Article Text

Abstract
Objective The aim of this study was to explore whether patients with Sjögren’s syndrome (SS) were susceptible to bisphosphonate (BP)-related osteonecrosis of the jaw (BRONJ) after tooth extraction in the entire population of Taiwan.
Design A nationwide population-based retrospective cohort study.
Setting Data were extracted from Taiwan’s National Health Insurance Research Database (NHIRD).
Methodology Medical conditions for both the study and control group were categorised using the International Classification of Diseases, 9th Revision. ORs and 95% CIs for associations between SS and osteonecrosis of the jaw (ONJ) were estimated using Cox regression.
Results Overall, 13 398 patients diagnosed with SS were identified from the NHIRD. An additional 53 592 matched patients formed the control group. At the 3-year follow-up, patients with SS started to exhibit a significantly increased cumulative risk of developing BRONJ compared with that of patients without SS (log rank test <0.001). At the end of the follow-up period, patients with SS exhibited a significantly increased incidence of ONJ compared with that of the controls (0.08%vs0.03%, p=0.017). The Cox regression model showed that patients with SS also exhibited a significantly increased risk of developing BRONJ compared with that of the patients without SS (adjusted HR=7.869, 95% CI 3.235 to 19.141, p<0.001).
Conclusion Patients with SS exhibit an increased risk of developing BRONJ after tooth extraction. BPs should be used with caution in patients with SS.
- sjögren’s syndrome
- bisphosphonate
- osteonecrosis of the jaw
- national health insurance
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The strength of our study is its population-based cohort design with a large number of patients and long-term follow-up, which aims to evaluate the association between Sjögren’s syndrome and osteonecrosis of the jaw (ONJ) after tooth extraction.
The National Health Insurance Research Database registry could not provide detailed information regarding laboratory results, family histories and health-related lifestyle factors.
We did not evaluate the association between ONJ and other antiresorptive and antiangiogenic agents in this study.
Introduction
Osteonecrosis of the jaw (ONJ) is detrimental to patients. The incidence of ONJ is greatest in the oncology patient population (1%–15%). In the osteoporosis patient population, the incidence of ONJ is estimated as 0.001%–0.01%, which is marginally higher than the incidence in the general population (<0.001%).1 Medication-related osteonecrosis of the jaw (MRONJ) is a severe side effect of antiresorptive and antiangiogenic therapies used for the management of oncological and osteoporotic patients.2 Periodic dental checks, non-surgical treatments including antiseptic mouth rinses and cyclic antibiotic therapy, and surgical removal of necrotic bone might be needed in patients with MRONJ. Bisphosphonates (BPs) and the more potent nitrogen-containing bisphosphonates (N-BPs) are used for the treatment of cancer-related bone metastasis, multiple myeloma and osteoporosis. The risk factors for the development of MRONJ include diabetes, tobacco use and treatment with corticosteroids, immunosuppressants or radiotherapy.3 Long-term use of BPs is an important risk factor in BP-related osteonecrosis of the jaw (BRONJ).
Sjögren’s syndrome (SS) is a systemic autoimmune disorder; patients with SS commonly present with dry eyes and dry mouth. The prevalence of SS could be as high as 4.8% in some populations when strictly defined according to the American–European Consensus Criteria, and SS is one of the most common autoimmune diseases.4 SS predominately affects women in the fourth decade of life.5 Dry eyes and dry mouth affect the patient’s quality of life. Patients with SS could have impaired oral hygiene due to dry mouth (xerostomia).6 7 Several molecular mechanisms, including dysregulated transforming growth factor-β (TGF-β) signalling pathways and matrix metalloproteinase (MMP) activation, are associated with the pathogenesis of both SS and BRONJ.8 9 However, the association between SS and BRONJ has not been thoroughly evaluated in large-scale studies.
Based on this evidence, we hypothesised that patients with SS may be susceptible to BRONJ due to shared risk factors and molecular pathways. Therefore, we aimed to determine whether patients with SS exhibit an increased risk of BRONJ after tooth extraction using the statistical analysis of a nationwide healthcare insurance claim database.
Methods
Data source
This is a nationwide population-based retrospective cohort study using data acquired from the Longitudinal Health Insurance Database (LHID) from 2000 to 2013; the LHID is a subgroup database of the Taiwan National Health Insurance Research Database (NHIRD). The National Health Insurance programme in Taiwan provides healthcare for 99% of the population (greater than 23 million people) and was implemented in 1995. The LHID contains deidentified secondary data that are available to researchers. Individual information was protected by encoding personal identifiers to prevent ethical violations related to the data. The LHID provides information on medical service utilisation using a randomly selected sample of approximately one million people receiving benefits, representing approximately 5% of Taiwan’s population. The accuracy of the diagnoses in the NHIRD, particularly diagnoses of major diseases, has been corroborated.10 11 The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnostic and procedure codes (up to five each), gender, birthday, dates of admission and discharge, and outcomes are coded.
Patient and public involvement
The NHIRD encrypts patient personal information to protect privacy and provides researchers with anonymous identification numbers associated with relevant claims information. Therefore, patient consent is not required to access the NHIRD. The International Research Board also waived the consent requirement. This study complied with the Declaration of Helsinki and relevant guidelines.
Sampled patients
The primary outcome of the study was to determine whether patients with SS exhibit an increased risk of developing BRONJ after tooth extraction. This study used study and comparison cohorts. Using the LHID (2000–2013), we enrolled adult patients aged >20 years who were newly diagnosed with SS. The date of SS diagnosis was used as the index date. Tooth extraction significantly increased the risk of BRONJ.12–14 Patients who developed ONJ after tooth extraction, including other specified diseases of the jaw, ONJ, osteomyelitis of the jaw, osteonecrosis and osteomyelitis, were then identified as having BRONJ. We excluded patients who had a follow-up time <6 months and patients who received the abovementioned diagnosis prior to the index date. Radiotherapy and medical treatments, including the use of steroids, BPs and chemotherapy, were analysed for associations with ONJ. Relevant comorbidities, including malignancy, osteoporosis, diabetes mellitus (DM), chronic kidney disease (CKD) and hypertension, were also identified. The relevant ICD-9CM codes are summarised in online supplementary table 1. Control candidate sampling comparisons were selected from individuals in the LHID who did not have a history of SS. The patient and control cohorts were selected by 1:4 matching according to the following baseline variables: age, sex and index year. The index year for control patients was the same as the year for the corresponding patients with SS. Propensity-matching analysis was performed in the logistic regression model. The potential confounders were index year, gender, age and comorbidities. The match tolerance was 0.15 with the nearest neighbour method. The study comparison cohort-matching ratio was fourfold (study:comparison=1:4).
Supplementary file 1
Statistical analysis
Continuous variables, which are presented as the mean and SD, were compared using t tests. Categorical variables, which are presented as percentages, were compared using χ2 or Fisher’s exact test. The associations between those outcomes (prognoses) and clinical characteristics were investigated using the Cox regression model. The results are presented as adjusted HRs with corresponding 95% CIs. The threshold for statistical significance was p<0.05. All data analyses were conducted using SPSS software V.22 (SPSS).
Results
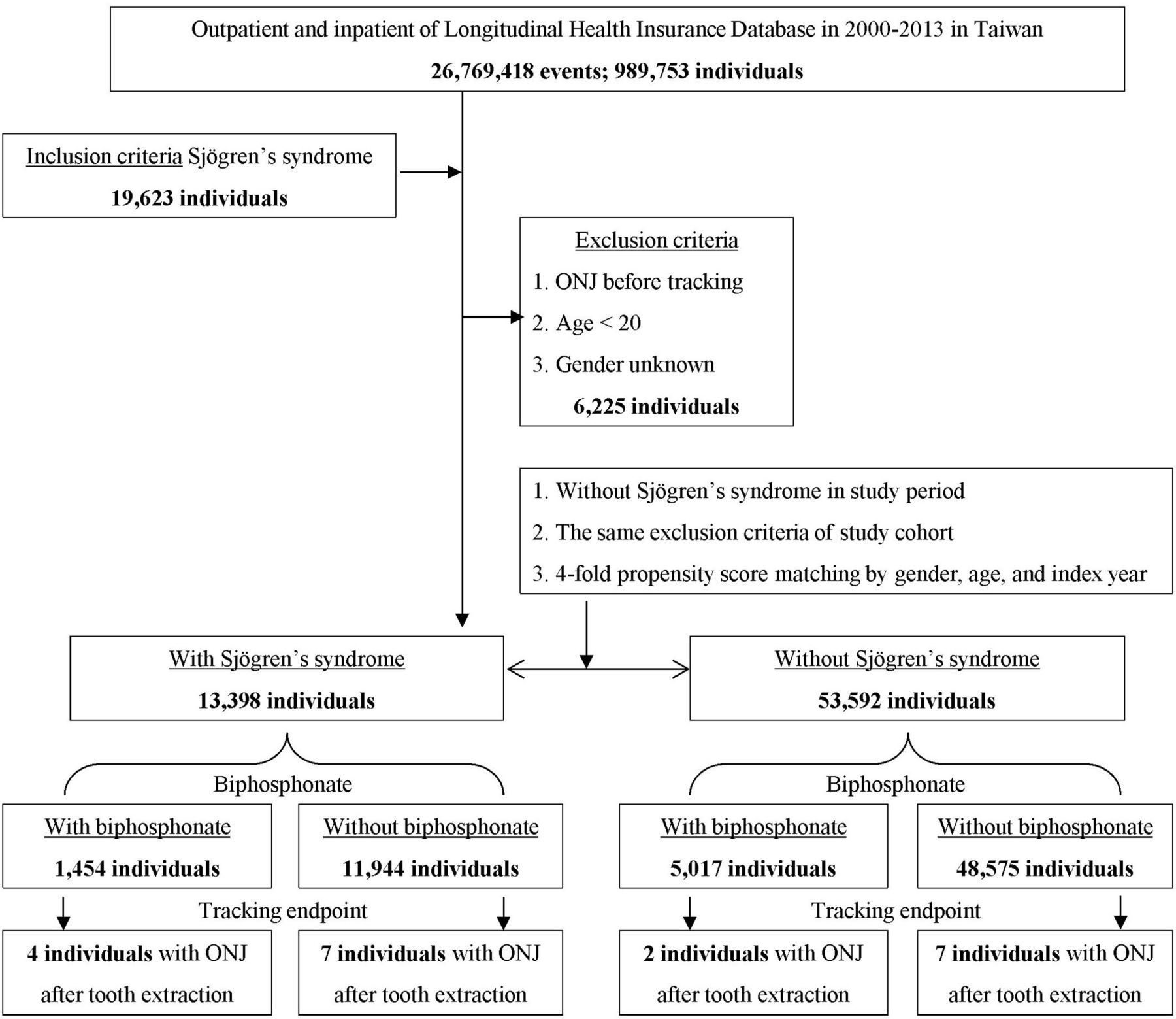
A flow diagram of the patient enrolment procedure is shown in figure 1. In total, 13 398 patients diagnosed with SS were identified in the NHIRD, which contains a total of 989 753 individuals. An additional 53 592 propensity score-matched patients were designated as controls. After matching, compared with the controls, patients with SS had fewer malignancies and lower incidence rates of DM and CKD but more frequent use of BPs and treatment with radiotherapy and steroids (table 1). After 3 years of follow-up, patients with SS started to exhibit a significantly increased cumulative risk of developing ONJ after tooth extraction in subsequent years compared with that of patients without SS (log rank test <0.001, figure 2). Table 2 presents the incidence of ONJ during the 13-year follow-up period. At the end of the follow-up period, patients with SS exhibited a significantly increased incidence of ONJ compared with that of the controls (0.08% vs 0.03%, p=0.017), with increased exposure to BPs (10.85% vs 9.36%, p<0.001), chemotherapy (1.06% vs 0.72%, p<0.001) and steroids (19.65% vs 0.26%, p<0.001). Patient with SS had lower incidences of malignancy (12.06% vs 17.18%, p<0.001), DM (9.64% vs 15.86%, p<0.001) and CKD (1.63% vs 3.54%, p<0.001) than the controls. The Cox regression model showed that independent of the effects of gender and age, patients with SS also exhibited a significantly increased risk of developing ONJ compared with that of patients without SS (adjusted HR=7.635, 95% CI 3.126 to 18.649, p<0.001, table 3). Use of BPs (adjusted HR=2.488, 95% CI 1.005 to 6.156, p=0.045) and male gender (adjusted HR=2.573, 95% CI 1.115 to 5.556, p=0.020) but not chemotherapy, radiotherapy or the use of steroids was associated with an increased risk of ONJ (table 3). Figure 3 shows the interactive effects of SS and BPs after adjusting for other factors. The risk of BRONJ in SS patients without BP treatment was 5.316-fold higher than that of patients without SS and BP treatment. The risk of BRONJ in patients with SS was 19.475-fold higher than that of patients without SS and BP treatment (p<0.001). There were no differences in the incidence of tooth extraction between patients with SS and without SS (9% vs 9%, respectively).

Patient selection flow chart. ONJ, osteonecrosis of the jaw.

Kaplan-Meier curve of the cumulative risk of osteonecrosis of the jaw (ONJ) due to Sjögren’s syndrome.

{kind=link}
{kind=link}
{kind=link}
Interaction between the risk of osteonecrosis of the jaw due to Sjögren’s syndrome and the use of bisphosphonates.
Characteristics of the study participants at baseline
Incidence rates of osteonecrosis of the jaw (ONJ) and other characteristics in the enrolled study participants at the end of the 13-year follow-up period
Factors associated with osteonecrosis of the jaw according to the Cox regression model
Discussion
We found that patients with SS were more susceptible to ONJ than patients without SS. Patients with SS were even susceptible to BPs, with a nearly ninefold increased risk of BRONJ after tooth extraction compared with those without SS.
There is a high risk of underdiagnosis of ONJ due to a lack of awareness and the absence of unified diagnostic criteria.15 Although the incidence of ONJ is rare, the development of ONJ can be devastating. Recognition of patients who are at higher risk is therefore crucial. Risk factors for BRONJ include DM, cancer and the use of corticosteroids, immunosuppressants and radiotherapy. A significant association between ONJ and SS was observed in a recent study analysing the Food and Drug Administration (FDA’s) Adverse Event Reporting System.16 In this study, we further confirmed that patients with SS were susceptible to BRONJ after tooth extraction. We speculate that impaired oral health due to dry mouth could increase susceptibility to ONJ in patients with SS. Dry mouth could result in increased tooth wear, high rates of caries and repeated failure of dental restoration.6 17 18 In the current study, there were no differences in tooth extraction between patients with and without SS. Low saliva flow combined with acid reflux could lead to a low pH in the oral cavity and overgrowth of acidophilic pathogens, which promote tooth decay and mucosal erosion.16 Even when patients with cancer were excluded, the use of BPs, suppuration and extractions remained associated with ONJ.19 Changes in immune cell function and inflammation, with an increased risk of chronic infection, predispose patients with DM to the development of MRONJ.20 Rats with diabetes were also more susceptible to experimental BRONJ than rats without diabetes.21 Steroids may be used to treat SS-induced joint and muscle pain.22 23 Whether the use of steroids increases the risk of ONJ is still controversial. However, one study found that the use of steroids did not increase the risk of ONJ in patients with DM.20 We further found that exposure to steroids, radiotherapy or chemotherapy does not increase the risk of ONJ in patients with SS. In this regard, we recommend caution with regard to the use of BPs in patients with SS.
In the current study, we also found that patients with SS were even more susceptible to BRONJ. Dysregulation of the TGF-β/Smad signalling pathway and MMPs is associated with both BRONJ and SS. Even low doses of BPs can significantly affect the expression of genes involved in osteoblast growth and differentiation through the production of TGF.24 Potent N-BPs, such as zoledronate, can inhibit ischaemia-induced neovascularisation by impairing the mobilisation of endothelial progenitor cells and angiogenic functions, as well reducing bone mineralisation within tooth extraction sockets, with impaired bone healing.25–27 Zoledronate suppresses TGF-β-induced fibrous tissue through the inhibition of Smad-dependent signal transduction.28 Increased TGF-β signalling was observed in salivary glands with increased Smad2 phosphorylation and concomitant increases in extracellular matrix deposition. In a murine model of SS, aberrant TGF-β overexpression caused salivary gland hypofunction.29 While many studies indicated that zoledronate could reduce the expression or activity of MMPs, zoledronate had been shown to increase the amount and enzymatic activity of MMP-9 during oral wound healing after tooth extraction in a rat model.27 Activation of the innate immune system and the production of interferons could be the first stages of primary SS pathogenesis.30 In human salivary gland cells, interferons modulate and increase the expression of MMP-2 and MMP-9.31 The circulating levels of MMP-9 were increased in patients with SS.32
Limitations
Although we adjusted for confounding factors extensively using multivariate logistic regression models, there were several limitations and unmeasured confounders in our study. Although this is a nationwide population-based study, there was a limited number of BRONJ cases. The NHIRD contains up to five ICD-9-CM diagnostic codes for each medical utilisation. Some minor diseases and inactive medical problems could be lost thereafter. The NHIRD registry is not able to provide detailed information on laboratory results, family histories and health-related lifestyle factors, such as alcohol consumption and tobacco use. In this study, we used chronic obstructive pulmonary disease as a surrogate for tobacco use. However, other confounders, such as alcohol consumption, that lack suitable ICD-9CM coded surrogates could still influence the results. The identification of BRONJ by using tooth extraction could also cause selection bias. The relative risk of BRONJ after tooth extraction in patients with cancer who are receiving BP is reported to be up to 50 times higher than that in patients receiving BP who have not undergone tooth extraction.12 13 33 34 We did not address the association between ONJ and other antiresorptive and antiangiogenic agents since there were limited treatment periods and only small amounts prescribed. Although our study identified the association between SS and BRONJ, the cohort study design did not enable the determination of a cause–effect relationship. Further prospective follow-up studies, mechanistic studies and animal experiments should be performed.
Conclusion
Patients with SS exhibit an increased risk of developing BRONJ. BPs should be used with caution in patients with SS.
References
Footnotes
Patient consent for publication Not required.
Contributors M-TL and S-HT wrote the manuscript. J-CW and S-HT conceived and designed the study. W-CC and C-HC provided the materials and analysis tools for the study. C-HC and S-JC analysed the data. All the authors approved the manuscript.
Funding This study was supported by grants from the Taoyuan Armed Forces General Hospital (AFTYGH-10706 and 10707), the Tri-Service General Hospital of the National Defense Medical Center in Taipei, Taiwan (TSGH-C107-004, TSGHC107- 045, TSGH-C107-047) and the Ministry of Science and Technology (MOST 106-2314-B-016-031 and MOST 106-2314-B-016-008-MY3).
Competing interests None declared.
Ethics approval This study protocol was approved and carried out by the Institutional Review Board of the Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional unpublished data from the study.