
Exposure The patients were categorised into type A/AB and type B/O blood groups.
Primary and secondary outcome measures Primary outcome measure was aortic valve reoperation, and secondary outcomes were heart failure and all-cause mortality. We report risk estimates that account for the competing risk of death.
Results In total, 3417 patients were identified: 1724 (50.5%) with blood type A/AB and 1693 (49.5%) with blood type B/O. Both groups had similar baseline characteristics. The cumulative incidence of aortic valve reoperation was 3.4% (95% CI 2.5% to 4.4%) and 3.6% (95% CI 2.6% to 4.6%) in the type B/O and the A/AB group, respectively, at 15 years of follow-up (absolute risk difference: −0.2% (95% CI −1.5% to 1.2%)). There was no significantly increased risk for aortic valve reoperation in patients with blood type B/O compared with type A/AB (HR 0.95, 95% CI 0.62 to 1.45). There was no significant difference in absolute or relative risk of heart failure or death between the groups.
Conclusions We found no significant association between patient blood type and clinical manifestations of structural valve deterioration following porcine aortic valve replacement. Our findings suggest that it is safe to use porcine bioprosthetic valves without consideration of ABO blood type in the recipient.
Trial registration number NCT02276950
- cardiac surgery
- valvular heart disease
- epidemiology
- adult cardiology
- cardiac epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Data were obtained from high-quality national Swedish health data registers including Swedish Web system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies.
The study exposure, that is, blood group, is genetically determined, and associations between exposure and outcomes are therefore robust to measured and unmeasured confounding.
Other strengths of the study are the reporting of both relative and absolute risks, and the long and complete follow-up.
One limitation of the study was that the porcine blood type for each implanted valve was not known.
Another limitation was that we were unable to precisely measure structural valve deterioration, and had to rely on surrogate endpoints.
Introduction
Bioprosthetic aortic valve replacement with bovine or porcine tissue is one of the few xenotransplant procedures in common practice. Ionescu et al performed the first porcine bioprosthetic heart valve procedures implanted in mitral, tricuspid and aortic positions in 1967.1 Since then, the use of biological heart valves has increased to become the most common type of heart valve implanted.2 The primary advantage of bioprosthetic valves is that they do not require anticoagulation. The European guidelines from 2017 include a class I level C recommendation to choose a bioprosthetic valve according to patient desire, when good-quality anticoagulation is unlikely or contraindicated, and for reoperation for mechanical valve thrombosis despite good long-term anticoagulant control.3
The main disadvantage of biological prostheses is the risk of structural valve deterioration.4 Structural valve deterioration presents as calcification, leaflet thickening, reduced leaflet motion and tearing. Some factors in this process are known, but research suggests that there are additional unknown contributing mechanisms. The most accepted hypothesis is that various immune responses and mechanical stress results in activation of immune cells and complement factors causing fibrosis, thrombosis and calcification.4
Xenogeneic carbohydrate structures and glycans have been shown to remain on commercial bioprosthetic valves even after pretreatment.5–7 Several studies have shown a humoral response in patients after bioprosthetic valve implants, including increased levels of IgM and IgG levels against the major glycan xenoantigen galactose-α-1,3-galactose (Galα(1-3)Gal), an ABO-like oligosaccharide.8–10 Porcine species express only the A and O blood groups of the ABO system, with type A phenotype the more common.11 12 Thus, A antigen on bioprosthetic valves could trigger an immunogenic response in blood type B/O patients due to the presence of anti-A antibodies, similar to an ABO-mismatched organ transplant or blood transfusion. It is not known whether this potential pathway is important in the development of structural valve deterioration in porcine bioprosthetic aortic valves.
The aim of this study was to analyse the association between ABO blood type and clinical manifestations of structural valve deterioration in patients with porcine bioprosthetic aortic heart valves.
Patient and public involvement
There was no patient or public involvement in the design or conduct of this study.
Study design
The design of the study was a nationwide, population-based, observational cohort study. Study reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology and REporting of studies Conducted using Observational Routinely collected health Data guidelines for observational studies using routinely collected data.13 14 The Swedish Web system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies (SWEDEHEART) register15 was used to identify patients who received porcine bioprosthetic aortic valves in Sweden between 1995 and 2012. The register collects pre, peri and postoperative parameters and outcomes of patients receiving cardiac surgery in Sweden.16Patients with concomitant procedures involving any other valves were excluded.
ABO blood type was obtained from the Scandinavian Donations and Transfusions Database (SCANDAT2).17 This database contains information including blood type on persons donating or receiving blood in Sweden and Denmark. The study population was categorised into two groups: A (blood type A and AB patients) and non-A (blood type B and O patients). Baseline characteristics were obtained from The National Patient Register18 and the Cause of Death Register,19 maintained by the National Board of Health and Welfare, and the Longitudinal Integration Database for Health Insurance and Labour Market Studies, maintained by Statistics Sweden. Individual-level data linking between the registers were possible because of the Swedish personal identity number.20
Outcomes
The primary outcome was aortic valve reoperation; this information was obtained from the SWEDEHEART register. Secondary outcomes were hospitalisation for heart failure and all-cause mortality, obtained from the National Patient Register and the Cause of Death Register, respectively. The hypothesis was that the anti-A immune response increased the rate of structural valve deterioration in porcine aortic valve bioprostheses. However, because structural valve deterioration is difficult to quantify by variables available from national registers, clinically relevant surrogate measures were selected to represent the presentation of structural valve deterioration. Valve reoperation served as a surrogate measure for prosthesis failure, and heart failure hospitalisation as an indication of progressive valve stenosis or regurgitation.
Missing data
Some baseline patient characteristics were missing: left ventricular ejection fraction (41%) and emergent status of surgery (41%) were missing for all patients operated before 2001. Estimated glomerular filtration rate was missing in 13% of patients. We categorised all patients with missing information regarding the emergent status of surgery as not having emergent status of surgery. Missing data for left ventricular ejection fraction and estimated glomerular filtration rate were handled by multiple imputation by chained equations under the assumption that data were missing at random.21 The imputation models included all variables in table 1, year of surgery, hospital, the event indicator and the Nelson-Aalen estimator of the cumulative baseline hazard.22 Ten datasets were imputed and estimates from these datasets were combined according to Rubin’s rules.
Baseline characteristics in 3417 patients with porcine aortic valve bioprostheses according to ABO blood group
Statistical analysis
Baseline characteristics were described as means and SD, or medians and quartiles for continuous variables. Categorical variables were described as frequencies and percentages. Balance between the groups was assessed by t-tests, X2 tests and standardised mean differences. A standardised mean difference of 10% or less (absolute value) is generally considered an ideal balance.23 Time to event was calculated as time in days from the date of surgery until the date of respective event or end of follow-up (31 December 2013 for aortic valve reoperation or death, and 31 December 2012 for heart failure hospitalisation). We used the Kaplan-Meier method to estimate cumulative survival. Cox proportional hazards regression was used to estimate crude and adjusted HR and 95% CIs for the association between patient blood type and outcomes. The cause-specific hazard for aortic valve reoperation or heart failure was explored by treating competing events (deaths) as censored in the Cox regression analyses. We fitted both univariate models, models including only ABO blood type, age, and sex, as well as fully adjusted models including a range of possible confounding factors. The following variables were included in the fully adjusted Cox regression model: patient age, sex, left ventricular ejection fraction, estimated glomerular filtration rate, atrial fibrillation, hypertension, chronic obstructive pulmonary disease, prior myocardial infarction, prior stroke, hyperlipidaemia, peripheral vascular disease, alcohol dependency, heart failure, diabetes, prior major bleeding event, prior venous thromboembolism and emergent operation. Flexible parametric survival models were used to estimate the cumulative incidence and the cumulative incidence difference of aortic valve reoperation and heart failure, respectively, accounting for the competing risk of death.24 We compared survival probabilities in the study population to that of a Swedish reference general population matched for age, sex and year, available from the Human Mortality Database (http://www. mortality.org).25 We calculated the difference in restricted mean survival time with 95% CI for the aortic valve reoperation outcome at 15 years.26 Data management and statistical analyses were performed using Stata V.15.1 (StataCorp LP) and R version V.3.4.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
We identified 3417 patients: 1724 (50.5%) in the type A/AB group and 1693 (49.5%) in the type B/O group. There was no significant difference in baseline characteristics except for hyperlipidaemia (8.9% vs 6.1%), peripheral vascular disease (10.7% vs 8.6%) and prior myocardial infarction (19.4% vs 16.0%), all more common in the type A/AB group. The standardised difference was less than 10% for all variables except hyperlipidaemia (standardised difference 10.6%). Baseline characteristics are described in table 1. Incidence rates for aortic valve reoperation, heart failure and death were similar in both groups during follow-up and are reported in table 2.
Incidence rate of aortic valve reoperation, heart failure admission or death in 3417 patients with porcine aortic bioprostheses according to blood group
The crude and adjusted risk of aortic valve reoperation, heart failure hospitalisation or death are shown in table 3. The median follow-up time was 6.8 years and 7.1 years in type A/AB group and type B/O group, respectively. There was no increased risk for aortic valve reoperation in the type B/O group compared with the type A/AB group (HR 0.95, 95% CI 0.62 to 1.45). There was no increased risk for heart failure (HR 0.92, 95% CI 0.77 to 1.08) or all-cause mortality (HR 0.95, 95% CI 0.87 to 1.05) in the type B/O group compared with the type A/AB group.
Crude and adjusted risk of aortic valve reoperation, heart failure admission or death in 3417 patients with porcine aortic bioprostheses according to blood group
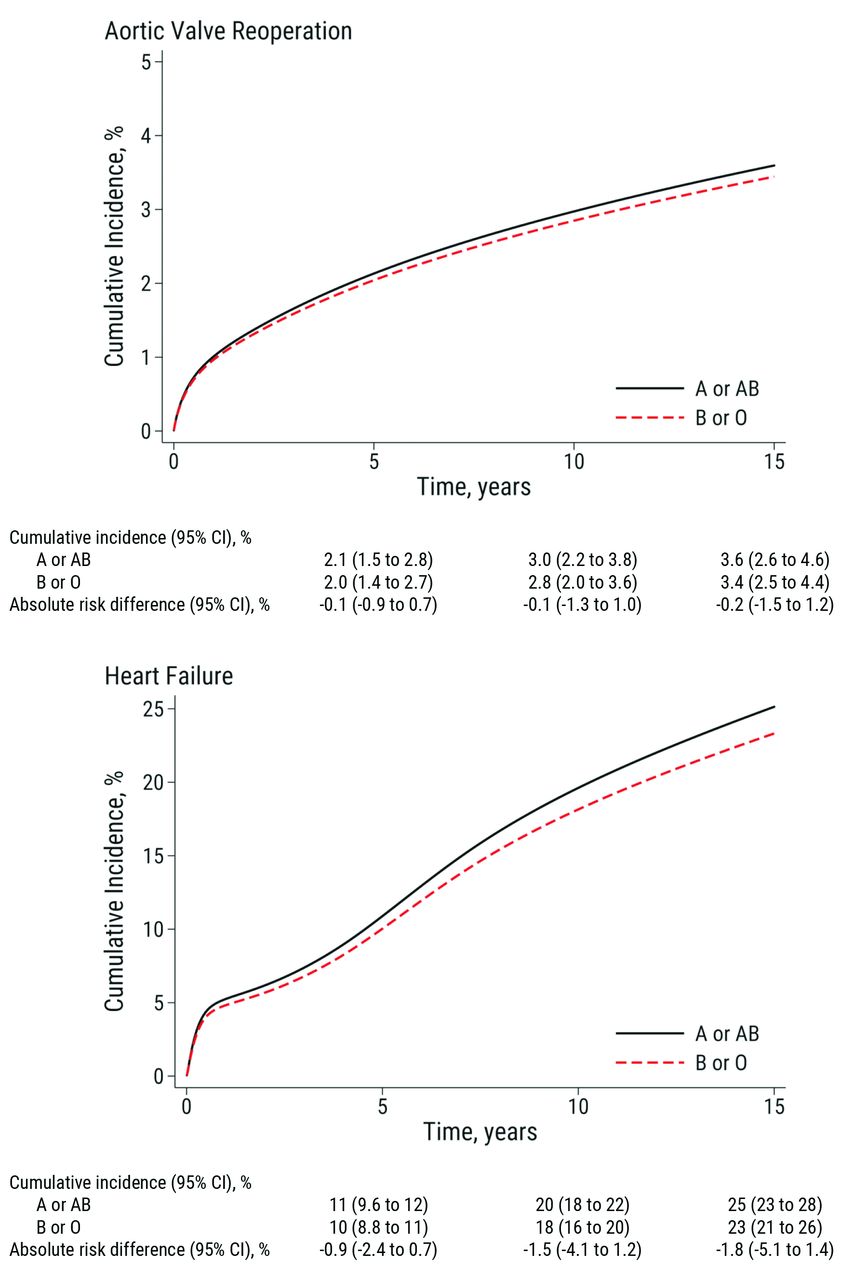
The cumulative incidence of aortic valve reoperation was 3.4% (95% CI 2.5% to 4.4%) and 3.6% (95% CI 2.6% to 4.6%) in the type B/O group and the type A/AB group, respectively, at 15 years of follow-up. This corresponded to an absolute risk difference of −0.2% (95% CI −1.5% to 1.2%) (figure 1). Similarly, there was no significant difference in restricted mean survival time for aortic valve reoperation between the type B/O and the type A/AB group at 15 years (6 days, 95% CI: −58 to 70 days, p=0.855). For hospitalisation for heart failure, the cumulative incidence at 15 years was 25% (95% CI, 23% to 28%) in the type A/AB group and 23%, (95% CI 21% to 26%) in the type B/O group, corresponding to an absolute risk difference of −1.8% (95% CI −5.1% to 1.4%). The analyses were repeated in a subset of patients who were operated after 2001 (with less missing data), and we found results that were very similar to the main analyses. We also used a multivariable model that excluded ejection fraction, glomerular filtration rate and emergent status (ie, those variables with most missing data), and we found practically identical results as in our main analysis.

Cumulative incidence of aortic valve reoperation (upper panel) and heart failure hospitalisation (lower panel) in 3417 patients with porcine aortic valve bioprostheses according to ABO blood group.
There was no difference in Kaplan-Meier estimated survival between the groups during 15 years of follow-up (figure 2). The observed overall survival in the total study population was compared with the expected survival of an age and gender-matched Swedish population and is shown in figure 3.

Cumulative survival in 3417 patients with porcine aortic valve bioprostheses according to ABO blood group.

{kind=link}
{kind=link}
{kind=link}
The observed overall survival (95% CI) in the total study population (red line) compared with the expected survival of an age and gender-matched Swedish population (black line).
Discussion
We found no significant difference in the risk of aortic valve reoperation between type A/AB and type B/O patients after porcine bioprosthetic aortic valve replacement during 15 years of follow-up. Furthermore, there was no difference in the risk of heart failure hospitalisation or all-cause mortality. Taken together, these findings suggest that it is safe to use porcine bioprosthetic valves without consideration of ABO blood type in the recipient. Our data also indicate that even if an immune reaction occurs against type A antigens, the clinical manifestation is negligible and does not result in symptomatic structural valve deterioration.
The underlying mechanisms for valve deterioration are not fully understood, although mechanical stress and immune reactions are likely culprits. Humoral response against several xenogenic antigens has been shown in patients receiving bioprosthetic heart valves,8 10 27 and a recent case report has identified specific immune responses as the direct cause of increased valve deterioration in specific patients.28
One of the most well-studied antigens in this context is Galα1,3Gal,29 which has a similar structure to the terminal part of certain blood group antigens. It is present on various tissues on most mammals with the exception of Old World apes and humans, and is known to be the antigen responsible for red-meat allergy.30 In a case report, Hawkins et al 28 reported early bioprosthetic failure without signs of endocarditis in two patients with a history of allergic reactions after red meat consumption coupled with increased titres of circulating anti-Galα1,3Gal IgE antibodies.28 Anti-Galα1,3Gal IgM and IgG have also been reported to increase after bioprosthetic aortic valve replacement,9 10 consistent with studies showing Galα1,3Gal epitopes remaining on commercial bioprosthetic valves after pretreatment with, for example, glutaraldehyde.5
These findings support the idea that type A antigens also remain on commercial valves and can initiate immune responses by anti-A antibodies in a manner similar to that occurring in ABO-mismatched organ transplants and blood transfusions.
It is likely that bovine species also express blood type antigens, and there are data to support the presence of xenogenic antigens.31 However, the bovine blood type system is more complicated with a high degree of polymorphism especially in the B type.32 This would introduce more unknown factors in this exploratory study, and so the authors choose to focus on porcine species with a limited ABO blood system.
Strengths and limitations
One limitation of the study is that the porcine blood type for each implanted valve was not known. Small experimental studies indicate that type A is slightly more common (ranging from 55% to 94%), and the only other known blood type in the porcine ABO system is type O.11 12 It is possible, but highly unlikely, that all the valves were from type O pigs, which would not yield an ABO mismatch reaction. Another limitation is that we were unable to precisely measure structural valve deterioration, and we had to rely on surrogate endpoints. We lacked the necessary echocardiographic parameters to estimate the incidence of structural valve deterioration according to current standardised definitions,33 and therefore, our study cannot definitively rule out a possible small or subclinical effect of patient blood group on the true rate of structural valve deterioration. However, the clinically important effects of structural valve deterioration are an increased rate of hospitalisation for heart failure (due to increased stenosis or regurgitation), an increased rate of reoperation (due to prosthesis failure) or an increased rate of death associated with the conditions previously mentioned; therefore, the chosen outcome measures would be relevant to patients. In this study, the exposure was patient blood type, and exposure occurred nearly randomly enough to constitute a natural experiment. Another limitation was that we lacked information regarding the cause of death. Baseline characteristics were indeed well balanced between the groups, and residual confounding was likely insignificant. The crude analyses performed here should provide valid estimates of the association between blood type and clinical outcomes, and we found only small changes in the point estimates after multivariable adjustment. Other strengths of the study are a thorough long-term follow-up. Limitations regarding the generalisability of the study findings are the lack of information regarding bioprosthetic valve model and blood group for some patients who underwent surgery during the study period. Only patients who had donated or received blood were included in the SCANDAT2 database, meaning that a different method of obtaining blood type for all patients with known bioprosthetic type would have yielded a larger study population.
Conclusions and clinical interpretation
We found no significant association between patient blood type and clinical manifestations of structural valve deterioration following porcine aortic valve replacement. The absolute risk difference between patients with type A/AB and type B/O blood groups at 15 years was negligible. Our findings suggest that it is safe to use porcine bioprosthetic valves without consideration of ABO blood type in the recipient.
Acknowledgments
We thank the SWEDEHEART steering committee for providing data for this study.
References
Footnotes
Contributors MP, GE, MD, NG, MLO, AF-C, MH and US conceived and designed the research. MP, GE, NG, MH and US acquired the data. MP and US performed statistical analyses with important contributions from GE. MP, GE, MD, NG, MLO, AF-C, MH and US contributed to the interpretation of data. MP and US drafted the manuscript. MP, GE, MD, NG, MLO, AF-C, MH and US made critical revision of the manuscript for key intellectual content and have seen and approved the final version.
Funding This work was supported by the Swedish Heart-Lung Foundation (grant numbers 20160522, 20160525 to US, 20090710 to GE and 20150603 to MH); the Mats Kleberg Foundation (grant number 2017-00096 to US); Karolinska Institutet Foundations and Funds (grant number 2016fobi47721 to US); Swedish Heart and Lung Association (grant number E101/16 to US); Åke Wiberg Foundation (grant number M17-0089 to US); Magnus Bergvall Foundation (grant number 2017-02054 to US); the regional ALF agreement between Stockholm County Council and Karolinska Institutet (grant number 20160329 to US); a donation from Fredrik Lundberg (to AF-C); governmental grants for clinical research to university healthcare in Lund, Sweden (grant number ALFSKANE-446521 to MLO); the Knut and Alice Wallenberg Foundation (grant number 2014.0312 to MLO); the Swedish Research Council (grant numbers 2014-71X-14251 to MLO and 2011-30405, 2007-7469 to GE); the Swedish Society for Medical Research (to GE) and the Strategic research program in Epidemiology at Karolinska Institutet (to GE).
Competing interests MH received consultancy honoraria from Actelion and Pfizer.
Ethics approval The study was approved by the regional Human Research Ethics Committee, Stockholm, Sweden (Dnr: 2017/886–32).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No data are available.
Patient consent for publication Not required.