Article Text

Abstract
Objectives Patient experience is being widely considered in the evaluation of healthcare service quality, which is a key target for public hospitals under China’s New Healthcare Reform. This study aimed to illustrate patients’ experiences in county-level public hospitals, and identify aspects that need to be improved.
Setting and participants Between 2016 and 2018, a cross-sectional study with 500 outpatients and 800 inpatients was conducted in 10 county-level public hospitals from Shandong Province, Hubei Province and Chongqing Municipality.
Method A three-part questionnaire was used to evaluate patients’ experiences during their visits to hospitals. It comprised a questionnaire for basic information, the Picker Patient Experience (PPE-15) Questionnaire and the overall evaluation (a 3-point Likert scale to express patients’ satisfaction and patient loyalty). Patients’ experiences were classified according to six dimensions (information transmission and patient education, respect for patient preference, emotional support, physical comfort, involvement of family or friends and continuity of medical service). Both univariate and multivariate analyses were performed to evaluate patient experience.
Results A total of 1241 valid questionnaires were analysed. The mean PPE-15 score was 41.33 (range, 23–56). The better the patient experience and satisfaction, the higher the patient loyalty (p<0.001). Except for hospital disparities, patients’ age and occupation status had a significant impact on patient experience (p<0.05). Of the six dimensions, the physical comfort score was the highest, while the respect for patient preference score was the lowest. Additionally, a strong correlation was found between the respect for patient preference dimension and patients’ overall satisfaction with their treatment experience.
Conclusions Hospital managers and staff members should pay close attention to the preferences of patients and their families to improve patient experience.
- health services management
- health service safety
- quality in health care
- patient experiences
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The Picker Patients Experience Questionnaire was first used to reflect patients experience during visiting time in China’s county-level hospitals.
This was a cross-sectional study comprising a large sample size of 1300 patients from three different provinces.
The experiences of both inpatients and outpatients were evaluated with the same mature scale without considering the visit type.
Both unitary analysis and multivariate analysis were used to examine the present status and obtain a better understanding of patients’ negative experiences in China’s county-level hospitals.
As this is a real-time survey, the findings may not reflect the changes in patients’ experiences.
Introduction
Healthcare service quality is the essence of hospital development and a key factor influencing patient loyalty.1–3 Traditionally, from a healthcare supplier’s perspective, professional service skills and advanced technology were regarded as key factors to improve healthcare service quality.4 However, from a healthcare user’s perspective, one important and obvious factor influencing patients’ choice of hospital is their experience or thoughts when receiving medical services,1 5 6 including the opportunity to express any concern, anxiety, fear or pain that they may experience.7
Patients are the receivers of healthcare services, and patients’ experiences are one of the most common indicators used to evaluate the quality of healthcare services.2 6 8–10 As an integral component of healthcare quality, patient experience includes several aspects of healthcare delivery that patients value highly when they seek and receive care; for example, timely appointments, easy access to information and good communication with healthcare providers.1 11 12 Regardless of the development of medications and technology, patient experience of illness and medical care is always at the heart of clinical services.2 13–15 Among the various aspects of patient experience, one can assess the extent to which patients receive care that is respectful of and responsive to individual patient preferences, needs and values.1 16 17 Patient experience and patient satisfaction appear to be synonymous but are entirely different.8 12 Patient satisfaction surveys tend to ask patients subjective questions about their satisfaction with their care (eg, outcome measure: satisfaction with health status following treatment),8 9 18 while patient experience evaluations focus on patients’ actual objective experiences during their visit to healthcare institutions and aim to avoid value judgements that influence existing expectations.1 19 20
County-level hospitals play an important role in providing basic healthcare in China.21 Accounting for 94% of the geographical area, counties are the most important and fundamental administrative units in China.22 Over 900 million residents live in the county area, comprising 60% of the population. County-level hospitals are the main providers of health services in rural areas.22 23 Based on the functional orientation of the three-tiered healthcare system, tertiary general hospitals are the topmost healthcare service providers in China, whereas county-level hospitals are the main providers of secondary care, providing comprehensive medical services for rural residents, who normally present with common diseases. A total of 13 640 typical county-level hospitals with a capacity of 2.33 million beds and 2.40 million healthcare workers are mainly responsible for healthcare delivery in rural areas.23 Compared with urban tertiary hospitals with highly qualified medical staff and high-quality facilities, county-level hospitals are associated with limited health resources, leading the public to distrust their healthcare quality. A comprehensive reform of county-level hospitals focusing on quality improvement initiated by the state council was launched in pilot counties from 2011 to 2015 and in all counties thereafter. With a great financial subsidy,24 county hospitals have demonstrated a tremendous improvement in the quantity and quality of healthcare service delivery after the reform (online supplementary appendix Ⅰ).
Supplemental material
As a slogan and target of the national ‘Further Improvement of Healthcare Services’ action plan, understanding patient experience is a key step in moving towards patient-centred care, which has been widely advocated at home and abroad.7 11 24 25 At the same time, as a guidance on orderly medical service in the new healthcare reform, the development of a hierarchical medical system aimed to treat 90% of diseases in county-level hospitals.26 27 Moreover, when implementing the project of hierarchical diagnosis and treatment, the most important issue in improving the quantity of healthcare services in county-level hospitals is to increase the trust and loyalty of rural citizens. A great amount of work has been conducted to evaluate the reform effects, such as operating efficiency evaluation, assessment of diagnosis and treatment level and calculation and prediction of hospital scale.28–30 Meanwhile, most patient experience studies have focused on urban tertiary hospitals,4 17 and established scales and self-developed questionnaires have both been used after verifying its validity and reliability to evaluate patient satisfaction and experience.31 32 However, reports on patients’ experiences using international scales in county-level hospitals are lacking17 21 ; thus, performing a horizontal comparison of patient experience with other areas is difficult. Moreover, the lack of uniform standards could hinder the improvement of patient experience in rural patient-centred healthcare systems in China.
Patient experience during hospital visits is an effective indicator that can directly reflect the progress and results of the comprehensive reform of county-level hospitals.1 3 20 To better understand the improvement of healthcare service quality in county-level hospitals, the present study aimed to analyse the current situation of patient experience in these hospitals focusing on the whole visit process, and to identify the main problems affecting patient experience.
Method
Study design and setting
A multicentre, cross-sectional, questionnaire-based survey was conducted from August 2016 to March 2018 with patients in 10 county-level public hospitals from different areas to evaluate patient experience. Data were obtained from the patient questionnaires and official statistical reports.
Under the proposal of China Statistical Bureau, all provinces were divided into three areas, namely eastern, central and western, based on their economic development and geographical position at the time of the study. Data from the special administrative regions and Taiwan Province were excluded from this study. The eastern area refers to developed areas,22 including 11 provinces or municipalities (ie, Beijing, Tianjin, Hebei, Liaoning, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong, Guangdong and Hainan). The central area refers to developing areas, including eight provinces (ie, Shanxi, Jilin, Heilongjiang, Anhui, Jiangxi, Henan, Hubei and Hunan). The western area refers to underdeveloped areas, including 11 provinces or autonomous regions (ie, Chongqing, Sichuan, Guizhou, Yunnan, Tibet, Shaanxi, Gansu, Inner Mongolia, Ningxia, Qinghai and Xinjiang). A pilot study was conducted in a county-level hospital in Hubei Province to ensure that the questionnaire was intuitive, understandable and flexible. Subsequently, the main field research was conducted by randomly selecting one province from the different areas: Shandong Province (Eastern China), Hubei Province (Central China) and Chongqing Municipality (Western China). Three counties from each of the three provinces were then chosen by convenience sampling. In each county, the public hospital with the largest healthcare delivery system was selected, and the questionnaire-based investigation of patients was conducted.
Participant selection and procedure
A total of 1300 patients (50 outpatients and 80 inpatients per hospital) who visited the county-level hospitals from 2016 to 2018 were recruited into the study (online supplementary appendix II). Online supplementary appendix Ⅲ provides the sample size formula.
The inclusion criteria were as follows: (a) patients over 18 years of age; (b) received treatment at the department of internal medicine, gynaecology or surgery; (c) able to understand the questions and provide clear responses; and (d) having already received the medical service.
The two exclusion criteria were (a) not completing the questionnaire; and (b) more than 20% missing information in the questionnaire. The effective sample size and selection is provided in online supplementary appendix Ⅳ.
A convenience sampling method was used to select interviewees for the patient questionnaire. Two teams, each with two interviewers conducted the survey in the outpatient and inpatient department, respectively. To avoid influencing the medical service process and the intervention of the medical staff, all interviews were conducted after the patients received treatment. The interviewers randomly selected patients that they encountered and assessed the inclusion criteria, and ended the survey when the number of interviewees met the required sample size (80 inpatients/50 outpatients). The present study excluded some participants during the analysis process because of missing information. Participants’ concerns, such as privacy protection, refusal to answer and responsibility to answer questions based on their true experiences were explained in both oral and written form. All participants provided verbal consent for their information to be used. Trained team members from our college who had professional interviewing skills conducted the investigation in each province to ensure quality control and reliability of the data.
The patient experience questionnaire
The Picker Patient Experience (PPE) Questionnaire is a valid and reliable tool assessing inpatient experience that has been used to evaluate hospital service quality in many countries.7 13 14 33 34 The present study used the PPE-15, which is a short version and is considered to represent a universal set of items applicable for most patients.33 After an expert consultation and two rounds of group discussions, we used the PPE-15 Questionnaire to assess both inpatient and outpatient experience and to compare the different service types. The PPE-15 Questionnaire was translated into Chinese based on Brislin’s translation model.35 Orthogonal translation, synthesis, back translation, and group discussions were performed by one professor and four students with extensive experience in medical service research and proficient English translation skills (online supplementary appendix Ⅴ).
Overall satisfaction and patient loyalty (ie, possibility of revisiting) were also assessed for comparison with other studies conducted in China. Patient satisfaction directly reflects the thoughts and the pleasure level of patients regarding the healthcare service, whereas the possibility of revisiting the hospital indicates patients’ loyalty and trust toward the hospital.
Overall, the questionnaire survey contained 25 items divided in to three parts: basic information of patients (gender, age, education level, marital status, occupation status, basic health insurance type and service type), specific aspects of patient experience (PPE-15) and overall evaluation. The PPE-15 comprised 15 items divided into six dimensions (S1: information transmission and patient education, S2: respect for patient preference, S3: emotional support, S4: physical comfort, S5: involvement of family or friends and S6: continuity of medical service). The third part contained the overall evaluation of visit satisfaction and patient loyalty (ie, possibility of revisiting). Both the PPE-15 and overall evaluation mainly included closed questions and used a 3/4-point Likert scale (eg, graded as 1–4 corresponding to ‘often’, ‘sometimes’, ‘never’ and ‘I don’t need to ask’, respectively). The higher the score, the better the patient experience (online supplementary appendix Ⅵ).7 13 25
Patient and public involvement
Health is a basic human right, and people seek help from medical staff not only for themselves but also for their family or friends, which means that not only patients but other individuals also have their opinions and experiences regarding hospitals. Patients and public were involved in the questionnaire translation stage of the study to make the questionnaire easy to understand. Meanwhile, five volunteers who had hospital visiting experience and three hospital managers helped in designing the questionnaire and training the investigators. After translation of the original questionnaire to Chinese, a pilot study with 100 patients was conducted in a county-level hospital in Hubei Province. Patients with different diseases, educational backgrounds, occupations and visit experiences were involved in the pilot study after providing verbal consent. The patient experience questionnaire was disseminated to all research partners, managers at sample hospitals and anyone interested in patient experience. All evaluation results were shared with relevant hospitals as evidence of feedback for the improvement of healthcare service quality.
Statistical analysis
EpiData3.0 (The EpiData Association, Odense, Denmark) was used for data entry and SPSS V.13.0 was used for statistical analysis. All of the data from the pilot study hospital and nine formal survey hospitals were analysed. The content validity index (CVI) was used to determine content validity, while Cronbach’s α and Kaiser-Meyer-Olkin (KMO) were used to verify the reliability of the questionnaires. Univariate and bivariate statistical models were adopted to evaluate the data. Continuous variables (age, evaluation scores) were described using mean and SD. Categorical variables (gender, age group, education level, marital status, occupation status, basic health insurance type, service type and problems identified in each item of PPE-15) were reported as counts and percentages. The six dimensions of the PPE-15 scale were specified as six separate criterion variables. Furthermore, the t-test, analysis of variance (ANOVA) test and Student-Newman-Keuls test were used to compare mean scores of patient experiences of different subgroups. The gamma grade correlation coefficient was used to analyse the association between patient experience items (the independent variables) and overall evaluation (the dependent variable). Demographic and other basic information were analysed using Pearson correlation analysis and multiple regression analysis to determine the factors affecting patient experience during visiting time: the dependent variable of linear regression analysis was PPE-15 score, while the dependent variable of the order regression analysis was overall satisfaction. Statistical significance was set at p<0.05 for a two-sided test.
Ethical considerations
Personal identifying information was removed and participants remained anonymous during the entire study process (online supplementary appendix Ⅶ). All the paper questionnaires and electronic data were maintained by the research team.
Results
Sample
The CVI for the questionnaire was 0.9 and the item-CVI was (0.85, 1.00), while the validity test results of the questionnaire’s reliability (Cronbach’s α=0.82, KMO=0.77) showed good internal consistency, and the correlation coefficient test (p<0.001) showed good structural validity among different dimensions and the overall score.
A total of 1241 questionnaires were analysed (effective response rate of 95.46%, online supplementary appendix Ⅳ). Among all participants, 54% were women and their mean age was 43.54 years; 55% of patients were employed, while 51.7% were covered by the New Rural Cooperative Medical System. Those aged 25–44 years accounted for 43.7% of the study population (table 1).
Participants’ demographic information and PPE-15 scores
Patient experiences evaluation
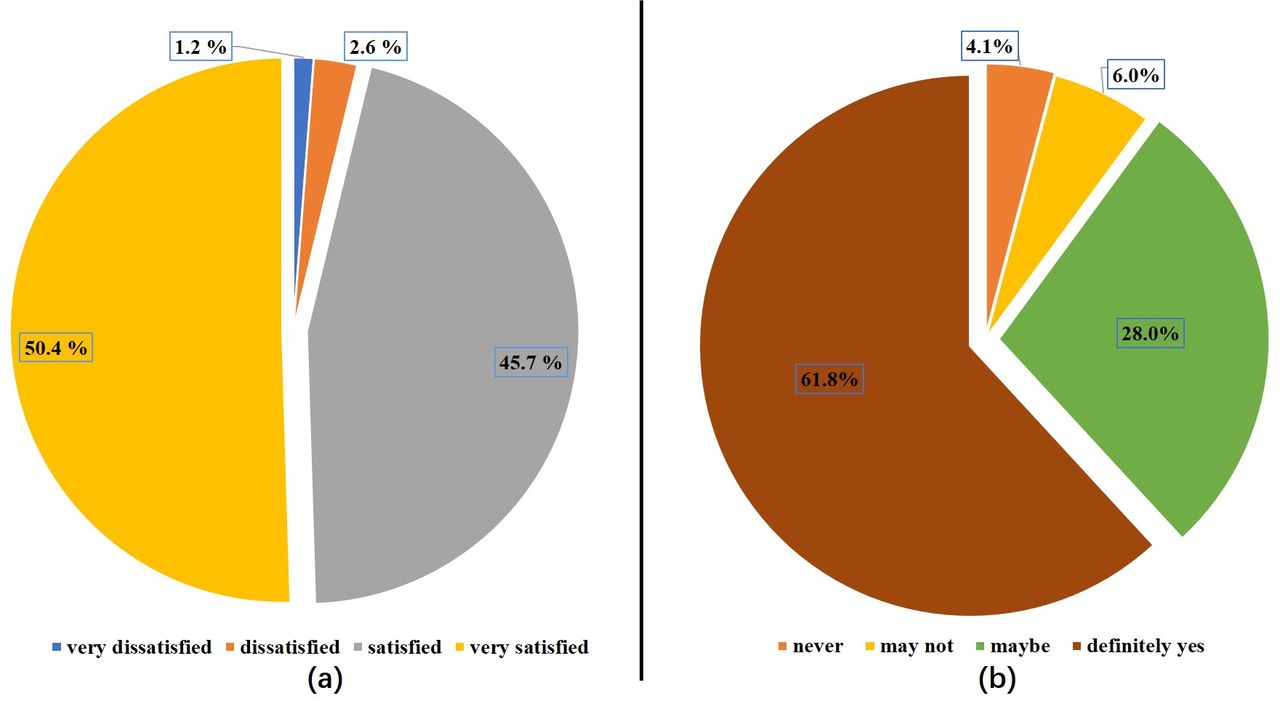
The maximum and minimum PPE-15 scores were 56 and 15, respectively. The mean PPE-15 score was 41.33±4.749 (range, 23 to 56); a total of 626 (50.4%) patients thought that they received a very satisfactory healthcare service. Meanwhile, 767 (61.8%) patients provided a positive answer to the possibility of choosing the same hospital again if they have other healthcare demands (table 2, figure 1).
Scores of patient experience in sample hospitals
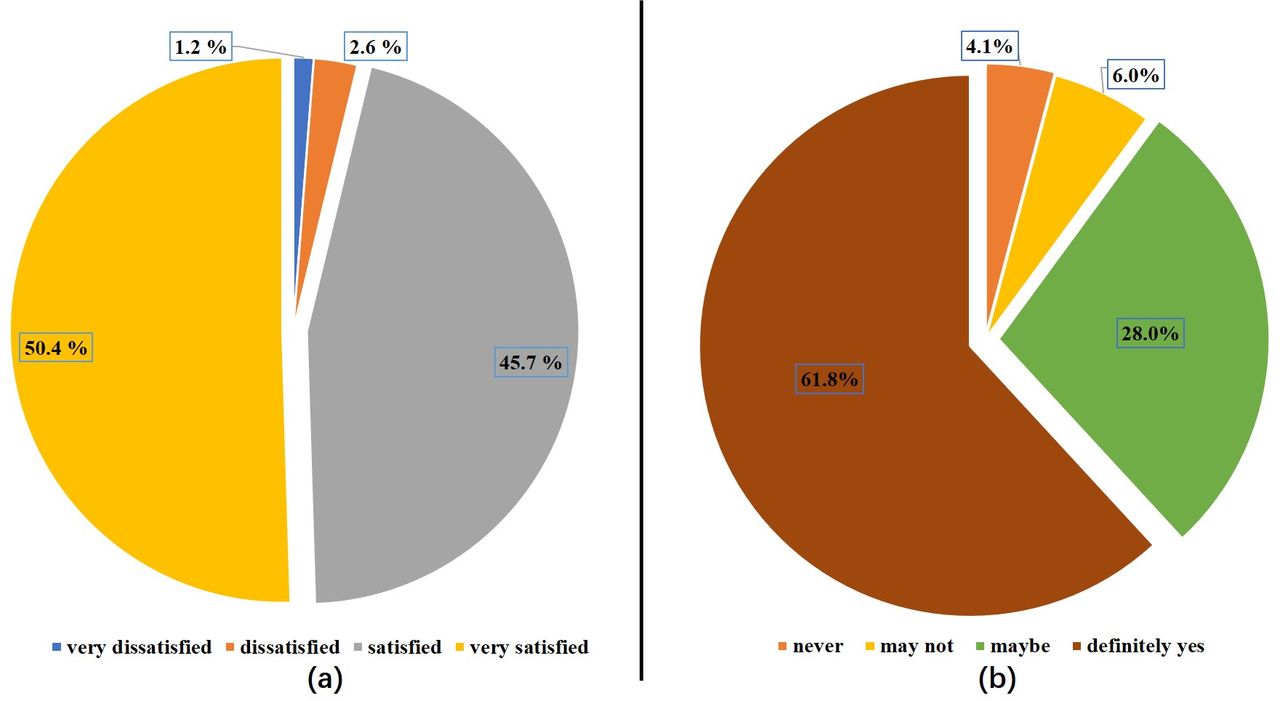
Pie charts of patients’ overall evaluation. (A) Pie chart of patient overall satisfaction (4-level) and (B) pie chart of patient revisiting possibility/patient loyalty (4-level).
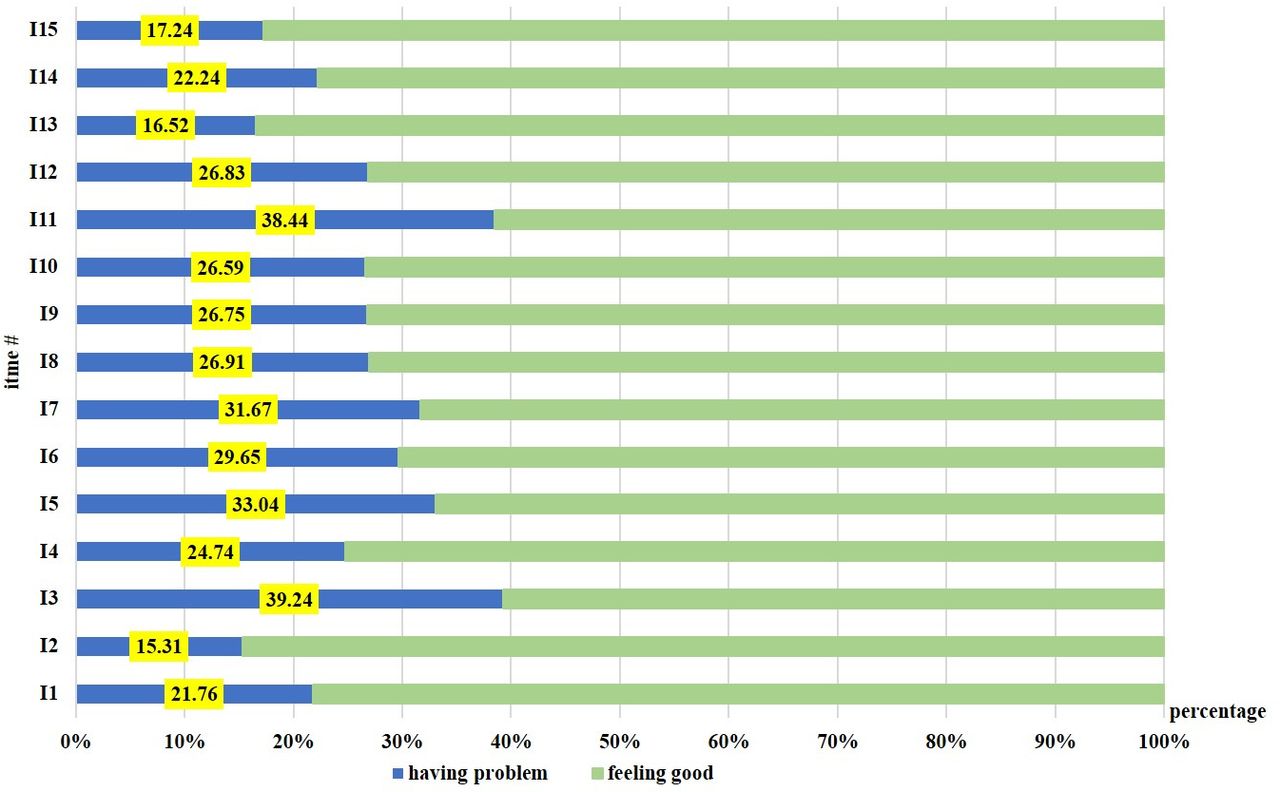
For the convenience of comparison, an adjusted score of the six dimensions is shown in figure 2. Among the six dimensions, the physical comfort dimension (S4, score=2.97) score was the highest, whereas respect for patient preference dimension score (S2, score=2.67) was the lowest. Patients from the study hospitals reported ‘staff providing conflicting information’ to be the most common problem (39.24%; figure 3, online supplementary appendix Ⅵ). Moreover, the total scores of PPE-15 in the 10 participating hospitals showed a significant difference (ANOVA test, F=15.361, p<0.01).

Score for each dimension of patient experience in the 10 sample hospitals. S1, information and patient education; S2, respect for patient preference; S3, emotional support; S4, physical comfort; S5, involvement of family or friends; and S6, continuity of medical service. PPE, Picker Patient Experience.
{kind=link}
{kind=link}
{kind=link}
Problems identified by the PPE-15 Questionnaire. PPE, Picker Patient Experience.
Patient satisfaction, loyalty, and experience
Pearson’s correlation results showed a positive relationship between patient experience (PPE-15)-satisfaction (p<0.05) and experience (PPE-15)-loyalty (p<0.05). The higher the patient experience score, the higher the patient satisfaction, and higher the possibility for patients with health demands to visit the hospital again. Pearson’s correlation coefficients of experience-satisfaction and experience-loyalty were 0.366 and 0.474, respectively.
Associations between different factors and patient experience
The t-test and ANOVA test showed that patients in different subgroups (age group, education level, marital status, occupation status) showed significant different patient experience (table 1); the score of outpatients (41.39) and inpatients (41.29) did not differ significantly (p=0.73), except in the dimension of respect for patient preferences (t=−2.93, p=0.003<0.05) and physical comfort (t=2.85, p=0.004<0.05, table 3).
Picker Patient Experience (PPE-15) scores of outpatients and inpatients†
The gamma correlation coefficients indicated that six items were significantly correlated with overall satisfaction (G≥0.5, p<0.05): respect for patient preference (S2) and continuity of medical service (S6) were strongly correlated with overall satisfaction (table 4).
Gamma grade correlation coefficient between different items of the PPE-15 Questionnaire and overall satisfaction
Table 5A and B shows the multiple correlations between different factors and patient experience. The linear regression analysis showed that except for hospital difference, age and occupation status had a strong influence on patient experience. Moreover, respect for patient preference (S2) was the most important predictor of overall satisfaction.
Results of the linear regression analysis between different factors and patient experience (PPE-15)
Results of the order regression analysis between different dimensions of PPE-15 and overall satisfaction
Discussion
Principle findings
After the new healthcare reform in China, the quality of healthcare services in county-level hospitals gradually improved, especially in terms of patient experience and satisfaction.21 24 The mean PPE-15 score in the 10 sample hospitals was 41.33. Moreover, 61.8% patients thought that they received a very satisfactory healthcare service, and 50.6% responded positively to the possibility of visiting the hospital again in case of a need. In general, patients visiting county-level hospitals during the study period had a good experience and were satisfied, and the better the patient experience, the higher the satisfaction and also the patient loyalty.36 37 Our findings also showed that outpatients and inpatients had a similar experience during their visits.
Strengths and weakness
As a universally used scale to evaluate patients’ experiences in hospitals, the PPE-15 focuses more on inpatient experience.7 34 Nevertheless, in China, hospitals play a key role in providing both inpatient and outpatient services. This study evaluated both outpatient and inpatient experience of county-level hospitals with a well-established scale. The translated PPE-15 questionnaire showed good validity and reliability in the pilot study. The research was conducted in only 10 hospitals from three provinces, which might not be enough to reflect the national status of patient experience in county-level hospitals. As a cross-sectional study, this work might not reflect the changes in patient experience during the reform. In future, we aim to expand the sample size and continue to focus on the improvement of healthcare services in the sample hospitals. Additionally, measures of patient experience vary widely, with different tools using complex or ambiguous concepts. Thus, the evaluation of inpatient and outpatient experience with the PPE-15 may yield different findings from those obtained using other evaluation scales or tools. Last but not the least, there are many different kinds of factors that influence experience during visiting time, and we would like to consider other influencing factors of patient experience in a subsequent study to improve the quality of healthcare services in China’s county-level hospitals.
Interesting findings on patient experience in China’s county-level hospitals
In general, improving inpatient experience and overall satisfaction is an effective way to increase patients’ loyalty to a hospital, which is a crucial issue to improve the quality of healthcare services in county-level hospitals. Other research groups also reported similar findings.36 37 Our findings also showed that outpatients and inpatients had a similar experience during their visiting time. Using a well-established scale, our findings thus suggest that the service improvement programme led to a balanced ability of fulfilling different health demands of various kinds of patients. Reducing the pain that patients experience is more feasible for improving patient experience.8
China’s new healthcare reform has improved the services of county hospitals; however, patient experience still needs to be improved.29 37 38 Different subgroups of patients had different experiences during their visit. Patients of different age groups and occupation status showed significant differences in patient experience, whereas gender, education level, marital status, service type and insurance type had no significant effect on PPE-15 scores; these findings partly differed from the results of previous research conducted in other areas in China,7 29 36 38 India5 and Southeast Norway.11 Regardless of the differences in results, these finding cannot be used as an excuse for medical staff to deal with selected patients but need to guide professionals to manage different kinds of patients more effectively.
Analysing the details of patient experience, we identified several problems that need to be addressed. Even though overall patient experience was good, there were obvious problems that needed to be handled. The lowest score of PPE-15 was respect for patient preference in the present study. In the correlations between different patient experience items and overall satisfaction, the items with strong correlations suggest that county-level hospitals in core areas could improve patients’ satisfaction by showing more respect for patient preference, which was similar to findings in other countries.25 34 However, items with weak correlations cannot be considered unimportant factors, and they should be given more attention in future studies. Information transmission and patient education are not only essential steps for medical staff to improve the health literacy of rural citizens,21 26 but are also goals of the ‘Healthy China’ strategy.24
Furthermore, the most common problem was receiving answers from different medical staff. More than one-third (39.24%) of the participants reported that ‘staff provided conflicting information’. Conflicting information may confuse patients about their condition and diminish their trust in doctors. Once patients fail to trust the medical staff, their loyalty to the hospital will decrease.39 40 About 38.44% of patients thought ‘family or friends did not get the opportunity to talk to doctors’. The present study showed that doctors, patients, their family and friends were all considered important in terms of communication. With the rapid development of treatment skills, patients are more concerned about the comfort of the service than the quality of the treatment and diagnosis they receive.4 10 41 The longer the communication time with medical staff, the better the experience of patients during their visit.1 10 25 42 Compared with urban tertiary hospitals, having fewer patients allows medical staff in county-level hospitals to spend more time taking care of patients’ demands, and this aspect should be developed into a strength for county-level hospitals. These results suggest that the need for more effective communication, which involves more talking time with patients and those close to them, and more consistent information are core problems of patient experience improvement in China’s county-level hospitals.
Conclusion
Among the elaborate goals of the hospital reform, improving patient experience can enhance the quality of care, governance, public accountability and patient choice.20 The results of this study can lay the foundation for further comparisons with international reports and enrich multicentre research on patients’ experiences in county-level hospitals. The results from patient experience surveys can be added to the hospital performance evaluation scale for continuous quality improvement and for identifying the main problems from the patients’ perspectives. In the development of modern county-level hospitals, managers and health service providers in county-level hospitals should listen closely and properly address the demands of patients and their families by meeting patients’ needs, improving the consistency of information and respecting patient preferences.
Acknowledgments
This research received considerable assistance from the National Health and Family Planning Commission of People’s Republic of China, relevant government authorities and participating hospitals. We would like to thank the study participants for their involvement. We would also like to thank Editage (www.editage.com) for English language editing. We are also grateful to Professor Fu Qiang from Saint Louis University, USA, and Dr Gan Yong and Dr Zhang Zinan from Tongji Medical College for their suggestions to the statistical analysis.
References
Footnotes
PF and BW contributed equally.
Contributors PF planned the study. PF and BW contributed to study design and contacted with sample hospitals. PF, RM, CZ and CT performed the research in the sample hospitals. RM, LL and CZ cleaned and analysed the data and drafted the manuscript. All the authors contributed substantially to the interpretation of the results and the writing of the manuscript. All the authors have read and approved the final version of the manuscript.
Funding This study was supported by grants from the China Medical Board-Opening Competition Program 2015 (No. CMB15-223) and Project funded by China Postdoctoral Science Foundation (2018M630871).
Disclaimer The sponsors played no role in the design and implementation of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and the decision to submit the manuscript for publication.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was granted approval from the ethics committee of our college (IORG No: IORG0003571).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The national data collected from China statistical yearbook can be accessed from the website of National Bureau of Statistics of China (http://www.stats.gov.cn/tjsj/ndsj/2016/indexeh.htm.). The national annual data collected from China health statistical yearbook can be accessed from the publication of China National Health Commission (NHC), or can be bought from the publisher (www.pumcp.com). Patient data are available from the corresponding author upon reasonable request.