Article Text

Abstract
Objectives Investigate the prognosis of adolescent knee pain, and evaluate its impact on health, care-seeking and career choices 5 years later.
Design Pre-registered, prospective cohort study.
Setting Population-based cohort initiated in school setting.
Participants From a cohort of 2200 adolescents aged 15–19 years in 2011, 504 reported knee pain on at least a monthly basis, and were followed prospectively in this cohort study, together with 252 controls who did not have knee pain in 2011.
Main outcome measures Outcomes included the Pain and Symptoms subscales from the Knee injury and Osteoarthritis Outcome Score (KOOS), pain intensity measured with a Numeric Rating Scale, pain frequency, knee-related and health-related quality of life, sports participation, physical activity level, KOOS subscales: Function and Sport/recreation, quality of sleep, healthcare consultations, treatments received for their knee pain, the use of painkillers and impact on choice of job or career.
Results At follow-up, 358 (71.0%) from the knee pain group and 182 (72.2%) from the control group responded. Of note, 40.5% (95% CI: 35.4% to 45.6%) from the knee pain group reported knee pain 5 years later which was frequent and intense compared with 13.2% (95% CI: 8.2 to 18.1) of the control group. Those from the knee pain group still suffering from knee pain reported poorer physical health (13 points worse on KOOS Function and 30 points worse on KOOS Sport/recreation), stopped or reduced their sports participation because of knee pain (60%), reported worse sleep quality and worse knee-related and general quality of life. In terms of health behaviours, those still with knee pain reported more healthcare consultations. One-third used pain killers regularly, and 15% (95% CI: 12% to 20%) reported that knee pain influenced their choice of job or career.
Conclusion Four out of every 10 adolescents with knee pain still experienced frequent and intense knee pain 5 years later, severe enough to impact health, health behaviours and career choices.
Trail registration number NCT02873143.
- youth
- health behaviours
- growing pains;
- care-seeking
- musculoskeletal
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first preregistered study to follow a population-based cohort of adolescents with knee pain into early adulthood.
This study used validated outcomes to investigate the impact of adolescent knee pain on health, care-seeking behaviour and career choices.
Outcomes were informed by adolescents with knee pain and their parents and highlights that adolescent knee pain has long-term impacts on domains important to these young people and their parents.
In this cohort, we do not know which structural findings, if any, are responsible for the adolescents’ pain, or if they are the same at follow-up as they were at baseline.
Due to the recurrent intermittent nature of many types of knee pain, our choice of quantifying persistent knee pain (knee pain in the previous week) may actually underestimate the number who continue to be troubled by knee pain.
Introduction
Knee pain is common in adolescents, affecting one out of every three, and is associated with low quality of life and reduced physical activity levels.1–3 A high proportion of adolescents with knee pain consult their general practitioner (GP),4 making knee complaints the fourth most common of all musculoskeletal-related consultations for children and adolescents.5 Overall, knee pain accounts for the second highest number of GP consultations, with approximately 10% of the caseload relating to youth musculoskeletal complaints.5 Perhaps due to its commonality, knee pain is often considered a natural part of adolescence, and thought to be self-limiting with no long-term impact. However, this assumption has been tested in two population-based studies,6 7 which show that as many as one in every two adolescents will still report knee pain 1 year later. Due to the short-term follow-up in these studies, little is known about the trajectory of knee pain in the transition from adolescence to adulthood.
Chronic knee pain during adolescence can be disabling, and result in reduced sports participation and physical activity.8 Adolescents who cease sports participation during youth may be at a higher risk of cardiometabolic disorders and inactive lifestyles during adulthood.9 Reducing or ceasing leisure-time physical activity because of knee pain may initiate a cascade effect, in which reduced physical inactivity leads to poor cardiorespiratory fitness, increased adiposity and poor health outcomes.10 This highlights the importance of examining the long-term prognosis and consequences of adolescent knee pain.
In 2011, we started the Adolescent Pain in Aalborg 2011 (APA2011) cohort, a population-based cohort consisting of 2200 adolescents between 15 and 19 years of age at the time of recruitment. The prevalence of self-reported knee pain was 33%,1 and in the 2-year follow-up of this cohort, more than 50% of these adolescents still reported having knee pain.8 Long-standing knee pain had a negative effect on the adolescents’ quality of life and sports participation.8 To build on these findings, it would be valuable to understand if knee pain continues to persist after adolescence, and understand its’ potential impact during the transition to early adulthood. This is a critical developmental period, in which youth are often required to make choices regarding their career and further education.
The purpose of this study was to investigate the prognosis of adolescent knee pain, and prospectively evaluate its impact on health, care-seeking and career choices 5 years later and compare with a control group without knee pain at study inception.
Methods
This study was designed as a population-based prospective cohort study. The reporting of the study follows the Strengthening the Reporting of Observational Studies in Epidemiology statement.11 The 5-year follow-up was pre-registered before participants were invited to participate.
Recruitment
In September 2011, all students at four upper secondary schools in the municipality of Aalborg, Denmark, were invited to answer an online questionnaire and to be part of the APA2011 cohort.1 The online questionnaire contained demographic questions on age, sex, height, weight and the name of the school. They were then presented with a mannequin with a frontal and posterior view of the human body. All of the body regions were written next to the mannequin. The adolescents had the option of clicking on the name of the region or pressing the specific body region where they experienced pain; the colour of the selected region then changed. After that they were asked separately about the frequency of pain in the selected regions: rarely, monthly, weekly, more than once per week or almost daily. Pain frequency was chosen as a simple measure of pain severity, as higher frequency has been associated with higher pain intensity and poor prognosis.7 After the pain mannequin and pain frequency questions, the adolescents were asked if they participated in leisure-time sport (sports activity besides the mandatory physical education classes during school hours) and, if so, how many times they participated each week. The last page of the questionnaire contained the EuroQoL 5 Dimensions (EQ-5D 3L), which measures health-related quality of life.12
From 2846 potential responders, 2200 adolescents responded to the questionnaire, corresponding to a response rate of 77%. A total of 670 adolescents reported knee pain at least monthly or more frequently; however, 60 of them did not report their telephone numbers in the questionnaire, leaving 610 potential responders for the follow-up. A total of 504 adolescents indicating knee pain at least monthly were successfully contacted, and subsequently included in the follow-up (a response rate of 83% of those who reported their telephone numbers). The sample size at baseline determined the sample-size for this 5-year follow-up. See flow chart in figure 1.

STROBE flow chart. STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
Follow-up
At the 5-year follow-up in September 2016, all 504 adolescents were contacted by telephone, SMS or email and asked to answer an online questionnaire (questionnaire can be seen in online supplementary appendix 1). If they agreed to participate, an email with a link to the questionnaire was sent to them. To create an incentive to reply, we offered the participants a cinema ticket after they responded to the questionnaire.
Supplemental material
This 5-year follow-up examined the overall prognosis and impact of adolescent knee pain by comparing those who reported knee pain in the past week after 5 years, versus those who did not. To ensure a meaningful comparison and interpretation of the different outcomes, and to control for normal developments during adolescence (eg, changes in sports participation after completing school), we contacted 252 randomly selected adolescents from the same cohort who did not report knee pain at baseline in 2011. These 252 were also part of the 2-year follow-up in 2013.8
Patient and public involvement
Information from previous semi-structured interviews with adolescents and their parents were used to inform choice of outcomes, which were structured into the domains of pain, health, care-seeking and treatments, and career choices. These interviews were done to identify the most important questions surrounding prognosis as perceived by adolescents and parents. The questionnaire was pilot tested for comprehensibility by 10 young adults of similar age, who were not part of the cohort. Based on their feedback a series of minor changes were made to ensure comprehension. Patients were not involved in the recruitment of other patients. Study results will be communicated to participating patients through a short screencast (video) sent by email that will explain the main findings of the study.
Outcomes assessment
Pain
At the 5-year follow-up in September 2016, participants were asked the same primary question on knee pain during the past week as they were asked during the 2-year follow-up. In addition, they were asked about knee pain during the past month to align with the eligibility criteria used at baseline to define the cohort. This was followed up with questions regarding frequency and intensity of knee pain (worst pain in the previous week measured on a Numeric Rating Scale). They were also asked to complete the patient-reported outcome Knee injury and Osteoarthritis Outcome Score (KOOS), where the Pain and Symptoms subscales were included as part of the pain outcomes.13 Finally, they were asked if and when their knee pain resolved, and if they experienced pain in other body regions.
Health
Participants were asked if they participated in leisure-time sport and if yes, how many times per week, and if their knee pain had an effect on their sports participation. Physical activity level was measured with the International Physical Activity Questionnaire, which has been validated in several European countries.14 Individuals who reported 150 min or more of moderate physical activity (including walking), at least 75 min of vigorous activity per week, or an equivalent combination of moderate and vigorous activity (ie, any combination accumulating 600 MET minutes/week) were classified as meeting WHO recommended levels of physical activity. The Quality of Life subscale from the KOOS captured knee-related quality of life, while the EQ-5D 3L was used to measure health-related quality of life. The impact of knee pain on knee function, sport and recreational activities was measured with the KOOS Activities of Daily Living and Sport/recreation subscales. Finally, participants were asked about sleep problems and if their knee pain had influenced mood or their choice of activity level. Weight and height were collected through self-report.
Care-seeking
Participants were asked whether they had sought treatment for their knee pain in the previous 12 months, which health professional they had contacted, and which treatments they had been prescribed. They were also asked whether they used pain medication, which types and how frequently.
Career choices
To measure the impact of knee pain on important choices during the transition to early adulthood, we asked the participants if their knee pain influenced their choice of education or professional career.
Statistical analyses
The statistical analysis consisted of descriptive statistics, with results expressed as mean and 95% CIs or median and IQR, depending on the distribution of data. For the primary outcome, we reported it using a 2×2 table and reporting the percentages with knee pain at the 5-year follow-up. For comparisons of other outcomes, we considered non-overlapping 95% CIs to indicate that a real difference was present. These were compared between the three following groups.
Those with knee pain at baseline and follow-up; categorised if they had knee pain at baseline and reported knee pain in the previous week at follow-up.
Recovered; those with knee pain at baseline but reported ‘no’ to pain in the previous week at follow-up.
Control group; those without knee pain at baseline.
The dropout analysis compared baseline data from adolescents who completed the 5-year follow-up and adolescents with no available follow-up data. Stata V.11 was used for all statistical analyses.
Results
At the 5-year follow-up, 358 (71.0%) adolescents with knee pain and 182 (72.2%) from the control group answered the questionnaire; 73% of the entire sample were women. Mean age at follow-up was 22.4 years (±1.1) and mean body mass index was 23.6 kg/m2 (±4.2). Baseline information of the cohort is presented in table 1. The dropout analysis showed that there were no significant, or relevant, difference in any of the baseline characteristics between those who completed the 5-year follow-up and those that did not.
Baseline demographics, physical activity, quality of life and pain
Pain
Overall, 40.5% (95% CI: 35.4% to 45.6%) of the adolescents with knee pain at baseline also reported knee pain in the past week 5 years later (knee pain at baseline and follow-up group) (table 2). Only 13.2% (95% CI: 8.2 to 18.1) of the with no knee pain at baseline (control group) reported pain at 5-year follow-up. The subsequent results will be stratified into the following three groups, with the following terminology used throughout:
Those with knee pain at baseline and follow-up; categorised if they had knee pain at baseline and reported knee pain in the previous week at follow-up.
Recovered; those with knee pain at baseline but ‘no’ to pain in the previous week at follow-up.
Control group; those without knee pain at baseline.
Proportion having knee pain at baseline and follow-up
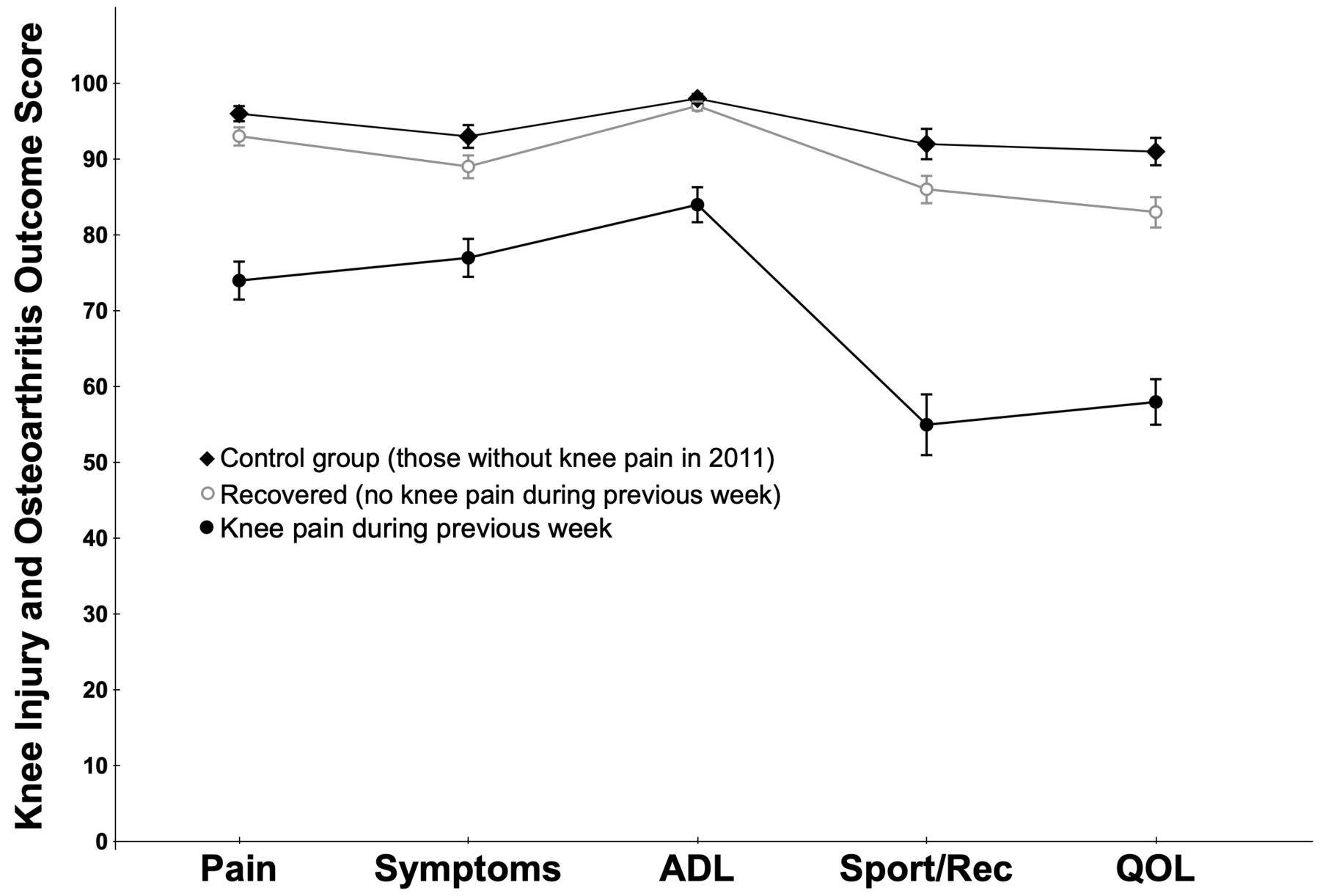
The young adults reporting knee pain at baseline and follow-up were characterised by frequent and intense knee pain (table 3). The group who had knee pain at baseline and follow-up up also had significantly worse KOOS Pain (20 points (95% CI: 17 to 22)) and KOOS Symptoms (13 points (95% CI: 10 to 15)) compared with those who recovered from knee pain at follow-up (figure 2).
{kind=link}
{kind=link}
Mean (95% CI) KOOS subscale scores for the young adults who responded ‘yes’ to having knee pain in the previous week at follow-up (n=145) compared with the recovered group who responded ‘no’ to having knee pain during the previous week (n=213) compared with the control group without knee pain in 2011. KOOS is scored 0–100, worst to best. ADL, activities of daily living; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, quality of life.
Outcome data presented as mean (95% CI) for the group with knee pain during the past week, without knee pain during the past week and the control group at 5-year follow-up
Health
Those with knee pain at baseline and follow-up participated less frequently in sport, and 60% had reduced their sports participation as a result of their knee pain (table 3) compared with the recovered and control groups. The group who experienced pain at baseline and follow-up had worse knee function, knee-related quality of life, general health-related quality of life and worse sleep compared with the recovered group and the control group (table 3). Body mass index was similar between the group with knee pain at baseline follow-up (23.7 (95% CI: 23.1 to 24.3)) and the recovered group (23.5 (95% CI: 22.9 to 24.2)). Of the young adults, 32.9% (95% CI: 25.6 to 41.0) with knee pain at baseline and at follow-up reported their knee pain impacted on their mood, compared with 6.5% (95% CI: 3.8 to 10.8) of the recovered group.
Care-seeking
Among the young adults with knee pain at baseline and follow-up, one in every three had sought medical attention for knee pain during the previous 12 months (table 3) and the most commonly prescribed treatments were exercise and painkillers. Among those who had knee pain at baseline and follow-up, 31% used painkillers with the most frequent types being NSAIDs, or paracetamol or a combination of the two.
Career choices
Of the participants, 15% (95% CI 12% to 20%) reported that their knee pain had an impact on their choice of job and/or career.
Discussion
Contrary to common beliefs, knee pain during adolescence is not associated with a favourable prognosis and, for many, it continues to persist into early adulthood. Disturbingly, our data reveal that four out of 10 adolescents with knee pain in late adolescence, still experienced pain five years later, severe enough to negatively impact their quality of life, sports participation, and in one out of seven, affect their choice of job or education. One-third of adolescents with knee pain at follow-up reported regular use of painkillers. Despite meeting the WHO guidelines on the recommended amount of physical activity (based on the International Physical Activity Questionnaire (IPAQ)), most had problems with running (86%) and walking on stairs (78%). Considering their young age, these results with basic functional tasks are concerning, and highlight the impact of knee pain on their young lives.
Strengths and limitations
One of the main strengths of this study lies in the design; the study was pre-registered, and based on a population-based cohort, including a random sample of controls to allow for comparison. The population based design and high response rate mean that our results are generalizsable to the general population of adolescents, indicating quite a high proportion of all adolescents will continue to suffer from knee pain into adulthood. Another strength is that the choice of outcomes was informed by adolescents with knee pain and their parents, highlighting that adolescent knee pain has long-term impacts on domains important to these young people. In this cohort, we do not know which structural findings, if any, are responsible for the adolescents’ pain, or if they are the same at follow upfollow-up as they were at baseline. Due to the recurrent intermittent nature of many types of knee pain, our choice of quantifying knee pain at follow-up (knee pain in the past week) may actually underestimate the number who continue to be troubled by knee pain, and may not truly reflect the participants who have ‘recovered’. This underestimation is documented by 42% of those responding ‘no’ to knee pain during the past week, reported experiencing knee pain during the past month. The use of IPAQ may overestimate physical activity levels, but this bias is present across all adolescents (both those with or without knee pain at follow-up).15
Comparison with previous studies
Adolescent knee pain is an understudied area, and, to date, its prognosis has only been evaluated in two population-based studies.6 7 While these studies corroborate our findings, indicating that as many as one in every two adolescents continues to suffer from knee pain, they are limited by their shorter term follow-up and lack of investigation of the long-term impact on the domains important to the adolescents. Looking broadly at prognosis of general musculoskeletal pain in adolescents, the most recent systematic review identified nine prospective cohorts. In general, studies found that between 15% and 60% of adolescents still experienced pain years after they developed musculoskeletal pain.16 The majority of these studies followed adolescents for no more than 3 years, with none investigating the 5-year prognosis for knee pain. Combined with the published literature, the current study underlines the high persistence of adolescent knee pain and other types of musculoskeletal pain. Our population-based cohort fills a knowledge gap by tracking the trajectory of adolescent knee pain into early adulthood. Combining this with other important parameters of pain, health and care-seeking, this study provides a more comprehensive picture of the long-standing and far-reaching impact of adolescent knee pain than has been done before.
Possible explanations and implications
One in every three young adults with knee pain at the 5-year follow-up reported that they had sought medical treatment for their knee pain in the previous 12 months. The most commonly prescribed treatments were exercise and painkillers. This is reflected in the high number (one in every three) who reported using painkillers. Considering painkillers are neither advised or effective for managing long-term musculoskeletal pain, the prevalence of this medication use, as well as other treatment types, require further attention.17
While a large proportion of the adolescents with knee pain at follow-up reported having reduced their sports participation because of pain (60%), they still appeared to be physically active, as quantified by the IPAQ. This may be explained by the fact that many of them had modified their activity (42.9% reported changing activates as a result of their knee pain) to participate in activities which did not aggravate their pain. This is reflected in the relatively high proportion reporting trouble with running, and not playing sports. The large impact knee pain had on knee function may explain how knee pain may influence their choice of job and education. Blue collar work, such as that carried out by carpenters, electricians and blacksmiths, and similar vocations, involve manual labour which requires adequate knee function. This highlights the far-reaching effects of long-standing adolescent knee pain. When presented with a young adolescent suffering from knee pain, clinicians should not assume that adolescent knee pain will resolve itself.
Unanswered questions
A high proportion of young adults with knee pain at follow-up report concurrent sleep problems. This warrants further investigation, as poor sleep negatively impacts pain the following day,18 and is associated with higher pain-related disability19 and psychological factors.20 21 The role of sleep as a prognostic factor or potential future target for treatment in young adults with long-standing knee pain needs to be examined.
While this study highlights the unique problem of adolescent knee pain, it is still unclear why so many (nearly 50%) still suffer from persistent pain into adulthood. For some, this may be sustained due to a failure to reduce or modify their pain-causing activities. However, there were at least some, who had decreased and/or switched to less aggravating activities, so other factors must have been responsible for the persistence of their pain. Recent data suggest that adolescent musculoskeletal pain is related to medical, and social welfare benefits later in life, as well as utilisation of mental healthcare services in young adulthood.22 23 Further research is needed to fully quantify the societal burden of adolescent knee pain, and evaluate whether pain in youth may be an entry point for other chronic pain conditions (eg, osteoarthritis), misuse of painkillers including opioids or other chronic health conditions later in life.
Conclusion
This is the first prospective population-based study examining the 5-year prognosis of knee pain from adolescence into early adulthood. Four in every 10 adolescents with knee pain still experienced frequent and intense pain 5 years later, severe enough to impact physical health, health behaviours and life choices.
References
Footnotes
Contributors MSR, SH, CS, MBJ, JLO and ER all participated in the conception and design of the study. MSR, SH and CS were responsible for the collection of data. MSR and SH conducted the analyses and all authors took part in the interpretation of the results. All authors critically revised the manuscript for important intellectual content and approved the final version of the manuscript. MSR is the guarantor.
Funding The project was funded by the Danish Rheumatism Association. The funder was not involved in the actual study or the interpretation, drafting, approval of the manuscript.
Competing interests None declared.
Ethics approval The ethics committee did not require an individually signed consent form, but did require that the schools informed the parents about the study and that participation in the study was voluntary. This study was approved by the local ethics committee of the North Denmark Region (N-20110020).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available upon reasonable request in anonymised form by contacting the lead author.
Patient consent for publication Not required.