Article Text

Abstract
Introduction The strong correlation between domestic and family violence (DFV) and mental health has been well documented in studies. Pregnancy is a period when both DFV and mental distress tend to occur and/or accentuate. Although limited, available evidence from developed countries has shown continual support and education as psychological first aid that can reduce DFV and improve mental health. However, there is significantly less number of studies from resource-constrained countries; thus, there continues to be a substantial gap in knowledge and awareness regarding effective interventions for DFV.
Methods and analysis A two-arm randomised trial with a nested qualitative study has been planned to assess feasibility and treatment effect estimates of a counselling-based psychosocial intervention among pregnant women with a history of abuse. A total of 140 pregnant women who meet the inclusion criteria will be recruited into the study. Block randomisation will be used to allocate women equally into two groups. The intervention group will receive a counselling session, an information booklet and continuous support by a researcher, while women in the control group will receive contact information of local support services. Feasibility measures, such as rates of recruitment, consent and retention, will be calculated. Qualitative interviews with participants and healthcare providers will explore the acceptability and usability of the intervention. Outcome measures, such as psychological distress, quality of life, social support and self-efficacy, will be measured at baseline, 4 weeks postintervention and 6 weeks postpartum.
Ethics and dissemination This study has obtained ethical approval from the Griffith University Human Research Ethics Committee, the Nepal Health Research Council and the Institutional Review Board of a tertiary hospital in Dharan, Nepal. The findings will be disseminated via peer-reviewed publications and conference presentations and will be used to inform a future multicentre trial.
Trial registration number 12618000307202; Pre-results.
- counselling
- domestic violence
- family violence
- Nepal
- randomised trial
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study will be the first study focussing on the impact of a counselling intervention on the mental health of abused pregnant women in Nepal.
The intervention has been developed after extensive literature review and content validation was done by seeking feedback from experts and target participants.
Ideally, a longer follow-up would be preferable to assess the sustained effects of the intervention; however, due to financial and time constraints, follow-up time is limited.
Recruitment of participants will be carried out from a single setting; hence, the sample may not be representative of abused women in general.
Introduction
Domestic and family violence (DFV) during and around pregnancy is an issue of global concern with prevalence rates ranging from 2% to 57%.1 2 Developing countries witness a higher magnitude and severity of DFV during pregnancy when compared with developed countries.3 Almost one in five pregnant women are victims of DFV in Nepal.4 However, there is a greater likelihood that these self-reported figures are underestimated as many women still consider DFV as a normal family matter that needs to be kept within the four walls of a house.5
Reports have unequivocally established that DFV leads to severe negative effects on both women’s and children’s mental and physical health.6–10 There is a clear evidence of a dose–response relationship in which perinatal mental disorders, such as post-traumatic stress disorder, anxiety and depression, increase with the frequency and severity of domestic violence (DV).9 11 12 Such disorders tend to persist long after the abuse ends.11 13–15
Despite an impressive increase in evidence-based knowledge related to healthcare interventions in addressing DFV, there remains considerable ambiguity. The generalisability of published research in this scholarly area is problematic because any available evidence remains largely skewed towards high-income countries, and there exists substantial heterogeneity in both outcomes and methodologies of studies.16 17 Although limited, available evidence suggests advocacy, continual support, access to referral services and education to be combined with stress-reduction techniques and/or cognitive behaviour therapy to keep women safe from DFV and address its negative health consequences.18–20 Few studies have shown counselling-based interventions to be effective in improving safety behaviours, mental health and pregnancy outcomes, and reducing levels of DFV among pregnant women.21–23
DFV is not determined solely by a woman’s behaviours; rather depends largely on behaviours of perpetrators as well as broader sociocultural factors.24 Therefore, it is unlikely that a brief intervention will reduce the episodes of DFV and fix everything that a victim is experiencing.23 25 However, it is possible for victims to adopt strategies to promote their safety and well-being.22 26 Considering this, safety planning has been the core concept of most DFV interventions.25 27 However, women with poor mental health may face difficulty to adhere to safety behaviours and/or effectively use support services.28 In addition, stigma and fear of retaliation associated with disclosure inhibit help-seeking behaviours.29 Thus, in order to improve coping mechanisms against DFV, it is essential to enhance mental health of victims.
There is an urgent need for the development and implementation of context-specific and culturally safe interventions to improve the mental health and the quality of life (QOL) of women experiencing DFV. In Nepal, despite legal and institutional commitments to safeguarding women, the transition of such provisions into action is far from satisfactory; only 13% of women were aware of anti-DV law and 34% had used support services.30 31 Furthermore, there is lack of evidence on effectiveness of response mechanisms.32
Streamlining interventions for mental health and DFV within antenatal care (ANC) is likely to increase service accessibility, and reduce treatment gaps and stigma.12 WHO and the Centers for Disease Control and Prevention (CDC) have considered these intersecting issues—DV and mental health—as major targets for prevention and intervention.13 Within the context of developing countries including Nepal, implementing an intervention in antenatal period has several advantages: (a) cost-effective33; (b) repeated interactions with healthcare providers (HCPs) facilitates disclosure34 and (c) potential to reduce the risk of postnatal mental disorders and possible negative effects on fetal development.9 Presently, 84% of women have at least one ANC visit in Nepal30; therefore, it is applicable and feasible for women to gain some benefit from even a single session intervention delivered during their antenatal visit.
A randomised controlled trial (RCT) will be conducted at an antenatal clinic in a tertiary hospital within the eastern region of Nepal. The aims of the trial are to (a) assess the feasibility and acceptability of a counselling-based psychosocial intervention delivered in a healthcare settings; (b) assess the efficacy of the intervention on mental health, QOL, perceived social support and help-seeking behaviours of participants; (c) explore facilitators and barriers related to the intervention delivery and (d) generate recommendations for scaling up intervention in future.
Conceptual model of the study
A conceptual framework for this study has been adapted from the framework developed for the Safe and Sound intervention.35 36 The intervention will be primarily informed by the psychosocial readiness model (PRM), which takes into account the changeable nature of women’s actions and desires, and acknowledges improvement in QOL and help-seeking behaviours as desirable actions for women who do not want to leave their relationship.37 Recent studies have used the PRM to guide an intervention aimed at improving relationships and safety decisions.25 36 38 It is considered that when all three internal factors, awareness, perceived support and self-efficacy, are in place, a woman may feel a readiness to change, while a weakness in any one factor may pose a resistance to change.37 Integration of the Kennedy model into the PRM explains how the intervention facilitates the victims’ decision to seek help and access resources.35 39
Studies have shown self-efficacy and perceived social support as important psychological resources for improving mental health of abused women.25 38 40 It is not the number of supportive people available that acts as a substantial buffer against DFV and poor mental health, but the perceived quality of and satisfaction with support available.39 It is hypothesised that a woman’s own recognition of abuse along with an awareness of available support services will enhance her self-efficacy, improve her mental health and prepare her for adopting effective coping mechanisms at the times of DFV (figure 1).36
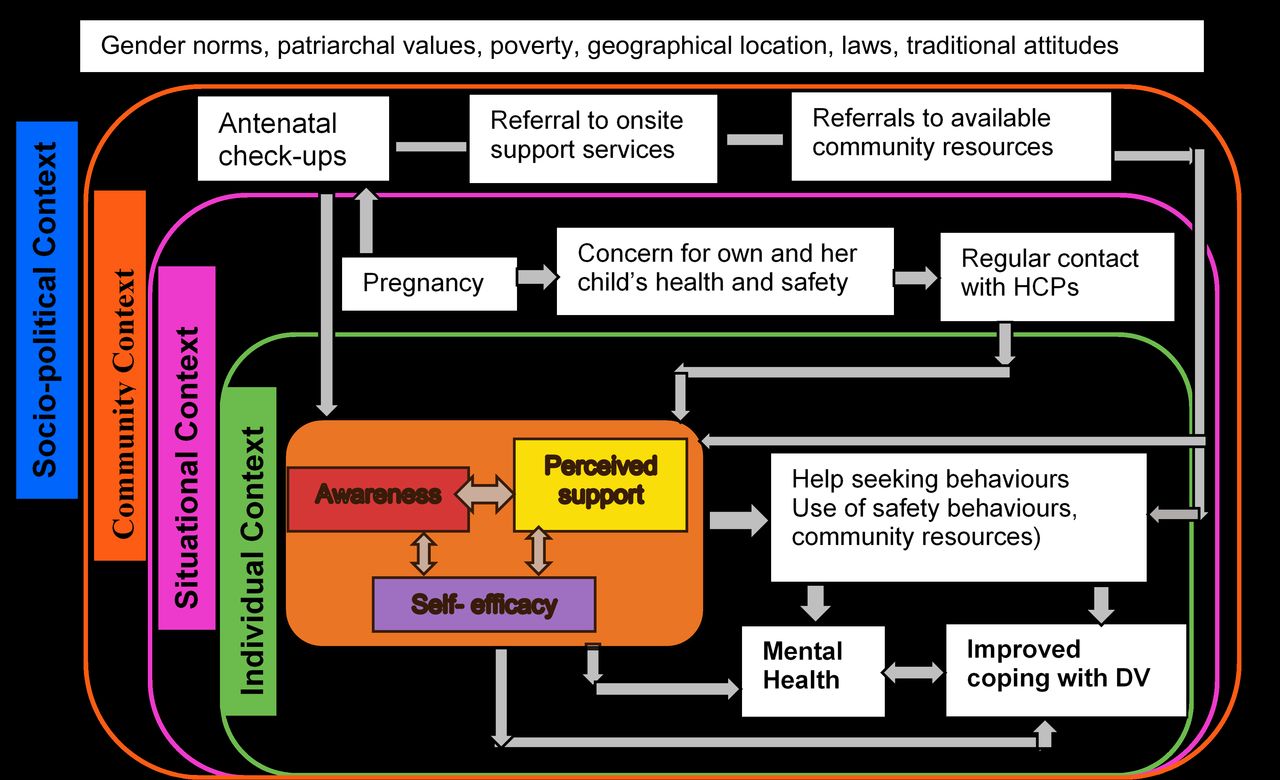
Conceptual framework of the study. DV, domestic violence; HCPs, healthcare providers.
Methods and analysis
Standard Protocol Items: Recommendations for Intervention Trials (SPIRIT) reporting guidelines have been used.41
Study design
A two-arm parallel-RCT with a nested qualitative study will be employed. CONsolidated Standards Of Reporting Trials (CONSORT) has been used to illustrate the design of RCT (figure 2).42
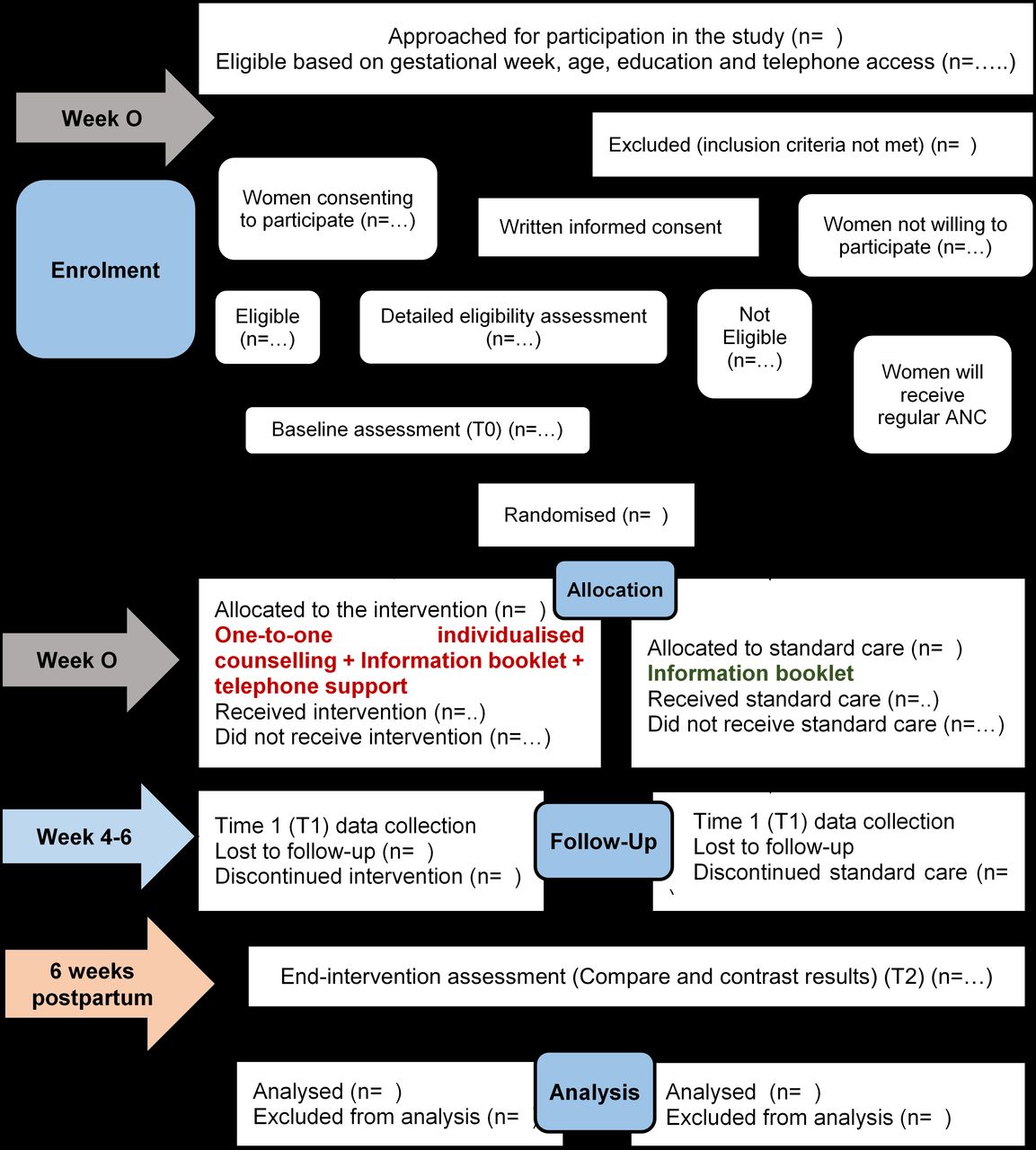
CONSORT diagram of the study. ANC, antenatal care; CONSORT, CONsolidated Standards Of Reporting Trials; T0, time 0; T2, time 2.
Study setting
BP Koirala Institute of Health Sciences (BPKIHS), the largest tertiary hospital with a 750-bed capacity, located in the eastern region of Nepal was selected purposively for data collection. Approximately 120–150 pregnant women visit ANC clinic every day (based on discussion with the head of obstetrics department and review of antenatal register).
Sample size
Since no studies were found to be similar to the proposed study, Cohen’s recommendation on effect size has been considered sample size estimation.43 It is acknowledged, however, that this is a feasibility study where we will aim to calculate the effect size to use in further larger studies. In the absence of standardised effect size, the moderate effect size is usually considered clinically significant and attainable.43 Furthermore, a condition, such as DFV, is a sensitive issue with limited disclosure, and with the given inclusion and exclusion criteria, it will be difficult to recruit a large sample within a limited time period. Calculation was performed using G*Power. With 80% power, alpha level 0.05, two-tailed, medium effect size (0.5) for differences between two independent means and 10% expected attrition rate,22 44 the overall sample is 140.
Participants’ inclusion and exclusion criteria
Women will be included if they (a) are aged 18 years or older; (b) are 24–34 weeks pregnant; (c) have a history of DFV (at least one affirmative response in Abuse Assessment Scale)45; (d) can read and understand Nepali language and (e) have access to a telephone. Women will be excluded if they (a) are at risk of ending their lives; (b) are displaying severe mental health disorders (psychotic disorders and substance dependence); (c) have severe cognitive impairment (severe intellectual disability or dementia) or (d) have hearing impairment.
Description of the intervention
The proposed intervention is based on empowerment counselling model, which has been found to be effective in developed settings,21 22 and are also being adopted in some studies from low- and middle-income countries (LMICs).36 46 This intervention aims to provide abused women with the means to ventilate their feelings and discuss strategies to improve their mental health and social support. Stress management and problem-solving techniques will be discussed based on ‘Problem Management Plus’, which was found effective in improving mental health of abused women in low-income countries (LICs).47 48 Interactive components of this intervention are depicted in figure 3.

{kind=link}
{kind=link}
{kind=link}
Interactive components of the intervention.
Supportive counselling
Empathetic listening to and counselling of woman will be offered in a non-judgemental way, similar to other studies from LMICs.36 44 Being supportive and offering practical help is considered as a psychological first aid.49 When a woman feels that her experiences have been validated and listened to, her self-efficacy improves,50 and she feels empowered to move out of her traumatic experiences.22 26
Mentoring/education
The provision of evidence-based information will fill any gaps in knowledge and facilitate informed decision-making.21 22 51 The booklet includes evidence-based information with relevant examples, and it will be used to facilitate interactive discussion.
Facilitative strategies
Continuous access to the research team and encouraging participants to call when needed will enhance woman’s feelings of being supported. Consistent support is considered particularly important in promoting woman’s emotional health.25 52
The intervention will consist of the following:
A counselling and education session lasting about 30–40 min in the ANC clinic.22 44 The session will adhere to the key skills of effective counselling and follow the guidelines provided by WHO for working with women subjected to DFV.53
An information booklet, including information about DFV, stress and problem managing techniques, safety planning and social support, has been prepared in simple Nepali language with figures and examples as appropriate. It also includes contact details of locally available emergency and support services for DFV.54
Contact details of the researcher will be provided and women will be encouraged to contact and seek advice in managing their daily stressors or family issues as needed.
Description of the standard care
Standard care group will receive a booklet containing contact details of local referral services including shelter homes, counselling, legal support, and police and child protection, based on minimum standards given by WHO in 2016.54 Interested women from this group can have access to the booklet prepared for intervention group by contacting ANC staff after completion of the study. Booklets designed for both groups also contain general information about pregnancy and childbirth.44
Training to the research team
A 1-day workshop will be conducted, which will include brief information about the objectives and implications of the research, and ethical issues regarding conducting intervention research in Violence Against Women (VAW).54 The research nurse will be trained on screening, consent taking and data collection using participatory discussion and role plays. The research nurse has completed her master degree in psychiatric nursing and has several years of experience in research, patient counselling and management. The local supervisor will be responsible for administrative support and supervision of fieldwork. ANC staff who is unable to attend the workshop will be provided with a written description of the study including the eligibility criteria of participants.
Data collection procedures
Phase 1: recruitment, baseline data collection and randomisation
Recruitment of study participants
A participant flyer and one-to-one invitation will be used as recruitment strategies. At the time of registration for their appointment, ANC staff will inform potential participants about the study. Interested women will be asked to go to the counselling room adjacent to the registration room. As only women are allowed in this room, complete privacy during interview can be ensured. Written informed consent including permission to conduct eligibility screening, provide contact details to the research staff, access to medical records, participate in intervention or control group and carry out one-to-one interview will be obtained. Women will be asked whether they want to and if it is safe for them to take the information sheet and consent forms to their homes; if not, the research staff will keep them secure. If a woman reports suicidal thoughts or if there is a serious risk of violence to her and/or her baby, she will be immediately referred to the support services and not included in the study.
Anticipating the possibility of loss of women who screen positively for DFV, an intervention will be delivered on the same day of enrolment. However, if some wish to take more time to consider their participation, they will be provided with an opportunity to participate during their next antenatal visit or arrange suitable date and time with the researchers for data collection. Ineligible participants will be provided with an explanation for their exclusion from the study. Considering time and financial constraints, participants will be recruited for 3 months; however, if the estimated sample size is achieved early, recruitment will be stopped.
Baseline data collection and randomisation
Baseline assessment (T0) will take on average 20–30 min. Considering the small sample size, block randomisation will be used to reduce bias and ensure an equal balance between the intervention and control groups. Randomly varying block sizes of two, four and six have been developed in an MS Excel sheet by a statistician who is not directly involved in the study.55 The research staff will be unaware of the development of the random sequence. The research nurse will not be aware of the allocation status and will provide sequentially numbered and sealed envelopes to participants after baseline data collection.
Phase 2: intervention delivery
The intervention nurse, principal investigator (PI) of this study, will open the sealed envelope and provide counselling to those in intervention group. She is a trained counsellor with previous experience of working with victims of DFV. Motivational interviewing skills, such as clarifying, paraphrasing and reflecting the content and feeling, will be used to ensure that the researcher clearly understands participants’ feeling. All attempts will be made to build a good rapport and participants will be encouraged to express their concerns and problems openly. A guide containing instructions for conducting the intervention along with sample scripts has been developed. However, this guide is not prescriptive, rather indicative and attempts will be made to conduct the session in a natural conversational style responding to woman’s individual needs. All topics may not be covered in same depth with every single woman as different women may have different needs; however, the intervention nurse will ensure that key points outlined in the intervention delivery guide are covered. Women enrolled in both groups will receive their regular ANC care from their HCPs. They will be informed that after 4–6 weeks of the initial session, postintervention data collection will be conducted during their next antenatal visit.
Phase 3: follow-up
Follow-up interviews will be collected at 4–6 weeks postintervention (T1) and 6 weeks post birth (T2) by the research nurse. The intervention nurse will ask participants in the intervention group about the perceived support from the intervention and recommendations to improve the intervention in future in both follow-up assessments. If a woman is unable to be located or does not turn up for her check-up, a telephone interview will be conducted. The researcher will ensure if the right person picks up the phone and it is safe to talk. If not, she will disguise the call as a follow-up call to check on the progress of the baby and will ask the woman to call back her at any time feasible for her. Guidelines for conducting telephone interview have been prepared in Nepali and will be followed strictly. After T1 data collection, HCPs (two nurses, two clinicians and one manager) involved in the care of pregnant women will be purposively selected for key informant interviews. A number of approaches, such as interviews with HCPs and women enrolled in intervention group, reflective opinions by the researchers and meeting notes, will be used to gain a better understanding about the feasibility and acceptability of the intervention.
Retention of study participants
Alternative safe contacts and preferred time for making phone calls to women will be recorded. At least two phone calls in each provided numbers will be made as a reminder for follow-up. However, if the researcher is unable to locate women after two attempts, then in the interest of safety, no further calls will be made and they will be coded as lost to follow-up. Efforts will be made to use friendly, warm communication strategies to establish good rapport with participants. Participants will be provided with a small incentive (NRS 200 equivalent to US$1.69) during each visit as reimbursement for transportation and/or meal costs.
Data collection tools and techniques
Standard tools will be used for one-to-one interview with the participants. Time points of measurement of different outcomes along with a brief description of data collection tools are illustrated in table 1.
Description of outcome measures and time points of assessment
Data management and analysis
The SPSS V.25 will be used for statistical analysis. Feasibility measures will include a number of women screened eligible for the study, providing consent to the study, completing the intervention, completing postintervention assessment and lost to follow-up. Participant characteristics will be analysed using descriptive statistics, such as frequencies, percentages, means and SD. Intervention effectiveness will be assessed by comparing changes in outcome measures between baseline and postintervention assessments in both groups using an independent t-test or χ2 test as appropriate. Analysis of covariance will be used to assess the impact of intervention on primary outcome with adjustment of covariates, baseline measurement and group allocation. Modified intention-to-treat analysis will be carried out to include the missing data. Qualitative interviews will be transcribed and line-by-line coding will be conducted to generate the codes. Descriptive thematic analysis will be carried out via NVivo software V.12 (QSR International Pty Ltd, London, UK and US). Qualitative data will be used to provide information regarding the feasibility and applicability of implementing the intervention in healthcare settings, and to triangulate the quantitative findings.
Validity and reliability of the tools
Standard tools used in similar studies will be used for data collection. Forward and backward translation of tools has been done by two bilingual translators. Pilot testing of the translated tools has been conducted to ensure that the tools are easily understood by the participants. Internal consistency of the tools will be assessed by calculating Cronbach’s alpha. Subject experts and potential participants were asked to assess the validity of the booklet and the necessary modifications were made.
Patient and public involvement
Potential participants were included in evaluating the face validity of the booklet as well as in pilot testing of the tools. The summary of the findings will be provided to the hospital and women will be informed that they can access the results by contacting the local supervisor.
Ethics and dissemination
To minimise the unintended risks to the researchers and research participants, ethical and safety guidelines recommended by WHO for intervention research on VAW will be strictly followed.54 The study will strictly adhere to the protocol and any deviations from the protocol will be notified immediately to the ethics committee by the PI.
The researcher will take every possible measure to limit possible harm and maximise potential benefit. Though less likely, the risk of women getting distressed (such as becoming quiet, crying, angry and looking distracted) will be mitigated with the use of trained researchers, who can provide support and assistance to participants appropriately. If a woman needs and/or prefers additional support, she will be provided with an opportunity to visit a psychosocial counsellor available at the hospital. In addition, women will be provided with contact details of local organisations working against DFV and encouraged to seek advice and help. The research will be conducted in a separate and private place. Any data collected will be kept confidential and disclosed only with women’s permission or in compliance with the law. For women with children greater than 2 years of age, the researcher will take care of the children in the playroom of the hospital during the recruitment or data collection phase.
Any inconvenience experienced by the women by participating in the research has been dealt by making the intervention as brief as possible and conducting it at the same time when women visit hospital for their regular antenatal and postnatal check-up. The study will be conducted during waiting time of women at the ANC clinic,35 36 which usually takes up to 3–4 hours; thus, they will not have to give up any additional time for the study. Respondents will be forewarned that if interview session is interrupted by anyone, the researcher will change the subject of discussion to the pregnancy and postpartum care. Extreme care will be taken to ensure woman’s safety at all points of the study; for example, study related information will not be discussed with anyone else other than the woman herself. The research team and hospital staff will discuss the study as a study aimed at promoting women’s health during pregnancy. The information booklet will be of similar size as that of the ANC card with the same front cover for women belonging to both groups. As such, it can be easily kept hidden within the ANC card.35 36 The booklet will have no reference to DFV on its front page and will be titled as Healthy mother makes healthy child.
The findings of the study will be presented at hospital in Nepal and at Griffith University and also in national and international conferences. In addition, findings will be submitted to peer-reviewed journals.
Monitoring and managing risks during the study
Given the short timeframe of this study, it is unlikely that the issue of overwhelming benefit or futility will arise. Hence, this study does not require the Data and Safety Monitoring Board. The study will be conducted according to the protocol and any deviations will be formally notified. Adverse events will be recorded in adverse events reporting form developed according to the guidelines provided by WHO,54 and PI will be notified immediately and PI will notify ethics committee for further action. Conducting research in such sensitive topic may cause emotional upset, stress and anxiety to the researchers. Regular monthly meetings with the team will facilitate discussion about the progress of the study and support research staff in managing emotional and psychological effects of the research.
Discussion
This is a robustly designed trial, comparing a single session counselling session along with an information booklet to standard care using both quantitative and qualitative approaches. The current study seeks to test the hypothesis that women in the intervention group have significantly different mean scores in mental health, QOL, perceived social support and use of safety behaviours compared with those in standard care group. It is further hypothesised that these improvements will be maintained postdelivery. By testing the feasibility, applicability and efficacy of a piloted intervention, this study will enable future researchers to critique and add to the development and implementation of the programme. This study will add to the global stock of literature on effectiveness of psychosocial intervention as a viable strategy for dealing with DFV and its mental health consequences in low-resource settings.
The trial has several strengths. The study is first of its kind in Nepal. The intervention has been developed from an extensive review of the literature and an intervention manual has been prepared. The manual specifies the protocol for conducting intervention; thus, ensures its fidelity and replicability. Measures of treatment efficacy are robust. The study sample will be drawn from a tertiary hospital visited by a large number of socially and culturally diverse group of people.
There are some limitations that should be considered. Recruitment of study participants will be undertaken from a single setting; thus, the sample might not be representative of abused women in general. The limited duration of follow-up may underestimate the intervention effects; however, due to time and financial constraints, a longer follow-up cannot be done. Nevertheless, numbers of promising studies have shown the average follow-up duration to be 6 weeks.22 44 Considering the brief nature of the study, it is likely that the disclosure of DFV may be underestimated; however, every attempt will be made to make participants comfortable and open up. Because of ethical reasons, women in the control group will also be provided with the contact details of support services.54 Researchers’ enquiry about their experiences of violence may make women aware that violence is a problem that needs to be notified and tackled timely. This awareness and provision of referral list has a strong potential to influence the study outcomes.16 36 44
Acknowledgments
This study is being conducted as a part of the PhD of DS, who is a recipient of Griffith University International Postgraduate Research Scholarship and Griffith University Postgraduate Research Scholarship. We are very thankful to the target participants and subject experts who have evaluated and provided feedback to validate the information booklet.
References
Footnotes
Contributors DS is the guarantor of this paper and has conceived the original research idea with guidance from DA, KMB and AS. DS developed the first draft of the protocol and DA, KMB and AS contributed to the revisions of the protocol. PR and RP assisted in validating data collection tools and booklet. DS developed the first draft of manuscript and KMB, AS, PR, RP and DA were involved in its revisions. All authors have read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval Ethical approval is provided by the Griffith University Human Research Ethics Committee (GU Ref. No.: 2018/227), the Nepal Health Research Council (Reg. No. 73/2018) and the Institutional Review Committee of BPKIHS, Nepal (IRC/1250/018).
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.