Article Text

Abstract
Objectives Autoimmune connective tissue diseases (ACTDs) commonly involve the shoulder joint; however, clinical epidemiological studies investigating their association with tendons are scant. Rotator cuff (RC) tears can cause shoulder disability, and surgical intervention is usually required. The study investigated RC repair surgery risk in ACTD patients. The effect of anti-inflammatory medication on RC repair surgery risk was also investigated.
Methods We conducted a retrospective cohort study with a 7-year longitudinal follow-up period. Patients with systemic lupus erythematosus, systemic sclerosis, sicca syndrome, dermatomyositis and polymyositis diagnoses between 2004 and 2008 were enrolled. The control cohort comprised age- and sex-matched controls. The HR and adjusted HR (aHR) were estimated for the risk of RC surgery between ACTD and control cohorts after adjustment for confounders. Furthermore, the effects of steroid and non-steroidal anti-inflammatory drug (NSAID) use on the HR and aHR of RC surgery risk were analysed.
Results We enrolled 5019 ACTD patients and 25 095 controls in the ACTD and control cohorts, respectively. RC surgery incidence was 49 and 24 per 100 000 person-years in the ACTD and control cohorts, respectively. In the ACTD cohort, the crude HR for RC surgery was 2.08 (95% CI , 1.08 to 4.02, p<0.05), and the aHR was 1.97 (95% CI, 1.01 to 3.82, p<0.05). The ACTD patients who used NSAIDs had an aHR of 3.13 (95% CI, 1.21 to 8.07, p<0.05) compared with the controls, but the ACTD patients who used steroids did not have a significantly higher aHR than the controls.
Conclusions ACTD patients had an increased risk of RC repair surgery. However, no difference was found in RC surgery risk when steroids were used compared with the control cohort. This could indicate that inflammation control may be a strategy for managing subsequent RC lesions.
- rheumatology
- orthopaedic sports trauma
- shoulder
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
First large-scale, population-based study on the risk of rotator cuff (RC) lesions among patients with autoimmune connective tissue diseases (ACTDs).
Detailed information of ACTD severity could not be presented.
Although steroids can lower the risk of RC repair surgery among patients, our study did not analyse disease-modifying antirheumatic drugs, which might have influenced the inflammatory status of the study cohort.
To enhance the accuracy of study outcomes, we only investigated the risk of RC lesions and the requirement of subsequent repair surgery; therefore, patients with minor tears or who did not require surgical intervention might have been missed.
Introduction
Autoimmune connective tissue diseases (ACTDs), such as systemic lupus erythematosus (SLE), systemic sclerosis, sicca syndrome, dermatomyositis and polymyositis, are systemic autoimmune disorders that affect multiple organ systems and exhibit intermittent relapse and remission. Owing to the various organs involved in the chronic inflammatory process caused by autoantibody deposition and related inflammatory reactions, ACTD patients—particularly SLE patients—usually present heterogeneous clinical manifestations.1 The musculoskeletal system is one of the organ systems that is often affected, and initial musculoskeletal symptoms are often similar to those of autoimmune diseases.2 The severity of clinical musculoskeletal symptoms varies among individuals. SLE patients can present mild arthralgia without deformity or erosion, non-erosive deforming arthritis or erosive symmetric polyarthritis. In addition, the musculoskeletal symptoms of these patients can include osteonecrosis, tendonitis, myositis and tendon rupture.3 However, few studies have investigated or emphasised lesions of the enthesis in SLE patients in connection with other ACTDs.4 5
Rotator cuff (RC) tear or rupture is one of the most common causes of shoulder dysfunction. RC tears may be asymptomatic, or their clinical presentations can be pain accompanied by a limited range of movement. RC disorders are observed in 30%–70% of patients presenting with shoulder pain, and the incidence of RC tears is 5%–40%.6 Because RC tears can be asymptomatic, studies have reported diverse prevalence rates of RC tears. An ultrasound screening study revealed that the prevalence of RC tears was 20.47% among 1366 shoulders with or without clinical symptoms, and the prevalence increased with age.7 Initially, RC tears can be treated using conventional methods such as exercise or injections.8Patients with extensive RC tears experience limited shoulder function when performing daily activities or working. Surgical repair is recommended to relieve symptoms and restore function. RC repair surgery and subsequent possible complications can increase patients’ medical expenditure and the economic burden on healthcare systems.9
A cross-sectional study investigated hand tendons and revealed the predominance of tenosynovitis or tendonitis.10 Case reports have described the rupture of patellar and hand tendons in SLE patients.11 12 Thus, we hypothesised that SLE patients have a relatively high risk of RC repair surgery because of tendon lesions. In addition, case reports of tendon rupture have mentioned other ACTDs such as dermatomyositis.13 A massive RC tear can cause shoulder disability and surgical intervention is usually required. However, sufficient epidemiological research has not been conducted to prove that SLE and other ACTDs are risk factors for RC tears requiring repair surgery. Thus, we hypothesised that ACTD patients have a higher risk of RC lesions that require repair surgery and conducted this longitudinal, retrospective cohort study to investigate this risk. In addition, we investigated the effect of anti-inflammatory medication on the RC repair surgery risk for ACTD patients.
Methods
Study design
Using a healthcare database, this longitudinal retrospective cohort study analysed the risk of RC repair surgery for ATCD patients. We included patients who had been diagnosed with ACTDs between 1 January 2004 and 31 December 2008. Their data were obtained from the Taiwan Longitudinal Health Insurance Database 2005 (LHID2005), part of Taiwan’s National Health Insurance Research Database (NHIRD). A control cohort consisting of five age- and sex-matched non-ACTD controls per ACTD patient was obtained using the same database. We retrieved data from the database since 2004 with a follow-up period of 2–7 years or until the end of 2010. The follow-up period ended when the patients or controls received RC repair surgery. To ensure patient privacy, their names and identity numbers were replaced by numbers and letters from the English alphabet codes that are used for identifying patient data in the NHIRD. Because the linked identity data were removed, patients’ data could not be identified, and thus, the requirement for informed consent was waived.
Brief background of Taiwan’s National Health Insurance system, National Health Insurance Research Database and Longitudinal Health Insurance Database 2005
Taiwan’s National Health Insurance (NHI) system is a form of social insurance that covers more than 96% of the population of Taiwan.14 15 The NHI programme covers almost all medical services, such as outpatient visits, admission services and emergency hospitalisations. Diagnoses made using International Classification of Diseases Ninth Revision, Clinical Modification (ICD-9-CM) codes, medical prescriptions, procedures and surgeries are recorded in the NHIRD. As previously mentioned, the data used in this study were obtained from the Taiwan LHID2005, which contains the data of 1000000 beneficiaries randomly sampled from the Registry for Beneficiaries of the NHIRD. For research purposes, the National Health Research Institutes of Taiwan collects and maintains registration files and original claims data from the NHI administration and then releases them publicly through the NHIRD.
Inclusion and exclusion criteria
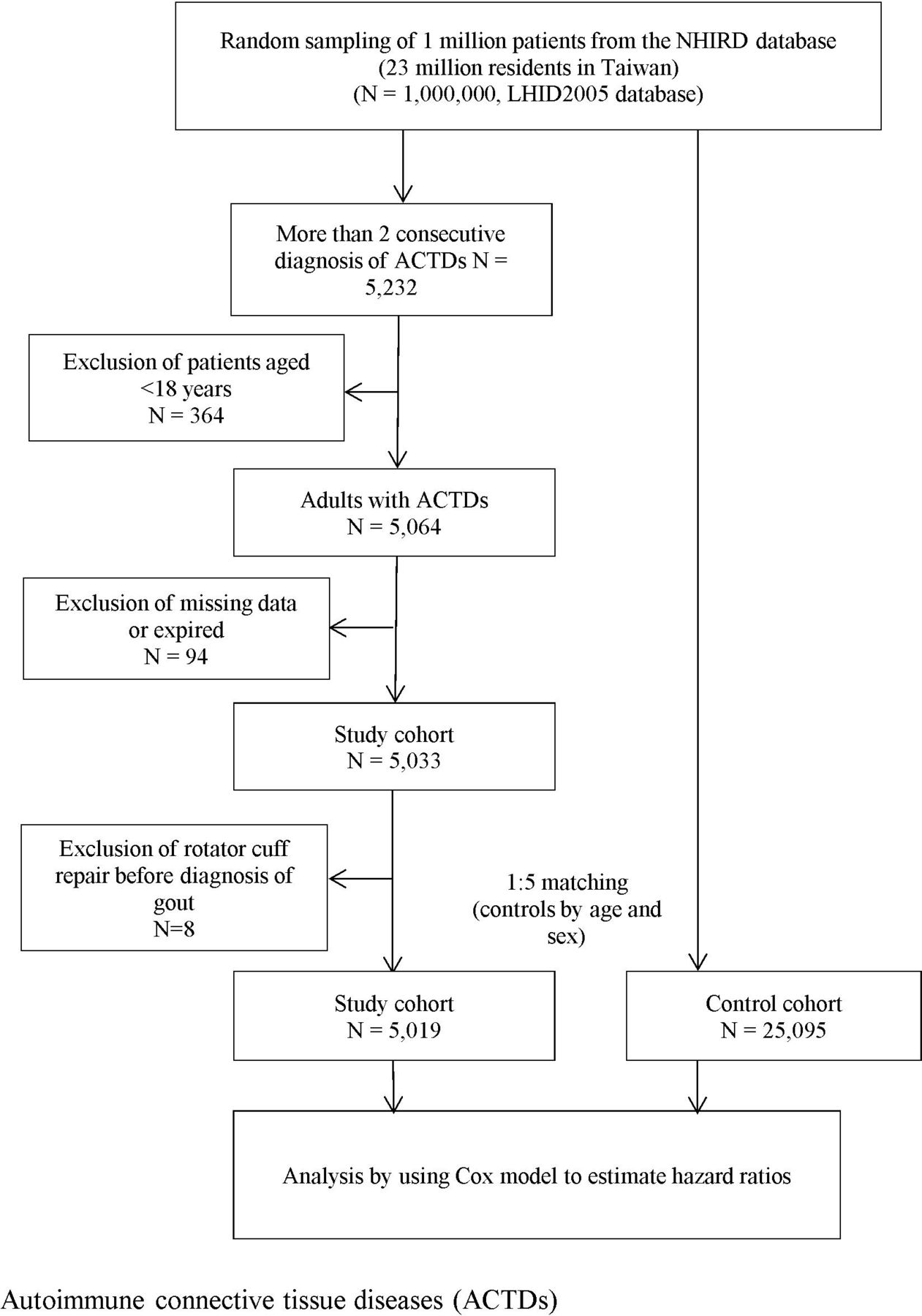
The study cohort included ACTD patients diagnosed with SLE (ICD-9-CM code 710.0), systemic sclerosis (ICD-9-CM code 710.1), sicca syndrome (ICD-9-CM code 710.2), dermatomyositis (ICD-9-CM code 710.3) and polymyositis (ICD-9-CM code 710.4) by using the American College of Rheumatology criteria between 1 January 2004 and 31 December 2008. To ensure high accuracy of the ACTD diagnoses, this study only selected patients diagnosed with ACTDs at least twice consistently, according to ICD-9-CM codes, in outpatient clinics or those who had a primary diagnosis of ACTDs during hospitalisation within 1 year and were older than 20 years. ACTD patients who had undergone RC repair surgery before 2004, had missing data or had died during the follow-up period were excluded from the study. Finally, 5,019 ACTD patients were enrolled into the study cohort (figure 1).

Flowchart showing the study design. LHID, Longitudinal Health Insurance Database; NHIRD, National Health Insurance Research Database.
Confounders and propensity score adjustment
In addition to the demographic variables of age and sex, economic status and comorbidities such as diabetes mellitus (ICD-9-CM codes 250 and 251), hypertension (ICD-9-CM codes 401–405), hyperlipidaemia (ICD-9-CM codes 272.0–272.4), coronary heart disease, gout, non-steroidal anti-inflammatory drugs (NSAIDs), steroid use (defined as 3 months of consecutive use) and fractures were analysed in this study. Regarding thyroid diseases and RC tear risk, we also analysed thyroid disorders as a morbidity.16 Furthermore, comorbidities were determined at the specific time point that the patients were enrolled into the study and not changed during the follow-up period. To minimise bias in data selection from the study database, we used propensity scores adjusted for comorbidities and income, as shown in table 1.
Demographic characteristics and comorbidities of autoimmune connective tissue disease (ACTD) patients and controls from 2004 to 2008
Outcome identification
We used the first RC repair surgery with the relevant application codes (64121B and 64122B) as the study endpoint from the same database. All participants were followed from the index date to the endpoint or until 31 December 2010, whichever was earlier, and the final-date observations were censored observations.
Statistical analysis
Demographic characteristics and comorbidities were analysed using Pearson’s χ2 test. We calculated the incidence of ACTDs and compared the risk of RC repair surgery between the two cohorts by using the Cox model after propensity score adjustment. Furthermore, we compared the risk of repair surgery in the ACTD patients who did or did not receive medication (NSAIDs and steroids) with that in the non-ACTD controls. To clarify the association between medication and RC tears, Kaplan–Meier hazard curves were plotted for RC tears in the ACTD patients who did or did not receive NSAIDs and the controls as well as in the ACTD patients who did or did not receive steroids and the controls for a 7-year follow-up period. All data analyses were performed using Stata (V. 11) and SAS (V. 9.1.3; SAS Institute, Cary, NC, USA). A value of p<0.05 was considered statistically significant.
Patient involvement
No patients were involved in developing the hypothesis, specific aimsor the research questions, nor were they involved in developing plans for the design or implementation of the study. No patients were involved in the interpretation of the study results or writing of the manuscript. No plans exist to disseminate the research results to the study participants or the relevant patient community.
Results
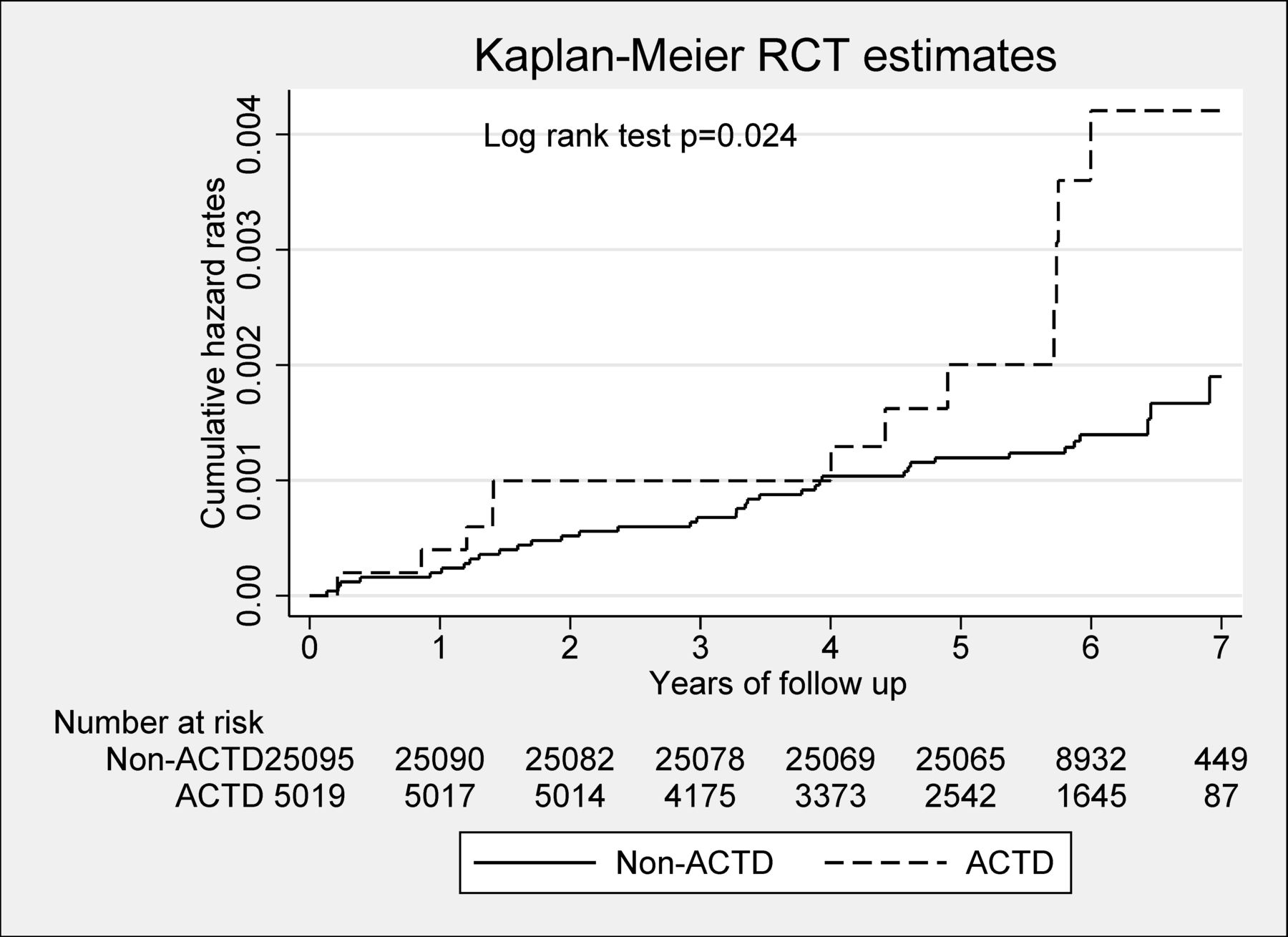
In total, 5019 ACTD patients were in the study cohort and 25 095 patients were in the control cohort. Women constituted 77.5% of each cohort and no statistical differences existed in age or sex. The prevalence of the comorbidities hyperlipidaemia (17.8%), coronary heart disease (13.2%), gout (12.1%) and thyroid disorders (8.3%) were higher in the ACTD cohort than in the control cohort (table 1). The incidence of RC repair surgery was 49.0 and 24.0 per 100 000 person-years in the ACTD and control cohorts, respectively. In the ACTD cohort, the crude HR of RC repair surgery was 2.08 (95% CI), 1.08 to 4.02, p<0.05), and the adjusted HR (aHR) was 1.97 (95% CI, 1.01 to 3.82, p<0.05) (table 2). Figure 2 presents the Kaplan–Meier hazard curves for the risk of RC repair surgery in the ACTD and control cohorts during the 7-year follow-up period. A comparison of the patients who did and did not use NSAIDs (separately) with the controls revealed that the ACTD patients with records of NSAID use had a higher risk of RC repair surgery (aHR=3.13, 95% CI, 1.21 to 8.07, p<0.05) than did the ACTD patients without records of NSAID use (table 3). Figure 3 presents the Kaplan–Meier hazard curves for the risk of RC repair surgery in the ACTD patients who used NSAIDs, the ACTD patients who did not use NSAIDs, and the controls during the 7-year follow-up period. Further analysis of the association between steroid use and the risk of RC repair surgery showed that the crude HR was 2.32 (95% CI, 1.03 to 5.22, p=0.042) among the ACTD patients who used steroids. However, the risk of RC surgery in the ACTD patients was not significantly higher than that in the controls in terms of aHR (aHR=2.22, 95% CI, 0.98 to 5.03, p=0.067) when using steroids (table 4). figure 4 represents the trend of the risk of RC repair surgery; the risk increased among the ACTD patients who used steroids, but it was not significant during the 7-year follow-up period.

Kaplan–Meier hazard curve for rotor cuff tears (RCTs) in patients with autoimmune connective tissue diseases (ACTD) and controls over a 7-year follow-up period.

Kaplan–Meier hazard curve for rotor cuff tears (RCTs) in patients with autoimmune connective tissue diseases (ACTD) with or without non-steroidal anti-inflammatory drug (NSAID) use and controls over a 7-year follow-up period.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier hazard curve for rotor cuff tears (RCTs) in patients with autoimmune connective tissue diseases (ACTD) with or without steroid use and controls over a 7-year follow-up period.
Crude and adjusted HRs for rotor cuff tear (RCT) between the autoimmune connective tissue disease (ACTD) and non-ACTD cohorts during the 7-year follow-up period, starting from the index date of an ambulatory care visit (n=30 114)
Crude and adjusted HRs for rotor cuff tear (RCT) in patients with autoimmune connective tissue diseases (ACTDs) with or without NSAID use and non-ACTD controls during the follow-up period, starting from the index date of an ambulatory care visit
Crude and adjusted HRs for rotor cuff tear (RCT) in patients with autoimmune connective tissue diseases (ACTDs) with or without steroid use and non-ACTD controls during the follow-up period, starting from the index date of an ambulatory care visit
Discussion
Although case reports have described spontaneous ruptures in the supraspinatus tendon, patellar tendon and hand flexor tendon,11–13 17 no relevant epidemiological study has investigated the risk of RC lesions among ACTD patients until now. In our population-based cohort study, the ACTD patients had a higher risk of RC repair surgery than the controls. This finding indicates that in addition to the joints, the periarticular soft tissue is affected in ACTDs. During the 7-year longitudinal follow-up period, the number of RC repair surgery events increased with disease progression. To improve quality of life of ACTD patients, prevent negative effects of RC injuries and develop an effective prevention strategy, identifying the possible mechanism of ACTD pathogenesis is crucial.
The factors involved in RC injury pathogenesis can typically be classified into extrinsic and intrinsic factors.18 For ACTD patients, we supposed that intrinsic pathogenic aetiologies play a crucial role in increasing the risk of RC injuries and the subsequent requirement of repair surgery. ACTD patients exhibit the characteristics of systemic inflammatory processes, and subsequently, inflammation reactions affect the RC tendon. Subclinical inflammation persists in these ACTD patients even after their clinical symptoms are under control. Subclinical chronic inflammation can disrupt the tendon healing and remodelling process, which can lead to weakening of the tendon, thereby increasing the risk of subsequent tendon rupture. Previous case reports have found perivascular mononuclear cell infiltration in the ruptured tendon, which was caused by the ACTD inflammatory process.19 20 The inflammatory phenomenon can also be detected using ultrasound techniques. A study reported that 49.4% of ultrasound abnormalities were tenosynovitis.21 In addition to tenosynovitis, ultrasound detected chronic tendinopathy, which led to degeneration of the tendon; the weakened structure was highly vulnerable to injuries. These intrinsic aetiologies of tendon inflammation and subsequent tendon degeneration can lead to a high risk of RC injuries and the subsequent requirement of repair surgery among ACTD patients.
ACTDs represent complicated chronic inflammatory autoimmune diseases with no curative treatment options. To arrest the progression of autoimmune diseases, systemic steroids are often used and combined with non-steroidal medication to control flare-up episodes.22 Corticosteroids can accelerate the progression of weakness by inhibiting collagen synthesis and impairing blood supply.23 Corticosteroids inhibit collagen synthesis and may also impair blood supply, thereby weakening the tendons.5 A critical zone near the insertion of the supraspinatus has been described using microangiographic evidence of an area of hypovascularity in the tendon close to its humeral insertion. Relative ischaemia in this zone is reported to mimic tendon degeneration.6 In addition, studies have mentioned that chronic synovitis, tenosynovitis and long-term steroid use can lead to degeneration, thereby increasing the vulnerability of the flexor tendon in ACTD patients.24 25 However, our study revealed that steroid use in all patients and controls did not significantly increase the risk of RC repair surgery. Relevant studies have shown that inflammatory changes occur at the site of tendon rupture; these changes have been observed in ACTD patients.19 26 Although steroids can lead to tendon degeneration, inflammatory processes can be arrested by steroid administration. We hypothesised that the net effect of steroid use can increase the risk of RC repair surgery; however, this effect was not significant in the ACTD patients. Furthermore, the ACTD-induced chronic inflammatory process and related degeneration can accelerate the weakening of RC with ageing.
Our study revealed that ACTDs are a risk factor for RC repair surgery. We hypothesised that the possible mechanism underlying this association was chronic inflammation and tendon degeneration, which damage and weaken the RC’s structure. The strength of this study is its large sample size and data analysis. Moreover, it is the first epidemiological study to investigate the association between ACTDs and the risk of RC lesions and surgery. Nevertheless, this study has several limitations that must be addressed. First, the diagnosis of ACTDs and comorbidities were defined using ICD codes from the database; hence, the accuracy should be examined. For accurate payments, the Bureau of NHI reviews medical records regularly. Patients with SLE, dermatomyositis and polymyositis in Taiwan can apply for catastrophic illness registration cards, and copayment is free for SLE-related medical problems. In addition to the accuracy of ACTD diagnosis, the definite onset duration of ACTDs could not be obtained from the database, and the diversity of follow-up periods for the study cohort must be addressed. Second, laboratory data of the inflammatory status and severity of ACTDs could not be obtained from the database. Moreover, the severity and status of ACTDs could not be categorised in the database and we could not identify which statuses of ACTD patients were at a high risk of tendon lesions. Furthermore, disease-modifying antirheumatic drugs (DMARDs), which could influence the severity of ACTDs, were not analysed because of the complexity of use from this database. Further studies on DMARDs’ effect on RC lesions are required to investigate separate diseases among ACTDs. Third, extrinsic factors affecting RC injuries include repeated impingement and overuse during work and daily living activities. These factors can increase the risk of repair surgery. However, data on work status, daily activities, body weight, alcohol consumption and smoking are not available in the database; although a large sample size was obtained, these confounders could not be excluded completely from this study. Finally, for higher accuracy, we only investigated the risk of RC lesions and requirement of subsequent repair surgery; therefore, patients with minor tears or those who did not require surgical intervention might have been missed. Despite the limited information available on the types of RC lesion, our population-based study provided crucial information on the high risk of RC surgery among ACTD patients.
Conclusion
The results of this 7-year longitudinal population-based retrospective cohort study showed that ACTD patients had a 1.97-fold higher risk of RC repair surgery than the controls. Additional studies on inflammation severity in ACTDs and the effects of ACTD-related medication on the risk of RC lesions are recommended.
References
Footnotes
Contributors SWH participated in the study design, conducted the data analysis, drafted the initial manuscript and approved the final manuscript as submitted. CLL conducted the data analysis, drafted the manuscript and approved the final manuscript as submitted. LFL contributed to the study design, reviewed and revised the manuscript, and approved the final manuscript as submitted. CCH reviewed and revised the manuscript and approved the final manuscript as submitted. T-HL participated in the study design, reviewed and revised the manuscript and approved the final manuscript as submitted. RE designed and conceptualised the study and approved the final manuscript as submitted. H-WL participated in the study design, conducted the data analysis, revised the manuscript and approved the final manuscript as submitted.
Funding This study was supported by the Taipei Medical University and Shuang Ho Hospital (107TMU-SHH-08). The funding sources played no role in the design, implementation, data analysis, interpretation, or reporting of the study.
Competing interests None declared.
Ethics approval Institutional Review Board of the University of Taipei (UT-IRB No: IRB-2018-07).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.
Patient consent for publication Not required.