Article Text

Abstract
Objectives The aim of this research was to estimate the prevalence of type 2 diabetes mellitus (T2DM), impaired fasting glucose (IFG) and impaired glucose tolerance (IGT), in African women of childbearing age.
Study design Systematic review and meta-analysis of relevant African studies published from January 2000 to December 2016.
Data sources We searched several databases, including EMBASE, MEDLINE, CINAHL, grey literature and references of included studies.
Setting Studies carried out in African communities or any population-based studies were included.
Participants We included studies, carried out in Africa, with non-pregnant women of childbearing age. Studies must have been published between the years 2000 and 2016.
Outcomes The primary outcome was prevalent T2DM. The secondary outcomes were IFG and IGT.
Data extraction and synthesis Two reviewers independently extracted data and, using the adapted Hoy risk of bias tool, independently assessed for risk of bias. We used random-effects meta-analysis models to pool prevalence estimates across studies. We used Cochran’s Q statistic and the I2 statistic to assess heterogeneity.
Results A total of 39 studies from 27 countries were included, totaling 52 075 participants, of which 3813 had T2DM. The pooled prevalence of T2DM was 7.2% (95% CI 5.6% to 8.9%) overall and increased with age. The pooled prevalence was 6.0% (95% CI 4.2% to 8.2%) for impaired fasting glycemia while the prevalence of IGT ranged from 0.9% to 37.0% in women aged 15–24 and 45–54 years, respectively. Substantial heterogeneity across studies was not explained by major studies characteristics such as period of publication, rural/urban setting or whether a study was nationally representative or not.
Conclusion This review highlights the need for interventions to prevent and control diabetes in African women of childbearing age, in view of the significant prevalence of T2DM and prediabetes.
PROSPERO registration number CRD42015027635
- type 2 diabetes mellitus
- impaired fasting glucose
- impaired glucose tolerance
- women of childbearing age
- prevalence
- Africa
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- type 2 diabetes mellitus
- impaired fasting glucose
- impaired glucose tolerance
- women of childbearing age
- prevalence
- Africa
Strengths and limitations of this study
This research has included many population-based surveys from a broad range of African countries than previous systematic reviews has been carried out in a rigorous and transparent manner.
This is one of the first reviews to investigate the prevalence of type 2 diabetes mellitus (T2DM), impaired fasting glucose (IFG) and impaired glucose tolerance (IGT) in African women of childbearing age, a key population in the fight against the rise of non-communicable diseases in Africa.
One limitation of the research is that gender stratified data are not reported in many studies of T2DM prevalence, making them unusable in the current meta-analysis.
Further, this review has limitations in that the methods of screening for dysglycaemia and representativeness of the data in some of the included studies were not very satisfactory.
There was substantial heterogeneity in prevalent T2DM, IFG and IGT which could not be explained by the major study characteristics.
Introduction
Worldwide, the estimated number of people with diabetes has quadrupled from 108 million people in 1980 to 422 million in 20141 and is projected to reach 640 million by 2040.2 It is predicted that the greatest increase in numbers will occur in Africa, where in 2014, 14.2 million adults aged 20–79 years had diabetes, with over two-thirds unaware of their diabetic status.3 In African women in general, type 2 diabetes mellitus (T2DM) prevalence more than doubled, from 4.1% in 1980 to 8.9% in 2014.4 The rapid increase in diabetes has led to calls by the International Diabetes Federation (IDF) for the establishment of national diabetes programmes to better deliver prevention and control solutions.5 In line with the United Nations Sustainable Development Goal (SDG) 3.4, aiming to reduce premature mortality from non-communicable diseases (NCDs) by one-third by the year 2030,6 identifying special at-risk populations and delivering context appropriate interventions is one of the most important strategies in combating the T2DM epidemic.
Up to 70% of people with intermediate states of impaired glucose metabolism (impaired fasting glucose (IFG) and impaired glucose tolerance (IGT)) progress to T2DM within a decade.3 To date, most diabetes prevention programmes have focused on people with IGT, although some have intervened in another group at risk, that is, women with previous gestational diabetes (GDM). However, data on intermediate states of impaired glucose metabolism such as GDM, IFG and IGT are scarce in Africa. Overweight and obesity, the biggest single attributable risk factor for T2DM, is increasing in all African women, with the age-standardised body mass index (BMI) having increased from 21.9 kg/m2 in 1980 to 24.9 kg/m2 in 2014, possibly implying future obesity-driven T2DM increases in women.4 In 2017, the WHO, recognising the differential effects of NCDs (T2DM included) on gender, recommended a gender-based approach in prevention and treatment policies, in the Montevideo Roadmap 2018–2030.7
African women are affected by diabetes in more ways than their male counterparts, often assuming unpaid caregiver roles for affected family members in addition to taking care of their own diabetes/themselves.7 Further, if a woman with diabetes becomes pregnant, her unborn child is at an increased risk of developing T2DM in adulthood,8 thereby accelerating the intergenerational risk of T2DM. Mapping the prevalence of T2DM in this population is important as it has implications for future trends and monitoring of the T2DM burden in the Africa.
The WHO defines women of childbearing age as women aged between 15 and 49 years.9 Apart from the IDF estimates, a number of systematic reviews have investigated the prevalence of T2DM in Africa,1 10 11 but none have examined the T2DM prevalence in women of childbearing age, nor the prevalence of IFG and IGT in women of this age group despite their contribution to the risk of both GDM and T2DM. While two systematic reviews12 13 have examined GDM prevalence on the continent, reporting a prevalence ranging from 0% to 14%, the reviews highlighted the sparse data on GDM prevalence and the absence of active GDM screening programmes in most African countries. As T2DM and impaired glucose metabolism affect both maternal and child health, it is important to understand the prevalence of T2DM and its distribution in African women of childbearing age to inform better planning of preventive interventions and treatment and monitoring strategies.
The aim of this systematic review is to address the research question: what is the respective prevalence of T2DM, IFG and IGT in African women of childbearing age between 2000 and 2016? The T2DM estimates from this systematic review will complement those of the IDF to enable assessment of progress towards reaching the Global Action Plan for NCDs and SDG 3.414 in women of childbearing age.
Methods
The study protocol of this review is registered on PROSPERO and published in a peer-reviewed journal.15 We searched for eligible studies, published during the period 1 January 2000 to 31 December 2016, with the aid of an expert librarian, from the following databases; MEDLINE via PubMed, EMBASE via OVID, ISI Web of Science, Cochrane Central, Global Health, Scopus, CINAHAL, POPLINE, AfricaWide, Google scholar as well as grey literature databases such as OpenSigle. All the databases were searched using an African search filter. In addition, we hand-searched the reference lists of included studies and asked experts for any studies they knew of. We wrote to authors requesting non-reported data. The search strategy is shown in online supplementary appendix 1.
Supplementary file 1
Eligibility criteria
We included population based cross-sectional studies, published since the year 2000 as older studies would not have use the WHO 1998 T2DM diagnosis guidelines, that assessed the prevalence of T2DM in at least 100 African women of childbearing age, in any language. We excluded case–control studies, hospital-based studies and studies on migrant Africans. For the meta-analysis, we included only studies that reported age and gender-specific prevalences.
Study selection, quality assessment and data extraction
After the retrieval of articles and sorting duplicates, three reviewers (TC, IM and MW) independently screened the titles, abstracts and, if necessary, full articles for inclusion. The reviewers resolved any differences by discussion and consulted a fourth reviewer in the case of disagreement. The three reviewers assessed each included study for risk of bias and internal and external validity using the tool by Hoy et al 16 as adapted by Werfalli et al 17; online supplementary table 1.
Four reviewers (TC, MW, IM and LC) independently extracted from the selected articles, two reviewers per study. The investigators compared their findings and any differences were resolved through discussion. We extracted data on study characteristics including the first author’s name, date of publication, country where study was conducted, number of participants included and proportion of participants who were women of childbearing age, diagnostic method and diagnostic criteria, sampling method, response rate and unadjusted T2DM prevalence estimates.
Primary and secondary outcomes
The primary outcome was T2DM, defined as fasting plasma glucose (FPG) of at least 7.0 mmol/L, fasting blood glucose of at least 6.1 mmol/L, 2-hour oral glucose tolerance test (OGTT) plasma glucose of 11.1 mmol/L or an existing T2DM diagnosis.18 The secondary outcomes were IGT (fasting blood glucose <6.1 mmol/L and 2-hour OGTT blood glucose of at least 7.8 mmol/L but <11.1 mmol/L) and IFG (fasting blood glucose >6.1 mmol/L but <7.0 mmol/L).
Data synthesis and analysis
We compiled a summary of extracted data in a table and a narrative synthesis of all the 80 included studies. We then conducted a meta-analysis with the studies that provided age and gender-specific diabetes prevalence. Our population of women of childbearing age was defined as African women between the ages of 15 and 49 years, per WHO definition. However, in this review, we used the upper cut-off of 54 years as most studies used age groups starting from 15 to 24, 25 to 34, 35 to 44 and 45 to 54 years.
We pooled the T2DM prevalence using the statistical software STATA V.15,19 and metaprop package.20 We applied the random-effects meta-analysis framework as we expected variability in the prevalence estimates from different studies. The package first models the prevalence estimates using the exact binomial distribution and then applies the Freeman-Turkey double arcsine variance stabilising transformations, normalising the estimates before pooling and then back transforming the estimates. The pooled estimates are then computed using the procedure described by DerSimonian and Kacker.21
We assessed heterogeneity between studies using Cochran’s Q statistic22 and estimated the percentage of total variation across studies due to true between-study differences rather than chance, using the I2 statistic.23 We explored sources of heterogeneity through subgroup analysis using study-level characteristics. In addition, we assessed the presence of publication bias by examining the funnel plots, supplemented with a formal statistical testing using the Egger test24 and the Begg’s test25 for publication bias.
Patient and public involvement
We did not involve patients in the development of the research question, development of the study outcomes, design of the study or the conduct of the study.
Results
Search results
The flowchart of the search is shown in figure 1. Out of a total of 6046 studies identified via searches, 129 remained after removing obviously irrelevant studies and duplicates. A further 41 studies were identified through screening of references of included studies (13 studies) and from the WHO STEPwise country reports on the WHO website (28 studies). The final number of studies included was 78, of which only 39 studies were included in the meta-analysis as they reported age group and gender-specific diabetes outcomes. Forty-one studies were included in the narrative description only because either they did not report age group-specific data (38 studies) or reported only the percentage of participants with T2DM but did not report the raw frequencies (3 studies). There were two major age groups systems used by authors, 25 studies (64%) used the format: 15–24, 25–34, 35–44 and 44–54 years, 7 (18%) used the format: 20–29, 30–39 and 40–49 years. We merged some age groups into either of the two systems depending on which systems they were most related to, for example, the age group 18–25 years was merged with 15–24 years while the age group 20–29 years was merged with the 18–29 years. The remaining seven studies (18%), used other age groups which were very different from the two main systems described above (15–29, 30–44 years (four studies), 25–44 years (two studies) and <50 years (one study)) and we did not attempt to merge them into either of the systems.

Flowchart showing search, selection of and final included studies. IGT, impaired glucose tolerance; T2DM, type 2 diabetes mellitus.
Characteristics of included studies
Online supplementary appendix 2 shows the list and characteristics of all the 78 included studies from 39 countries. Most of the studies were from Nigeria, 14 (17.9%), South Africa, 8 (10.3%), Tanzania, 5 (6.4%), Cameroon, 4 (5.1%) Kenya, 4 (5.1%), Tunisia, 3 (3.8%); 10 countries contributed 2 eligible studies while the remaining 23 countries each contributed a single study. Most studies were published during the years 2014, 12 (15.4%), 2013, 11 (14.1%) and the year 2015, 9 (11.5%) and 2016, 7 (9.0%). Forty-five studies, that is, 57.7%, were conducted in both urban and rural populations, 19 (24.4%) in urban settings only, 14 (17.9%) in rural settings only and 1 study26 did not clearly state the setting. The reported response rate ranged from 40%26 to 100%.27 Of the 78 studies, 31 (39.7%) were nationally representative studies, with 28 (35.9%) of these being WHO STEPwise surveys and one national demographic and health survey from Namibia.28 Online supplementary appendix 1 contains the characteristics of the included studies.
Just over three-quarters of the studies, n=59 (75.7%) used FPG, 20 (25.6%) used the 2-hour OGTT, while 2 studies used the haemoglobin A1C (HbA1c) test for the diagnosis of T2DM. There were a total of 197 848 participants in the included studies of which the proportion of all women included ranged from 21%29 to 100%.27 The prevalence of T2DM in both sexes in the included studies ranged from 0.8%30 to 33%,31 while the T2DM prevalence in all women in the studies ranged from 0.5%30 to 36%31. Figure 2 shows the map of pooled T2DM prevalence for each country, in women of age 15–54 years. Regarding risk of bias, 74 (94.9%) of the included studies scored a low risk, 3.8% scored moderate risk and the remaining 3.8% scored high risk of bias (online supplementary appendix 3).

Map showing pooled T2DM prevalence in African women aged 15–54 years in each country. T2DM, type 2 diabetes mellitus.
T2DM prevalence in women aged 15–54 years
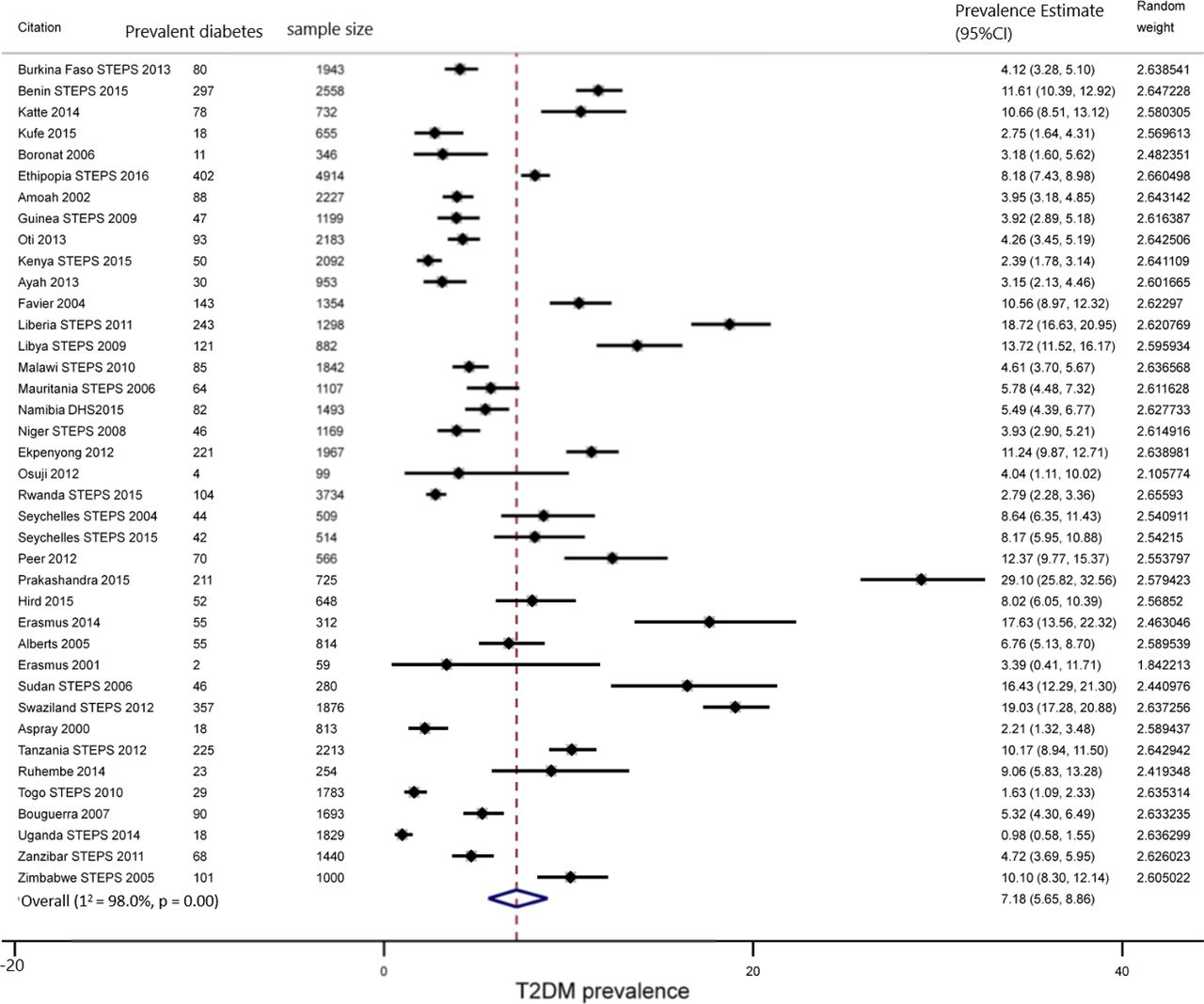
A total of 39 studies, from 27 countries, with 52 075 women of childbearing age, of which 3813 had T2DM were included in the meta-analysis. The T2DM prevalence in women aged between 15 and 54 years ranged from 1% in Uganda32 to 29% in South Africa.31 The pooled prevalence was 7.2% (95% CI 5.6% to 8.9%, n=39 studies), with significant heterogeneity (I2=98%, p<0.001), figure 3.

Forest plot of T2DM prevalence in African women aged 15–54 years, from studies published during the period 2000–2016. Studies must have used WHO 1999 or equivalent guidelines for the diagnosis of T2DM. T2DM, type 2 diabetes mellitus.
Prevalence of T2DM by age group
The lowest pooled T2DM prevalence was found in the 15–24 years age group (2.0%, 95% CI 1.0% to 3.4%, n=11 studies, I2 =83.2%, p<0.001) and the 25–34 years age group (3.0%, 95% CI 1.7% to 4.5%, n=24 studies, I2=90.0%, p<0.001). The highest pooled T2DM prevalence was observed in the 45–54 years age group (13.1%, 95% CI 9.8% to 16.8%, n=23 studies, I2=94.3%, p<0.001) (table 1 and online supplementary figure 1). T2DM prevalence significantly increased with age, compared with the 15–24 years age group, with a higher prevalence observed in the following age groups; 30–44, 35–44, 40–49 and 45–54 years (p<0.001) (table 1).
Summary of subgroup meta-analysis of T2DM, IFG and IGT in women aged 15–54 years
Prevalence of T2DM in urban and rural settings
The highest pooled T2DM prevalence was 9.2% (95% CI 5.5% to 13.7%, I2=97.7%, p<0.001) in the 11 studies from urban settings only, 6.6% (95% CI 4.9% to 8.6%, I2=98.2%, p<0.001) in the 26 studies with mixed urban and rural participants and 4.2% (95% CI 3.3% to 5.2%, I2=90.7%, p<0.001) in the 2 studies in participants from rural settings only; p=0.1418 (table 1 and online supplementary figure 2).
Prevalence of T2DM by diagnostic methods
The pooled T2DM prevalence was significantly higher in the 12 studies that used the 2-hour OGTT (10%, 95% CI 6.2% to 14.5%, I2=97.7%, p<0.001), compared with the pooled T2DM estimate in the 27 studies that used the FPG (6.1%, 95% CI 4.6% to 7.8%, I2=98.2%, p<0.001); p=0.003 (table 1 and online supplementary figure 3).
T2DM prevalence by period of publication
The median year of publishing was 2012. The pooled T2DM prevalence for the 18 studies published during the period 2000–2011 was 6.5% (95% CI 4.6% to 8.6%, I2=98.5%, p<0.001), compared with 7.8% (95% CI 5.6% to 10.4%, I2=97.0%, p<0.001) for the 21 studies published during the period 2012–2016; p=0.175 (table 1 and online supplementary figure 4).
T2DM prevalence comparing nationally representative and local/regional studies
The prevalence of T2DM was 7.4% (95% CI 5.4% to 9.8%, I2=98.3%, p<0.001) in the nationally representative studies compared with 6.9% (95% CI 4.6% to 9.6%, I2=98.3%, p<0.001) in regional and local studies; p=0.949 (table 1 and online supplementary figure 5).
IFG prevalence in African women aged 15–54 years
There were 22 studies from 17 countries with IFG data; 4 (18%) were South African, 2 (9%) were Cameroonian while the rest were individually from the remaining 15 countries. These studies included 34 483 participants, of which 2128 had IFG. The overall IFG prevalence was 6.0% (95% CI 4.2% to 8.2%) (figure 4). There was significant heterogeneity in the pooled estimate of IFG (I2=0.96, p<0.001). In subgroup analyses, there was no significant differences in the IFG prevalence between different age groups (p=0.870), rural and urban studies (p=0.603) and between the studies published during the period 2000–2011 and the studies published during 2012–2016; p=0.998 (figure 4, online supplementary figure 6 and 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing IFG prevalence in African women aged 15–54 years, from studies published during the period 2000–2016. IFG, impaired fasting glucose.
IGT prevalence in African women aged 15–54 years
There were six studies that reported age and gender categorised data on IGT; five of the studies were from South Africa, and one each from Ghana and Mauritius (online supplementary appendix 1). Due to the wide variation in IGT between the studies and the few studies available, meta-analysis was not performed. The lowest IGT prevalence (0.8%) was in women aged 15–24 years in South Africa in 2008 while the highest prevalence (37%) was in women aged 45–54 years in 2016, both in urban KwaZulu Natal province. In Ghana, IGT prevalence was 7.3% and 13.0% in women aged 25–34 and 45–54 years, respectively, while in Mauritius, in 2004, IGT prevalence ranged from 5.9% to 15.9% in women aged 20–29 and 40–49 years, respectively.
Publication bias assessment
We found no evidence of publication bias, as shown in online supplementary figure 8 and 9 and using Begg’s and Egger tests; for T2DM (Begg’s p=0.07, Egger’s p=0.293) and for IFG (Begg’s p=0.367, Egger’s p=0.202).
Discussion
The implications of diabetes on the health of both the mother and that of the offspring have been researched in detail elsewhere,8 33–36 and evidence is mounting that this may contribute to the developmental origins of chronic disease in exposed offspring, especially metabolic abnormalities, in later life.37–39 In this systematic review, we investigated the prevalence of dysglycaemia in African women of childbearing age, as reported in studies published during the period 2000–2016. The major findings of this systematic review and meta-analysis of 39 studies are an overall pooled T2DM prevalence of 7%, an overall pooled IFG prevalence of 6% while IGT prevalence ranged from 0.9% to 37%, with substantial heterogeneity in all three outcomes. Subgroup meta-analysis did not explain the heterogeneity observed. Further, we found a significantly higher prevalence of T2DM in studies which used the OGTT compared with studies which used the FPG for the diagnosis of T2DM.
To date, ours is the only systematic review that has assessed the prevalence of T2DM, IFG and IGT in women of childbearing age in Africa, thus limiting our ability to compare our findings with those of existing reviews. Most of the existing reviews have investigated the prevalence of T2DM, IFG and IGT either in both men and women or in all women. In 2015, the IDF, used an analytic hierarchical process which included sample representativeness, diagnostic criteria, sample size and age of study to select studies from which to estimate the T2DM prevalence. Only 13 high-quality data sources from 12 African countries during the years 2000 to 2015 met the stringent criteria for inclusion.3 However, there are notable similarities between our data and the IDF data for African women of childbearing age. The T2DM prevalence for African women aged 20–54 years from IDF data sources ranged from 0.001% to 32%, compared with our reported data which ranged from 0.5% to 36%. In the IDF data, reported T2DM prevalence in women aged 20–54 years ranged from 0.1% to 23% in Europe, from 1.4% to 43% in the Middle East and North Africa region, 1.3% to 34% in the North American and Caribbean region, 1.5% to 21.5% in the South and Central America region, 1% to 36% in the South East Asia region, while the highest reported T2DM prevalence was reported, as expected, in the Western Pacific region (range 0.1%–62%).
There are other published systematic reviews which did not investigate the T2DM prevalence in women only but rather in both African men and women (T2DM prevalence ranged from 1% to 12%).11 40 Hilawe et al,41 using a systematic review and meta-analysis of 36 studies, found a T2DM prevalence in African women aged 15 years and above in sub-Saharan Africa, of 5.9 (95% CI 4.6% to 7.6%), that overlaps with our finding of 7% (95% CI 5.6% to 8.9%). Our review differed from that of Hliawe in several areas. First, in contrast to Hilawe et al, we included only women from 15 to 54 years and not under the age of 15 years or women above 54 years. Second, Hilawe et al included studies from 1984 until 2011—only 23 studies are common to both reviews. Third, the diagnostic criteria differ: the studies included in the Hilawe et al review were based on the WHO or American Diabetes Association diagnostic criteria used at the time of the study, while the studies in our review all used a standard WHO 1998 criterion.
More recently, the NCD-Risk Factor Collaboration (NCD-RisC), using more data sources (76 reports), and robust methods, estimated the T2DM in 2014 at 8.9% in all African women.4 The difference between our prevalence estimate and the NCD-RisC estimate can be partly explained by the inclusion of older women in the later estimate, as T2DM prevalence increases with age. For example, Werfalli et al,10 using a systematic review and meta-analysis, found a T2DM prevalence of 15% in African women aged 55 years and above, highlighting the higher prevalence in older women.
We are also limited in comparisons of our IFG and IGT estimates with existing systematic reviews. Very few primary studies have reported IFG and IGT outcomes and, consequently, these are infrequently reported in systematic reviews and meta-analyses. The IDF’s 2015 report did not report IFG prevalence in Africa but estimated the IGT prevalence in African men and women at 7.9% (95% CI 4.8 to 21.7), which is in line with our findings. Bos and Agyemang40 in a systematic review of T2DM in North African countries found an IFG prevalence in all women of 5.1% (1 study) in Tunisia, 2.2% in rural Sudan and 13.1% in urban Egypt (n=5 studies). The review by Bos and Agyemang included studies published during the period from 1990 to 2012, and included any studies reporting diabetes, regardless of how it was defined, which makes it slightly difficult to compare with our findings.
We identified 22 studies which reported IFG prevalence while only 6 studies reported IGT prevalence. The smaller number of studies reporting IGT reflects that most epidemiological studies use the FPG, instead of the OGTT for the diagnosis of T2DM, IFG and IGT. The time requirement and labour intensive nature of the OGTT makes it an unfavourable tool for diabetes screening in epidemiological studies. However, there is mounting evidence that the two impaired glucose regulation states are distinct entities, with isolated IFG reflecting impaired insulin secretion while isolated IGT reflects impaired insulin sensitivity.42 43 Furthermore, the use of the FPG only for the identification of impaired glucose regulation states could result in up to 20% of IGT cases being missed.43 Several studies have shown that disorders in insulin secretion and sensitivity are already present when the FPG is within normal ranges and are more likely to be detected as IGT.42 44 Although it has been suggested that HbA1c could be used for screening for impaired carbohydrate metabolism,45 as it is more convenient, faster, does not require prior fasting and is becoming more affordable, there is no conclusive evidence on the HbA1c cut-off points that correspond to either IFG, IGT or both, in African populations.
Risk factors for T2DM in African women of childbearing age are on the increase, driven by the nutrition transition, urbanisation and decreasing physical activity.46 African women may be more insulin resistant than their Caucasian counterparts, while antiretroviral therapy for HIV contributes to more fat deposition in affected women.46 Further, in sub-Saharan Africa, HIV-positive women are more likely to be young and overweight or obese.46 In addition, evidence suggests that the mean BMI in African women increased from 21.9 kg/m2 in 1980 to 24.9 kg/m2 in 2014.4 All these factors suggest that we may see a high future diabetes burden in African women of childbearing age, compared with the present prevalence.
Africa is one of the continents where the IDF expects the greatest increases in the numbers of people with diabetes to occur between the years 2015 and 2035. African health systems are already overburdened by infectious diseases such as HIV, tuberculosis and malaria while at the same time catering for people already diagnosed with NCDs, diabetes included.47 Prevention of new cases is therefore a priority. Prevention of diabetes can be achieved using either a population-wide approach or a ‘screen and treat’ approach or a combination of both. The population-wide approach targets everyone through public health policies, for example, the sugar tax to help reduce overweight and obesity, advocated by the WHO,48 which has already been implemented in a number of European countries, such as Norway, Ireland and the UK, while in Africa, the tax was introduced in South Africa in 2017. On the other hand, the screen and treat stratergies, used in various diabetes prevention Programmes, involves identifying at risk groups, such as people with IFG, IGT or GDM, and offering targeted interventions, which are usually pharmacological, or lifestyle change interventions or a combination of both. Despite the success of various diabetes prevention programmes,49 in the USA,50 China51 and India,52 among other countries, studies investigating the effectiveness of either pharmacological or lifestyle change interventions in delaying or preventing T2DM in African women are scarce. In 2017, the WHO,7 in the Montevideo RoadMap on NCDs, stressed the double impact of NCDs such as T2DM, where women may become sufferers and unpaid caregivers to family members with chronic NCDs. In the same policy document, the WHO advocates for gender-based approaches to the prevention of NCDs. The prevention of T2DM in women of childbearing age is one such area where a gender-based approach will be appropriate. Women with IFG, IGT and GDM are special at-risk populations for T2DM. While we did not investigate the prevalence of GDM in this review, systematic reviews published in 2014 and 2015 found reported GDM prevalences as high as 14% in African women.12 13 Identifying women with IGT and IFG in Africa is not part of routine care or national programmes. On the other hand, many African health settings screen women for GDM, and perhaps this is a group with which screen and treat approaches could be used, to prevent or delay future T2DM, particularly in the maternal and child health context. Research is needed to investigate the effectiveness of lifestyle, and even pharmacological, interventions in delaying or preventing T2DM in African women with IFG, IGT and GDM, in the context of limited resources and possibly different modifiable environmental risk factors to those in the higher income countries.
A strength of the current study is that it is based on a larger number of population-based surveys from a broader range of African countries than previous estimates. However, the quality of included surveys, the inclusion of studies with small sample sizes, methods of screening for dysglycaemia and the representativeness of the data remain of concern. Of the 39 studies included in our meta-analysis, 20 could be described as nationally representative. All the 20 studies, except for the Namibian Demographic and Health Survey28 were WHO STEPwise surveys. Further, we acknowledge that variations in economic development may explain some of the heterogeneity across the studies and that our estimate may not be representative of the prevalences across the African continent due to this. Included studies rarely report data on the detection, treatment and control of diabetes/dysglycaemia as well as prevalent chronic diabetes complications in the surveyed populations. Therefore, the current review is unable to comment on the performance of health systems in preventing and controlling diabetes in African women of childbearing age.
We planned to use the WHO definition of women aged 15–49 years for this review, but as most studies utilised the 15–24, 25–34, 35–44 and 45–54 years age group system for operative reasons, we capped the upper age at 54 years. It is likely that we included a proportion of women who were not of childbearing age in the review, and consequently, that we may have overestimated the T2DM, IFG and IGT prevalence in our analysis.
Conclusions
Our study demonstrates that T2DM, IFG and IGT prevalence are high in African women of childbearing age. Due to the long-term and short-term implications, on both the mother and child of any form of diabetes, it is imperative to develop interventions targeted at at-risk women, within the maternal and child health framework.
Acknowledgments
Dr Jennifer Hirst, Nuffield Department of Primary Care Health Sciences, University of Oxford—for assistance with formatting forest plots. Mr Shakespear Makamanzi and Dr Alfred Musekiwa, CDC Pretoria—for assistance with plotting the map of pooled T2DM prevalence in African women aged 15–54 years per country.
References
Footnotes
Contributors TC: conception of, drafting and revision of manuscript, data extraction and data analysis. Guarantor of review. IM: revision of manuscript and data extraction, and approval for final submission. RLC and MW: revision of manuscript, data extraction and risk of bias assessment and approval for final submission. APK: conception of, drafting and revision of manuscript, data analysis and approval for final submission. SAN: conception of, revision of manuscript and approval for final submission. NL: conception of, revision of and approval for final submission.
Disclaimer The depiction of boundaries on the map(s) in this article do not imply the expression of any opinion what so ever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The map(s) are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data relevant to the study are included in the article or uploaded as supplementary information. This is a systematic review and meta-analysis of published data. The data may be available in the primary studies.
Patient consent for publication Not required.