Article Text

Abstract
Objectives To investigate the association between caesarean section (CS) birth and body fat percentage (BF%), body mass index (BMI) and being overweight or obese in early childhood.
Design Prospective longitudinal cohort study.
Setting Babies After Screening for Pregnancy Endpoints: Evaluating the Longitudinal Impact on Neurological and Nutritional Endpoints cohort.
Participants Infants born to mothers recruited from the Screening for Pregnancy Endpoints study, Cork University Maternity Hospital between November 2007 and February 2011.
Outcome measure Overweight or obese defined according to the International Obesity Task Force criteria.
Results Of the 1305 infants, 362 (27.8%) were delivered by CS. On regression analysis, BF% at 2 months did not differ significantly by delivery mode. Infants born by CS had a higher mean BMI at 6 months compared with those born vaginally (adjusted mean difference=0.24; 95% CI 0.06 to 0.41, p value=0.009). At 2 years, no difference was seen across the exposure groups in the risk of being overweight or obese. At 5 years, the association between prelabour CS and the risk of overweight or obesity was not statistically significant (adjusted relative risk ratio, aRRR=1.37; 95% CI 0.69 to 2.69) and the association remained statistically nonsignificant when children who were macrosomic at birth were excluded from the model (aRRR=0.86; 95% CI 0.36 to 2.08).
Conclusion At 6 months of age, children born by CS had a significantly higher BMI but this did not persist into future childhood. There was no evidence to support an association between mode of delivery and long-term risk of obesity in the child.
- caesarean section
- body composition
- body fat
- obesity
- childhood
- Ireland
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Data were obtained from a well-phenotyped contemporary prospective longitudinal cohort study.
Body fat percentage was measured by air displacement plethysmography which is regarded as the gold standard method.
A limitation was the unavailability of maternal pre-pregnancy body mass index.
The number of overweight and obesity cases at 2 and 5 years of age was limited.
Introduction
Over recent decades, caesarean section (CS) rates have risen considerably worldwide and in some countries, CS rates now exceed 50%.1 The aetiology of the global CS rate increase is multifactorial and includes a decline in vaginal births after caesarean, physician fear of litigation, maternal request, more multiple pregnancies resulting from greater assisted reproductive technology use and access to private health insurance.2–7
Although a timely CS can be both necessary and life-saving, for example, in cases of obstructed labour, transverse lie and fetal distress/compromise, it nevertheless conveys complications. For the mother, these include an increased length of hospital stay, infection and haemorrhage, as well as a higher risk of respiratory complications in the infant and consequent admission to the neonatal intensive care unit.8
Birth weight is the most commonly used indicator of in utero growth; however, body composition at birth, the relative proportion of fat and fat-free mass can provide a more accurate picture.9 We have shown retrospectively that neonatal body fat percentage (BF%) is more closely linked to risk of CS than birth weight.10 Therefore, conversely changes in BF% could be an early and more sensitive indicator of future health. It has been hypothesised that the described association between abnormal birth weight and future cardiometabolic disease11 across the life course can be more closely attributed to differences in early life body composition than to birth weight differences.9
CS itself has been consistently associated with an increased risk of obesity later in life, although studies have been inconclusive.12–14 It is also unclear whether this increased risk pertains to elective/prelabour CS or emergency CS/CS in labour. Making this distinction is challenging because of limited literature so much so that the latest systematic review and meta-analysis on the topic (2018) performed an analysis including all CS and did not differentiate.15 Several research papers have been able to distinguish between elective and emergency CS but these have been limited by small sample sizes.16–18 With CS in labour, membranes are more likely to have ruptured, thereby exposing the infant to vaginal microflora.19 However, lack of exposure to the vaginal microflora among infants born by elective CS, where membranes are more likely to be intact, has been suggested as the main causal mechanism for the increased risk of obesity later in life.20–22 Some have disputed this23 24; nevertheless, robust data from animal experiments demonstrate a potential causal role for CS delivery in the development of childhood obesity.25
Given the worldwide increase in nonmedically indicated prelabour CS,8 this type of CS represents a potentially modifiable risk factor for childhood obesity. The aim of this study was to investigate the relationship between CS delivery, particularly prelabour CS, and childhood body composition and growth, using a well-phenotyped prospective longitudinal birth cohort with detailed clinical phenotyping of both mothers and their children. We wanted, in particular, to examine the potential confounding effect of macrosomia, as this is both a risk factor for CS and for long-term obesity.
Methods
Data source and population sampled
Data were obtained from the Irish cohort of the prospective Screening for Pregnancy Endpoints (SCOPE) study of ‘low-risk’ nulliparous women with singleton pregnancies (ACTRN12607000551493, www.scopestudy.net/) and its follow-up prospective Irish birth cohort, the Babies After SCOPE: Evaluating the Longitudinal Impact on Neurological and Nutritional Endpoints (BASELINE) study (NCT01498965, www.baselinestudy.net/).
The SCOPE and BASELINE study methodologies are reported in detail elsewhere.26 27 Briefly, the aim of the SCOPE study was to develop screening approaches, clinical and molecular, to predict fetal growth restriction, pre-eclampsia and spontaneous preterm birth in healthy nulliparous women during early gestation. Exclusion criteria included the following: (1) considered to be at high risk of fetal growth restriction, pre-eclampsia or spontaneous preterm birth due to underlying medical conditions (chronic hypertension, diabetes, renal disease, systemic lupus erythematosus, anti-phospholipid syndrome, sickle cell disease, HIV), previous cervical knife cone biopsy ,≥3 previous terminations or ≥3 miscarriages, current ruptured membranes; (2) had a major uterine anomaly, a known major fetal anomaly or abnormal karyotype or (3) received an intervention that could modify pregnancy outcome (eg, aspirin therapy, cervical suture).
In brief, the BASELINE cohort participant’s mothers were recruited at 15±1 weeks of pregnancy from Cork University Maternity Hospital between November 2007 and February 2011. Of the 2579 women approached to participate, 1774 (69%) gave their written informed consent. From those, 1537 (87%) had infants recruited into the BASELINE study. The sociodemographic, lifestyle and physical measurements were collected by trained research midwives. A complete audit trial was available for the data that were entered into a centrally accessed internet database (MedSciNet AB, Stockholm, Sweden).
Exposure and outcome ascertainment
Delivery mode was grouped into four categories, namely unassisted vaginal delivery (VD), operative VD, prelabour lower segment (LS) CS and LSCS in labour. Operative VD constituted delivery by either vacuum extraction or forceps.
Whole body density was calculated from naked weight measured by an electronic scale (seca 384; seca, Birmingham, UK) to the nearest gram divided by body volume estimated by the PEA POD air displacement plethysmography system (COSMED, Concord, CA, USA) within the first 4 days of life and also at age 2 months. The PEA POD agrees highly with the gold standard four-compartment model and is noninvasive, fast and safe.10 28 29
Based on body density and a two-compartment model of body composition (fat and fat-free mass), using values established by Fomon,28 BF%, the primary outcome, was calculated as follows: ([fat mass, kg/body mass, kg]×100).
The child’s height and weight were measured by a trained interviewer using standardised protocols and medically approved instruments. At birth, 2 months, 6 months, 1 year, 2 years and 5 years of age, body mass index (BMI) in kg/m2 was calculated for each child. At age 2 and 5 years, BMI was classified as thin, normal, overweight or obese, according to the International Obesity Task Force (IOTF) criteria.30 31 The IOTF classification begins at age 2 years.
The following potential confounders as reported in the literature12–14 32 33 were included a priori: maternal age, education, ethnicity, marital status, infant sex, maternal smoking during pregnancy, maternal BMI at the first antenatal visit, gestational age (at delivery), birth weight and pre-eclampsia. For instance, smoking cigarettes is a potential confounder because it is a risk factor for both CS birth34 and for childhood obesity.35
Statistical analysis
Stata V.14SE (StataCorp LP College Station, TX, USA) was used for statistical analysis. Categorical variables were described using frequency (n) and per cent (%). Numeric variables were described using the mean (SD) or median (IQR).
Crude and adjusted linear regression models were used to examine the association between mode of delivery and BF%. Linear regression models were also used to evaluate the association between delivery mode and BMI as a continuous measure.
Crude and adjusted multinomial logistic regression models were used to examine the association between mode of delivery and the risk of being overweight or obese. Adjusted mean differences and adjusted relative risk ratios (aRRR), for the linear and multinomial logistic regression models, respectively, were calculated with 95% CIs. Unassisted VD was the reference category and normal BMI was the base outcome for the multinomial logistic regression models. Models were stratified by whether infants were macrosomic or not which was defined as a birth weight >4000 g or ≤4000 g, respectively. We also explored interaction by infant sex. Statistical significance was defined as a p < 0.05.
Patient involvement
Participants were not involved in establishing the research question, outcome measures including the study design and interpretation or writing of this paper. The results will be disseminated via the study website, social media, information evenings and by newsletter.
Results
Of the 1305 infants, 943 (72.3%) were delivered vaginally. The remainder of the deliveries (27.8%) were by CS; prelabour LSCS (12.0%) and LSCS in labour (15.8%), respectively (table 1). At birth, 13.0% of infants were macrosomic (>4000 g); 11.0% were large for gestational age (>90th percentile for customised birth weight centiles). At 2 years of age, 116 (10.9%) children were overweight or obese (using IOTF cut-offs). At age 5 years, the respective number was 118 (14.5%). At age 2 months, the mean (SD) BF% was calculated at 21.8% (±4.3%). BF% approximated to the normal distribution.
Characteristics of the study population at 2 months
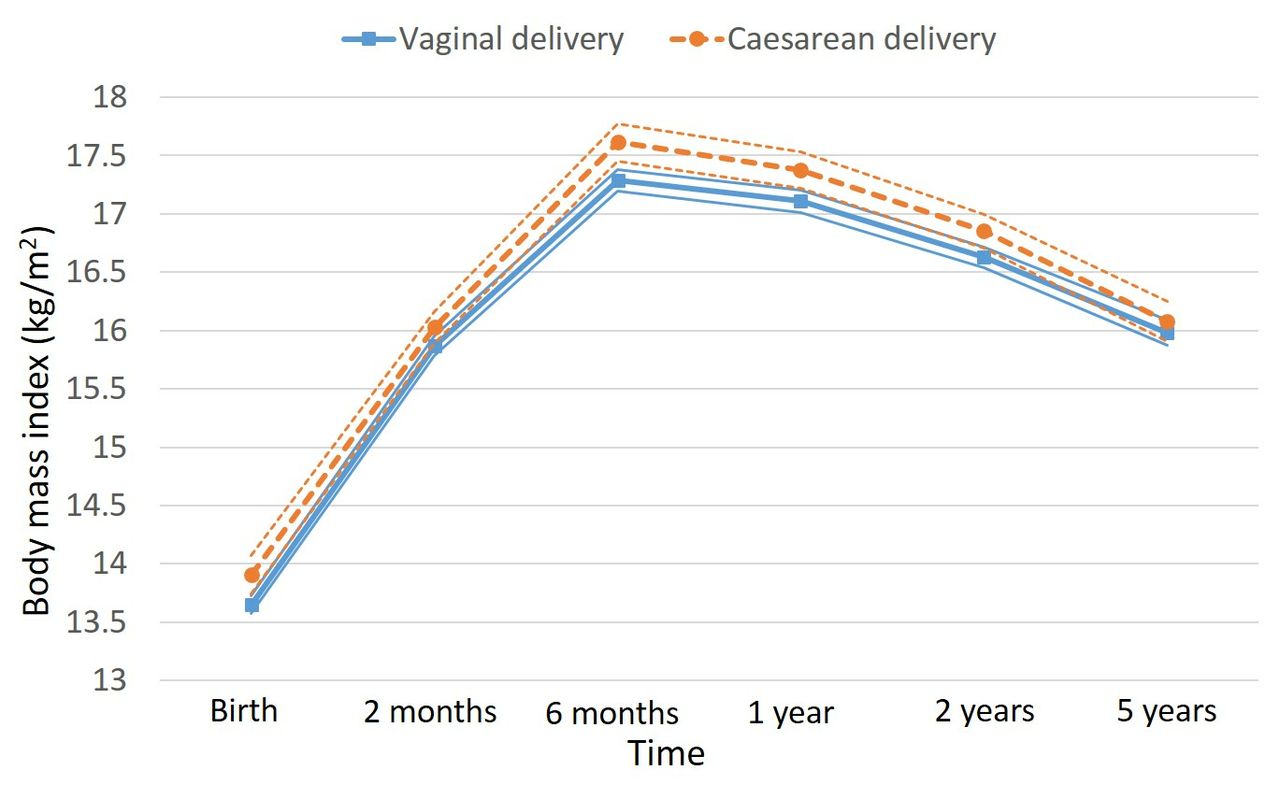
The average BMI, by the four birth modes, at each of the six time points is depicted in figure 1 and for all vaginal and CS births in figure 2. The maximum divergence in BMI by delivery mode occurred at 6 months of age. At 6 months, the mean BMI of infants delivered vaginally and those born by CS was 17.3 kg/m2 and 17.6 kg/m2, respectively.

Mean BMI from birth to 5 years of age: Please note that the time axis has been expanded below age 1 year to permit clearer visualisation. BMI, body mass index; LSCS, lower segment caesarean section.
{kind=link}
{kind=link}
Mean BMI from birth to 5 years of age with 95% confidence intervals (CIs) around the mean BMI—thin lines. There is no overlap of the 95% CIs at 6 months of age. Please note that the time axis has been expanded below age 1 year to allow clearer visualisation. BMI, body mass index .
Across delivery mode, missing data were distributed equally for the primary and secondary outcomes, BF% and BMI, respectively. Thus, missing data were unlikely to have affected the results or conclusions (online supplementary table 1).
Supplementary file 1
Mode of delivery and BF% at age 2 months
At age 2 months, there was no association between prelabour CS and BF% (adjusted BF% mean difference=0.46; 95% CI −0.46 to 1.40) and LSCS in labour (adjusted BF% mean difference=0.07; 95% CI −0.88 to 0.73) in comparison to the reference group of children delivered by unassisted VD (table 2).
Mode of delivery and body fat per cent at age 2 months
Mode of delivery and BMI at age 6 months, 2 years and 5 years
Infants born by CS had a significantly higher mean BMI at 6 months compared with those born vaginally (adjusted BMI mean difference=0.24; 95% CI 0.06 to 0.41, p value=0.009). Limiting analysis to non-macrosomic infants resulted in an adjusted BMI mean difference=0.26; 95% CI 0.07 to 0.45, p value=0.008.
There was, however, no statistically significant differential effect by sex (p value for the interaction term was 0.70; online supplementary figure 1).
There was no statistically significant association between prelabour CS (aRRR=1.38; 95% CI 0.73 to 2.62) or LSCS in labour (aRRR=0.88; 95% CI 0.48 to 1.61) and the risk of being overweight or obese at age 2 years, as compared with the reference group (table 3). Limiting analysis to non-macrosomic infants at age 2 years resulted in the association between prelabour CS and the risk of overweight and obesity being (aRRR=0.95; 95% CI 0.44 to 2.05) and for LSCS in labour (aRRR=0.89; 95% CI 0.44 to 1.82) (online supplementary table 2).
Mode of delivery and body mass index at age 2 years
At age 5 years, there was a nonsignificant association between prelabour CS and the risk of being overweight or obese (aRRR=1.37; 95% CI 0.69 to 2.69) (table 4). There was also no association between LSCS in labour and the risk of being overweight or obese (aRRR=1.69; 95% CI 0.92 to 3.08). Limiting analysis to non-macrosomic infants at age 5 years resulted in the association between prelabour CS and the risk of overweight and obesity being (aRRR=0.86; 95% CI 0.36 to 2.08) and for LSCS in labour (aRRR=2.37; 95% CI 1.19 to 4.68) (online supplementary table 3).
Mode of delivery and body mass index at age 5 years
Discussion
Main findings
There was no significant difference in BF% at age 2 months between modes of delivery. A statistically significant difference in BMI at age 6 months was observed between infants born by CS and VD. Infants born by CS had a higher mean BMI. There was no evidence to support a link between prelabour CS and our secondary outcome, being overweight or obese, at 2 and 5 years of age.
Strengths and limitations
A major strength was the availability of data from a well-phenotyped prospective longitudinal cohort that is among those with the most data available for BF%. This allowed us to investigate the role of factors such as cigarette smoking prior to conception, which is often not available from prior or extant cohorts. In addition, we used robust measures of body composition obtained by air displacement plethysmography, which is regarded as the gold standard method.
A homogeneous sample where 98% of the cohort’s participants were Caucasian, primiparous and ‘low risk’27 could limit the generalisability of these findings to heterogeneous populations. However, the cohort reflected Ireland’s demographics of reproductive age women (15–49 years), where 93% are Caucasian women.36 The variable pre-pregnancy BMI was unavailable; this variable attenuated effect size estimates towards the null12 in previous studies. BMI at 15 weeks’ gestation, a good proxy for pre-pregnancy BMI, was used because 15 weeks is prior to the occurrence of most weight gain in pregnancy. It has been suggested that any association between CS birth and childhood obesity is due to antibiotics administered during CS, with CS delivery serving as a proxy; nonetheless, this proposition has not been supported by evidence.37 38 The major limitation was the low number of cases at 2 and 5 years of age.
Interpretation
The relationship between CS delivery and offspring being overweight or obese has been explored by several systematic reviews and meta-analyses.12 14 15 39 A positive association was the most common finding. Our findings are similar to those of infants, born in 2010, from a Danish prospective cohort study which found that the largest BMI difference by delivery mode, from birth to 5 years of age, occurred at 6 months’ age and that this difference did not track into later childhood at age 5 years.38 In addition, similar to this study, no significant difference in BF% by delivery mode was found. It is worth highlighting that the first 2 years of life have been identified as a critical developmental window during which perturbations in growth and development are more likely to result in lifelong sequelae.40 This Danish study, like ours and also as reported by the systematic reviews and meta-analyses,13 32 did not find a sex-specific growth pattern by mode of birth. This suggests that in humans CS birth might not influence sex-specific growth patterns as has been observed in mouse studies.25
Childhood fat mass index data from a Brazilian longitudinal cohort also showed no significant difference between children born by CS and VD at 6 years of age.41 The declining influence of CS birth on the risk of obesity as children grow older has been attributed to the increasing influence of other risk factors for obesity like physical inactivity, family dietary habits, watching television (and the use of other electronic devices).42 Indeed, a study which utilised a sibling-pair design attributed the observed association between CS birth and childhood obesity to unmeasured confounding.43
Our results are dissimilar to those of children from a Boston, United States (US) cohort study which found a positive association between delivery mode and being overweight or obese at age 5 years.37 The Boston study, unlike ours, did not subclassify CS births into elective and emergency for example, and unusually there were more girls delivered by CS,44 this might indicate reduced external validity for the US study.
A few studies have been able to differentiate between elective/prelabour CS and emergency/LSCS in labour and they have been limited by small sample sizes.16 17 However, a higher risk of childhood obesity for infants born by emergency CS than elective CS was reported.17 Finding an association at age 5 years between LSCS in labour, when membranes are more likely to have ruptured, and being overweight or obese, but not with prelabour CS suggests an attenuated role for vaginal flora in the genesis of children being overweight or obese. A possible explanation for the LSCS in labour association is confounding by the indications for CS. The exact indications for CS were not available for this cohort. However, a divergent BMI trajectory in mid-infancy which then converges by age 5 years between VD and CS babies may suggest a transient role for the vaginal microflora. Further exploration, around mid-infancy, of the association between CS birth and BMI is required.
The CS rate of 27.8%, in this cohort, is consistent with published national estimates of 27.1% to 28.6% that prevailed during the study’s recruitment period from 2007 to 2011.45 This suggests the generalizability of findings to the Irish population, particularly ‘low-risk’ first-time mothers. A macrosomia (>4000 g) prevalence of 13.0% is almost double that of another high-income country, the USA at 7.5% during a similar time period, and suggests high baseline Irish rates of excess adiposity.46 The general Irish population had at age 3 and 5 years a prevalence of 24% and 20%, respectively, for obesity and being overweight47 which is higher than that observed in this cohort. This cohort’s low-risk population likely explains its lower prevalence of being overweight or obese compared with the general Irish population.
Conclusion
We have found no evidence to support a relationship between prelabour CS and offspring being overweight or obese in early childhood. No significant differences in outcome at 2 months and 2 years, and an increased risk of being overweight or obese in children born by CS in labour, but not prelabour CS at 5 years, suggests that the previously hypothesised causal effects due to vaginal microflora are also unlikely at least in the long term.
Acknowledgments
We are grateful to the pregnant women who agreed to participate in the SCOPE study. We thank mothers who permitted their new-born infants to participate in the BASELINE study.
References
Footnotes
Contributors GM, FPM, PNB, LCK, SMBM, DMM, JOH and ASK conceived and designed the study. GM and ASK analysed the data and all authors interpreted the results. GM wrote the first draft of the article and FPM, PNB, LCK, SMBM, DMM, JOH and ASK revised it critically for important intellectual content. All authors approved the final version and agree to be accountable for all aspects of the work.
Funding SCOPE Ireland was supported by the Health Research Board, Ireland (CSA 2007/2). The BASELINE cohort was funded by the National Children’s Research Centre, Dublin, Ireland, and the Food Standards Agency of the United Kingdom (grant no. TO7060). GM is supported by the Irish Centre for Fetal and Neonatal Translational Research (INFANT) (grant no. 12/RC/2272). The other authors report no support relevant to this article.
Competing interests None declared.
Ethics approval Clinical Research Ethics Committee of the Cork Teaching Hospitals (Ref: ECM5 (9) 01/07/2008.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data may be accessed by request from the Babies After SCOPE: Evaluating the Longitudinal Impact on Neurological and Nutritional Endpoints (BASELINE) study. Contact details are available on the study website http://www.baselinestudy.net/.
Patient consent for publication Not required.