Article Text

Abstract
Purpose Low-income and middle-income countries such as Tanzania experience a high prevalence of non-communicable diseases (NCDs), including anaemia. Studying if and how anaemia affects growth, placenta development, epigenetic patterns and newborns’ risk of NCDs may provide approaches to prevent NCDs.
Participants The FOETALforNCD (FOetal Exposure and Epidemiological Transitions: the role of Anaemia in early Life for Non-Communicable Diseases in later life) Study is a population-based preconception, pregnancy and birth cohort study (n=1415, n=538, n=427, respectively), conducted in a rural region of North-East Tanzania. All participants were recruited prior to conception or early in pregnancy and followed throughout pregnancy as well as at birth. Data collection included: maternal blood, screening for NCDs and malaria, ultrasound in each trimester, neonatal anthropometry at birth and at 1 month of age, cord blood, placental and cord biopsies for stereology and epigenetic analyses.
Findings to date At preconception, the average age, body mass index and blood pressure of the women were 28 years, 23 kg/m2 and 117/75 mm Hg, respectively. In total, 458 (36.7%) women had anaemia (haemoglobin Hb <12 g/dL) and 34 (3.6%) women were HIV-positive at preconception. During pregnancy 359 (66.7%) women had anaemia of which 85 (15.8%) women had moderate-to-severe anaemia (Hb ≤9 g/dL) and 33 (6.1%) women had severe anaemia (Hb ≤8 g/dL). In total, 185 (34.4%) women were diagnosed with malaria during pregnancy.
Future plans The project will provide new knowledge on how health, even before conception, might modify the risk of developing NCDs and how to promote better health during pregnancy. The present project ended data collection 1 month after giving birth, but follow-up is continuing through regular monitoring of growth and development and health events according to the National Road Map Strategic Plan in Tanzania. This data will link fetal adverse event to childhood development, and depending on further grant allocation, through a life course follow-up.
- anemia
- malaria
- embryology
- developmental programming
- epigenetics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The uniqueness of this study lies in the establishment of a population followed continuously before and during pregnancy with accurate estimation of gestational age using early ultrasound and detailed, high-quality data including fetal weight and placental blood flow monitoring.
To the best of our knowledge this is the largest preconception study (n=1415) conducted in a rural African setting.
The study involved stringent screening of important factors influencing fetal growth such as anaemia, prepregnancy nutritional status, gestational hypertensive disorders, diabetes, malaria and HIV.
The study included a substantial biobank of plasma, serum, cord blood and placenta, including stereology and epigenetic markers.
The study succeeded in recruiting more pregnant women than expected, but with a lower prevalence of anaemia than anticipated, therefore some outcomes may have less power including birth outcomes in severe anaemia. Yet, the higher number of mild anaemia cases might relate more to areas of the world where mild pregnancy anaemia prevails.
Introduction
Non-communicable diseases (NCDs) are a major public health concern1 2 causing 30 million deaths per year, of which 70% occur in low-income and middle-income countries (LMICs).3 NCDs are anticipated to overtake infectious diseases as the primary cause of death in Africa by 2030.3 Here, cardiometabolic diseases develop earlier and increase faster than in the ‘western’ world.3
Anaemia is a global health problem affecting 24% of pregnant women in Denmark to 36%–60% of pregnant women in LMICs such as Tanzania.4 Anaemia in pregnancy may decrease birth weight,5 and low birth weight (LBW) is associated with an increased risk of NCDs.6 Hales and Barker’s fetal programming hypothesis, linking LBW with risk for developing cardiometabolic diseases in later life,7 prompted us to hypothesise that anaemia before conception or during pregnancy could play an essential role in NCD programming. The alarmingly high prevalence of anaemia in LMICs is a key health threat, but is also an opportunity to reveal the role of anaemia in the global epidemic of NCDs and provide potential approaches to prevent NCDs, in particular, in societies in fast transition.
During pregnancy, anaemia is defined as haemoglobin (Hb) <11 g/dL, (preconception: Hb <12 g/dL).4 A major cause of anaemia is iron deficiency which compromises the fetal iron supply,8 9 and severe–moderate anaemia (Hb ≤8 or 9 g/dL) is associated with increased risk of being born small for gestational age (GA).5 10 Anaemia in the first two trimesters has been associated with decreased fetal growth and preterm delivery whereas the consequences of anaemia in the third trimester are less clear.5 11 12 Iron supplementation has indeed been shown to improve birth weight outcomes.5 13–15 The insulin-like growth factor (IGF) axis has been suggested to play a role in fetal response to anaemia.16 It is also debated whether high Hb concentration in pregnancy has a positive or negative effect on birth and childhood outcomes, that is, it has been shown that high Hb concentrations (≥14.6 g/dL) were associated with an increased risk of stillbirths in a Swedish case-control study,17 and furthermore that reduction in Hb concentration from early pregnancy to delivery was associated with increased birth weight.18 Anaemia in pregnancy has also been associated with adverse development of the placenta15 19 including increase in size and vascularity.20 In the placental villous bed, a switch from branching to non-branching angiogenesis in weeks 20–25 of pregnancy ensures proper placental development to accommodate the increasing nutrient and oxygen demand of the growing fetus.21 Anaemia may affect the oxygen tension and hence the vascular endothelial growth factor A (VEGF-A) and placental growth factor (PlGF) balance and the villous branching pattern.21 22
Tanzania is undergoing fast epidemiological transition from a population affected by anaemia and infectious diseases, towards NCDs within one generation.23 24 Malaria is prevalent in both Tanzania and many other LMICs, and is a major risk factor for anaemia and LBW.25 Therefore, malaria should also be considered when studying the effect of anaemia on pregnancy outcome. In spite of a high prevalence of anaemia and its potential severe consequences for mother and offspring, there are only few studies in LMICs that have followed women before pregnancy, throughout pregnancy until delivery,8 26 27 and none, to the best our knowledge, linking anthropometry, fetal growth, infections, growth hormones, micronutrients, placental blood flow, epigenetics, placental stereology and histology.
The FOETALforNCD (FOetal Exposure and Epidemiological Transitions: the role of Anaemia in early Life for Non-Communicable Diseases in later life) Study is a population-based preconception (n=1415), pregnancy (n=538) and birth (n=427) study, conducted in a rural region of North-East Tanzania. By using an interdisciplinary approach, the overall objective of this study is to evaluate anaemia-induced alterations of fetal and placental development and susceptibility to NCDs, taking into consideration the contribution of malaria. We anticipate the project will provide new knowledge on how health, even before conception, might modify the risk of developing NCDs and how to promote better health during pregnancy. The specific objectives are described below.
The preconception study
The objective is to characterise the health of women from a rural region in Tanzania, before conception. We will examine the prevalence and risk factors of anaemia (including malaria, micronutrient deficiencies and socioeconomic determinants) as well as of hypertension, diabetes and fertility.
The pregnancy study
The objective is to evaluate the effect of anaemia on fetal and placental development. We will evaluate how first-trimester and second-trimester compared with third-trimester anaemia and/or malaria alters fetal and placental development and later neonatal body composition. Placental development will be evaluated as degree of villous branching. Finally, we will characterise how first-trimester, second-trimester and third-trimester anaemia and/or malaria may change the VEGF-A/PlGF balance and the IGF-axis.
The -omics study
The objective of the -omics studies are to explore genetic variation (maternal and fetal), genome-wide DNA methylation and consequent RNA expression in cord blood and placenta from pregnancies affected by anaemia and/or malaria compared with controls. Epigenetic variation established in utero has indeed emerged as a candidate mediator of long-term programming of NCDs.28 29 Characterisation of epigenetic changes after exposure to anaemia may potentially enable us to detect biomarkers to identify groups at risk of developing NCDs.
In this paper we present the overall set-up of the interdisciplinary study, including selection and baseline characterisation of the participating population.
Cohort description
Study setting
The field studies were conducted in Korogwe, Tanga Region, North-Eastern Tanzania (figure 1). The central field site was the Maternity Ward and the Reproductive and Child Health Clinic at Magunga Korogwe District Hospital (KDH). Mobile clinics were set up in 48 villages in the two districts, and 17 dispensaries (including Kwandolwa, Kerenge, Segera, Mgombezi, Makuyuni and Mbaghai) functioned as outreach satellite sites supporting the antenatal care provided by the study team (figure 1). Clinical investigations and sample collection took place at KDH, the dispensaries and mobile clinics in the catchment areas, whereas all follow-up activities during pregnancy were performed at KDH.

Map of Korogwe district and the dispensaries in the study.
Study groups and recruitment
Non-pregnant women were invited to participate in the preconception study. Sensitisation campaigns were held to ensure a sufficient number of participants. A total of 2629 women was screened for inclusion between July 2014 and December 2015. The inclusion criteria were based on a high likelihood of becoming pregnant within the study period and included: age between 18–40 years, a negative urine pregnancy test, not having tried to conceive for more than two consecutive years (regarded as subfertile), no usage of modern contraceptive methods except condoms, not having a child less than 9 months old, living in an accessible area, and on conception willing to attend antenatal care and give birth at KDH. The women were invited to participate in the pregnancy study if conception occurred between July 2014 and March 2016. To ensure early pregnancy inclusion, women were invited to report for pregnancy testing every third month or if they suspected they were pregnant.
The pregnancy study population was supplemented with screening of 445 women in early pregnancy from April 2015 to March 2016. These pregnant women were recruited on a 1:1 basis with a Hb ≤8 g/dL (severe anaemia) or Hb 8.1–10.9 g/dL (mild–moderate anaemia): Hb ≥11 g/dL (non-anaemic), and with a GA of ≤14 weeks based on ultrasound. Follow-up of pregnant women was completed in December 2016 when the last woman in the cohort gave birth.
Patient and public involvement
Patients or the public were not involved in the design of the study concept and protocol, but the research questions and outcome measures were developed considering the women included and disease patterns observed in our previous Strategies TO Prevent Pregnancy-Associated Malaria (STOPPAM) Study conducted in the same region.30 However, the logistic implementation of the present study including recruitment and retaining participants was conducted in close collaboration with the local communities and personnel in the governmental health systems.
Sample size calculations
Sample size calculation was originally based on the observed effect of severe anaemia (Hb ≤8 g/dL) in the second trimester on z-score of birth weight (−0.31) in the STOPPAM Study30 conducted in the same area, with a significance level of 0.05, power of 0.80 and assuming 15% lost to follow-up. With balanced inclusion into the study, we aimed to enrol 480 pregnant women in the first trimester on a 1:2 basis as the severe anaemia group (Hb ≤8 g/dL) versus a group that did not have severe anaemia. The latter group was further divided into two groups (8.1–10.9 g/dL and ≥11 g/dL). However, the percentage of women with severe anaemia was much lower than anticipated. Many of our aims are exploratory, not all depend on birth weight alteration, and the effect on placental development, vascularisation, the IGF-axis and epigenetic alterations might already be observed when moderate–mild anaemia is present, although the exact effect size is not known. It was therefore decided to continue with the study but by including the participants in a 1:1 ratio (Hb <11 g/dL vs Hb ≥11 g/dL). This might have resulted in too little power to detect the actual difference in birth weight, but still helps achieve the other objectives.
In addition, we aimed to include 1500 non-pregnant women irrespective of Hb levels, since it is unknown whether the effect of anaemia on developmental outcomes, including epigenetics, is continuous. Assuming that 30% would become pregnant within the project time line, and that 60% would be identified, we expected to include at least 270 pregnant women.
Data collection
An overview of the study activities and methods is shown in figure 2 and table 1.

Overview of study activities.
Study activities, data collected and methods used
Socioeconomic status, medical history and clinical examination
The following characteristics were documented at inclusion: ethnicity, socioeconomic status (based on housing, education and occupation), religion, partner characteristics (age, ethnicity, education and occupation), contraceptive methods, gravidity history, medical history and obstetric history, substance abuse, anthropometry, blood pressure (BP), Hb, diabetes, malaria and HIV. Intestinal helminths were tested in a subgroup of 486 women. Women with an average systolic BP ≥140 mm Hg and/or diastolic BP ≥90 mm Hg were scheduled for a follow-up visit to confirm BP status. Diabetes was screened for by measurement of blood glucose and HbA1c. If glucose levels were ≥11.1 mmol/L the woman was scheduled for a fasting blood glucose test.
During pregnancy, at all antenatal visits, the women were monitored for anthropometry, anaemia, infections and hypertensive disorders. Sickle cell trait, thalassaemia and glucose-6-phosphate dehydrogenase deficiency were examined, and an oral glucose tolerance test was done during pregnancy at 32–34 weeks.
All women were offered daily iron and folic acid supplementation from the time pregnancy was recognised and until delivery (combination tablet of 200 mg ferrous sulfate [~43 mg elemental iron] and 400 µg folate per day [Ferrolic–LF, Laboratory and Allied, Mombasa, Kenya]). If anaemia was diagnosed, it was treated with increased supplementation with either two to three combination tablets of iron-folic acid per day or with Hemovit multivitamin syrup (200 mg ferrous sulfate, 0.5 mg B6, 50 µg B12, 1.5 mg folic acid and 2.33 mg zinc sulfate per 5 mL [Shelys Pharmaceuticals, Dar es Salaam, Tanzania]) in a dose of 10 mL two to three times daily depending on severity.
Blood sample collection
Venous blood was collected in EDTA and serum tubes at the time of inclusion, all antenatal visits, delivery, neonatal visits if cord blood was missed and paternal visits (EDTA tube only). Serum tubes were kept light-protected and all blood samples were kept at 2°C–8°C until processed at KDH within 2 hours of collection.
Hb was measured at the time of inclusion, all antenatal visits and delivery. Bilirubin, ferritin, folic acid, vitamin B12, alanine aminotransferase, C reactive protein and albumin were measured at the time of inclusion, 32–34 weeks of gestation and delivery. Sampling of placental development markers (VEGF-A, Soluble fms-like tyrosine kinase-1 [sFlt-1], PlGF, Pregnancy‐associated plasma protein A [PAPP-A]) was performed at inclusion into the pregnancy study if before GA 11 weeks, at 11–14 weeks, 20–22 weeks and 26–28 weeks of gestation and delivery. Blood sampling for fetal growth markers (IGF-1, IGF-2, Insulin Like Growth Factor Binding Protein 1 [IGFBP1]) was performed at inclusion into the pregnancy study, 11–14 weeks, 26–28 weeks and 32–34 weeks of gestation and delivery in both venous and cord blood.
Ultrasound
Serial, transabdominal ultrasound was used to estimate GA using crown-rump length in the first trimester and head circumference in the second trimester.31 32 If included before week 11 of pregnancy, the GA was estimated again between weeks 11–14. Ultrasound for fetal weight was performed at GA of 20–22 weeks, 26–28 weeks, 32–34 weeks and 37–39 weeks of pregnancy. Additional ultrasound was done if intrauterine growth retardation was suspected and biweekly until delivery for all women diagnosed with gestational diabetes. The Hadlock formula on head circumference, abdominal circumference and femur length was used for weight estimation.33 Placental blood flow was estimated using both uterine and umbilical artery blood flow with pulsatile and resistance index as well as the systolic-diastolic ratio each time fetal weight was estimated. Uterine blood flow was also evaluated at weeks 11–14 and diastolic notching noted at each investigation.34 35
Newborn examination
At the time of delivery and at 4–6 weeks postnatally, weight, length, head circumference, abdominal circumference, mid upper arm circumference, skinfold thickness of biceps, triceps, subscapular and thigh of the newborn were measured. Newborn assessment was performed within 24 hours, and, if delayed due to home delivery, as soon as possible. Z-scores were estimated using a reference chart produced for Tanzania in the STOPPAM Study and the Intergrowth-21st reference charts.30 36–38
Cord blood and placenta samples for genetic analyses
Cord blood samples were collected in EDTA, serum and PAXgene tubes, primarily before the placenta was born. The placenta was processed within 15–20 min after delivery at the hospital, and for home deliveries within 2 hours, when possible. EDTA tubes were placed cold directly after collection and processed within 2 hours, including collection of buffy coat. PAXgene tubes were stored at room temperature for 2 hours, and subsequently at −20°C for 24–72 hours, before storage at −80°C.
The cord and amnion were removed, and the placenta was weighed. Using a biopsy punch, biopsies were collected from each quadrant, from the cord insertion and at the edge of the placenta at the area furthest from cord insertion. Each biopsy was washed with saline solution and divided into the maternal and fetal side. A ~1 cm3 cord tissue sample was collected from the cord end closest to insertion. All biopsies were snap frozen in liquid nitrogen and stored at −80°C. The placentas were macroscopically examined for signs of disrupted development. Membranes, cord, placental size, thickness, shape and parenchyma infarcts were described. Pictures of each placenta were taken to document morphology.
Genome-wide DNA methylation and RNA expression will be performed in cord blood and placenta biopsies using Illumina Infinium MethylationEPIC arrays and RNA sequencing on Illumina Nextseq. Genome-wide association studies will also be performed in both cord blood and maternal blood using CoreExome/OmniExpressExome Illumina arrays.
Stereological placenta samples
Ten full-depth placental tissue blocks were collected using systematic uniform random sampling and vertical sectioning, and conserved in 10% formalin. Isotropic uniform random sampling and Mattfeldt orientator was used to collect slides for paraffin embedding.39 Information of the sample position was collected regarding whether the sample block was from the placental periphery or centre. The slides were orientated so the vertical section contained both the maternal and fetal sides. The tissue was immunohistochemically stained with CD34 to visualise the vessels. Stereological analysis will be applied to assess the placental vascular morphology in placentae from women with or without anaemia and/or malaria during pregnancy. The total villi volume and vessel length, surface and diameter of transport and diffusion villi, will be examined.
Legal and ethical aspects
Explanation about the study was given to village leaders and community members before women were invited. After giving oral information, written informed consent (or thumbprints of illiterate women) was obtained prior to enrolment. All procedures were conducted in accordance with the Declaration of Helsinki. All participants were treated according to Tanzanian national guidelines. Antenatal and perinatal care followed guidelines from The National Road Map Strategic Plan.40 The project assisted all participants in obtaining the best local medical care available if disease was diagnosed.
Patients and public society were not involved in the design of this study.
Statistics
Assumptions of equal variance and normally distributed residuals will be visualised in Q-Q plots and histograms. For univariate analyses, normally distributed data will be presented as mean±SD and compared by Student’s t-test, whereas non-normally distributed data will be presented as median and IQR and compared by the Mann-Whitney U test. Proportions of categorical data will be compared using χ2 test. For multivariate analyses on risk factors for poor preconceptional health, and analyses on the effect of anaemia and malaria on fetal and stereological outcomes, multivariate regression analysis will be used. If appropriate, mixed regression modelling will be used on repeated outcome measures including fetal growth trajectories and biomarkers of placental and fetal development. For epigenetic analyses, appropriate bioinformatic analyses will be used taking into consideration the false discovery rates.
Findings to date
Preconception study characteristics
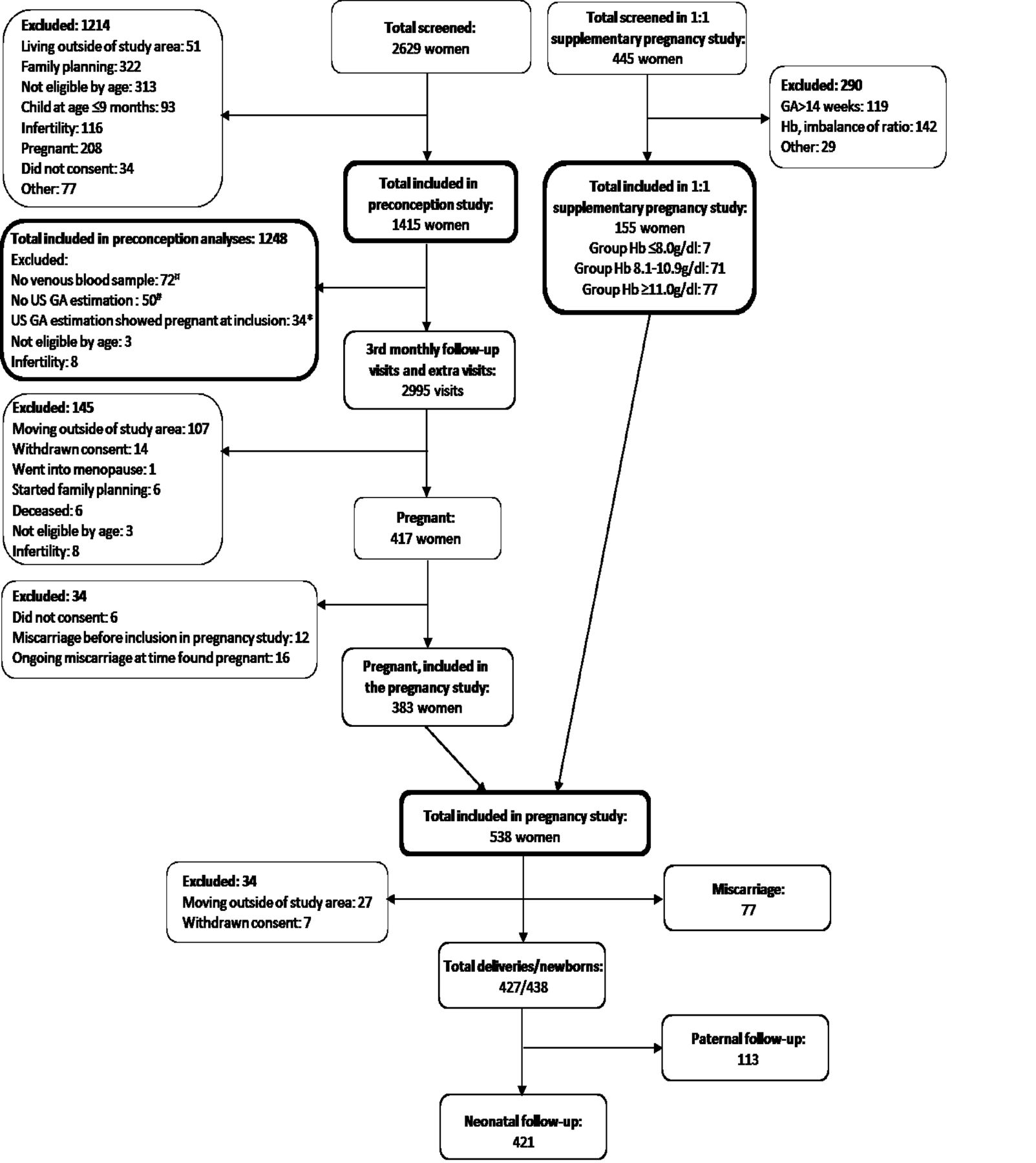
Of the 2629 women screened, 1415 were included in the preconception study (figure 3). Main causes for exclusion were use of modern contraception methods (27%) and age eligibility (26%). Among the 1415 women, 72 did not have venous blood collected at preconception, 34 had an ultrasound dated GA that showed they were already pregnant at time of inclusion (although very early in pregnancy) and 50 never had GA estimated with ultrasound. Additionally, 11 women were later found not to meet all inclusion criteria, leaving 1248 truly preconception women to be included in the final analyses (figure 3 and table 2). Average age, body mass index and BP of the 1248 preconception women were 28 years, 23 kg/m2 and 117/75 mm Hg, respectively (table 2). In total, 458 (36.7%) women had anaemia (Hb <12 g/dL) and 34 (3.6%) women were diagnosed as HIV-positive (table 2). Soil transmitted helminths were detected in 13 (2.7%) women.
{kind=link}
{kind=link}
{kind=link}
Overview of study cohort. Number of women screened, included and excluded in the preconception and pregnancy study. ¤: venous blood samples were not collected for 72 women at time of inclusion and were therefore excluded in the final analyses of the preconception study. #: 50 women were excluded because they never had GA estimation with US performed (this included 4 of the 6 women who refused inclusion into the pregnancy study, the 16 women who had an ongoing miscarriage when found pregnant, 18 women who had a miscarriage after inclusion into the pregnancy study and the 12 women who had a miscarriage in between preconception follow-up visits). *34 women were excluded because the US dated GA showed that they were already pregnant at the time of inclusion. GA, gestational age; Hb, haemoglobin; US, ultrasound.
Maternal characteristics in preconception study
Pregnancy study characteristics
A total of 2995 third monthly visits were conducted for the 1415 women. During these follow-up visits, additional 134 women were excluded for various reasons (figure 3). In total 417 women were later found pregnant and 383 women were followed during pregnancy (figure 3). Further, 155 women were included in the pregnancy study within the first 14 weeks of pregnancy, in a ratio of 1:1 (mild, moderate or severe anaemia versus non-anaemic). Of the 155 women, 7 had severe anaemia (Hb ≤8 g/dL), 71 had mild–moderate anaemia (Hb 8.1–10.9 g/dL) and 77 were non-anaemic (Hb ≥11 g/dL). In total, 538 women were included in the pregnancy study (figure 3).
During pregnancy, 359 (66.7%) women had anaemia (Hb <11 g/dL) of which 85 (15.8%) women had moderate-to-severe anaemia (Hb ≤9 g/dL) and 33 (6.3%) had severe anaemia (Hb ≤8 g/dL). In total, 185 (34.4%) women were diagnosed with malaria and 17 (3.4%) women were diagnosed with HIV during pregnancy. In total, 147 (27.3%) women were non-anaemic and never had malaria throughout pregnancy (table 3).
Maternal and birth characteristics and available samples, in the pregnancy study
Birth study characteristics
Of the 538 pregnancies (figure 3), 80 women had a miscarriage (16%), of which 72 were early (≤14 weeks) and 8 were late (>14 weeks, ≤22 weeks)—5 without and 3 with pregnancy outcome data collected at the time of miscarriage (figure 3 and table 3). The birth cohort consisted of 427 women (79%) having given birth to 438 neonates including the 3 women who had a late miscarriage at the hospital and complete outcome data collected.
For the 424 women who had given birth after week 22 of gestation, the average GA was 280 days, and 27/424 (6.4%) women delivered preterm (>22 weeks, <37 weeks). Average birth weight was 3016 g and 10.3% were born with LBW (<2500 g) among singleton live births without congenital anomalies. Twelve deliveries were stillbirths. Neonatal data were collected on 421 of the 426 live births (99%) (table 3 and figure 3). Among the 421 neonates with follow-up data, 13 neonates did not survive until day 28. For the remaining 408, neonatal anthropometric measurements were documented for 400 (98%) (table 3 and figure 3).
Only women with data on time of delivery/late miscarriage were considered potential for paternal follow-up, which was performed for 113 fathers (table 3 and figure 3).
Strengths and limitations
The uniqueness of this study lies in the establishment of a population that is followed continuously before and during pregnancy with an accurate estimation of GA using early ultrasound, and includes detailed, high-quality data of fetal weight and placental blood flow monitoring, stringent screening for development of hypertension or diabetes, and a substantial biobank of plasma, serum, cord blood and placenta, including stereology and epigenetic markers, which to our knowledge have not been collectively studied before in a rural African setting. Anaemia before, during and after pregnancy is much more prevalent in LMICs, compared with high-income countries (HICs) which mainly have high prevalence of anaemia during pregnancy.4
There are only few previous preconception birth cohort studies in sub-Saharan African countries, with participant numbers ranging from n=30 to n=376.26 41–43 These do not include data as comprehensive as in our study and do not include continuous ultrasound examinations, and biological sampling for both placenta stereology and epigenetics. To the best of our knowledge our present cohort study is the largest in sample size conducted in a sub-Saharan African country, with preconceptional data. The uniqueness of this cohort in contrast to other large birth cohort studies from more developed countries is the high co-occurrence of malaria and anaemia as well as presence of HIV, allowing us to study these exposures separately as well as simultaneously. Notably, few studies have been undertaken, exploring the potentially modifiable risk factor of anaemia for NCDs in later life through epigenetic monitoring.
The aims of this study include use of fetal and placental growth markers and epigenetic changes as end points in analyses of the effect of anaemia of fetal health. However, we acknowledge that these measurements are only proxy markers for future NCDs. It will be highly important to follow up the children of this cohort to further investigate the outcome of developmental programming with focus on risk markers of NCDs, for example, hypertension, metabolic profile and obesity. Longitudinal studies, commencing prior to conception and with continuous follow-up, are indeed required to unravel the potentially complex interplay between maternal health and offspring epigenetic profile to understand how epigenetic mechanisms may contribute to disease risk.
We succeeded in recruiting more pregnant women than expected, but with a lower prevalence of anaemia than anticipated, therefore some outcomes may have less power including birth outcomes in severe anaemia. Yet, the higher number of mild anaemia cases might relate more to areas of the world where mild pregnancy anaemia prevails, so our subsequent analyses may reveal if even slight decrease of Hb may have adverse effects. In addition, with this study design, we will be able to account for the effects of moderate-to-severe anaemia versus mild anaemia, versus no anaemia as well as high Hb concentrations. Still it is important to recognise that causes of anaemia may highly vary from LMICs to more westernised countries, that is, Denmark, and therefore the consequences of anaemia may also be different.
Although several studies report that prenatal anaemia is associated with adverse birth outcomes,5 10 prenatal iron deficiency is not necessarily associated with neonatal iron deficiency, as shown in a recent randomised control study by Angulo-Barosso et al.44 To account for the dynamics of iron deficiency during pregnancy, we have obtained repeated measurements of iron and Hb concentrations at preconception and throughout pregnancy. Cord blood serum and plasma are also stored and available for future measurements of iron markers. Therefore, we will be able to include the iron and Hb dynamics in subsequent analyses, which will improve the understanding of how maternal iron deficiency may or may not lead to fetal iron deficiency and adverse birth outcomes.
In conclusion, the FOETALforNCD Study includes interdisciplinary and transgenerational approaches enabling us to understand effects of anaemia and/or malaria on fetal development and programming for NCDs, including epigenetic mechanisms. The study is expected to shed light on the mechanisms behind the rapid epidemiological transitions in LMICs and whether risk factors for NCDs, beyond those well known from HICs, may have to be included to control NCDs in the next generations.
Acknowledgments
The authors thank all the participating women and men in the study, and all committed healthcare workers assisting in the care for the women and their children. The authors also thank the current and past FOETALforNCD Study team members in Tanzania (Agness Lugendo, Doris Bakari, Emmanuel Kessy, Maria Stuart, Neema Malle, Rashid Mtumba, Lightness Mswaga, Walter Maranga, Mwanamgeni Mwasema, Veronica Mtonga, Zeno Manjulungu, Gerson Maro, Edwin Ndunguru, Francis Mkongo, Andrew Kilimali, Elihudi Mwakiposa, Majuto Shebila, Salama Kiberiti, Simba Athumani, Mohamed Mapondela, Lucy Sarikoki, Eva Rimoy, Ester Cosmas) for their tremendous work efforts in recruitment, collecting data and generating the biobank. The authors are also thankful for the collaborations with the NIMR-Tanga Centre, Joint Malaria Programme and the administration at Korogwe District hospital.
References
Footnotes
Contributors Study design: SM, DM, OM, BBN, DLC, TT, KN, LGL, JL, CS and ICB. Epigenetic study design: LH, LGG, LG and RP. Project management: SM, DM, OM, JL, CS and ICB. Field work and data collection: LH, SM, DM, OM and CS. Statistical analysis: CS. Manuscript writing: LH, SM, DLC, LGG, CS and ICB. All authors approved the final manuscript.
Funding The study and core analyses were funded by the Danish Council for Strategic Research, grant number 1309-00003B.
Disclaimer The depiction of boundaries on the map(s) in this article do not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The map(s) are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Ethics approval Medical Research Coordinating Committee of the National Institute for Medical Research (reference number NIMR/HQ/R.8a/Vol. IX/1717).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data sets obtained and analysed in the current study are available from the last authors (Dr. Schmiegelow and Prof. Bygbjerg) on reasonable request.
Collaborators The FOETALforNCD data set is administrated by the Section of Global Health, Department of Public Health and the Centre for Medical Parasitology, Department of Immunology and Microbiology, both University of Copenhagen, Denmark. Data will be available and can be accessed upon reasonable request to the Section of Global Health, University of Copenhagen, and the senior authors of the present paper. Collaborations are encouraged with researchers working with similar cohorts or interested in initiating new future cohorts with the potential of complementing or replicating the findings in the FOETALforNCD cohort. Restrictions and requirements for reuse of the collected data include approval from the Tanzanian Medical Research Coordinating Committee of the National Institute for Medical Research ethics, and compliance to the signed consent form. Sharing of any data or biospecimens needs to be approved by the FOETALforNCD consortium.
Patient consent for publication Not required.