Article Text

Abstract
Objective To explore the level of cardiopulmonary resuscitation (CPR) knowledge among allied health professions (AHPs) students and its associated factors.
Methods This is a cross-sectional study assessing CPR knowledge among AHP students. A multidisciplinary expert panel designed a survey, which then was piloted to 20 potential participants. The survey had two sections, including demographics and knowledge questions. Knowledge questions scores ranged from 0 to 10, where 10 indicates all questions were answered correctly.
Results A total of 883 students completed the surveys and were included in the study. The mean age was 21 years (±1.6) and the majority were females (73.1%). A total of 693 (78.5%) students did not receive previous CPR training and the top barriers to receiving CPR training were unawareness of training opportunities and a lack of time. Participants had a mean CPR knowledge score of 3.9 (±1.7) out of 10 maximum potential points. Trained participants had a higher mean score compared with the untrained (4.6 (±1.6) vs 3.8 (±1.6), p<0.001). Previous training (adjusted β=0.6; 95% CI 0.2 to 0.9; p<0.001) and being in the physical therapy programme (adjusted β=0.5; 95% CI 0.1 to 0.8; p=0.01) were associated with higher knowledge.
Conclusion There is poor knowledge of CPR among AHP students including trained individuals. Efforts to increase the awareness of CPR should target students and professionals who are highly likely to encounter patients requiring CPR. Compulsory training courses, shorter training periods as well as recurrent and regular refreshing courses and use of various media devices are recommended.
- cardiopulmonary resuscitation
- CPR
- knowledge
- allied health professions
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study assessing cardiopulmonary resuscitation (CPR) knowledge among allied health profession (AHP) students in Jordan.
The results of this study will provide a baseline for future research regarding CPR among AHP in Jordan.
Our study findings and recommendations can influence strategies to improve CPR knowledge and willingness to deliver CPR in Jordan.
There is no standardised or validated CPR survey. However, a multidisciplinary expert panel designed a survey, which was piloted to 20 potential participants.
The inherent nature of the cross-sectional design of this study and potential recall bias of CPR training may have affected reporting the association with knowledge.
Introduction
Cardiac arrest is a major healthcare problem with poor survival rates. Early cardiopulmonary resuscitation (CPR), including bystander CPR, is significantly associated with improved survival to hospital discharge rates from out-of-hospital cardiac arrest (OHCA).1–3 It is also a crucial element in the chain of survival in OHCA.1 2 4 Therefore, training of large numbers of people continues to be a priority for the American Heart Association (AHA) and Red Cross/crescent organisations around the world.5
Reports indicated that the Middle-East and North Africa (MENA) populations are increasing significantly over upcoming decades, including Jordan.6 With expected longevity, there will be an increasing incidence of cardiovascular diseases.7 Moreover, a small study in Northern Jordan reported that only 3% OHCA patients survived (n=79), explaining this by the lack of CPR knowledge and skills.8 Furthermore, allied healthcare professionals and students are expected, and often have to attend life-threating emergencies including cardiac arrests. Furthermore, international studies also reported that trained individuals were more willing and confident to perform bystander CPR.5 9 10 Therefore, trained professionals or students may be able to perform early CPR, initiate resuscitation efforts and speed up the access to prehospital and definitive care. This may lead to the increased survival rates and improving patient outcomes.11–16 In addition, studies concluded that basic and advanced life support skills deteriorate after only 6 months post-training.12 13 17 Therefore, it is imperative to continuously refresh trainees knowledge and skills on a regular basis.
There is a paucity of research regarding CPR knowledge in Jordan in general. Therefore, as a first step, this study explores the level of knowledge among allied health professions (AHPs) students and possible factors that contribute to their knowledge. This line of research is highly needed to establish effective strategies for improving CPR knowledge and skills in Jordan, including Jordanian universities. The study will also provide a baseline for future research regarding CPR knowledge and training among AHP professionals in Jordan. These effective strategies and future research may provide a model that can be adopted within Jordan as well as in the MENA region.
Methods
Design and setting
This is a cross-sectional study assessing CPR knowledge among AHP students in the Faculty of Applied Medical Science (FAMS). FAMS is a relatively newly established comprehensive allied health sciences faculty at Jordan University of Science and Technology (JUST) with nine undergraduate programmes: medical laboratory sciences, physical therapy, occupational therapy, speech pathology, dental technology, allied dental science, radiological technology, optometry and paramedicine. A multidisciplinary expert panel, including paramedicine, physical therapy and occupational therapy academics, designed and assessed the questionnaire for face and content validity. A second group of four paramedicine graduates also evaluated the survey providing feedback that further improved the validity of the survey. The study survey was primarily designed based on the 2015 AHA recommendations for laypersons CPR training as well as the relevant literature (Survey questions and potential answers are provided in online supplementary appendix A).1–4 The survey (in the Arabic language) was then piloted with a group of 20 AHP students and 5 paramedicine professionals to further evaluate its validity. Following this, the survey was updated based on students’ and professionals’ feedback. The main changes included changing one knowledge question answers to give more clarity and modifying the wording of two other questions to improve readability. The expert panel approved the final version.
Supplemental material
The survey was paper based, anonymous and included two sections: the demographics section (section 1) included participants’ demographic, university level (which year in the programme), university cumulative grade point average (GPA), the status of previous CPR training, as well as motivators and barriers to learning CPR. The knowledge section (section 2) included 10 questions that evaluated the knowledge about performing CPR and a question about the emergency phone number in Jordan. Nine of these questions had four different potential answers with only one correct answer, while one question was a true/false question. The scores of the questionnaire range from 0 to 10, where 10 indicates all questions were answered correctly.
Sample and setting
A convenient sample consisting of second, third and fourth-year AHP university students were invited to voluntarily participate in the study. The FAMS offers 4-year Bachelor of Science programmes of nine AHP majors. Of these, we approached eight majors including medical laboratory sciences, physical therapy, occupational therapy and speech pathology, dental technology, allied dental science, radiological technology and optometry.18 Trained individuals were primarily defined as students who had CPR certification and/or hands-on training with post-training summative assessment by professionals. However, to be less restrictive, individuals who learnt via interpersonal demonstration were also considered trained individuals.19
The principal investigator (AOO) and research assistants recruited student participants, explained its purposes and collected surveys on completion. A sample size larger than 500 participants is considered excellent in cross-sectional studies.20 In addition, there were at least 30 participants in each major. Furthermore, participants who were in their first year and those included in the pilot study were excluded. First-year students were excluded as they can change their admissions, after their first year, to programme other than AHP. All participants in this study signed IRB informed consent forms and received no compensation for their participation.
Statistical analysis
Continuous variables were reported as means and SD. Participants were categorised as trained if they have received any CPR training, whereas untrained individuals were students who never had any CPR training. Comparisons between trained and untrained groups performed using independent Student’s t-test. To compare the mean between the groups, analysis of variance (ANOVA) with post hoc analyses using Bonferroni correction was used. Categorical data were presented as counts and proportions, and the difference between trained and untrained groups was compared using X2 tests followed by two-sample test of proportions to identify between-groups differences. Associations with students’ knowledge (maximum potential score of 10 points) were examined using univariate linear regression analyses. Variables with a p<0.2 were then taken forward to the multivariate regression analysis. Furthermore, to identify the variables independently associated with CPR knowledge, a multivariate regression model with stepwise backward elimination was used. In all multivariate regression analyses, a p value of 0.05 was specified for addition to the model, whereas we specified p>0.1 for removal from the model. Linear regression assumptions including collinearity were checked and no violation was present (none of variable inflation factor was over 5).21 All statistical analyses were undertaken using STATA (V.14.0).
Patient and public involvement
No patients involved.
Results
Descriptive analyses
The FAMS at JUST included 1525 students of the second, third and fourth year, with about 70% females (n=1068). Data were collected in April 2018 with 917 (60.1% of the total population) students responding to the survey; however, 883 (response rate of 96.3%) students had completed the survey successfully and were included in the final analysis. Whereas 3.7% were excluded due to incomplete surveys and missing key information.
Table 1 includes descriptive statistics of students as well as comparisons between those who had prior CPR training versus those who never had any CPR training. The mean age of participants was 21 years (±1.6) with the majority being females (73.1%). Only 190 (21.5%) students in this study had previous CPR training (20.6% of males vs 21.9% of females). Trained participants were older than untrained (21.5 years (±1.5) vs 20.9 years (±1.6), p<0.001). Moreover, compared with second-year students, higher proportions of trained individuals were from fourth year (42.6% vs 18.4%; p=0.01) and third year (39% vs 18.4%; p=0.03). Additionally, no significant statistical differences were observed based on sex (p=0.7), having family members with a cardiac history (p=0.7) or grade point average (GPA; p=0.6).
Participants demographics with a comparison between CPR trained versus untrained participants
Table 1 also shows statistically significant differences between at least two groups across the AHP majors and/or between trained and untrained individuals. Based on the two samples test of proportions, the only statistical difference between trained and untrained groups was observed in the physical therapy major (23.2% vs 9.2%, p=0.046). On the other hand, when comparing untrained proportions across majors, a higher untrained proportion was observed in participants from dental technology compared with physical therapy (24.0% vs 9.2%; p=0.01), optometry (24.0% vs 9.1%; p=0.01), occupational therapy (24.0% vs 4.2%; p=0.02) and allied dental sciences (24% vs 2.9%; p=0.03) whereas no differences were observed across majors in the trained group (all p>0.05).
The majority of trained students were trained at the university (57.9%), followed by schools (17.9%), private work or non-governmental organisations (16.8%) or self-learning/private centres (7.4%).
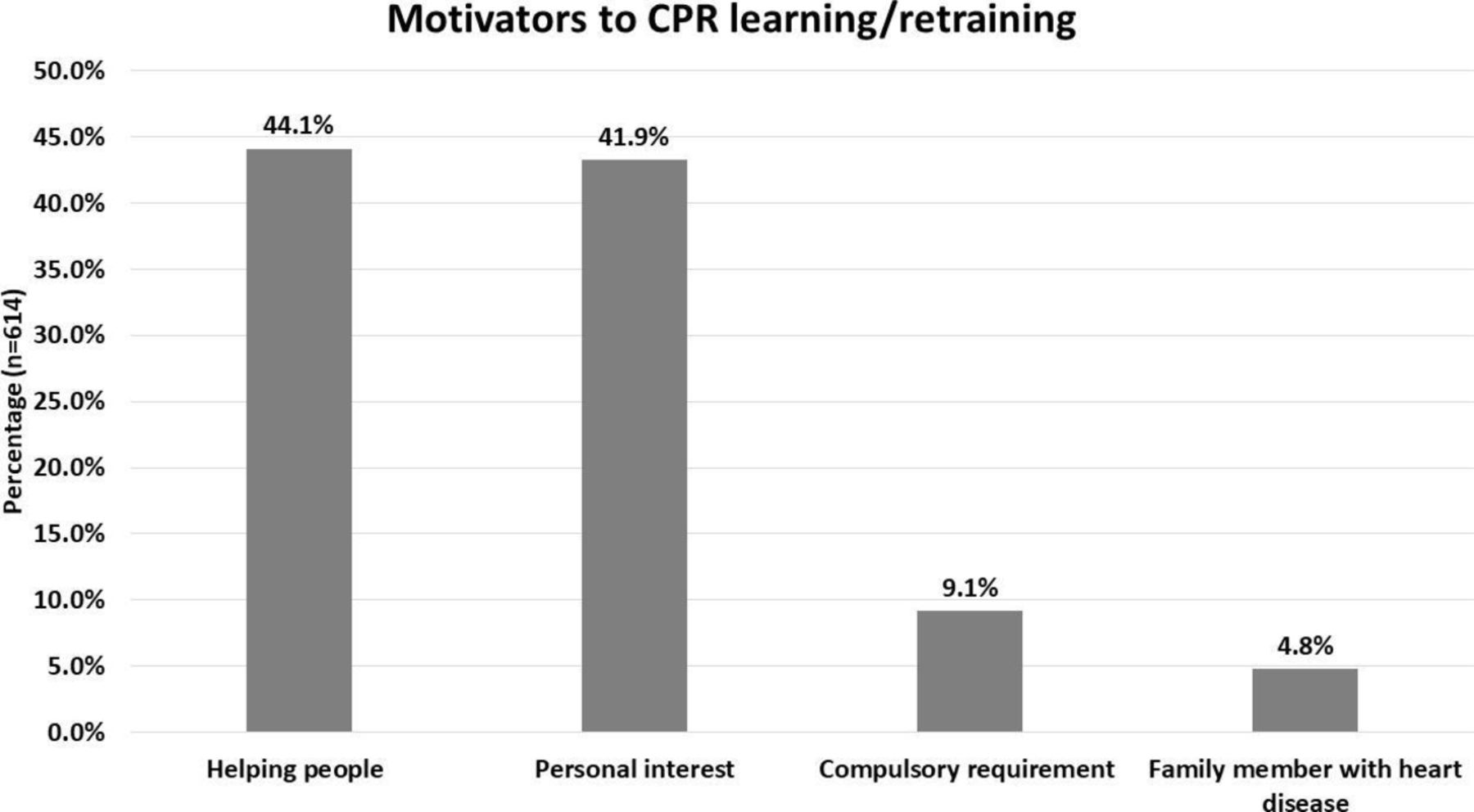
Figure 1 includes the top five barriers that participants indicated for their inability to take the CPR training. The top causes were unknown training locations (33.0%) and the lack of time (32.1%). Moreover, as shown in figure 2, the majority of participants (n=614, 69.5%) indicated that they were willing to enrol in CPR training (or retraining). Helping people (44.1%) and personal interest (41.9%) were the top two motivators to learn or retrain in CPR. Also, motivations for CPR training, of those trained, included personal interest (44.4%), compulsory requirements (40.6%), helping other people and having family members with heart diseases (15.0%).

Barriers to CPR training (n=722). CPR, cardiopulmonary resuscitation.

{kind=link}
{kind=link}
Motivators for CPR training/retraining (n=614; not mutually exclusive). CPR, cardiopulmonary resuscitation.
Table 2 summarises the knowledge scores and their differences among different groups. The overall mean score was 3.9 (±1.7) out of 10 maximum potential points. Additionally, while physical therapy and occupational therapy had the highest mean scores of 4.8 (±1.6) and 4.5 (±1.6) respectively, speech and audiology students had the lowest mean score of 3.3 (±1.4).
Summary and comparisons of knowledge scores
There was no statistically significant difference in CPR knowledge score between males and females (p=0.3). However, the trained group had a higher mean score compared with the untrained group (4.6 (±1.6) vs 3.8 (±1.6), p<0.001). Moreover, using ANOVA, the knowledge score was statistically different between at least two study levels (F (2, 880)=3, p=0.049). Post hoc analysis, using Bonferroni correction, showed a statistically higher knowledge score among fourth-year students compared with second year (4.1 vs 3.8, p=0.045).
In addition, ANOVA results showed significant differences in knowledge scores between at least two academic pragmas (F (7, 875)=9.99, p<0.001). Post hoc analysis, using Bonferroni correction, showed that mean knowledge scores of physical therapy, occupational therapy and radiology were significantly higher than those of speech and audiology (p<0.001) as well as dental technology (p<0.05). Furthermore, physical therapy had a higher knowledge score compared with optometry (p=0.05) and medical laboratory sciences (p<0.001). No other differences were observed in the remaining comparisons.
Furthermore, the knowledge score ranged from 1 to 9 among trained individuals, with 108 students (56.8%) scoring 5 or more points. In addition, when asked about the last time of training, 33.0% had their training recently (<1 year), 24.3% past 2 years, 27.6% in the past 3–4 years and 15.1% more than 5 years ago.
Regression analysis
Table 3 summarises the factors included in the regression analyses. Factors significantly associated with higher knowledge scores were previous CPR training (β=0.9; 95% CI 0.6 to 1.1; p<0.001), age (β=0.1; 95% CI 0.01 to 0.1; p=0.03), fourth-year study level (β=0.3; 95% CI 0.01 to 0.5; p=0.04) and being in the physical therapy, occupational therapy or radiology programmes. Moreover, being in the second year of study and enrolled in dental technology or speech and audiology programme were associated with lower knowledge scores. Having a family member with cardiac disease was not statistically significant (β=0.2; 95% CI −0.03 to 0.5; p=0.1).
Linear regression analyses of factors associated with CPR knowledge
Using a stepwise multivariate regression analysis with backward elimination, previous training remained statistically significant (adjusted β=0.6; 95% CI 0.2 to 0.9; p<0.001). Moreover, being in the physical therapy programme was positively associated with higher knowledge scores (adjusted β=0.5; 95% CI 0.1 to 0.8; p=0.01). On the other hand, lower knowledge scores were associated with speech and audiology (adjusted β=−0.8; 95% CI −1.2 to -0.5; p<0.001), dental technology (adjusted β=−0.5; 95% CI −0.8 to -0.3; p<0.001) and medical laboratory sciences programmes (adjusted β=−0.4; 95% CI −0.7 to -0.1; p=0.02).
Furthermore, table 4 outlines the univariate and multivariate analyses examining the factors associated with knowledge among trained individuals. Time since last training was the only factor associated with CPR knowledge in both analyses. Compared with recent training (<1 year), longer times since last training was negatively associated with the knowledge scores.
Linear regression analyses of factors associated with knowledge scores among trained individuals
Discussion
The study aimed to explore the level of CPR knowledge among AHP students and possible factors that contribute to their knowledge. We recruited a representative sample from eight different majors from the FAMS. Our study shows a poor level of CPR knowledge among AHP students. Surprisingly, this poor knowledge is also observed among the trained group. We also identified an independent association between CPR training and being in the physical therapy. On the other hand, lower knowledge scores were associated with speech and audiology, dental technology and medical laboratory sciences programmes. Moreover, among trained individuals, time since last training was the only factor to predict trained individual level of knowledge. To our knowledge, this is the first study to explore the level of knowledge among AHP students in Jordan. This study can guide future research and provide recommendations and be a model to improve the level of CPR Knowledge in Jordan as well as the MENA region.
Although the variation is not too high, trained individuals were older than their untrained counterparts. This is due to the characteristics of the included sample (the vast majority with age range 19–22 years); therefore, a small variation will cause a significant difference. This may also be due to the increased likelihood of older student to obtain opportunities for training and study major requirements that involved CPR training.
Higher mean knowledge scores were found in physical therapy, occupational therapy and radiology than those of dental technology and speech and audiology. This can be explained by the fact that physical therapy and occupational therapy curricula include an introduction course that mandates CPR training and evaluation. Furthermore, in the physical therapy programme, the curriculum also includes a cardiac rehabilitation course where students have also mandatory CPR training and evaluation with training being delivered by paramedic programme staff. Finally, the radiology programmes also have a patient care-oriented course, which also mandates CPR training.
The majority of participants who did not receive CPR training reported unawareness of training locations and the lack of time as the top barriers. Nevertheless, the majority of participants were willing to be enrolled or repeat CPR training, motivated by their willingness to help people in need and having a personal interest in learning CPR skills.
Despite the differences in populations and survey questions, our results are similar to other studies reporting higher knowledge among trained individuals, despite the poor level of knowledge.22–25 Aroor et al, in study conducted in South India, reported an overall awareness and knowledge of basic life support (BLS) mean score of 4.16 (SD ±1.40) of a 10 maximum indicating a poor knowledge score among nursing, dental and medical individuals including undergraduate, internship and postgraduate groups. However, these knowledge scores based on a survey about BLS knowledge which is not similar to our survey. In addition, the authors found that age, gender, level of training, programme of study and previous exposure to BLS were significantly associated with knowledge level.23 While our regression analysis accounted for most of these factors, only CPR training and being in the physical therapy programme were with the only significant predictors of better knowledge. Barriers to learning CPR, in the Aroor et al study, was similar to the top reported barriers in our study being lack of time and unawareness of where these workshops are held.23
Furthermore, a study in Pakistan including 250 medical students also reported that medical students with BLS training had higher knowledge (mean, SD) compared with those untrained.22 Moreover, Ghanem et al examined the knowledge of CPR among 823 medical university students reporting 27% of participants who received BLS training. The study also reported similar results where CPR knowledge was associated with previous CPR training, despite their overall poor level of knowledge. The majority of participants were males (88.3% of 824) which is different from our study. In addition, despite the low percentage of female participants, the study reported higher knowledge scores among females (p<0.001).24
Other international studies have also reported that trained individuals were more willing and confident to perform bystander CPR.5 9 10 This may reflect that higher knowledge of CPR is associated with previous training. Our results are in concurrence with other studies reporting that BLS skills deteriorate with time post education and training.12 13 17 Therefore, continuous education can increase the level of knowledge and optimise CPR performance.
Furthermore, the poor level of knowledge urges designing compulsory and regular training programmes/courses or graduation requirements. This is arguably especially important for medical and healthcare majors, which are supported in recommendations made in numerous reports.3 22 23 25 Such programmes can teach hands-only/compressions only CPR, which is highly recommended by the AHA4 and was reported to be associated with participants being more willing to perform CPR and higher survival rates.2
To overcome the barriers to taking a CPR course, short training workshops (<30 min) can also be designed.26 This can be combined by introducing media, mobile devices and self-learning videos to expand the number of potential participants who are willing to learn CPR.5 27 Furthermore, Arabic versions of CPR can be developed and validated for the public in Arabic speaking countries, so students and healthcare professionals can help training larger numbers of the population at life-threating risks.
It might be difficult to train all people in Jordan including Jordanian University students, therefore, it is essential to target high-risk groups and/or staff and students who are highly likely to encounter cardiac arrest patients. This may include training the students who report family members with cardiac diseases, students in health-related programmes as well as students in non-medical programmes with the likelihood to encounter cases that can benefit from CPR. Moreover, universities can adopt initiatives to increase training rates as well as maintaining these training. This may include train the trainers initiatives, where academic staff and students in health-related programmes are trained by professionals to qualify them as trainers. This can be followed and/or accompanied by campaigns to train students and the public. Including professional mandatory CPR training and evaluation in certain courses in different study years may also aid in improving CPR knowledge. In addition, short educational videos can be distributed through university applications and can be a mandatory requirement for students’ registration. Furthermore, a work requirement that mandates training in BLS can further improve the level of knowledge among AHP graduates and professionals.
In the developed countries, CPR training is delivered to school students; however, this is not available in Jordan.28 29 Therefore, similar programmes can be adopted to train the teachers and students at various cities and schools in Jordan, this will increase the awareness of CPR and improve survival rate. Moreover, global initiatives such as Restart-a-Heart Day held in October 2018, in which JUST participated and trained over 800 students and staff. This initiative was supported by International Liaison Committee on Resuscitation and trained over 200 000 potential lifesavers.
Although it could be more clinically relevant to display how many students know correct CPR, the aim of this study was to explore how much the FAMS students know about CPR using a 10-point scale. However, future research with different designs can consider measuring the proportion of participants who are able to perform CPR correctly.
The poor level of knowledge found in our study may indicate an inadequate knowledge level among professionals who interact with patients on a daily bases. Further studies are also recommended to examine the professional knowledge and attitude towards CPR in Jordan as well as skill and knowledge retention.
Limitations
The inherent nature of the cross-sectional design of this study and recall bias of CPR training may have affected reporting the association with knowledge. There is no standardised published survey regarding CPR knowledge; however, we adopted our questionnaire based on the AHA 2015 recommendations as well as the relevant literature regarding CPR.1–4 Moreover, an expert panel designed and reviewed the survey from paramedicine and other allied health science fields. The survey was also piloted to 20 AHP students and modified based on their feedback in an attempt to improve validity and reliability.
There is a paucity of research regarding CPR knowledge among AHP students in general. However, we compared our results to studies including university students with health-related majors including medicine, nursing and any AHPs, which considered to be comparable to our cohort due to similar study designs and level of questions.
Generalisability
Although a potential gender skew may be questioned, this percentage is representative of the student in FAMS (70% females). This is more likely due to cultural uniqueness in Jordan, as more females are willing to enrol in health-related disciplines compared with males. Therefore, the gender distribution in this study is expected to be observed at other universities with faculties similar to FAMS at JUST as well as the MENA region. However, generalising the findings of our results should consider the inclusion criteria, type of questions, setting, type of participants and the type of outcome measures used in this study. As per the reported barriers of the AHP students, which are considered a highly educated group in the Jordanian population, a poor level of knowledge could also be expected among the public in Jordan. This poor knowledge is also expected due to lack of public initiatives and mandatory training courses in Jordan.
Conclusion
There is a poor level of knowledge CPR among AHP students in Jordan. However, higher knowledge scores were associated with the previous CPR training as well as more recent training. The study also found that the top barriers were unawareness of training locations and lack of time. Finally, compulsory training courses, shorter training periods and use of various media devices are recommended to reach wider communities. Various initiatives to increase the awareness of CPR among university students and other population are highly recommended.
Acknowledgments
We would like to thank our colleagues, research assistants and participating students for their participation and cooperation during our study.
References
Footnotes
Twitter @alaa_oteir
Contributors AOO conceived the study idea, collected the data, conducted the statistical analyses and drafted the manuscript. AOO, KAA, SFK, MTA and BW had made a considerable contribution to the study design, interpretation, writing and reviewing the manuscript. The final manuscript had been approved by all authors.
Funding This project was funded by Jordan University of Science and Technology (project number: 24/112/2018).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Jordan University of Science and Technology Institutional Review Board approved the study (project number: 24/112/2018).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data sets generated and/or analysed during the current study are not publicly available due to them containing information that could compromise research participant privacy/consent but are available from the corresponding author on reasonable request.