Article Text

Abstract
Introduction Plantar heel pain syndrome(PHPS) is a common cause of heel pain. It may worsen a patient’s quality of life, and potentially lead to knee, hip or lower back problems. Previous studies have shown that electroacupuncture (EA) and manual acupuncture (MA) are effective treatments for relieving pain in patients with PHPS. However, little evidence supports the use of one intervention over the other.
Methods and analysis A total of 92 patients diagnosed with PHPS will be recruited and randomly assigned to an EA group or an MA group at a ratio of 1:1. Patients in both groups will receive a 30 min acupuncture treatment (three times per week) for a total of 12 sessions over 4 weeks. The primary outcome will be the proportion of patients with at least 50% reduction from baseline in the worst pain intensity measured by visual analogue scale (0–100, higher scores signify worse pain) at first steps in the morning after 4-week treatment. The secondary outcomes will include change in worst pain intensity at first steps in the morning, change in mean pain intensity at first steps in the morning, change in worst pain intensity during the day, change in mean pain intensity during the day, change in the pressure pain threshold, change in ankle-dorsiflexion range of motion, change in Foot and Ankle Ability Measure total score and subscale scores, patients’ global improvement assessment, patients’ expectations for acupuncture and safety evaluation. We will perform all statistical analysis following the intention-to-treat principle.
Ethics and dissemination The study has been approved by our ethics review board (Protocol Approval No. 2018–010-KY). The study findings will be disseminated through presentation at a high-impact medical journal, with online access. We also to plan to present it in select conferences and scientific meetings.
Trial registration ChiCTR-1800016531; Pre-results.
- acupuncture
- randomized controlled trial
- plantar heel pain syndrome
- protocol
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study is the first randomised controlled trial comparing electroacupuncture versus manual acupuncture for pain relief in participants with plantar heel pain syndrome (PHPS).
Strictly standardised endpoints and objective criteria, long-term follow-up, strict quality control and evaluation of patients’ expectations for acupuncture aiming to reduce the risk of bias.
Eligible participants will be restricted to those in a tertiary A hospital in China, the results might not apply to primary hospital or other countries.
Due to the nature of the study, participants and the acupuncturist will not be blinded, which may bring bias and influence the results.
Considering ethics and the acceptance of participants, a placebo/sham/waitlist group will not be assigned, which could not exclude the placebo effect of acupuncture and a possible spontaneous remission of the PHPS.
Background
Plantar heel pain syndrome (PHPS), also referred to as plantar fasciitis, is a common cause of heel pain.1 2 It is characterised by pain exacerbated with the first walking in the morning or after a long period of rest.3 In the USA, more than 2 million people per year seek treatment due to heel pain,4 and approximately 10% of the general population is affected by heel pain during their lives.5 Excluding conditions, such as fat pad atrophy, plantar fibromatosis and calcaneal stress fracture, symptoms of plantar heel pain are attributed to PHPS in 80% of patients.6 Patients ranging in age from 40 to 60 years comprise the largest affected 20-year age group.7 PHPS usually occurs unilaterally with bilateral involvement occurring only 30% of the time.8 Common risk factors known to be associated with PHPS include obesity, decreased ankle dorsiflexion or shortened/tight Achilles tendon, excessive running, pes cavus (high arched foot type) and pes planus (flat foot).6 7 9 PHPS may worsen a patient’s quality of life,10 and potentially lead to knee, hip or lower back problems.
PHPS likely has multiple aetiologies in combination with degeneration and inflammation.11 The healing time of PHPS generally varies from 6 to 18 months, although it is a self-limiting condition.8 12 Different approaches are available for the treatment of PHPS, including instrumental-therapy, physical-therapy, drug-therapy and surgical-therapy.1 However, definite effects of instrumental-therapy and physical-therapy are still needed to be confirmed. Meanwhile, drug-therapy (eg, oral analgesics and corticosteroid injections) do not provide sustained pain relief effect,13 and corticosteroid injections may be associated with plantar fascia rupture and plantar fat pad atrophy.11 Surgical-therapy is indicated only after at least 6–12 months of conservative treatment has failed.14 Moreover, some patients are resistant to surgery because of fear or cost. There is little convincing evidence available to support various approaches for treating PHPS.15
Even lack of a unified standard on the definition of acupuncture, most hold the view that acupuncture is a technique of the stimulation of specific points on the skin by the insertion of needles based on the principles of traditional Chinese medicine (TCM).16 Acupuncture has been used to treat a variety of musculoskeletal pain-related conditions (including PHPS) for thousands of years. Acupuncturists’ conceptualisations of PHPS include ‘deficient Kidney Qi’, ‘Bi syndrome’ and others.17 At present, various acupuncture modalities, such as electroacupuncture (EA) and manual acupuncture (MA), are available to clinicians. Stimulation of acupuncture points through needling was shown to inducing analgesia via releasing neuropeptides, such as enkephalin, dynorphin, β-endorphin and endomorphin.18 Two recent systematic reviews concerning the effectiveness of acupuncture in treating PHPS have concluded that acupuncture may reduce PHPS pain in the short-term and acupuncture should be included in recommendations for the treatment of PHPS.19 20 Though broader questions, such as how practitioners choose between the various approaches in different contexts, remain unclear,17 future research should have a focus on exploring the optimum use of acupuncture for heel pain.20
EA and MA are the two acupuncture modalities frequently used, which may exert different therapeutic effects via different mechanisms related to the characteristics of diseases.21 EA has been indicated in some cases where treatment with traditional acupuncture has failed. Moreover, it has been demonstrated to produce a faster and better analgesic effect than MA.22 23
To the best of our knowledge, until now no randomised controlled clinical research has compared the effectiveness of EA with MA in treating PHPS. The objective of this study is to assess whether EA is superior to MA in reducing PHPS pain.
Methods and design
Study design
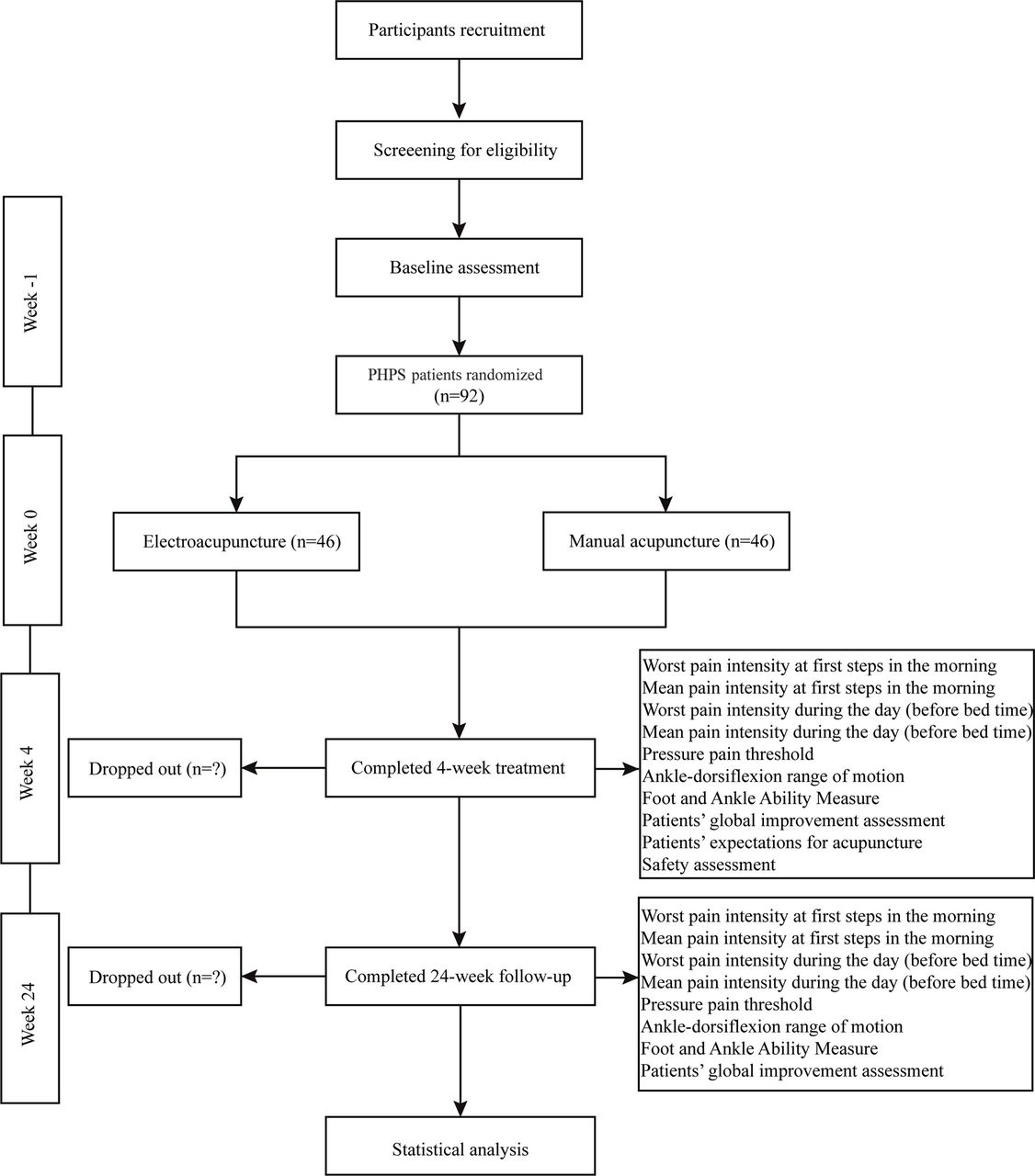
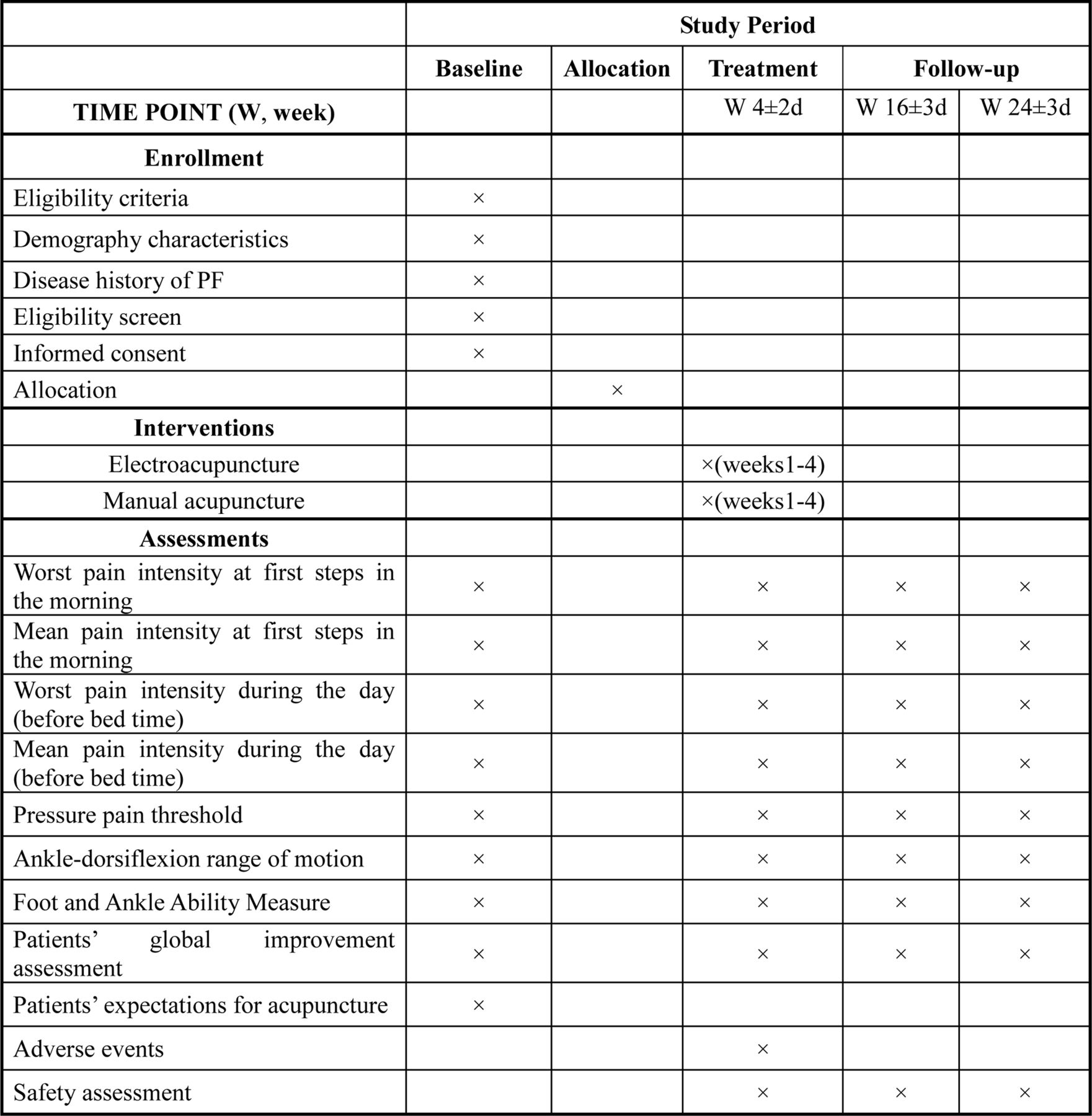
We will conduct a prospective randomised parallel-group assessor-blinded two-arm trial. The standard protocol items including Recommendations for Interventional Trials24 and the Standards for Reporting Interventions in Clinical Trials of Acupuncture25 guidelines will be followed during the development of the protocol of this study. The flowchart is shown in figure 1 and the time point of assessment is shown in figure 2.

Trial flow diagram.

{kind=link}
{kind=link}
The time point of assessment.
Study setting and recruitment
This trial will be performed at Guang’anmen Hospital, China Academy of Chinese Medical Sciences between October 2018 and December 2019. A total of 92 participants will be recruited through posters, hospital webs and networks. The duration of the study for each participant will be 29 weeks: 1-week baseline, 4-week treatment and 24-week follow-up.
Randomisation and blinding
A 1-week baseline assessment will be needed before randomisation. Participants will be randomly assigned to either the EA or MA group at a ratio of 1:1. To ensure equal distribution in treatment groups, the random block is set to a fixed size of four. The randomising scheme will be generated using the Statistics Analysis System software created by the Clinical Pharmacological Assessment Center at Guang’anmen Hospital. Random numbers and assigned groups will be signed and sealed in an opaque envelope by the staff who produced it and kept by other staff who took no part in this trial. Research assistants who did not participate in the assessment and treatment will open the envelopes according to the sequence numbers. The research assistants will be in charge of recruitment and data collection, and an orthopaedist will be in charge of the diagnosis of the participants. Participants and the acupuncturist will not be blinded to the allocation. The efficacy evaluator will be blinded.
Participants
Inclusion criteria
Participants aged from 18 to 75 years will be included in the study if they meet the diagnostic criteria for PHPS according to the Orthopaedic Section of American Physical Therapy Association,26 and conform to all the following conditions for at least 1 month:
Pain localised to the plantar medial aspect of the heel along the insertion of the plantar fascia.
Most noticeable plantar medial heel pain with initial steps after a period of inactivity (eg, initial steps in the morning) but also worse following prolonged weight bearing.
Palpation/provocation over the medial calcaneal tuberosity or along the plantar fascia.
Active and passive talocrural dorsiflexion range of motion (DFROM).
Positive windlass test as well as negative tarsal tunnel tests.
A minimum score of 40 in worst pain intensity at first steps in the morning according to the 100-point visual analogue scale (VAS).
Signed the informed consent prior to the inclusion.
Exclusion criteria
Participants who fulfil any of the following criteria will be excluded:
A history of ankle and foot fracture, surgery or tumour, or have a foot deformity.
A history of plantar fascia rupture, nerve entrapment syndrome or Achilles tendon lesions.
Neurological or systemic diseases including rheumatoid arthritis, diabetes, cardiovascular disorder, severe hepatic/renal insufficiency or coagulation disorder.
Existing systemic or local infection, or chapped heel skin.
Used local corticosteroid injections in the last 6 months.
Needle-phobic patients or had received EA or MA in the past 4 weeks.
Intervention and comparison
The intervention protocol of this trial is based on the meridian theory of TCM and the consensus of three acupuncture specialists, it is also used in a systematic review.19 Acupuncturists who hold an acupuncture license and have at least 1 year of experience in acupuncture will perform the treatment. Disposable acupuncture needle (size 0.30×40 mm) and SDZ-V EA apparatus (all Hwato brand, Suzhou Medical Appliance Factory, Suzhou, China) will be used in this trial. Acupuncture will be given on the heel pain side. If a subject experienced PHPS on both sides, the treatment will be performed on both sides with the more serious side evaluated.
EA group
Two Ashi points (the severer tender points over the anteromedial aspect of the heels), Chengshan (BL57), Taixi (KI3) and Kunlun (BL60) will be selected in this trial. On the basis of the principles of TCM, the major cause of PHPS is qi and blood deficiency in the kidney meridian. Sometimes, PHPS may also be associated with qi and blood stasis.27 Whatever the root cause, stimulation of Ashi points can unblock the qi-blood stagnation and result in alleviating pain.28 BL57, KI3 and BL60 will be selected to build and supply qi and blood to the local area and kidney as well as to the whole person. The location of the acupoints will be based on Nomenclature and location of acupuncture points 29 drafted in 2006 by the National Standard of the People’s Republic of China (GB/T 12 346-2006). After the local skin was routinely sterilised in a prone position, the participants’ Ashi points will be vertically inserted by the needles to a depth of 10–15 mm to the plantar fascia layer. For BL57, KI3 and BL60, needles will be vertically inserted approximately 15 mm. All needles other than Ashi points will be gently stimulated by lifting and thrusting combined with twirling and rotating the needle to reach de qi (the sensation of sourness, numbness, swelling and heaviness).30 Paired alligator clips of the EA apparatus will be attached to the needle holders of the two Ashi points. EA stimulation will last for 30 min with a continuous wave of 2 Hz and a current intensity of 0.1–1 mA. The current intensity will be increased until the skin around the acupoints shivers. The manipulation on BL57, KI3 and BL60 should be performed every 10 min; three times in 30 min. All needles were removed after 30 min and pressure applied using a dry sterilised cotton ball.
MA group
Participants will receive MA at the same points as the EA group, followed by the same manipulation as the EA group until de qi is reached. However, there will be no electric current attached to the needle holders. During needles retaining, the manipulation on BL57, KI3 and BL60 should be performed every 10 min; three times in 30 min.
Both treatment groups will receive 12 sessions of treatment over a 4-week period after baseline (three sessions every week). Each session will last for 30 min.
Rescue medication
Throughout the trial, participants will be discouraged from taking any medication or other therapy for PHPS. However, if heel pain is unbearable during the study period, ibuprofen (sustained release type, 300 mg/T) will be allowed for relief up to 600 mg per day (2 T/day) for 3 days. Details of drug use (name, time, frequency and dosage) will be recorded.
Outcome measures
Primary outcome
The primary outcome will be the proportion of responders after the 4-week treatment. The responder is defined as a participant with a decline (by at least 50%) in the worst pain intensity at first steps in the morning compared with baseline. The pain intensity will be measured using a 100 mm linear VAS with 0 representing no pain and 100 the worst imaginable pain. Additionally, the proportion of responders at weeks 16 and 28 will also be assessed.
Secondary outcomes
The secondary outcomes include the following items:
Change in worst pain intensity measured by VAS at first steps in the morning after 4-week treatment, weeks 16 and 28.
Change in mean pain intensity measured by VAS at first steps in the morning after 4-week treatment, weeks 16 and 28.
Change in worst pain intensity measured by VAS during the day (before bedtime) after 4-week treatment, weeks 16 and 28.
Change in mean pain intensity measured by VAS during the day (before bedtime) after 4-week treatment, weeks 16 and 28.
Change in the pressure pain threshold (PPT) at the most painful spot after 4-week treatment, weeks 16 and 28. PPT, known as the minimal pressure when the sensation of pressure changes to pain,31 will be measured by a pressure algometer (Fabrication Enterprises, Inc., White Plains, NY, USA; from 1 kg/cm2 to 5 kg/cm2) consisted of a metal probe with a rubber disc (0.5 cm2) at one end. The pressure applied by pressing the rubber disc to the painful spot perpendicularly moves the needle in the scale at a rate of approximately 0.1 kg/cm2/s through the metal probe. The mean score of three repeated measurements at the tested location will be used for the main analysis. Thirty seconds will be used between each trial. Discomfort felt at values below 1 kg/cm2 are defined as 0.5 kg/cm2.
Change in ankle-DFROM after treatment, weeks 16 and 28: DFROM will be measured by using a digital goniometer (Tangxia Electronic Instrument Factory, Dongguan, China, from 0° to 360°). Each participant will be asked to sit with the popliteal space at the edge of the table and their knees with 90° of flexion in a completely relaxed station. The axis of the goniometer will be centred over the lateral malleolus and the arms are aligned with the fibular shaft and the head of the fifth metatarsal. The examiner passively moves the ankle into dorsiflexion from a neutral starting position until a firm end feel is elicited.32 The examiner will measure the ankle-joint angle three times at maximum DFROM within 10 s between each examination.
Change in Foot and Ankle Ability Measure (FAAM) total score and subscale scores after 4-week treatment, weeks 16 and 28: The FAAM is a 29-item evaluative tool for the function of foot and ankle, which consists of 21-item activities of daily living (ADL) and 8-item sports subscales.33 Each item score ranges from 0 to 4, with higher scores indicating a higher level of function. The FAAM has a maximum potential score (116 total, 84 ADL and 32 sports subscales). The obtained score (total score, ADL and sport subscale scores) is divided by the maximum potential score and multiplied by 100 to get a percentage. If the patient cannot respond, it is left blank and is not a part of the final value of the questionnaire. In this trial, we will use the Chinese version of FAAM, which has been reported to have a satisfactory psychometric property.34
Patients’ global improvement assessment: Patients’ global improvement will be assessed by a 7-point self-reporting scale ranging from 1 to 7, where one indicates ‘complete recovery’, two indicates ‘obvious improvement’, three indicates ‘a little improvement’, four indicates ‘no change’, five indicates ‘a little worse’, six indicates ‘obvious worse’ and seven indicates ‘vastly worse’. The proportions of participants in each category of global improvement assessment will be measured after the 4-week treatment, weeks 16 and 28.
Patients’ expectations for acupuncture: We will assess patients’ expectation for acupuncture at baseline. It includes three brief questions to investigate whether patients believe that acupuncture treatment will help: ‘Do you believe acupuncture is effective for treating the illness?’, ‘Do you think acupuncture will be helpful to improve your PHPS?’ and ‘Which acupuncture manipulation do you prefer, MA or EA?’. For each question, participants will choose ‘Yes’, ‘No’ or ‘Unclear/whatever’ as the answer.
Safety assessment
All adverse events (AEs) will be monitored and reported through the whole trial. AEs will be categorised as treatment-related (eg, localised haematoma, localised infection, broken needle, fainting, nausea, dizziness, vomiting or palpitations) or non-treatment-related within 24 hours after their occurrence. Detailed information on AEs and serious AEs (SAEs)—including the name, onset and end date, intensity, relationship with acupuncture and outcome—will be recorded. Participants are discontinued if the treatments cause serious aggravation of symptoms, which will include an 80% or more increase of existing heel pain measured by VAS at the end of the first hour after acupuncture. Researchers will immediately report SAEs (eg, requiring hospitalisation, causing disability or impaired ability to work) to the Medical Ethics Committee of Guang’anmen Hospital and suspend the study.
Sample size calculation
The null hypothesis is that the proportion of participants with at least a 50% decrease from baseline in the worst pain intensity (as measured by the VAS at first steps in the morning after the 4-week treatment) will be same for MA and EA. A decline by at least 50% in the pain at first steps was regarded as clinically relevant.35 The previous studies reported that 73.3% of the participants had at least a 50% decrease in the pain as measured by the VAS at first steps after the 4-week EA treatment,36 and 44.4% after the 4-week MA treatment.37Power was defined as 80% for an alpha of 5%. Accordingly, 92 participants will be required (46 in each group), assuming a two-tailed test with a 10% loss to follow-up.
Statistical analysis
We will use SPSS V.20 software to perform all statistical analysis following the intention-to-treat principle. The CI will be established at 95%, and the significance level at 0.05. Missing data will be calculated using the actual observational value without imputation if the dropout rate is no more than 10%. For continuous data, the data will be presented as mean±SD deviation when normally distributed or presented as median (IQR) when not normally distributed. The longitudinal continuous data will be compared between groups using repeated-measures analysis of variance (ANOVA) including group and time–group interaction. The other continuous data will be analysed using Student’s t-test and Wilcoxon rank-sum test, and the categorical data using the Χ2 test or Fisher’s exact test, as appropriate. Sensitivity analysis will be performed if necessary. A p value <0.05 will be considered statistically significant.
Quality control
Prior to the trial, all staff will undergo special training on the purpose and content of the trial, treatment strategies and quality control. Acupuncturists in this trial will have an acupuncture license with at least 1 year of acupuncture experience. Monitors will check case report forms once every week as well as the acupuncture operation during the treatment period. Dropouts and withdrawals including the reasons will be detailed documented through the trial. Participants’ information will be stored in locked file cabinets at the study sites with limited access; only investigators have the right to access the data. All investigators will always maintain a strict privacy policy to protect confidentiality before, during and after the trial.
Patient and public involvement
The initial concept of investigating whether EA was superior to MA in reducing PHPS pain was first proposed by a patient who prefers EA rather than MA. No other patients will be included in the recruitment and conduct of the study. The burden of the intervention will be assessed by the patients themselves. The results will be disseminated to study participants via the website of our hospital.
Ethics and dissemination
The study was planned in accordance with the Declaration of Helsinki. The trial has been registered at the Chinese Clinical Trial Registry. All the participants will be fully informed about this trial and given enough time to inquire about details and decide whether to participate or not at first visit. Participants will be asked to sign the informed consent form if they agree to participate. Any modifications to the protocol will be reported and approved by the Ethical Committee of the Guang’anmen Hospital, China Academy of Chinese Medical Sciences and will be communicated with the trial registry, investigators and data monitoring researchers. The study findings will be disseminated through presentation at a high-impact medical journal, with online access. We also plan to present it in select conferences and scientific meetings after the paper about this trial’ results published.
Discussion
The results of this study will clarify the effect of EA compared with MA in treating PHPS. There were several trials assessing EA and MA in the treatment of PHPS.36 38 39 The results have already showed that EA or MA coupled with conventional treatments could reduce pain, disabilities and activity limitations in patients with PHPS compared with conventional treatments.36 38
According to some previous studies, EA can produce a faster and better analgesic effect than MA.22 23 However, no studies have reported the effect of a head-to-head comparison between EA and MA in the treatment of PHPS. This trial comparing EA with MA could fill a gap in the literature; thus, helping physical therapists and acupuncturists in their clinical decision-making.
The VAS is one of the most commonly used instruments for assessment of pain and has been validated to detect changes in pain intensity.40 Moreover, it has also been used in many studies applying acupuncture for PHPS.38 39 Because morning pain localised to the plantar medial aspect of the heel is the distinct feature of PHPS, we will choose the proportion of participant with a decline of at least 50% in the worst pain intensity at first steps in the morning after 4-week treatment compared with baseline as the primary outcome.
The result may help to clarify the effect of EA compared with MA on the pain relief of PHPS. In addition, considering that pain of PHPS can be categorised as pressure pain, PPT (which will be evaluated by an algometer) could be a reasonable objective secondary outcome to help investigating physiological changes of PHPS. Moreover, DFROM measured by a digital goniometer and FAAM are well suited for evaluating the effects of acupuncture treatment for PHPS. These would be supportive of the primary outcome and meaningful for the overall effectiveness evaluation.
Strengths of the study include its strictly standardised endpoints and objective criteria, long-term follow-up, strict quality control and evaluation of patients’ expectations for acupuncture. The trial also has some limitations. First, this is a single-centre study conducted at a tertiary A hospital in China and the results might not apply to primary hospital or other countries. Second, participants and the acupuncturist will not be blinded due to the nature of the study, which might bring bias and influence the results. Third, considering ethics and the acceptance of participants, we did not assign a placebo/sham/wait list group, which could not exclude the placebo effect of acupuncture and a possible spontaneous remission of the PHPS. Fourth, this study mainly focuses on Ashi points, BL57, KI3 and BL60 for PHPS, so that the findings may not be extended to other points for the same condition.
Trial status
No recruitment at present.
Acknowledgments
The authors appreciate the support and efforts from people who have been or will be included in this study. The authors are also grateful of the contribution of our patient adviser (Yang Wang) in the implementation of this trial. The authors would like to offer their sincere thanks to Medjaden Bioscience Limited for their editing work.
References
Footnotes
Contributors ZL is responsible for supervising the clinical study and for communicating important protocol modifications to relevant parties. WW and ZL conceived the idea and designed this trial. RJ is responsible for the recruitment and treatment of patients. YL and JZ are responsible for statistical analysis. This manuscript was drafted by WW and revised by ZL. All authors read and approved the final draft of the manuscript.
Funding This RCT is funded by Guang’anmen Hospital, China Academy of Chinese Medical Sciences, China (Grant No. 2017S393).
Competing interests None declared.
Ethics approval Ethical Committee of the Guang’anmen Hospital, China Academy of Chinese Medical Sciences (No. 2018-010-KY).
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.