Article Text

Abstract
Objectives This paper explores patient experiences and identifies barriers and opportunities for improving access to healthcare for patients from the Canadian north who travel to receive medical care in a Southern province.
Design A mixed-methods, cross-sectional study involved one-on-one interviews, focus group discussions and key informant interviews.
Participants 52 one-on-one interviews with Northwest Territories (NWT) patients and patient escorts and two focus group discussions (n=10). Fourteen key informant interviews were conducted with health workers, programme managers and staff of community organisations providing services for out-of-province patients. A Community Advisory Board guided the development of the questionnaires and interpretation of results.
Results Respondents were satisfied with the care received overall, but described unnecessary burdens and bureaucratic challenges throughout the travel process. Themes relating to access to healthcare included: plans and logistics for travel; level of communication between services; clarity around jurisdiction and responsibility for care; indirect costs of travel and direct costs of uninsured services; and having a patient escort or advocate available to assist with appointments and navigate the system. Three themes related to healthcare experiences included: cultural awareness, respect and caring, and medical translation. Respondents provided suggestions to improve access to care.
Conclusions Patients from NWT need more information and support before and during travel. Ensuring that medical travellers and escorts are prepared before departing, that healthcare providers engage in culturally appropriate communication and connecting travellers to support services on arrival have the potential to improve medical travel experiences.
- medical travel
- healthcare access
- healthcare services
- northern Canada
- patient experience
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
To our knowledge, this study is the first to explore the experience of medical travel from Northern Canada to an urban centre from the perspective of patients, patient escorts, healthcare providers, and support staff.
The mixed-methods design allowed the merging of data from different perspectives and findings will be of interest to other healthcare jurisdictions serving remote and isolated populations.
This study was able to document culturally relevant and patient-centred solutions to improve travel preparation and communication that would have a positive impact on patient experience and reduce healthcare costs.
The majority of respondents reported receiving outpatient, schedulable services and findings may not be generalisable to inpatients with acute or emergency care needs.
Further research is required to implement and test patient-led solutions, and to identify and address pretravel barriers to healthcare access.
Background
In Canada’s universal healthcare system, services are provided across a vast geography, in the context of decentralised management by provincial and territorial authorities, and based on principles of universality, comprehensiveness, portability, accessibility and public administration.1 For residents of rural and remote areas of Canada, the majority of primary care services are met close to home in communities and regional centres. Remote communities in Canada’s north are served through a nurse-based primary care model supported by periodic physician visits, and increasingly, telehealth services. However, certain health conditions require travel to more specialised services that are only available in larger centres, sometimes outside the province or territory. Only 3% of specialists live in rural or remote areas of Canada, where over 18% of the population resides.2
Out-of-province and out-of-territory medical travel in Canada comprises a small percentage of the total care provided, but it can be physically, financially and emotionally challenging for patients, families and communities, and it comes with a significant public sector cost.3 The government of Northwest Territories (NWT) provides medical travel benefits for NWT residents with a valid healthcare card, and administers the federally funded Non-Insured Health Benefits (NIHBs) Programme that covers registered First Nations and Inuit. NWT has the highest total health expenditure per capita in Canada.4 NWT relies on four main territorial healthcare facilities, with specialised diagnostic and treatment services accessed outside the territory in Alberta, Saskatchewan and British Columbia. In 2016–2017, the NWT Department of Health and Social Services (DHSS) spent US$32.5 million for residents to access medical services outside NWT, an increase compared with previous years, accounting for 7% of the total DHSS spending.5
The NWT DHSS released a revised medical travel policy in 2015 and accompanying guide in 2017.6 The medical travel policy covers return airfare, interfacility ambulance services for emergency medical evacuations, and some support for meals, accommodation and ground transportation. Under certain circumstances, NWT covers for a non-medical escort to travel with and assist the patient.6 7
Improving access to and experience with healthcare services has inherent value to health system users, and is associated with important clinical processes and outcomes,8 especially in relation to chronic disease prevention and management,9 10 adherence to medical advice11 and treatment plans.12 Recently, attention related to delivering better preventive and primary care close to home,13 medical travel for pregnancy14 and postnatal services,15 and reducing the cost of medical travel16 has increased, but with little focus on the experience of interprovince/territory medical travel.
This research aimed to identify barriers to accessing quality healthcare for medical travellers and potential opportunities for improving care. We applied a mixed-methods research design, sequentially merging quantitative information from medical travellers and escorts from NWT, with qualitative analysis of travel experiences, and key informant interviews with front-line health workers, programme managers and staff of community organisations providing services for out-of-province patients.
Methods
Setting
This study took place in Edmonton, the provincial capital of Alberta, and closest major urban centre to NWT, with a population of 1 million people. Medical travellers are provided accommodation in a boarding facility and transportation to local medical appointments. If patient volume is high, accommodation is provided at local motels.
Study design
Through the mixed-methods design, we collected data in different ways.17 Integrating qualitative and quantitative findings identified themes of access to and experiences with health services and potential solutions. The qualitative key informant interviews were conducted during August to September 2017 and informed the development of the questionnaire administered with medical travellers. Questionnaires were reviewed by the Community Advisory Board, and pilot tested before use. Focus group discussions with medical travellers and escorts provided additional context for the one-on-one interview data. Across all sources, more weight was placed on the open-ended narratives provided by participants. Interviews and focus group discussions were conducted during November to December 2017.
Data collection
MO, a female community liaison, and KK a female PhD student, conducted all key informant interviews. SLJ, SA, SL, all female research assistants, with KK and MO conducted one-on-one interviews. All data collectors received training specifically for this project. The study aims and objectives were explained to participants by the data collector prior to commencing. The interviewers did not have an ongoing relationship with the participants, but all members of the data collection team spent significant time with staff and residents at the boarding facility building trust, sharing daytime and evening meals, playing games, crafting and sharing information about the potential outcomes of the project.
Key informant interviews
Front-line health workers, programme managers and staff of community organisations providing services for out-of-province patients were purposively sampled, with a snowball sampling strategy until saturation was reached after 14 interviews. Two female interviewers trained in study procedures conducted the interviews in private offices. Data collection consisted of face-to-face, semistructured interviews 30–60 min in length. Interviews were audio recorded and later transcribed.
One-on-one interviews
Medical travellers and non-medical escorts residing at the boarding facility were invited to participate. Individuals who were residents of NWT and had attended at least one medical appointment in Edmonton were eligible. The sample size was based on the number of medical travellers from NWT in a 1-month period, accounting for an 80% response rate. In total, 43 patients and nine escorts participated. The interviewer-administered questionnaire consisted of sociodemographic characteristics, self-reported health status and experiences with the health system and medical travel. The interviewer transcribed open-ended responses verbatim. Patient escorts were invited to participate if the patient was unavailable. Escorts responded to questions relating to travel and experience, but did not provide information related to specific health concerns of the patient. Interviews were conducted in private offices or unoccupied meeting rooms and took between 22 and 71 min to complete.
Focus group discussions
Ten patients and escorts explored issues in more detail in two semistructured focus group discussions, advertised locally through word of mouth and posters. The discussions took place in the evening in a residence common area, and were approximately 60 min in length. One team member facilitated the discussion and one took field notes. Discussions were audio recorded and later transcribed.
Data analysis
Data were entered on a tablet using an online questionnaire developed with REDCap V.8.1.1.18 Quantitative data were analysed using Stata V.14.19 KK and SA transcribed audio files. Transcripts were analysed using NVivo Pro V.12 to code and categorise the data using conventional content analysis.20 In the analysis, access was defined as the ability of people to obtain appropriate healthcare resources to preserve or improve health.21 Experience with health services and healthcare providers was defined as the range of interactions between individuals and the healthcare system, including care provided by doctors, nurses and auxiliary staff.
Patient and public involvement
This research was part of a 4-year mixed-methods implementation research study on access to health services called Caring and Responding in Edmonton: The CARE Project. The inclusion of the experience of medical travellers came at the request of community partners and government of the NWT. A 60+ member Community Advisory Board, including representatives from NWT and staff involved in medical travel, helped guide the development of the questionnaires, interpretation and dissemination of results. Results were presented to the Community Advisory Board in May 2018, in a specific Northern gathering in November 2018, and in NWT in January 2019. Engagement is ongoing with medical travellers and healthcare providers to improve patient navigation, communication and experience through the intervention phase of The CARE Project.
Respondents were informed about the purpose of the study and provided written informed consent prior to participation.
Results
Background characteristics and details of medical travel
Table 1 summarises background characteristics of respondents. The shortest direct distance travelled to Edmonton was 725 km, and the furthest was 2030 km as the crow flies, with much greater actual travel distance. Figure 1 and box 1 illustrate the medical travel journey.
Example of a non-emergency medical travel journey
In remote Northern communities, the development and preservation of local skills and knowledge provide strength and resiliency. Connecting with land, culture and traditions is an important component of health and wellness in Northwest Territories (NWT) and beyond. However, when more complex health needs arise, residents may have to leave home for care.
There is no ‘typical’ medical travel journey. For the most medical travel, residents will need to see the visiting healthcare provider first, and some communities only have access to a doctor for three or four days every five weeks, resulting in potentially lengthy wait times. When a doctor refers a patient for travel, the patient is sent to the nearest regional centre, such as Inuvik or Yellowknife. Flight schedules vary, and most communities are not serviced by daily flights.
The logistics of Arctic air travel are complex and conditions can include blowing snow, extreme wind and whiteout. Special equipment and training is required for aircraft and crew and for patient care, and there is a significant risk of weather delays all year round. This means that a single short appointment could result in a week away from home. Following regional travel, and depending on the severity of the health concern and the treatment needed, the patient may end up being referred to a facility located thousands of kilometres south.
The cost of accommodation, food, most medical and travel costs are covered by the government of NWT or the federal government, and supplementary health insurance programmes. However, medical travellers can be out of pocket for incidental costs, and may have to pay up front for prescription drugs.
A non-medical escort may accompany the patient, but frequently, adult patients travel alone. Regular frustrations of travel such as flight delays or scheduling changes, lost luggage, unfamiliar signage and adjusting to new accommodation, can become overwhelming during medical travel. The steps depicted are not uncommon, with one individual needing to travel over 5000 km for a single health concern, resulting in weeks away from home.

A medical travel journey.
Self-reported characteristics of study participants, n=52
People from the most remote communities experienced increased burdens, and mobility or illness made the journey more challenging.
Some people are on oxygen or in a wheelchair…You spent two days traveling and you are here for a half hour appointment. Then sometimes…it could take them a few days to get home because of weather. And then it’s supposed to be one night in Yellowknife and it ends up being five or six. (key informant, 603)
The average stay in Edmonton was nine days, and 77% of respondents were first-time visitors to the boarding facility. Nineteen per cent had been staying for over two weeks, with 75 days being the longest stay. The majority of respondents were satisfied with the care received (figure 2). The single biggest challenge reported was making arrangements for children, pets and other household responsibilities while away (figure 3). This was particularly true for patients without definitive return dates. One respondent described: ‘The last time we were here, we didn't know that we’d be here for two months’ (medical traveler, 3522).

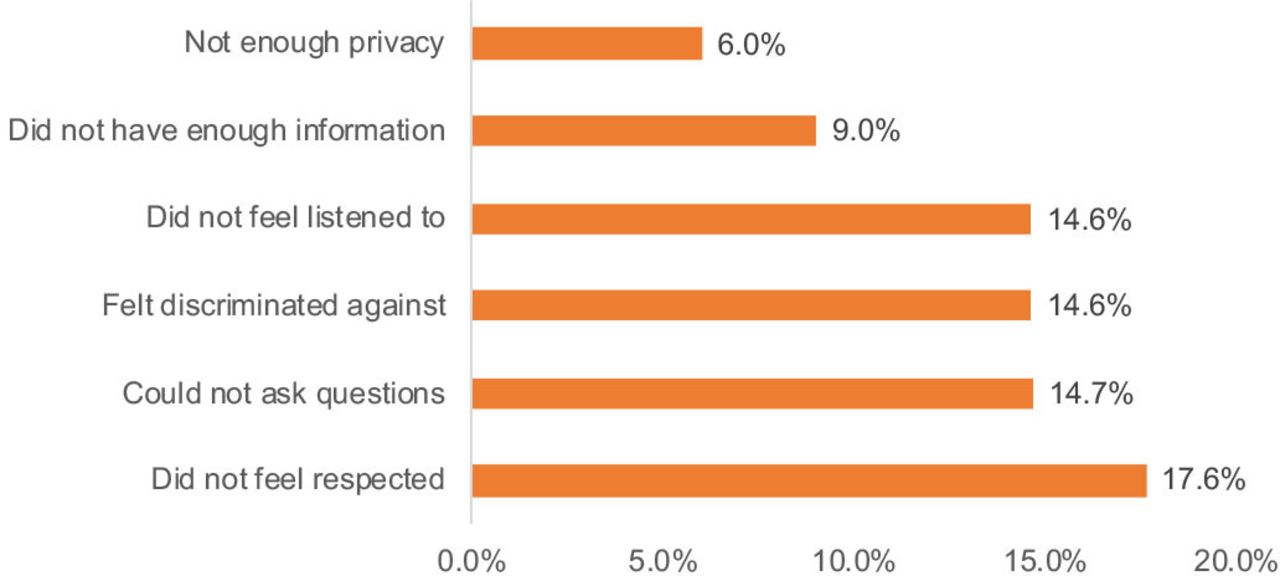
Satisfaction with most recent healthcare visit.

{kind=link}
{kind=link}
{kind=link}
The main difficulty related to medical travel.
Respondents described the impact of delays between obtaining approval and receiving care: ‘By the time [the patient] found out that he had cancer, it had metastasised already. Medical information took forever to reach us’ (patient escort, 3524). The perceived consequences of not being proactive were severe: ‘You really have to be up on your care. As some of my friends who did not push, now they are dead’ (medical traveler, 3527).
Factors influencing access to care
Five main themes were derived from the data (table 2): (1) medical travel logistics, (2) level of communication between services, (3) clarity around jurisdiction and responsibility for care, (4) cost of services and (5) having an escort or advocate.
Themes arising from interviews with key informants, medical travellers, patient escorts, and focus group discussions
Medical travel logistics
Of respondents who reported difficulties, 5.0% identified that travel to an unfamiliar city was the most challenging. The city’s size and range of services was described as overwhelming, especially in comparison to Northern communities. The ability to navigate complicated logistics had an impact on access to care. Respondents noticed limited information provided before travel, and unclear process of determining itineraries. As one traveller explained, ‘[Before travel we need] more information, more understanding. Give information to patients in plain, understandable words’ (medical traveler, 5502).
Communication between services
Limited communication between various levels of care and from decision makers could impact care. Respondents noted that healthcare providers in Edmonton are not always aware of the care that is available in the patients’ home communities. Continuity of care is a challenge given that remote and isolated communities rely on visiting healthcare providers from Southern centres, and there is a high turnover among providers.
Jurisdiction and responsibility for care
Reciprocal billing and aligning policies and procedures in the different health jurisdictions were described as recurrent obstacles. Medical travellers and non-clinical programme staff were unclear about what services were covered, and what to do when patients were turned away. Refusing or delaying services to patients that did not have an Alberta health insurance number was reported by travellers and patient escorts. The process of getting proof of NIHB Programme benefits was frequently noted as a challenge.
Direct and indirect costs
While some respondents appreciated the range of costs associated with medical travel that were covered, and around two-thirds of respondents had access to supplemental health coverage, 23% identified access to funds as a barrier in accessing needed care, and one-third of them cited lack of coverage for medications as the main gap.
Non-medical escorts and facilitated appointments
Having a companion to attend appointments and act as a support and advocate, particularly someone who is familiar with the patient’s home community and Edmonton was reported to increase access and positive care experiences. While navigator services exist at larger facilities, few local programmes are specific to Northern Indigenous cultures, and not all respondents were aware of these services.
Factors influencing the experience of care
Three themes affecting experience with healthcare providers and related solutions emerged from the data (table 2): (1) cultural safety and awareness, (2) respect and caring and, (3) medical translation.
Cultural safety and awareness
Respondents described the benefit of welcoming and safe healthcare environments that provide high-quality, trauma-informed and culturally appropriate care. Healthcare providers and staff that exhibited cultural competence were described as providing better support to patients. Respondents shared past experiences of discrimination towards Indigenous patients and expressed concern about a lack of understanding in the healthcare system about the cultural and historical context of different communities. To increase empathy related to medical travel, one respondent suggested, ‘taking health providers through what it must be like to come to a new place, [with] traffic lights, and people, and noise, and trees’ (key informant, 605).
Respect and caring
Especially for people travelling alone, or facing traumatic circumstances, respondents described how providers could offer extra respect and caring for patients who are far from home. One respondent recounted the story of a young woman who had an emergency evacuation from a small community during a high-risk pregnancy. She travelled with nothing and could not get a bag of her own things sent down; thus, she relied on donations of toiletries and clothing.
Medical translation
Communicating medical information with providers was mentioned as a challenge for numerous respondents, especially for the 17% whose primary language was not English. Respondents described some benefits and drawbacks of professional translator services compared with having an escort in the appointment.
Discussion
In this study, medical travellers, escorts and support workers were interviewed in the context of a larger project on improving access to healthcare for underserved populations. While Canada’s population distribution is unique, jurisdictions within Australia, USA, Norway, Finland and Greenland have similar geographies that depend on medical travel from remote and isolated communities, and present opportunities for learning. In this population, effective and transparent travel preparation, efficient communication across all phases of care and cultural knowledge were found to be central to ensuring both access to care and a positive patient experience.
Many medical travellers reported satisfaction with the care received, while also reporting significant stress involved with managing travel logistics across different health jurisdictions. With direct flights from only one NWT community, the first leg involves travelling to the nearest larger centre in NWT, which can add a day or more to the trip, with no designated facility or support for infirm travellers. This ‘multilocality’ of individuals moving between home and distant care facilities can become a long-term feature of people’s lives,22 creating disruptions to personal, family, community and cultural obligations.14
Medical travel can create additional challenges for an already vulnerable person in a health crisis. Almost all NWT residents are required to travel to access advanced medical care at some point.23 Such travel is further complicated by complex policies affecting healthcare delivery for Indigenous populations.23 Detailed policies surrounding medical travel and NIHB aim towards standardisation, but are not applied uniformly. This may reduce the ability to respond to shifting patient needs in dynamic situations, such as long-distance travel during a period of illness or injury.22 Access to information and communication across jurisdictions were particular areas of concern. Electronic health records between NWT and Alberta have allowed for more efficient sharing of patient information, but barriers to full utilisation of the system exist and important medical information does not always travel with patients to other jurisdictions.24 25 Medical travellers paid out-of-pocket for incidentals and some prescriptions and procedures, and some could not access social assistance benefits or bank accounts away from home. Interjurisdiction coordination has been a long-standing challenge, with negative consequences for health outcomes.22
Patient escorts were described as an important source of support and advocacy. Family members can support decision-making and adherence to treatment plans,23 but are not always the best escorts.26 Even with changes to the patient escort policy,22 26 respondents echoed that challenges still exist, such as unreliable escorts and inconsistent policy application. For patients alone, a local trained navigator or advocate could help with medical communication, providing emotional and cultural support.27 Communication predeparture and during the course of travel and treatment should use different formats and media to reach a larger audience with targeted information.
Participants called for more culturally appropriate care and cultural knowledge within the healthcare system. Challenges with cross-cultural health communication and health literacy can be particularly harmful.23 28 29 Respondents described the care and support provided by an Indigenous clinic, cultural helpers and a local Northern support unit staffed by healthcare professionals with experience living in remote settings, as extremely valuable. However, not all travellers were aware of or able to connect to services and resources. Recently, culturally relevant services have been shown to improve the experience of Indigenous patients requiring medical relocation for dialysis in South Australia,30 and have been identified as especially important for palliative care and cancer services provided away from home in Northern Territory, Australia.31 32
Respondents described the impact of negative healthcare experiences, including not feeling listened to or respected or discriminated against, on health-seeking behaviours. The unequal patient–provider power dynamic in healthcare, particularly within a colonialist historical context, is well described.33–35 Relying on patients to advocate for their health and needed services, underestimates the complex power relationships involved. Eight of the 94 summary recommendations arising from Canada’s Truth and Reconciliation Commission specifically pertain to health.36 Greater understanding of how residential schools, forced relocation and systemic discrimination have shaped Northern communities in Canada, and how to use that knowledge to change healthcare service delivery is still needed.
The barriers to medical travel can be overwhelming, leading to delays in receiving care, or an avoidance of care-seeking altogether,37 resulting in poorer outcomes and higher costs for aggravated health conditions.38 One study of medical travel in Arctic regions of Nordic countries estimated that the number of service hours per Northern patient is 2–3 times higher than urban populations.39 Continuity of care remains a challenge in the North; with only 31.1% of Indigenous territorial residents seeing a regular doctor, compared with 76.4% of Indigenous people outside the territories.40 One systematic review of the impact of distance to healthcare services on health outcomes in Northern settings found worse health outcomes among patients living further away from healthcare facilities and concluded that distance should be a consideration in discussions of treatment options.37
To our knowledge, this study is the first to explore the experience of medical travel from the perspective of outpatients, escorts, providers and support staff in an urban centre in Canada. The mixed-methods design allowed the merging of rich data from multiple different perspectives. One limitation of this study is the measurement of patient experience during the medical travel process, and not in the home community following the medical travel journey, which may have provided additional insight into continuity of care. Additionally, while patient travel escorts provided some context for hospitalised patients, respondents were mainly individuals receiving outpatient services, and the study findings may not be generalisable to inpatients with greater acute care needs. Finally, this study conducted interviews at the point of care and did not include individuals living in remote and isolated communities who were not able to get the required appointments, referrals or the paperwork to travel. Given the potential for delayed or deferred care-seeking, further research is needed to assess the barriers to healthcare access among Northern residents who are not able to access medical travel.
The experience of patients travelling a long distance for an extended period away from home is important to understand in order to provide quality care within Canadian provincial health systems, and will be relevant for other jurisdictions serving remote and isolated communities. The majority of medical travellers from NWT were satisfied with the care received. However, many also encountered serious challenges with medical travel, including significant delays in accessing and receiving care. Patients outside of their home jurisdiction are a unique and potentially vulnerable population that could benefit from increased access to and continuity of care. Healthcare providers and policy-makers may not be aware of the complexity of the medical travel experience and the stress involved with managing travel logistics across different health jurisdictions. More effective and transparent travel preparation and efficient communication across jurisdictions and with patients could help to improve the experience of medical travel for residents of the far north.
Acknowledgments
We are grateful to Larga for providing space for interviews. We thank all of the participants who graciously shared their insight and perspectives. We acknowledge the contribution of The CARE Project Community Advisory Board members who provided insightful feedback on the study design and interpretation of results. We would like to thank the Government of Northwest Territories, Alberta Health Services and the Hotıì ts’eeda SPOR SUPPORT (Support for People and Patient-Oriented Research and Trials) Unit for their ongoing partnership.
References
Footnotes
Contributors SS, FK and KK conceptualised the study, analysed and interpreted the data. SS, FK, KK, MO, SL, SLJ, SA, ML, MO, MQ, SI-F, CM, SB, DD, and AC contributed to the writing and review of the manuscript and interpretation of results. All authors approved the final manuscript. Each author has reviewed and approved the contents of the submitted manuscript for publication.
Funding This work was supported by the Royal Alexandra Hospital Foundation.
Disclaimer The funder had no role in the study design, nor in the collection, analysis, and interpretation of data, nor the writing of the manuscript, nor in the decision to submit the article for publication. The researchers confirm independence from funders and that all authors, external and internal, had full access to all of the data and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval University of Alberta’s Human Research Ethics Board, and the Northern Alberta Clinical Trials and Research Centre granted ethical approval (PR00069624).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.