Article Text

Abstract
Objectives Breast feeding is associated with health benefits for both mother and child, but many studies focusing on neurodevelopment have lacked information on important confounders and few randomised trials exist. Our objective was to examine the influence of breast feeding on child IQ at 5 years of age while taking maternal IQ and other relevant factors into account.
Design Prospective observational study.
Setting Population-based birth cohort in Denmark.
Participants We used data from The Lifestyle During Pregnancy Study 1782 mother–child pairs sampled from the Danish National Birth Cohort (n=101 042).
Outcome measures Child IQ was assessed at age 5 years by the Wechsler Primary and Preschool Scales of Intelligence-Revised. On the same occasion maternal intelligence was assessed by Wechsler Adult Intelligence Scale and Raven’s Standard Progressive Matrices. Exposure data on duration of breast feeding (n=1385) were extracted from telephone interviews conducted when the child was 6 and 18 months, and analyses were weighted by relevant sampling fractions.
Results In multivariable linear regression analyses adjusted for potential confounders breast feeding was associated with child IQ at 5 years (categorical χ2 test for overall association p=0.03). Compared with children who were breast fed ≤1 month, children breast fed for 2–3, 4–6, 7–9 and 10 or more months had 3.06 (95% CI 0.39 to 5.72), 2.03 (95% CI −0.38 to 4.44), 3.53 (95% CI 1.18 to 5.87) and 3.28 (95% CI 0.88 to 5.67) points higher IQ after adjustment for core confounders, respectively. There was no dose–response relation and further analyses indicated that the main difference in IQ was between breast feeding ≤1 month versus >1 month.
Conclusions Breastfeeding duration of 1 month or shorter compared with longer periods was associated with approximately three points lower IQ, but there was no evidence of a dose–response relation in this prospective birth cohort, where we were able to adjust for some of the most critical confounders, including maternal intelligence.
- cohort study
- observational study
- breast feeding
- intelligence
- wechsler scales
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Study based on a large population-based pregnancy cohort with prospective data assessments.
This study of the association between breast feeding and child IQ took into account maternal intelligence and home environment, two critical confounders.
Very few women did not breast feed (6/1385, 0.4%), so it was not possible to investigate this group separately.
Postnatal factors may have influenced child IQ that we have not been able to take into consideration.
Introduction
There is firm evidence for the beneficial effects of breast feeding on a wide range of maternal and child outcomes1 2 and to ensure healthy growth and development the WHO recommends that all children are exclusively breast fed for the first 6 months of life, followed by partial breast feeding.3
Since the very early observations by Hoefer and Hardy in 1929 of a positive association for breast feeding with cognitive performance at age 7–13 years,4 a large body of evidence has provided results in this field. Due to difficulties and ethical concerns intrinsic in designing an intervention targeting breastfeeding duration, few randomised trials exist.5–7 These have shown beneficial effects of breast feeding in relation with child neurodevelopmental outcomes, and one of these indicated that exclusive breast feeding may not confer superior effects compared with breast feeding and complementary foods introduced at 4 months of age.7 Several observational studies have shown positive associations for duration of breast feeding with cognitive developmental benefits in childhood8–16 and in adult life.17–20 Differences in nutrient compositions between human milk and formula have been suggested as one of several potential mechanisms underlying a beneficial effect of breast feeding on cognitive development.18 In some studies, crude positive associations between breast feeding and cognitive endpoints were attenuated on adjustment for potential confounders, including socioeconomic background21–25 which has made authors conclude that breast feeding may be a proxy for home environment or parental practices rather than a causal factor in itself.21–27 However, many studies have been relatively small (n<500), have had limited details on breast feeding or have not been able to take into account some of the critical confounders including maternal intelligence.9 12 26 A systematic review and meta-analysis in 2013 concluded that breast feeding is associated with increased performance in intelligence tests in childhood and adolescence of 3.5 points on average, and that maternal IQ, despite being an important confounder, can account only for part of this association.3 While the practical implications of such moderate differences in intelligence tests can be questioned, a recent study from Brazil20 indicated that a cognitive advantage by breast feeding was maintained until adulthood mediating effects on life outcomes including educational attainment and income even in a setting without strong social patterning of breast feeding.20 28
The aim of the present study was to assess, in an observational setting, the influence of breast feeding on child IQ at 5 years of age while taking maternal IQ and home environment into account in the Lifestyle During Pregnancy Study (LDPS).
Subjects and methods
The aim of the LDPS is to examine the relation between maternal lifestyle during pregnancy and offspring neurodevelopment by the age of 5 years.29 The study is a subsample of the large prospective Danish National Birth Cohort (DNBC).30 The DNBC recruited >100 000 pregnant women between 1996 and 2002, and data collection instruments included two pregnancy telephone interviews (in gestational weeks 12 and 30 approximately), two telephone interviews postpartum (at 6 and 18 months postpartum), as well as a detailed food frequency questionnaire which was mailed to the women in gestational week 25 and covered the dietary intake in the previous month.31 Information on birth outcome was obtained from the Medical Birth Registry.
The LPDS consists of 3478 mother–child dyads selected from the DNBC with oversampling of pregnant women with moderate weekly alcohol intake, alcohol binge drinkers and women with high versus low fish intake, iron intake and duration of breast feeding, respectively.29 A detailed description of the LDPS, including the sampling frame, has been published elsewhere.29 32 In brief, 3478 mother–child pairs from the DNBC were invited to participate in a follow-up around the time when the children turned 5 years. Of the selected dyads, 1782 mothers and children (51%) took part in a comprehensive 3-hour assessment of neurodevelopment focusing on global cognition, specific cognitive functions and behaviour of the child, and additionally mothers completed tests of adult intelligence (IQ).29
Exclusion criteria for the follow-up in LDPS were multiple pregnancies, inability to speak Danish, impaired hearing or vision of the child likely to compromise the ability to perform the cognitive tests, and congenital disorders likely to cause mental retardation, including trisomy 21.29 All test procedures were standardised in detail and carried out by 10 trained psychologists. The examinations took place in the four largest cities of Denmark: Copenhagen, Aarhus, Odense and Ålborg.29
Exposure variables
At both telephone interviews postpartum, when the child was 6 and 18 months, respectively, mothers answered questions about breast feeding. At the 6 months’ interview they reported whether they had never breast fed, were currently breast feeding or had stopped breast feeding. Those who were no longer breast feeding reported the child’s age when daily breast feeding stopped. At 18 months’ postpartum, mothers were asked whether they had breast fed their child beyond 6 months, and if so, whether they were still breast feeding; if not, they reported the child’s age at discontinuation of breast feeding. Combining the answers from these two data collection instruments we constructed a measure of duration of any breast feeding, not distinguishing between exclusive and supplemented breast feeding.
Outcome variables
We used child IQ assessed at the follow-up examination at age five with the Wechsler Primary and Preschool Scales of Intelligence-Revised (WPPSI-R).33 The WPPSI-R is one of the most widely used standardised tests of intelligence for children of 2–7 years of age. In its full form the test battery for WPPSI-R comprises five verbal subtests and five performance (non-verbal) subtests from which verbal IQ (VIQ), performance IQ (PIQ) and full scale IQs (FSIQs) are derived. The length of the examination was accommodated to match the age of the study participants (5 years), and therefore a short form of the WPPSI-R was used, which included three verbal (Arithmetic, Information and Vocabulary) and three performance subtests (Block Design, Geometric Design and Object Assembly). Standard procedures were used to prorate IQs from the shortened forms of the tests,34 and since no Danish WPPSI-R norms were available at the time of the study Swedish norms were used to derive scaled scores and IQs.35 The use of Swedish norms might cause a slight shift in the IQ distribution, and the theoretical mean of 100 (SD 15) cannot necessarily be expected in this sample. However, as the analyses conducted in this study are internal comparisons across exposure, a systematic shift in the IQ distribution should not affect our results.
Mother–child pairs available for analysis
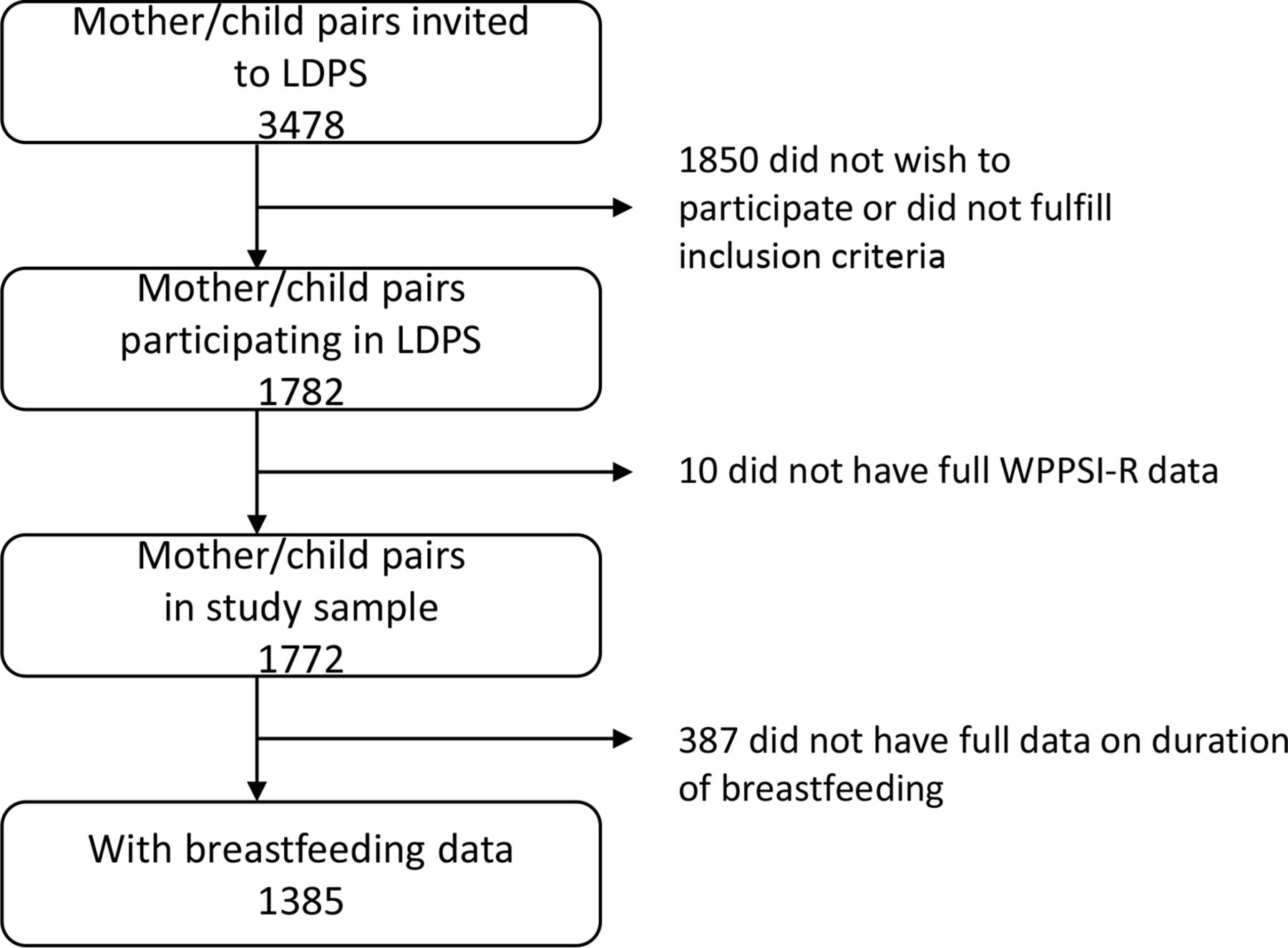
Out of the total number of participants in the LDPS (n=1782), the study sample for these analyses consisted of those 1772 (99.4%) mother–child dyads in the LDPS with full outcome data on the WPPSI-R. Full information on breast feeding was available for 1385 (78.2%) of these as lined out in figure 1.

{kind=link}
Overview of the study sample from the LDPS. LDPS, Lifestyle During Pregnancy Study; WPPSI-R, Wechsler Primary and Preschool Scales of Intelligence-Revised.
Covariates
We used information from the prenatal telephone interviews, a questionnaire at the 5-year follow-up examination, and from the Medical Birth Registry and Central Person Registry to define potential confounders that we included in our analyses as covariates. Maternal IQ was assessed at the follow-up examination by two verbal subtests (information and vocabulary) from the Wechsler Adult Intelligence Scale36 and non-VIQ by the Raven’s Standard Progressive Matrices.37 Raw scores of each of the two subtests (information and vocabulary) were standardised based on the results from the full sample. Subsequently scores from each of the two subtests were weighted equally into one combined score, and this combined score was then restandardised to a scale with a mean of 100 and SD of 15.
We defined the covariates as follows: parity (0, 1, ≥2 previous births); prenatal maternal smoking (yes, no); maternal prepregnancy body mass index (BMI) (weight (kg)/height (m)2); parental education (average educational length in years for the parents or of mother if that of the father was unavailable); marital status (single during pregnancy or at 5-year follow-up, married/cohabitating at both); postnatal parental smoking (yes if mother or father smoked in the home, no if otherwise); maternal average alcohol intake in pregnancy (0, 1–4, 5–8, ≥9 drinks/week); an index of the child’s health status (dichotomised as normal or suboptimal in the presence of any illness, diseases, handicaps and/or medication with potential influence on test performance); an index of the quality of postnatal home environment (dichotomised as normal or suboptimal in the presence of two or more of the following seven conditions: not living with a biological parent, changes in caregiver, day care for more than 8 hours/day before age 3, 14+ days of separation from the parents, breakfast irregularity, maternal depression and parental alcohol use above the maximum recommended level by the Danish Health Authority at the time of follow-up of 14 (women) or 21 (men) drinks/week); maternal age at pregnancy (in years); maternal IQ (score), sex of child (girl, boy) and age of child at the follow-up examination. Gestational age was calculated from the last menstrual period provided by the mother at study recruitment (gestation week 6–10) or from the expected date of delivery provided by the woman during the second telephone interview (gestation week 30) which was most often based on ultrasound results.38 The date of birth was extracted from the Central Person Registry, and the midwife who attended the child’s birth recorded birth weight which we extracted from the Medical Birth Registry and calculated sex-specific weight z-score at birth on the basis of published reference data.39 40
The 10 trained psychologists who carried out the testing of the study participants were blinded to the child’s exposure status, and we took tester differences into account by the inclusion of a categorical variable with 10 levels in the statistical analyses. In a sensitivity analysis tester was taken into consideration in the analysis by a random effect.
Statistical analyses
We used the median (IQR) to describe skewed variables; mean (SD) for normally distributed variables; and n/percentage for categorical variables. Throughout, when analysing associations with continuous measures p values from F tests (type II) are presented, for associations with categorical measures p values from χ2 test (type III) are presented.
The exposure variable, breastfeeding duration, was examined in relation to child IQ both as a continuous variable (breastfeeding duration in months), and categorised as any breast feeding ≤1 month, 2–3 months, 4–6 months, 7–9 months or ≥10 months. When analysing breast feeding as a continuous measure, we present p values from F test of trend across months of breast feeding, when looking at breast feeding as a categorical variable we present p values from overall F test of any difference in IQ score across groups of breastfeeding duration.
Furthermore, for supplementary analysis we dichotomised the exposure variable in order to examine the difference in FSIQ according to duration of any breast feeding ≤1 month versus >1 month, and ≤6 months versus >6 months.
We present differences in WPPSI-R FSIQ scores across exposure levels by using multivariable linear regression models to obtain β estimates and corresponding 95% CIs. In our multivariable analyses we adjusted for potential confounders in two steps: maternal IQ, parental education, maternal smoking during pregnancy, age of child at the follow-up examination and tester were considered core confounders, and we considered this our main analysis; in a more extensively adjusted model we furthermore included the following potential confounders: maternal age, maternal marital status, parity, sex of child, maternal prepregnancy BMI, postnatal parental smoking, health index, home environment and maternal average alcohol intake during pregnancy. Supplementary to this, a non-linear relation between duration of breast feeding (continuous) and child FSIQ was tested comparing a linear model to a model using restricted cubic splines with three knots placed at the 25th, 50th and 75th percentiles.41 To test for deviations from linearity, we used a likelihood ratio test (P curvature, F test) to compare the linear model with a model fit that was based on restricted cubic splines.
Due to the oversampling of study participants according to certain behavioural exposures, as described above (moderate alcohol use, binge drinking, fish, iron intake and duration of breast feeding) all analyses were weighted by sampling fractions to account for the complex stratified sampling design.32
For the 1385 mother–child pairs with data on exposures and outcome, data on child’s age at testing and testing psychologist was complete, whereas information on other covariates was missing for approximately 8% of participants (ranging from 7.9% for maternal smoking during pregnancy to 9.5% for maternal prepregnancy BMI). We substituted missing covariate values by multiple imputation using the standard procedure PROC MI in SAS, which utilises all the information available and imputes five different datasets based on which we calculated five different sets of effect and variance estimates, and subsequently used the procedure PROC MIANALYZE to compute a combined estimate and SE for each regression coefficient in our analyses. Results from alternative analytic strategies using complete case and substitution of missing values with mean/mode imputation did not alter our conclusions.
All analyses were carried out using SAS statistical software V.9.4 (SAS Institute), and all tests were two-sided with statistical significance set to p<0.05.
Supplementary analyses
To avoid overadjustment gestational age and birth weight z-score were not included in our main models. As supplementary analysis we furthermore excluded those mother–child pairs who never initiated breast feeding (n=6). We stratified by child sex, in order to examine potential sex specific effects. We also conducted separate analyses for PIQ and VIQ, respectively. Finally, we dichotomised the three IQ outcomes and conducted analyses by logistic regression models presenting χ2 tests evaluating statistical significance for overall association. Dichotomisation was made using the sample mean minus one SD for the relevant IQ score as described by Falgreen Eriksen42 (FSIQ dichotomised at 92.5, PIQ at 88.7, VIQ at 94.0) as a cut-off score for subnormal test performance, which implied categorising 209 (15.1%) as subnormal for FSIQ, 232 (16.8%) as subnormal for PIQ and 229 (16.5%) as subnormal for VIQ.
Patient and public involvement
Patients were not involved in this study. Results are disseminated to study participants through regular news letters, the website of the DNBC and DNBC on social media.
Results
The children in the LDPS were 60–64 months of age at follow-up (mean 5.2 years, range 5.0–5.3 years), and 53% of the children were boys.32 The mean (SD) FSIQ in the study sample was 105.3 (12.8). The study sample for the present analyses, who had information on breast feeding (n=1385) did not differ from the full LDPS sample with respect to maternal age (mean (SD) was 30.9 (4.4) and 30.9 (4.3) respectively), education (median (IQR) 13.0 (3.0) in both samples), smoking during pregnancy (32.4% and 31.5%, respectively) and cohabitation status in pregnancy (2.7% and 2.9% single, respectively).
Women who breast fed for less than 1 month compared with 7–9 and more than 10 months were generally younger, they were more likely to be nulliparous (had not previously given birth), have higher BMI, to have been smokers during pregnancy or to have their children be exposed to tobacco smoke postnatally, and have lower IQ (table 1). Duration of parental education and birth weight z-score was highest for children breast fed for 10 months or longer, and lowest for those who were breast fed for 2–3 months.
Study participants in the Lifestyle During Pregnancy Study distributed by maternal and child characteristics and by breastfeeding duration (n=1385)
Child IQ at the 5-year examination was directly associated with maternal IQ (Spearman r=0.29, p<0.0001), parental education, birth weight z-score and gestational age, whereas associations were inverse for parity, prepregnancy BMI, smoking during pregnancy and postnatal smoke exposure (data not shown). Mean IQ was slightly higher for girls compared with boys (see online supplementary table 1).
Supplemental material
Duration of breast feeding was associated with child IQ at 5 years, even after adjustment for core confounders which included maternal IQ (p from overall categorical test 0.03) (table 2). Compared with children who were breast fed 1 month or less, children who were breast fed for 2–3, 4–6, 7–9 and 10 or more months had 3.06 (95% CI 0.39 to 5.72), 2.03 (95% CI −0.38 to 4.44), 3.53 (95% CI 1.18 to 5.87) and 3.28 (95% CI 0.88 to 5.67) points higher IQ, respectively. These results remained very similar after more extensive adjustment of potential confounders. When analysing duration of breast feeding as a continuous variable, the association was statistically significant only in the unadjusted analyses (unadjusted β (95% CI): 0.33 (0.19 to 0.47), adjusted β: 0.04 (−0.10 to 0.18)). Furthermore, the estimates for 2–3, 4–6, 7–9, ≥10 months breastfeeding groups were not statistically different from each other (F-test categorical test for overall association omitting mother–child pairs with breast feeding ≤1 month, p=0.21), indicating that there was no dose–response, but that the difference in FSIQ lies between those breast fed ≤1 month versus >1 month. Dichotomising the breastfeeding variable by duration ≤1 month versus >1 month resulted in a 2.98 (95% CI 0.86 to 5.11) point lower FSIQ in adjusted analysis for children who were breast fed ≤1 month versus >1 month, whereas a dichotomisation of breast feeding by duration ≤6 months versus >6 months resulted in a difference of 1.61 (95% CI 0.29 to 2.93) points. We subsequently tested for a non-linear association using restricted cubic splines which provided significantly better fit compared with the linear model (p=0.02), and the model with splines was significantly different from the null (p for non-linearity=0.03).
Full scale IQ* among 1385 children from the Lifestyle During Pregnancy Study in association with breastfeeding duration
Adjustment for gestational age and z-score for birth weight in supplementary analyses did not alter our study results, and neither did using a random effect for testing psychologist. Exclusion of mother–child pairs that had never initiated breast feeding (6/1385, 0.4%) did not change our results for the association between breast feeding and child IQ, but interestingly the mean maternal IQ in the lowest breastfeeding group decreased (from 100.4 to 94.0). When we analysed subscales of IQ, associations were strongest for PIQ (table 3); for VIQ effect estimates went in the same direction as for FSIQ, but were attenuated and not consistently statistically significant across the different adjustment models.
Verbal and Performance scale IQ* among 1385 children from the Lifestyle During Pregnancy Study in association with breastfeeding duration
When we stratified for child sex, overall associations were the same and remained statistically significant for both boys and girls, even if confidence intervals widened considerably and effect estimates for the specific breastfeeding groups fluctuated between boys and girls (see online supplementary table 1).
Finally, analyses using dichotomised IQ measures indicated associations in the same direction as the main analyses, but CIs were wide, and associations were generally not statistically significant.
Discussion
In this relatively large study population which was sampled from the DNBC we investigated associations for duration of breast feeding with child IQ at age 5 years assessed with the WPPSI-R by a team of trained psychologists. We saw an approximate 3-point difference in IQ between those who were breast fed for 1 month or less compared with those who were breast fed longer.
Our results are in support of the previous studies that have shown beneficial associations for breast feeding with cognitive measures in children.9–12 43 44 It furthermore adds to the current body of literature, since we were able to take maternal IQ into account, had detailed information on breast feeding, clinical assessment of child IQ by a validated tool, as well as a relatively large sample size. Also, we find it relevant that our results are obtained in a population where less than 1% are never breast fed (0.4%), and more than 60% are still breast fed after 6 months, which seems to be among the highest breastfeeding rates in the world in a high-income setting.45 The observed difference in IQ score in our analyses corresponds well with the results of a recent meta-analysis which reported a pooled effect of 3.5 IQ points associated with breast feeding, and a slightly smaller difference of 2.2 IQ points in studies that were able to adjust for maternal intelligence.3 According to Jacobson et al the contribution of maternal intelligence to the child’s cognitive ability is both genetic and through a more stimulating rearing environment.46 Furthermore, studies that fail to include maternal intelligence when attempting to show that the link between breast feeding and cognitive outcome is not attributable to social factors underestimate a critically important factor.22 46 Our results thus point to some effect of breast feeding on child IQ over and above that of parent practices and heredity.
We found no clear dose response relation of breastfeeding duration with child cognitive development in our data; rather, our results point to a difference in IQ of approximately three points between children who are breast fed for a short period of 1 month or less compared with those who are breast fed longer. This is in line with the results of a study that used propensity score matching techniques16 as well as a longitudinal US-based study15; but stands somewhat in contrast with a meta-analysis from 19998 and a more recent systematic literature review1 which concluded that cognitive developmental benefits increased with duration of breast feeding. In our data such a relation was present in the unadjusted analysis only, and we can therefore speculate that effect patterns and sizes may differ between studies depending on other variables that influence IQ, or that previous studies have not investigated such threshold effects of breast feeding.
In our study sample, we categorised the shortest duration as ≤1 month, since very few women reported breastfeeding duration shorter than this, reflecting that by far the majority of mothers in Denmark choose to breast feed their children. Adding to the difficulty of obtaining an exposure group with shorter duration of breast feeding is the fact, that women who from the beginning choose not to breast feed may be different from those who do breast feed; for example, women who rely on medication for various reasons may choose not to breast feed because of concerns that medication in the breastmilk may harm the infant. This may explain the recent results from the Dutch Generation R Study (n=3761), which compared non-VIQ scores among those ‘never breast fed’ with different durations of breast feeding, and found a positive association that was, however, attenuated and no longer statistically significant after adjustment for maternal IQ and several potential confounders.24 Another explanation may be that they assessed non-verbal intelligence by two sub-tests of a Dutch non-VIQ test. We used the WPPSI-R, for which reliability coefficients for the IQs for the present age group are very high (0.90–0.96); in our study they are likely to be somewhat lower since IQs are based on only three verbal and three performance subtests.35
Our study sample was originally selected to investigate effects of low to moderate alcohol intake on child development, however, this did not seem to inflict on breastfeeding behaviour, since rates of breast feeding in our sample were similar to rates in the DNBC overall. The differences between women who breast feed or not can only be addressed entirely in a randomised controlled trial, such as the large PROBIT-study in Belarus, where randomisation of clinics and hospitals to breastfeeding promotion resulted in a substantial increase both in breastfeeding exclusivity and duration of any breast feeding. At age 6.5 years children from the PROBIT-study were followed up (n=13 889), and children from the intervention arm scored 7.5 points higher on VIQ from the Wechsler Abbreviated Scales of Intelligence, providing strong evidence for a beneficial effect of prolonged breast feeding on children’s cognitive development.5 Such effects may have a long term impact, as suggested by a Danish observational study, which showed a beneficial association between duration of breast feeding and adult intelligence in two non-overlapping samples (n=973 men and women, n=2280 men, respectively).18 According to Huang et al subsequent schooling and other socialisation experiences during adolescence do not eliminate the breastfeeding gap that appears in very early childhood.47 Furthermore, recent studies have found that the effects of breast feeding may translate into substantial educational differences in adult life20 and economic gains to society.48
Previous studies have suggested three different mechanisms underlying such associations: differences in nutrient compositions between human milk and formula, interplay around the feeding situation, and unidentified factors that correlate with both breast feeding and neurodevelopment, including residual confounding.18 With respect to differences in nutrient content, long chained polyunsaturated n-3 fatty acids, and docosahexaenoic acid (DHA) in particular, may be involved. DHA is deemed an essential fatty acid, because it cannot be intrinsically produced and must hence be provided by the diet, with fatty fish as the main source. Results from the DNBC showed both breast feeding and maternal fish intake to be independently associated with developmental milestones in the young offspring.10
It is a main strength of our study that we were able to include the most important confounders: maternal intelligence, parental education and home environment, which in separate analyses have been shown to account for 19%–29% of the variance in IQ,49 50 also in analyses conducted within the LDPS.51 Additional strengths to our study include the relatively large number of mother–children pairs in our sample, and the fact that child IQ was assessed by a state of the art clinical intelligence test with high reliability coefficients for IQ for the present age group.
The main limitations of our study are the different possible sources of bias inherent in an observational study design. As is the case in most large cohort studies, participants in the DNBC were generally better off and more health conscious compared with the overall Danish population of pregnant women. However, according to a study by Nøhr et al this selection did not result in biased estimates for selected aetiological associations.52 Furthermore, at the time the women in the DNBC reported on breastfeeding duration they were not aware of the outcome under study, making it less likely that their reporting was affected by this. Still, it may be regarded a weakness, that breast feeding was reported at two occasions, when children were 6 and 18 months old, requiring mothers to recall their practices used a few months before the actual assessment. Also, we were not able to investigate dose of breast feeding, since we did not restrict the exposure to exclusive breast feeding.
The LDPS oversampled mothers with moderate alcohol intake in pregnancy, which we adjusted for by weighing all analyses by the relevant sampling fractions. Furthermore, maternal alcohol use was not strongly associated with poorer performance at 5 years.32 53 54 We therefore believe it to be unlikely that any of the associations we observe are due to selection bias caused by the sampling in the LDPS. However, it may still be regarded as a limitation, that participants for this sub-study of the DNBC were not selected at random, but by very specific exposure criteria related to maternal behaviour during pregnancy. We believe that this has been remedied by our weighing of all analyses by sampling fractions, and that our results can therefore be seen as generalisable to the DNBC, and the Danish population.
Associations tended to be attenuated with increasing number of covariates in our analyses, suggesting unadjusted confounding or sparse data bias.55 As is always the case in observational studies, we cannot exclude that our results are affected by residual confounding or confounding by factors not accounted for in our analyses. Furthermore, there may be postnatal factors influencing child IQ that we have not been able to take into consideration; however, these may not act as true confounders but rather as intermediates, in which case they should not be included in the analyses.
Current recommendations from the WHO are that women should breast feed exclusively for the first 6 months. Our finding of a three point difference in IQ associated with any duration of breast feeding longer than 1 month is in support of current recommendations, and is even a relaxed message to mothers who struggle with exclusive breast feeding. Furthermore, our finding of a somewhat lower, but still significant difference of 1.6 IQ point between those breast fed for 6 months or longer compared with shorter durations underlines the advantage of adhering to the recommendations of the WHO of continued breast feeding beyond 6 months of age. Although negligible when considered at the individual level, seen from a public health perspective a difference of 3 IQ points must be considered substantial, and smaller effects have previously led to quite conservative precautionary recommendations, for example with respect to adverse effects of maternal exposure to environmental toxicants.56
Conclusion
In conclusion, in this large sample with high quality assessment of child IQ, we found support of a beneficial association for breast feeding with child IQ at 5 years of age, while adjusting for maternal IQ and parental education, which only few previous studies have been able to do. Taking the necessary precautions that our results may reflect residual confounding, our findings support current recommendations with respect to breast feeding in relation to cognitive development of the child.
References
Footnotes
Contributors The authors’ responsibilities were as follows: SFO and MS designed research. ELM, USK, SFO, TH, JO and MS provided essential materials and conducted research; MS and TH performed statistical analysis; MS, TH, ELM, USK, SFO interpreted the results. MS wrote paper; MS had primary responsibility for final content. All authors read and approved the final manuscript. All authors had full access to study data.
Funding The Lifestyle During Pregnancy Study was supported primarily by Centers for Disease Control and Prevention, Atlanta, Georgia, USA, and also from the National Board of Health, the Lundbeck Foundation, Ludvig & Sara Elsass’ Foundation, the Augustinus Foundation, and Aase & Ejnar Danielsens Foundation. Furthermore, the study was supported by the European Union (EU) Integrated Research Project EARNEST (FOOD-CT-2005-007036). The Danish National Birth Cohort has been financed by the March of Dimes Birth Defects Foundation, the Danish Heart Association, the Danish Medical Research Council, and the Sygekassernes Helsefond, Danish National Research Foundation, Danish Pharmaceutical Association, Ministry of Health, National Board of Health, Statens Serum Institut. The study is part of the research programme of the Centre for Fetal Programming (the Danish Council for Strategic Research grant no. 09-067124).
Disclaimer The funding sources had no role in the study design, interpretation of the data or publication of the results.
Competing interests None declared.
Ethics approval The study was approved by the DNBC Board of Directors, the DNBC Steering committee, the regional Ethics Committee, the Danish Data Protection Agency, and the CDC Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are not available for this study due to the data regulations from the relevant cohort responsible: the Lifestyle During Pregnancy Study and the Danish National Birth Cohort.
Patient consent for publication Not required.