Article Text

Abstract
Introduction Different surgical techniques are used to cover the defect in the floor of the lesser pelvis after an ‘extralevator’ or ‘extended’ abdominoperineal excision for advanced rectal cancer. However, these operations are potentially mutilating, and the reconstruction method of the pelvic floor has been studied only sparsely. We aim to study whether a porcine-collagen implant is superior or equally beneficial to a gluteus maximus myocutaneous flap as a reconstruction method.
Methods and analysis This is a multicentre non-blinded randomised controlled trial with the experimental arm using a porcine-collagen implant and the control arm using a gluteus maximus muscle and skin rotation flap. Considered for inclusion are patients with rectal cancer, who are operated on with a wide abdominoperineal rectal excision including most of the levator muscles and where the muscle remnants cannot be closed in the midline with sutures. Patients with a primary or recurrent rectal cancer with an estimated survival of more than a year are eligible. The randomisation is computer generated with a concealed sequence and stratified by participating hospital and preoperative radiotherapy regimen. The main outcome is physical performance 6 months after surgery measured with the timed-stands test. Secondary outcomes are perineal wound healing, surgical complications, quality of life, ability to sit and other outcomes measured at 3, 6 and 12 months after surgery. To be able to state experimental arm non-inferiority with a 10% margin of the primary outcome with 90% statistical power and assuming 10% attrition, we aim to enrol 85 patients from May 2011 onwards.
Ethics and dissemination The study has been approved by the Regional Ethical Review board at Umeå University (protocol no: NEAPE-2010-335-31M). The results will be disseminated through patient associations and conventional scientific channels.
Trial registration number NCT01347697; Pre-results.
- rectal cancer
- extralevator
- postoperative disability
- physical function
- myocutaneous flap
- porcine implant
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first head-to-head comparison of an acellular porcine-collagen implant versus a gluteus maximus myocutaneous flap to reconstruct the defect in the lesser pelvis after extended abdominoperineal resection.
This is a randomised controlled trial, thus ensuring minimal confounding.
The primary outcome of physical performance is objectively measured, clinically relevant and important to patient and physician alike.
The trial intervention is however impossible to blind, which might introduce bias.
The planned sample size is adequate to evaluate non-inferiority of the implant arm concerning physical performance, but might be inadequate for secondary and subgroup analyses.
Introduction
Background and rationale
Abdominoperineal excision (APE) of the rectum is a common procedure for rectal carcinomas situated too low for sphincter-saving surgery, especially if the levator and sphincter musculature is infiltrated.1 The local recurrence rate after APE has been reported to be from 5% to 47%.2 3 Consequently, much interest has focused on improved surgical technique, in which the levator musculature is included in the excision by a lateral dissection close to the pelvic wall, creating a cylindrical specimen, as described already by Miles.1 4 5 Encouraging oncological results for this extended APE (EAPE) have been reported.2 6 However, when the levator musculature is excised en bloc with the rectum, a large defect is created. While subcutaneous fat and skin can be approximated, primary closure of the pelvic floor is not possible, and reconstruction with prosthetic material or a myocutaneous flap might decrease the risk of a perineal hernia. Implantation of a collagen sheet has shown preliminary good results,7 8 and a recent trial indicated lower hernia rates with biological mesh compared with primary suture.9 Reconstruction with a gluteus maximus myocutaneous flap (GMF) has several theoretical advantages compared with the alternatives: compared with a transabdominal flap, the abdominal wall is not damaged, while foreign material is not implanted in comparison to a collagen sheet. Promising results with low local complication rates after a GMF have been presented.6 However, the gluteus maximus muscle is a strong hip extensor and important for posture and balance. Patients operated on with a GMF have been shown to have impaired physical function, as measured by the so called timed-stands test (TST); inability to sit down without adjuncts was also frequent.10 Newer muscle-sparing flap techniques have been introduced, but have not been studied extensively.11 As robust evidence is lacking,12 13 there is a need for high-quality prospective trials to compare different methods of reconstruction. As far as we know, functional outcomes and quality of life after the GMF have not been compared with alternative techniques earlier.
Objectives
We hypothesise that an acellular porcine-collagen implant (APCI) is equally beneficial or superior to a GMF for the reconstruction of the lesser pelvic floor after EAPE for rectal cancer as evaluated by physical performance, quality of life and surgical complications. The primary objective is to study whether an APCI results in a clinically equivalent or superior physical performance, in comparison to a GMF. The secondary objectives are to compare the techniques in relation to wound healing, late complications including inability to sit, pain as well as discomfort, and quality of life. Further, we aim to compare costs with the two techniques, and to perform a cost-utility analysis in terms of quality-adjusted life-years (QALYs) gained. Costs and health economics will be calculated only in centres that have routine registration (in electronic databases) of operation time, time in the intensive care unit, hospital length of stay, connected reoperations and readmissions, as well as outpatient visits related to the index operation.
Trial design
The Nordic EAPE (NEAPE) trial is designed as a randomised, controlled, non-blinded, multicentre non-inferiority trial with two parallel groups and a primary outcome of physical performance measured with the TST 6 months after surgery. Patients are block-randomised with a 1:1 allocation, stratified for centre and preoperative radiotherapy (RT). The protocol was drafted in accordance with the Standard Protocol Items: Recommendations for Interventional Trials reporting guidelines.14
Methods and analysis
Participations, interventions, outcomes
Study setting
This is a multicentre study conducted in Nordic hospitals that treat locally advanced rectal cancer patients with the EAPE procedure.6
Eligibility criteria
Inclusion criteria
Adult (18 years or older) patients with rectal cancer, primary or recurrent; individual patients can be included only once.
An APE is planned where a wide resection of pelvic floor muscles together with rectum and anal canal will make a reconstruction of the pelvic floor necessary, that is, primary suture of the pelvic floor in the midline is not possible; resection of coccyx is optional.
Exclusion criteria
Age lower than 18 years.
Resections including partial resection of sacrum and patients considered for bilateral flap reconstruction.
Concomitant resection of vaginal wall where total (vaginal) wound closure is not an option.
Expected survival is less than 1 year after the operation.
Patient does not sign the informed consent document; this group includes:
Patients who do not want to participate and undergo allocation to treatment by randomisation.
Patients or their legal representatives do not fully understand the role of participation.
Trial centre requirements
Centres can participate provided that (1) the operative technique is standardised according to this protocol, (2) the centre has resources for examinations of enrolled patients by a physiotherapist or a nurse, (3) the centre has one local investigator in charge and (4) the centre has an operative volume that enables at least six patients to be included/randomised during the anticipated 3-year study phase for inclusions. Centres that do not operate patients with locally advanced rectal cancers included in this study can also participate by arranging the preoperative examination and physical tests as well as follow-up of patients that are referred to other centres for the operation. In these cases, the operating centre cares for the randomisation, operation and start of postoperative rehabilitation while the study follow-up and final rehabilitation can be completed at the patients’ primary referral hospital. The primary referral hospital needs a site investigator in charge of study patients just like centres that perform the operations.
Interventions: surgical methods and postoperative rehabilitation
Preoperative measures
All patients should receive prophylactic antibiotics before surgery. One dose preoperatively is our recommendation, but if the operation takes more than 4 hours to complete, a second dose should be given within 24 hours from the first dose.15 16 If a second generation cephalosporine is used alone, two additional doses every 8 hours after the first dose should be used.17 Antithrombotic prophylaxis should be given with low molecular weight heparin and it should be continued for 28 days18.19 Enhanced recovery programmes may be used in whole or partially but the programme chosen by a clinic should not change during the study period. The patient should be informed about the postoperative rehabilitation programme by the physiotherapist. One of two available rehabilitation programmes should be chosen and used for all patients during the whole study period (refer to the Postoperative rehabilitation programmes section).
First part of the operation
The following technique description is cited directly from the publication of Holm et al.6 The abdominal part of the operation is performed as in a conventional APE, with one important modification: the mesorectum is not dissected off the levator muscle. Thus, the mobilisation is stopped at the upper border of the coccyx posteriorly, just below the autonomic nerves laterally and anteriorly just below the vesicles in men or just below the cervix uteri in women. The divided left colon is brought out to form a colostomy and the abdomen is closed.
The patient is then turned into the prone jack-knife position with legs spread to enable the surgeon to stand between the legs with one assistant on each side. The anus is closed with a double purse-string suture. An incision is made around the anus and extended cranially to the lower part of the sacrum. The dissection continues in the subcutaneous fat, just outside the subcutaneous portion of the external anal sphincter. Following this plane, the levator muscle is identified on both sides and the dissection is continued along the outer surface of the levator muscles proximally until the insertion on to the pelvic side wall. It is important to expose the levator muscles all around the circumference before entering the pelvis. The coccyx is then disarticulated from the sacrum and Waldeyer’s fascia divided. This permits entry into the pelvic cavity at the point where the intra-abdominal dissection stopped. The levator muscles are divided laterally on both sides, from posterior to anterior. The specimen is gently brought out and dissected off the prostate or the posterior vaginal wall. In the case of an anterior tumour, a portion of the prostate or the posterior vaginal wall may be resected en bloc. Finally, the remaining pelvic floor muscle fibres are divided just posterior to the transverse perineal muscles and the specimen is excised.6 Of note, excision of the coccyx is optional in this trial. Omentoplasty to fill the lesser pelvis can also be performed according to the surgeon’s discretion. A suprapubic catheter to the urinary bladder should be placed during the laparotomy and kept until normal bladder emptying occurs. An intra-abdominal drain is positioned with the tip in the lesser pelvis and kept for 3–5 days but can be removed earlier if the drainage volume measures less than 50 mL/day.
Reconstruction of the pelvic floor with APCI
A 10×10 cm or a 10×5 cm piece of the APCI (1.5 mm thick) is cut in the corners to fit the defect created in the floor of lesser pelvis. The implant is sutured in place with 2–0 polypropylene thread using interrupted sutures. Sutures attach to the edge of the sacrum or the coccyx posteriorly in the wound, laterally to remnants or cut edges of the levator muscle and anteriorly to the prostate capsule in men and to the vaginal wall in women. The implant can be folded anteriorly to produce a larger area of contact with the prostate or the vaginal wall. The wound is drained in two layers with the deep drain adjacent to the implant and the second superficially below the skin. The two deep layers of the wound and the skin are closed with resorbable 2–0 and 3–0 monofilament sutures, respectively. Any vaginal wall defects should be closed with absorbable sutures.
Reconstruction of the pelvic floor with unilateral GMF
The following technique description is cited directly from the publication of Holm et al.6 The unilateral flap is usually based cranially with the length about 1.5:1 in proportion to the base. At the lateral border of the base, a triangle of skin and fat is removed (Bürow’s triangle) in order to shorten the outer skin edge and to get it matched to the inner edge during the rotation. The design of the flap is shown in figure 1. The lines for skin incision are drawn after removal of the specimen. Local anaesthetic with epinephrine is used to reduce bleeding and postoperative pain. The skin and subcutaneous tissue are incised down to the gluteus maximus where the fascia is also incised along the whole length of the wound to add mobility to the flap. About one-third to half of the muscle is then divided at its medial border, away from the hip joint capsule which should not be exposed. It is important to be aware of and to avoid the sciatic nerve that runs under the muscle. At the submuscular level the dissection is extended in cranial and medial directions. The tissue layers are kept intact to avoid interruption of the perforating vessels. Mobility is tested continuously; as soon as the muscle part of the flap reaches the muscle on the other side of the defect without tension, the dissection is terminated. One of the two main vessels supplying the flap may occasionally be divided to attain sufficient mobility. The flap is sutured in four layers with interrupted sutures: in the muscle, in Scarpa’s fascia, in the deep dermis and in the skin. Two drains are placed and kept for 4–6 days, one deep to the muscle and one along the flap in the subcutis. The wound is dressed with surgical tape. Any vaginal wall defects should be closed with absorbable sutures.

Skin incisions for the extended abdominoperineal excision and gluteus maximus myocutaneous flap in prone jack-knife position.
Postoperative rehabilitation programmes
As postoperative rehabilitation programmes already are in use at various centres, we do not consider it realistic to prescribe a uniform programme. Instead, the patients will be allocated to either an established programme6 or to an accelerated programme that has been used in another centre. Both rehabilitation programmes are standardised, written and should be followed explicitly. The descriptions of both programmes can be downloaded from the study homepage on the Internet. Participating centres must choose one of the prescribed rehabilitation programmes and use that programme for all their study patients. The rehabilitation programmes at hand have been studied earlier and are considered safe.10
Adherence assessment
Standardisation of surgery will be accomplished with site visits from (or to) Karolinska University Hospital, Solna, Stockholm, where the standards for GMF and APCI operations are defined.
Concomitant therapy
Preoperative or postoperative RT or and/or chemotherapy can be used according to the local multidisciplinary team (MDT) decisions.
Outcomes
The primary outcome is physical performance as measured by the TST,20 21 reflecting strength, balance and absence of gluteal tenderness.10 The test metric (seconds) will be compared with the upper limit of reference values, matched for age and sex. Each patient will be categorised into meeting this limit, or not; the summary measure is the proportion of patients meeting the limit. The time point of 6 months after surgery is chosen for the primary outcome, as at this time the wound healing process is considered to have reached steady-state.
The secondary outcomes along with measurement variables, analysis metrics, aggregation methods and measurement time points, are presented in table 1.
Secondary outcomes in the NEAPE trial
Measures of physical performance and quality of life
The study physiotherapist or nurse will examine measures of physical performance.
The TST is to be performed by recording the time needed to stand 10 times from a standard chair.20 21 This is a validated test which measures lower extremity muscle strength, muscle coordination and tenderness of the gluteal region (especially when sitting), and also enables comparisons to a reference population studied earlier.20
An optional and complementary step test is performed at some participating centres.22
The study physiotherapist or nurse will evaluate and document measures of pain, discomfort and ability to sit during the visits. Data will be registered on paper forms or directly in the electronic database. Pain in different postures will be evaluated with a 100 mm Visual Analogue Scale (VAS). Discomfort and anatomical distribution of pain will be mapped with a specific figure or chart where patients can indicate areas of discomfort or pain.
The patients’ ability to sit will be evaluated during the initial interview by observation of how the patients sit in the chair during the first 10 min. Three categories of ability to sit will be used: (a) normal sitting during 10 min, (b) sitting with some kind of aid (cushion or ring) or compensating weight-bearing with an unrelaxed posture and (c) not able to sit at all.
Quality of life is measured with the global instrument EuroQol-5D (EQ-5D) and the cancer-specific instruments European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 and QLQ-CR29. The forms will be sent home to the patient prior to the follow-up visits with a request to fill them and bring them to the clinic. The study physiotherapist or nurse will collect the completed forms. Completeness of data should be checked during the visit so that any incomplete data can be corrected together with the patient.
Evaluation of physical performance, pain, discomfort, ability to sit and quality of life mentioned above are performed before the operation (baseline examination), at 3 months, 6 months and 1 year after the operation.
Measures of complications including the surgical and oncological result
Measures of complications and the surgical as well as the oncological result will be considered and registered by the attending surgeon during follow-up visits. Postoperative complications will be classified according to the Clavien-Dindo23 taxonomy and registered on a paper form, or directly in the electronic database.
Definitions of surgical result and wound healing measures
The local surgical result in the perineal wound will be classified according to the validated24 Southampton Wound Assessment Scale (SWAS)25 (table 2). The wound healing grade is registered for each patient at the 3 month follow-up event and applies for the present status or for the postoperative period up to 3 months, as the worst grading noted during this time should be recorded.
The Southampton Wound Assessment Scale25
In addition, at all follow-up visits there is registration of (a) persisting sinus or fistula in the perineal wound, (b) removal of implant (only APCI), (c) excision of a myocutaneous flap in part or whole (only GMF) and (d) occurrence of perineal hernia.
The healing of the laparotomy wound is not graded in this study but disturbances of such wound healing will be registered as an adverse event among other circumstances.
Definitions of oncological result
Local recurrence and/or metastatic disease are registered as soon as the attending surgeon has verified the existence of the complication. The diagnosis may be based on clinical examination, histology, radiological examination or a combination of investigations. Data on local recurrence and metastatic disease will be registered at every follow-up visit.
Safety measures, early postoperative complications and other clinical adverse events
Postoperative complications will be registered in the Swedish Colorectal Cancer Registry26 via the so-called information network for cancer treatment (INCA) web application directly by the participating units within Sweden. The registry collects data of postoperative complications occurring in the time intervals 1–30 days and from 31 days until 5 years after the index operation. This registration is routine for all patients treated for rectal cancer in Sweden and is not changed for patients participating in the study. Analysis of data on postoperative complications can be done for the early period as soon as the registration of the operation is completed in the registry. The delay of registration of the operation in this registry may vary between different units, but should be done within 2 months. The registration of complications occurring in the later period (31 days until 5 years) takes place after every follow-up visit and this data can be used as a safety measure during the study.
Participating units outside Sweden cannot register early or late postoperative complications in the Swedish Colorectal Cancer Registry, but a similar registration form will be available via the study homepage (www.norrlandskirurgi.se) for use of units outside Sweden.
Both the surgeon and the physiotherapists (as well as study nurses) involved in the follow-up examinations of patients should report every serious adverse event that is observed among enrolled patients later during the study. The reports of adverse events are made via the study homepage for units outside Sweden and in the Swedish Colorectal Cancer Registry for units in Sweden. These reports are continuously collected and evaluated by the study administration, and if any safety concern with the study appears, an independent advisor is consulted. This advisor has the authority, together with the principal investigator (PI), to stop the study if serious unexpected safety issues are observed. A decision to terminate the trial must be written, motivated in detail and distributed to all participating centres without delay.
Participant timeline
Entry procedures
Patients with primary or recurrent malignancies of the rectum are screened for enrolment during workup for assessing pre-treatment stage of the disease. It is not mandatory to document the screening process, and we acknowledge that the degree of screening may vary between participating centres.
Definitions related to registration
For this study, the following definitions are used:
Enter: The act of assessing eligibility of a patient for the study. All patients planned for APE or EAPE should be entered. This registration process can be performed before enrolment/randomisation (recommended) or at the same time as enrolment/randomisation (or postoperatively for those not randomised/enrolled).
Enrol: The act of assigning a patient to a treatment alternative by randomisation in the study. When the randomisation is done on the web application, the patient is registered with status entered and enrolled. The informed consent document must be signed by the patient before enrolment.
Registered patients: This denotes all patients registered (entered and enrolled, or only entered), who are assessed for eligibility when they are planned for APE or EAPE during the inclusion phase of the study. If the patient cannot be enrolled (randomised) because of intraoperative or preoperative circumstances, the entry must be registered via the web application without randomisation.
Disease diagnostic criteria
The diagnosis of rectal malignancy should be determined by histology before enrolment, but absence of definitive histology is not an exclusion criterion if the decision to operate leans on sound clinical judgement. Primary cancer of the rectum is defined as a malignancy that is not treated with curative intention before the operation. This definition allows preoperative oncological treatments if the plan is to cure the patient with surgery. Recurrent cancer is defined as a cancer that develops after a previous treatment with curative intention. The previous treatment does not have to be surgical.
Enrolment process
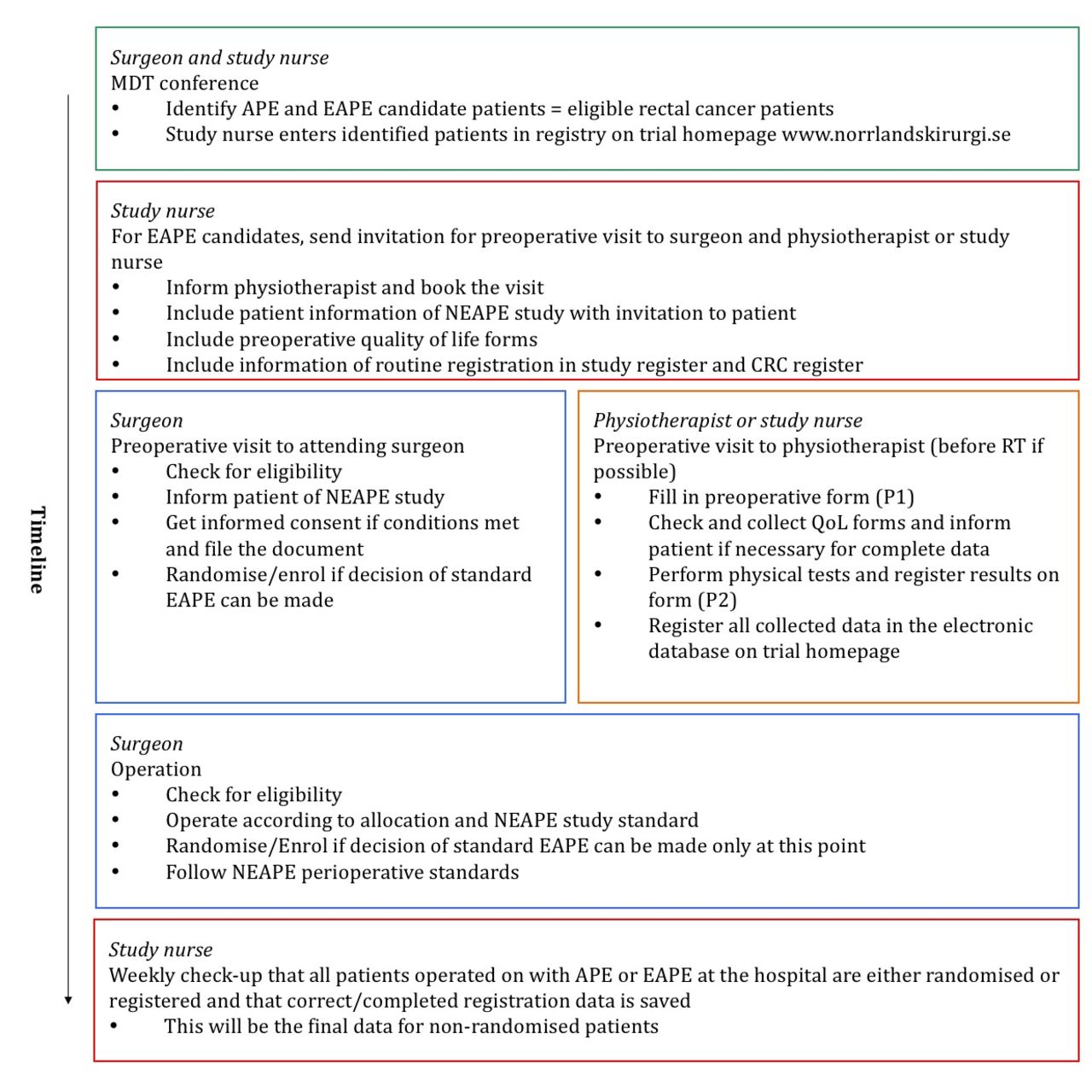
The enrolment of a patient in the study is finalised with the randomisation procedure done with a web application on the Internet. The enrolled patients are examined by a physiotherapist or a study nurse who is familiar with the protocol and the standard operating procedures (SOP) of the study. Examinations of physical performance, registration of quality of life and background information takes place within 1 week before the start of RT (or operation if examination before RT cannot be accomplished). Physical performance, quality of life and wound healing is examined 3, 6 and 12 months after the operation. A late follow-up at one time point at least 5 years after the operation can be executed if previous analyses indicate a need for long time follow-up; this evaluation will focus on long-term function such as ability to sit, chronic pain and complications such as perineal hernia. A flow chart of the study is shown in figures 2 and 3.

Flow chart of the NEAPE trial in the perioperative stage. APE, abdominoperineal excision; CRC, colorectal cancer; EAPE, extended APE; MDT, local multidisciplinary team; NEAPE, Nordic Extended Abdominoperineal Excision; QoL, quality of life; RT, radiotherapy.
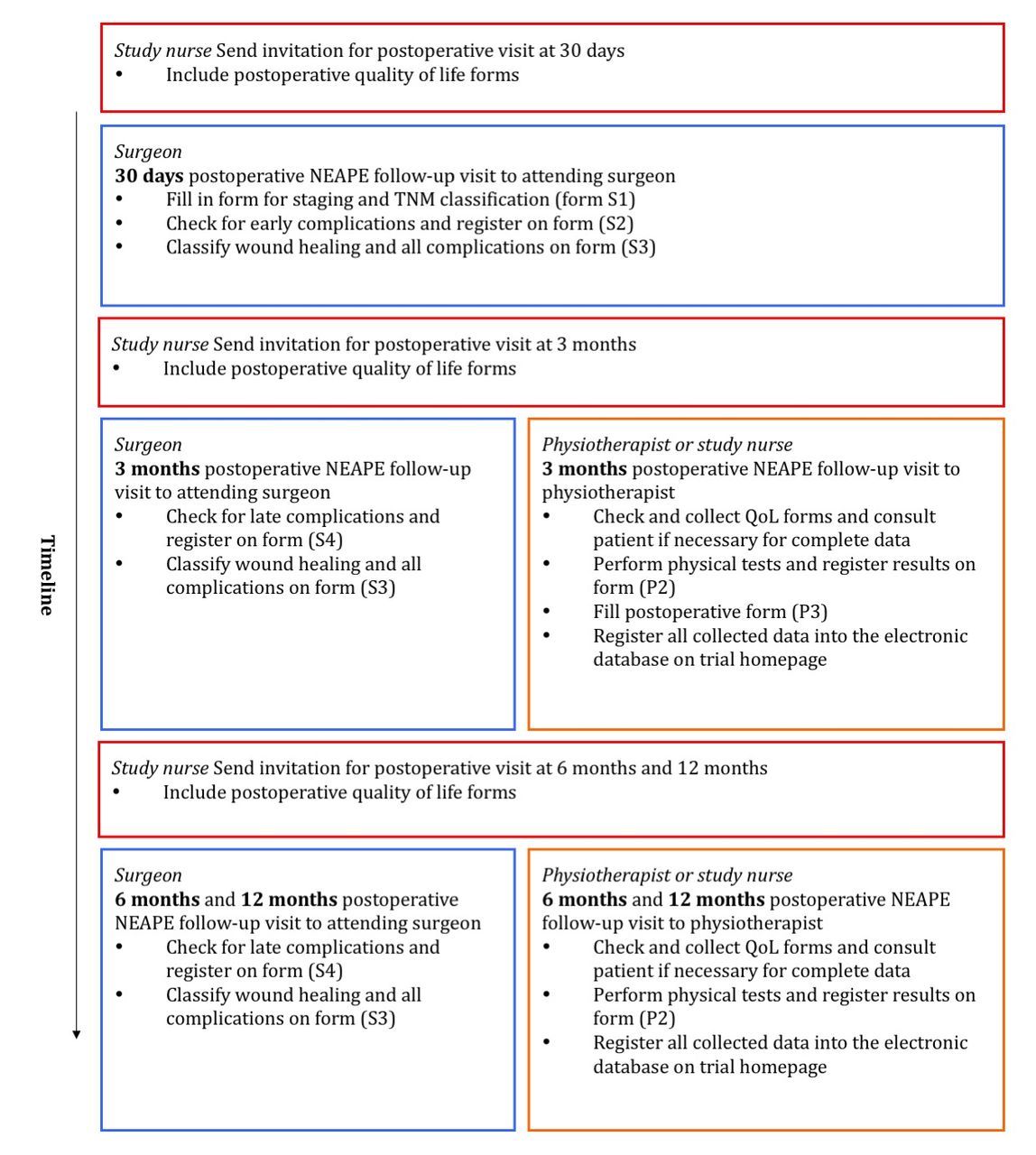
Flow chart of the NEAPE trial in the follow-up stage. NEAPE, Nordic Extended Abdominoperineal Excision; TNM, tumour, node, metastases.
Discontinuations
Different situations resulting in discontinuation may arise:
If a patient who does not meet eligibility criteria is inadvertently enrolled, that patient should be discontinued from the study and the PI of the central study administration must be informed.
Inevitable discontinuations, as if patients decease or are lost to follow-up are registered by the site investigator via the web application.
The patients are allowed to discontinue from the study without any reason if they wish according to ethical standards. If a patient chooses to discontinue from the study he/she should be asked if the study data collected until this point can be used or should it be erased.
All discontinuations should be registered via the study homepage. Outcome data from patients discontinued for reason 1 will be erased and are not included in the final analysis. Outcome data from patients discontinued for reason 2 (above) can be used until the date of discontinuation, while outcome data from patients discontinued for reason 3 can be used until the date of discontinuation or all data will be erased depending on the patient’s decision.
Sample size
The sample size is considered in relation to proving non-inferiority of the experimental APCI arm to the control GMF arm in terms of the primary outcome. The sample size is calculated with the following assumptions:
Proportion of patients with low performance in TST with GMF is estimated at 63%.
Proportion of patients with low performance in TST with APCI is estimated at 40%.
The non-inferiority margin is set at 10%.
The loss of data due to for example, mortality or discontinuation, is anticipated to be 10%.
The assumption concerning GMF is based on a prior study on this patient group,10 whereas the assumed share of low-performing APCI patients is our informed estimation, as no studies have been conducted using the TST on this patient group. The non-inferiority margin for the study is set on the basis of a minimally important clinical effect, which is also a subjective judgement of the best expertise available. This approach remains the only alternative since there are no trials using sham surgery in the field for guidance and for practical and ethical reasons such trials are not possible to conduct. With the above assumptions, a total of 76 patients (38 in each arm) are needed for 90% statistical power and a significance level of 5%.27 Considering attrition and missing data as well, 85 patients are necessary.
Recruitment considerations
We anticipate that study recruitment can be complete within 3 years, assuming that about 10 Nordic centres of differing sizes include 6–12 patients per year. To ensure rapid and thorough recruitment, we recommend that a study nurse enter/register a patient immediately after an MDT conference, in which a decision has been made to perform either APE or EAPE on the particular patient. We also recommend that the patient should be informed early, in conjunction with the invitation to a preoperative visit, about being included in the study register and for Swedish patients, in the national colorectal cancer registry.26 When the surgeon subsequently examines the patient preoperatively, the patient can be informed about the study, asked about participation, informed consent can be obtained and the patient can be enrolled/randomised if an EAPE operation is decided and the patient is eligible. The randomisation can be postponed to the operating room (intraoperative randomisation) if there is uncertainty of fulfilment of inclusion criteria up to this point. If the patient refuses participation and do not want registration or enrolment and the registration was already done by the nurse, a request of erasing the registration should be communicated to the study administration. This applies only for patients that do not want to be registered. Note that patients can refuse enrolment in the study but still accept registration which means that the study administration knows about that an APE or EAPE operation is planned or performed. In these cases, the registration stays but the patient is not randomised/enrolled. During the inclusion phase of the study, we recommend that the study nurse does a weekly check-up for patients operated during the past week with APE or EAPE. The nurse should secure that all these patients are either randomised or registered with limited but correct data. The data for non-randomised patients will be complete at this stage, later necessary for the Consolidated Standards of Reporting Trials (CONSORT) diagram in the final reports. The NEAPE trial enrolment process is illustrated in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Illustration of the enrolment process in the NEAPE trial. APCI, acellular porcine-collagen implant; APE, abdominoperineal excision; EAPE, extended APE; GMF, gluteus maximus myocutaneous flap; NEAPE, Nordic Extended Abdominoperineal Excision.
Assignment of interventions
Allocation
After patients give written informed consent and meet criteria for enrolment they may be randomised to one of the study arms before the operation if the EAPE procedure is decided upon and will be performed. If there is any doubt of the suitability of the procedure, and the definitive decision of EAPE is made in the operating room, the randomisation can be done intraoperatively. In these cases, written informed consent must be given before the operation and the patient is informed that the surgical technique is assigned during the operation.
The randomisation will be done online via a web application on the study homepage. Participants will be randomly assigned to either the control or the experimental arm with a 1:1 allocation. Permuted blocks are used and the computerised randomisation is stratified by centre and mode of preoperative RT, falling into three categories: (1) short-course preoperative RT, (5×5 Gy) with operation within 1 week from last RT dose, (2) short-course preoperative RT, (5×5 Gy) or long-course preoperative RT (25×2 Gy) with operation 4–8 weeks from last RT dose and (3) earlier RT of the lesser pelvis in connection to a previous therapy, but no additional RT before the current operation, or other RT dose or timing of operation. The stratification and block-randomisation ensure that all above defined subgroups of patients will contain patients allocated evenly (or close to evenly) in both study arms. The size of the randomisation blocks will vary by chance within predefined concealed limits.
Concealment mechanism
In order to alleviate selection bias due to inadequate concealment, the permuted block sizes will not be disclosed to neither the PI nor the co-investigators. The ‘raw’ allocation list was produced by a statistician and was further subdivided for specific centres and stratification groups by a system developer. The entire process of randomisation is completed on the study homepage, coding of which has been done by a system developer completely separated from the remainder of the study recruitment, conduct and subsequent analysis. The numerous centre and group specific allocation lists are stored on a secure server, accessible only by the above system developer who is working at Information and Communication Technology Services and System Development, Umeå University.
Blinding
Blinding in surgical studies is difficult to accomplish. This study is performed without attempts for blinding and thus the attending surgeon, the examiner of physical performance and the patient do not have to be blinded. This may cause detection bias by the assessors, a bias which is partly reduced by the use of validated outcome scales and questionnaires.
Data collection, management, analysis
Data collection methods including retention
The trial data will be collected as a consequence of routine registration in the Swedish Colorectal Cancer Registry, but also by using study-specific case report forms (CRFs); for centres outside of Sweden and thus not included in this registry, identical forms will be distributed.
Surgeons participating in this trial are asked to provide general clinical data from the first postoperative visit (supplementary file: Forms S1 and S2), specific complication data from all postoperative visits (supplementary file: Form S3) and late general complication data from visits later than 30 days after surgery (supplementary file: Form S4). Instructions for completion of these forms are found on the study homepage and on the forms themselves, and no specific training of the surgeons is undertaken.
Supplementary file 1
Supplementary file 2
Supplementary file 3
The physiotherapists and study nurses involved will fill in CRFs prior to treatment regarding general and physical health (supplementary file: Form P1), the primary and some secondary outcomes before and after surgery at various time points (supplementary file: Form P2), and data on RT as well as surgical technique and manufacturer of implant. (supplementary file: Form P3). In addition, at these pre- and postoperative visits, quality of life forms will be used (supplementary file: Forms EQ-5D, EORTC-C30 and EORTC-CR29). The physiotherapists and study nurses who participate receive specific training in the correct filling of forms, execution of physical performance tests and interpretation of outcomes and registration.
Supplementary file 4
Supplementary file 5
Supplementary file 6
Supplementary file 7
All study data will be registered on paper forms or directly in the electronic database, which comprises a study-specific extension of the regular Swedish Colorectal Cancer registry. The Regional Cancer Centre in the Northern Healthcare Region in Sweden is responsible for this registry, providing secure data storage. Paper CRF data will be transferred to this database using single input.
Compliance and retention
The study adds time that is consumed for the follow-up procedures of involved patients. Patients may have to travel long distances for follow-up visits for the study. From the patient’s perspective, this can be a positive experience provided that attempts are made to take care of the possible and actual problems that the patient may suffer from. For this reason, we recommend that all follow-up visits for the study are combined with visits to the attending surgeon, as this might increase the compliance to follow the study plan. A separate detailed SOP (protocol of standardised examination procedures) will be available for the physiotherapists and nurses involved in the study. A prestudy meeting for standardisation of examinations and in-depth study of the SOP will be arranged for participating centres.
Statistical methods: outcomes, additional analyses, analysis population and missing data
Analysis principles
All primary analyses in this study will be performed according to the intention-to-treat (ITT) principle, that is, patients will be allocated to treatment groups corresponding to their assigned treatment, even if the patient does not receive the correct treatment.
The ITT population will consist of all randomised patients who are operated with EAPE.
If non-inferiority is accomplished in the primary analysis, we will perform a per-protocol analysis in addition to the ITT analysis; if the results from the per-protocol are qualitatively similar, such an approach will provide more evidence of non-inferiority. The per-protocol population will consist of all patients in the ITT population who have met all protocol requirements and who have successfully completed the trial, including the 1 year follow-up.
Patient discontinuations
Reasons for discontinuations in the study will be compared between the two treatment groups. Tables or a CONSORT28 diagram will reveal the number and proportion of patients who have completed the study as well as patients that have discontinued, grouped by reason for discontinuation.
Primary outcome analysis
The main analysis in this trial consists of a comparison of the proportion of patients that perform worse than the upper limit of age- and sex-matched reference values for the TST at 6 months after surgery; the χ2 test will be used in an ITT analysis. A sensitivity analysis will be conducted, with adjustment for the stratification variables (ie, centre and RT category), as well as preoperative variables indicating for example, persistent musculoskeletal pain, chronic analgesic treatment, neurological disorders and previous arthroplasties. These adjustments, using binomial regression, are done in order to alleviate the impact of chance confounding, as this is a relatively small trial; estimates of relative risk ratios and absolute risk differences with 95% CIs will be produced. The same adjustments will be performed in the per protocol analysis, with the addition of confounders related to crossover from the experimental to the control arm, and vice versa; these covariates include tumor, lymph node and metastases (TNM) class, age and american society of anesthesiologists (ASA) class. There is also a risk of attrition bias due to patient knowledge of the treatment, as a GMF more than an APCI might reasonably induce patients to come to physiotherapist visits. If compliance to testing between groups differs more than 10%, an analysis with adjustment for prognostic factors will be done, that is, those factors also causing non-compliance such as TNM, age, ASA class.
Missing data
The amount of missing data will be appraised and according to type of variable and grade of missing, different strategies will be used. For the primary analysis, the 12-month TST measure will be imputed for a missing 6-month measure, as it is assumed that few differences in wound healing take place between these time points. Otherwise, a complete case analysis is planned for the primary outcome; however, multiple imputation techniques will be used for missing covariates in the sensitivity analyses and for missing quality of life data.
Secondary analyses
Comparison between proportions in study arms will be made with the χ2 test or the Fisher’s exact test, while comparisons of continuous variables will be made with the Student’s t-test or Mann-Whitney U test, as appropriate. The pertinent outcomes and time points are outlined in Table 1. The following comparisons between study arms will be conducted:
Change of physical performance, that is, the difference between preoperative and postoperative results in TST, evaluating the difference in proportions meeting the upper reference values.
Primary wound healing, categorised in subclasses (SWAS).25
Complications, categorised according to classification by Clavien-Dindo.23
Ability to sit, defined in three classes.
Pain and discomfort in gluteal region measured with VAS.
Quality of life, measured with EQ-5D and EORTC forms C30 and CR29, with the individual responses summarised to a health utility index using an appropriate table for the general population.29 30
Length of hospital stay.
Costs of surgical treatment.
Quality-adjusted life years.
Occurrence of local recurrence.
While the primary outcome analysis is considered confirmatory in nature, the above secondary outcome analyses are deemed subsidiary and thus exploratory. However, recognising that several statistical tests will be performed for the above secondary outcomes, we also plan to correct for multiple testing using the false discovery rate procedure.31
Subgroup analyses
Costs of surgical treatments and QALYs gained are calculated for a subpopulation of the study population. Registration of parameters needed for the health economic calculations is optional for the participating centres and the subpopulation will be included only from centres that collect health economic data in their computer systems. Costs of surgical treatments including surgical complications up to 12 months will be calculated according to health economic standards and QALYs gained will be compared between study arms.
Study status
As of 22 March 2019, 81 patients have been randomised from eight participating hospitals, while the total number of registered APE and EAPE patients amount to 487. Therefore, the planned 3-year recruitment goal has not been met, and the current assumption is that the NEAPE trial will be completed regarding the primary outcome in November 2019, when data analysis will ensue. During the recruitment period, some centres have ceased using myocutaneous flaps due to logistical difficulties, where, for example, plastic surgeon expertise has become unavailable, thus rendering further randomisation impossible; other difficulties such as availability of dedicated physiotherapist services have arisen also. This, along with sporadic uptake of the EAPE method, might explain the long recruitment period.
Monitoring and quality control
An independent observer will be appointed with the task to contact each centre yearly and ask for unforeseen adverse events and problems. If severe adverse events occur the PI and the independent observer have the responsibility to decide whether the study can continue or should be stopped after a safety analysis; no other interim analyses are planned in this study. All safety analyses comparing the treatment groups will be performed based on the intent-to-treat population. All statistical tests of safety will be conducted with a two-sided test, using an alpha level of 0.05. The safety analysis variables include, but are not restricted to:
Postoperative mortality within 30 days.
Postoperative complications grade IIIb or higher according to Clavien-Dindo.
Proportions of serious adverse events.
Quality assurance
To ensure accurate and reliable data the study administration will do the following:
Provide instructional material to the study sites, as appropriate (manual for physical examination etc).
Update study homepage at www.norrlandskirurgi.se with relevant information and study material.
Instigate start-up training and meetings with investigators.
Be available for consultation.
Conduct quality review of database (a monitor may be sent to participating centres).
There is no planned monitoring of the study interventions while the trial is under way; individual surgical teams and centres are responsible to adhere to the protocol.
Ethics and dissemination
Ethical review
This study will be conducted in accordance with the ethical principles stated in the most recent version of the declaration of Helsinki or the applicable guidelines on good clinical practice, whichever represents the greater protection of the individual. It is the responsibility of the investigators in other countries than Sweden to apply and hold the local ethical review board approval for the study.
Informed consent
The informed consent document (supplementary file: Informed consent) with study information will be used to explain in simple terms to patients what participation in the study means for the patient. The patient will receive information of the risks, benefits and the alternatives available.
Supplementary file 8
It is the investigators’ responsibility to ensure that informed consent is obtained from each patient or legal representative before enrolment in the study. The informed consent document must be signed, dated and subsequently stored in an archive at each participating centre. The signed document may also be photo-scanned to an electronic document and included in the hospital electronic patient file. Once the scan copy is secured to an electronic patient file, the paper document may be destroyed.
Patient and public involvement
This trial was not devised in direct collaboration with patients or public, although the authors’ experience as surgeons in the management of this patient group has informed the study design.
Confidentiality
The study participants’ data are entered from paper CRFs to an electronic data base. Each participant is deidentified, using a linking code, which is separate from the data base server; the code is encrypted, stored on a universal serial bus device and kept in a locked office space. Code access is limited to the PI and the independent observer, if need be. Only deidentified data is shared with co-investigators.
Access to data
The full dataset will only be accessible by the PI and the co-investigators who are involved in the analysis part of the drafted manuscripts.
Compensation for damage incurred
Every participant in the study may be compensated for damage incurred, by the regular insurance policy for patients as provided by the appropriate legal bodies in each Nordic country involved.
Publication policy
Every attempt will be made to reduce to a minimum the time interval between data collection completion and the release of study results. After data collection is finalised, we expect that a time period of at least 6 months is needed to compile the results and submit the findings to an appropriate journal. All results will be disseminated to the site investigators, patients and the general medical community.
Authorship rules
We aim to recruit co-authors for the reports of this study among the investigators in participating centres. The investigators in the three centres with the highest proportion of enrolments from patients undergoing an EAPE operation in this study will be offered co-authorship for reports and all other investigators will be acknowledged as participating investigators. If five or less centres are involved, one site investigator from each centre will be offered co-authorship.
Acknowledgments
MR revised the study protocol, advised on statistical analyses and provided critical review. JR collected advice from Swedish colorectal surgeons and assisted in the refinement of the study protocol and its implementation. MH initiated the study developed its design and wrote the protocol.
References
Footnotes
Contributors MR revised the study protocol, advised on statistical analyses and provided critical review. JR collected advice from Swedish colorectal surgeons and assisted in the refinement of the study protocol and its implementation. MH initiated the study, developed its design and wrote the protocol.
Funding County Council ofVästerbotten, Sweden, Grant VLL-187711 and Grant VLL-226241 with atotal amount of 1100 000 SEK. Swedish Society ofMedicine, Grant SLS-97651 and Grant SLS-176651 with a total amount of185 000 SEK. Swedish Society for Colonand Rectal Surgeons, Grant for start-up with a total amount of 25 000SEK
Competing interests None declared.
Ethics approval The principal investigator has applied for ethical board review at the Regional Ethical Review Board at Umeå University. The study was approved on 7 December 2010 with registration number 2010-335-31M. The application covers all study sites in Sweden, but centres in other countries may have to apply separately according to local regulations.
Provenance and peer review Not commissioned; externally peer reviewed.